
Abstract
The feasibility study was aimed to develop a web-based gaming tool for the therapy of alcohol use disorder to offer patients a cue-exposure-based extinction and decision training, enhanced with virtual reality. To increase the training effect, patients playfully experience situations that resemble critical real-life situations. For implementing the game, a combination of HTML5 and JavaScript was used. The application comes with an administrator interface, to allow editing the game content. Initially, we included 21 patients (Group 1), 18 suffering from alcohol use disorder and 3 using cannabis (18/3 male/female, mean age 39 ± 13 years). Considering the iterative process of a feasibility study, we developed the game design as suggested by participants of Group 1 and additionally included 11 novel participants (Group 2) (11 suffering from an alcohol use disorder, 7/4 male/female, mean age 46 ± 14 years). Basically, the game was very well received. Usability ratings were generally high, even in patients with little computer experience. Both groups rated the application as realistic, and would generally be willing to play it on a daily basis. Given that SALIENCE is inexpensive, easily available, and engaging, it might be a reasonable add-on intervention to the standard treatment of alcohol use disorder.
Introduction
Substance use disorders (SUDs), such as alcohol use disorder (AUD) and cannabis use disorder (CUD), have gained increasing social concern. They are highly prevalent, cause relevant direct and indirect psychological suffering, and to make matters worse, they are characterized by high relapse rates. Current findings highlight last year’s prevalence rates of 8.5 percent for alcohol 1 and 9.5 percent for cannabis. 2 The disability adjusted life years (DALYs) is a measure of the global burden of disease and integrates the number of years lost due to ill-health, disability, or early death. A recent systematic review 3 reported that in 2010, mental and substance use disorders caused approximately 183 million DALYs. Within these groups, AUD caused circa 18 million and CUD accounted for 2 million DALYs. 4
Despite many years of research, remission rates are low, and relapse risk is high. After detoxification, almost 90 percent of patients suffering from AUD 5 and 28 percent suffering from CUD 6 will relapse in a 1-year or 3-year period, respectively. Aside of general factors, such as motivation to abstain and self-efficacy to refrain from use, many other factors increase the relapse risk. These other factors include pretreatment peer contacts, direct offers to use, stress and interpersonal conflicts, aversive emotions, and withdrawal symptoms. 7 One further very relevant risk factor for relapse represents a “craving,” that is, a consuming desire to misuse a substance. To better understand “craving” and risk factors for craving, functional magnetic resonance imaging has emerged as a suitable tool. 8 It has been shown repeatedly that psychological and physiological responses to alcohol and cannabis stimuli, also called alcohol cue reactivity, trigger certain brain areas involved in relapse processes.8,9 Against this backdrop, and in support of the clinical significance of cue reactivity as a major trigger for relapse, cue-exposure therapy (CET) has been introduced to facilitate the therapy of patients suffering from AUD 10 and tobacco use disorders. 11 CET aims at removing pathological associations by exposing individuals to alcohol-related stimuli while their usual drink responses are prevented. This may result in extinction of the cue-response association, and, at best, in a decrease of the craving and relapse. 10 There is emerging evidence for the successful application of CET in the treatment of AUD. 12 Compared with pre-CET, cue-reactivity reduction was greater in the CET relative to the control group, especially in the anterior cingulate gyrus, the insula, as well as in the left ventral striatum. Other studies have shown that CET for alcohol-dependent patients reduced alcohol consumption and prolonged abstinence.13,14 Effect sizes of CET have been reported to range from 0.54 to 0.74. As a limitation, it has to be emphasized that CET might be particularly useful for anxiety disorders, specific phobias, and AUD but less suitable for other addictions. 14 Furthermore, one study 12 only assessed reduction of alcohol-associated brain responses but did not assess data on potentially beneficial treatment effects of CET with regard to relapse and drinking behavior necessary for any further conclusions with regard to CET efficacy. This might also suggest that CET is only affective for patients characterized by high cue reactivity. 15 Therefore, CET has been augmented with virtual reality (VR). 10 VR provides a broad spectrum of interactive possibilities, environments, and mechanisms by which new behaviors can be learned in novel and engaging ways. 16 By this means, VR interventions may be suitable for treating several psychiatric disorders, being flexible in intervention timing, cheap, and providing the possibility to develop personalized treatments at the same time. 16 In addition, the beneficial effects of add-on VR cues have already been demonstrated in the treatment of various anxiety disorders, such as social phobia and agoraphobia, 17 the fear of flying, 18 generalized anxiety disorders 19 (for a systematic review see 20 ), as well as posttraumatic stress disorders. 21
Furthermore, it has been shown that decision-making deficits 22 are associated with substance consumption and relapse risk. 23 Therefore, adding a decision-making training component to standard treatment might be promising. 24
Addressing these issues, we present here the gaming-based application SALIENCE (which stands for Stop ALcohol In Everyday life—New Choices and Evaluations). It refers to pathological levels of incentive salience being attributed to substance-associated cues in substance use disorders, 25 combining a classical cue-exposure paradigm, including decision training with VR.
Materials and methods
Participants
All participants were recruited from the day clinic of the Department of Addictive Behavior and Addiction Medicine at the Central Institute of Mental Health in Mannheim, Germany. The protocol (registration at: clinicaltrials.gov; NCT03765476) followed the principles of the Declaration of Helsinki for participants’ rights and study procedures and was approved by the local ethics committee (2018-593 N-MA). Informed consent for participation was obtained from all participants before entering the study.
We initially included 21 participants (Group 1) in the study, 18 suffering from AUD (2 of them with comorbid CUD) and 3 suffering from CUD according to the pertinent criteria of the DSM-IV-TR (3 females and 18 males, aged 39 ± 13 years). The mean duration of AUD was 11 ± 9 years.
Implementing suggestions and feedback of the first group of participants (we now highlighted doors and routes, used bigger and sharper images, and replaced a complete scene), and also considering our own reflections of how to improve the game, we additionally tested a second version of our serious game in a further group of novel patients (four females and seven males, aged 46 ± 14 years). The mean duration of AUD was 12 ± 10 years.
Inclusion criteria for both groups were as follows: minimum age of 18 years and a diagnosis of SUD according to pertinent criteria of the DSM-IV-TR. Comorbid disorders including major depression, panic disorder, agoraphobia, social anxiety disorder, and generalized anxiety disorder were accepted to maximize the generalizability of the findings. The concurrent use of antidepressants, anxiolytics, and hypnotics was deemed acceptable. Participants were excluded if they suffered from an Axis I or II disorder, excluding those listed in the inclusion criteria that were likely to have interfered with the patient’s ability to participate in the study, as judged by the investigators.
Development of the SALIENCE application
The game was implemented as a lightweight web application. This allows it to be played on various devices, including tablets, laptops, and desktop computers, since it does not require installation of additional software.
For implementing the game, a combination of HTML5 and JavaScript was used. To reflect the dynamic requirements of both the game and the authoring interface, AngularJS was used to provide a bidirectional data binding. This has the advantage that the content of the web page can be changed dynamically without reloading it in the client. The server side was implemented in JavaScript as well using the lightweight express framework running on the Node.js server software. Finally, an API was constructed that allows saving and load data in the JSON format as well as to load new images.
The image-based approach was used on purpose instead of a full three-dimensional (3D) virtual environment. A 3D virtual environment where players can freely move with a virtual avatar would allow for a higher degree of freedom for the players; however, creating such an environment and adding new content to it comes with considerable developmental effort, especially when creating a realistic-looking and believable world. If not done right, players might fall into the “uncanny valley,” rendering the possible training effects of the virtual environment useless. 26 The image-based approach, on the other hand, allows creating new realistic scenes at almost no cost.
The application comes with an administrator interface, which allows editing the game content based on the structure presented above. To add a new level to the game, the first step is to provide the assets, that is, the panoramic images for story scenes as well as the background image and pictures of beverages for the training scene. These can be added by anyone, both supervisors and patients. An administrator can then set up the level and the corresponding location in the web-based interface. No programming effort is needed for this task. Instead, the assets are uploaded to the server and can then be assigned to the different scenes and interactive objects in a graphical user interface. As soon as the location and level are added to a new or existing story, the new content is available to all players.
The game concept
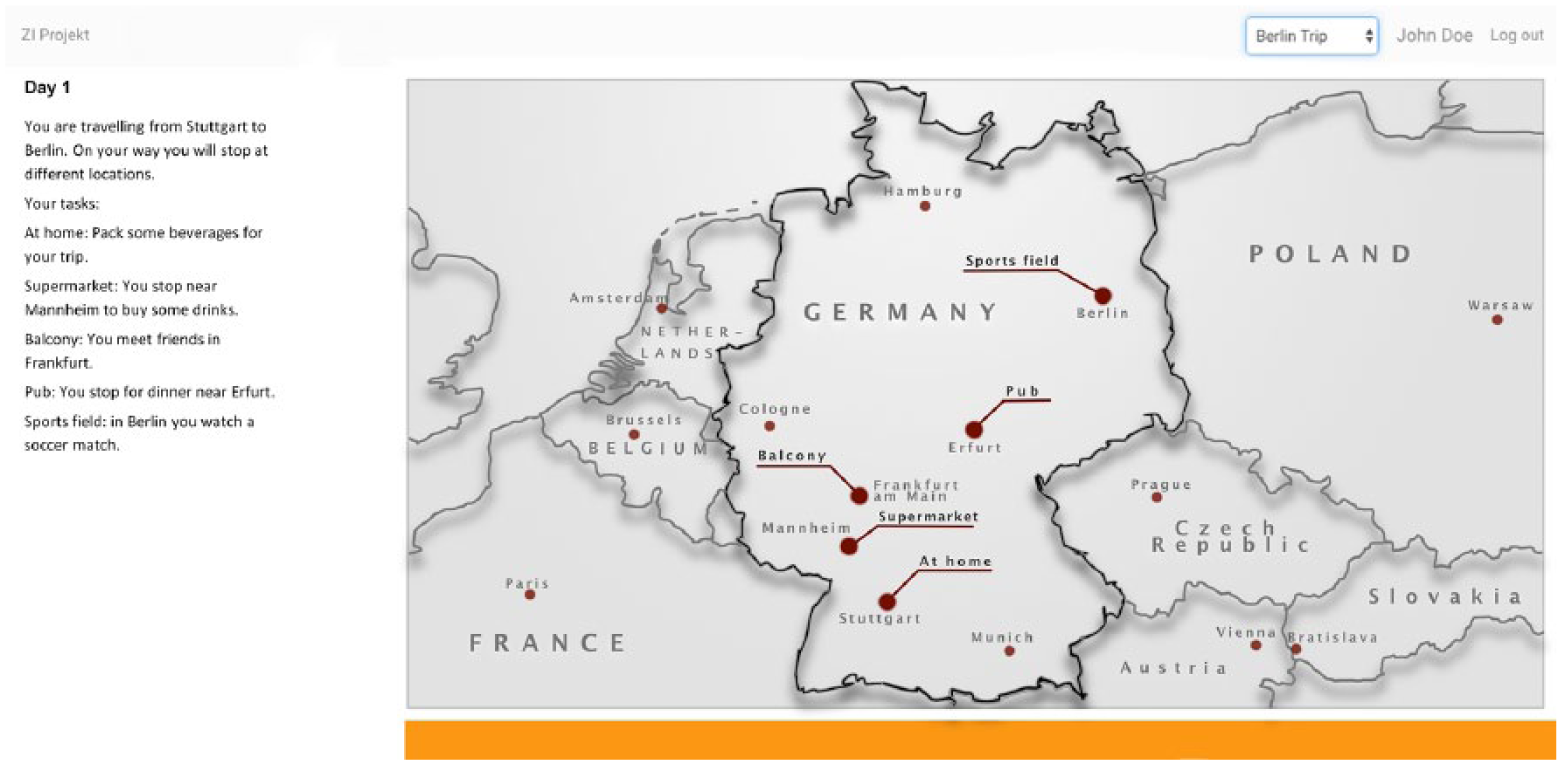
After logging in, players are presented with a map view (implemented with map data from Google©, see Figure 1). The application uses a variable data structure that allows managing all the different game contents. The highest logical element is a story. Each story consists of at least one location. A location is linked to a real-world geographic location so that it can be displayed on a map view. Markers on the map show the available locations that contain the different levels of a story, that is, a set of levels that correspond to a play session. The levels are based on real-world panoramic photos that were combined with interactive elements. In the style of a point-and-click adventure game, players can look around in the level by dragging the panoramic image, and interact with objects by clicking on them (for more details see Figure 2 and Supplemental Table 2).
Screenshot of the graphical user interface of the game SALIENCE, showing an exemplary task (left), which has to be conducted on a virtual route (right).

Screenshot of the game SALIENCE showing (a) a panoramic image and (b) a section with an interactive object (green box).
Each level consists of at least two scenes, which can be implemented as a story scene or a training scene. A story scene contains a panoramic image with interactive elements and a link to the next scene. A training scene leads to the actual augmented CET training. When the training has been performed, the level ends, and the locations are closed. The player can then pick another location from the map.
The implemented serious game resembles situations where patients might be confronted with alcohol during their daily routine (e.g. grocery shopping, stopping at the gas station, or meeting friends at a restaurant). The story takes patients from the start to the situation where they have the choice between an alcoholic and a non-alcoholic drink. To make the training more realistic, the pure CET was augmented with additional story and game elements, and it also includes a decision-training component, by presenting patients with familiar images from which the non-alcoholic beverages should be chosen. The application provides players with a series of the aforementioned situations in each play/training session. Multiple situations are combined to form a daily routine. This phase of the training should not be altered much so that the basic characteristics of the CET method are retained. For this feasibility study, the participants played one session of the game, which lasted about 10–15 min. As add-on treatment in a clinical setting, patients should play the game on a regular basis, for example, three times a week like in CET.
The Central Institute of Mental Health in Mannheim and the University of Mannheim, Germany developed the application jointly.
Instruments (questionnaires)
To evaluate the game, the participants (both groups) had to answer a questionnaire (for details see Supplemental Table 1). Participants were asked to rate the user-friendliness and whether they liked the playful character of the game. Moreover, they were asked: Did you find the game optically pleasing? Did you like the panorama control? How realistic was the game situation? Did the game include everyday situations? How frequently do you use computers? How much experience do you have with playing video games; can you imagine playing the game on a daily basis? What may the consequences of periodic training be on the success of your treatment? All but the last four questions had to be rated on a Likert-type scale ranging from 1 to 7 (questionnaire see Supplemental Table 1).
In Group 2, we additionally captured the participants’ craving status before, during, and after playing the game, applying the Alcohol Urge Questionnaire (AUQ,) 27 and by asking patients to rate their craving for alcohol on a visual analog scale (VAS) ranging from 0 (“no craving”) to 100 (“extremely extensive craving”). Moreover, we now measured total play time and reaction times for each participant (easy/hard context and with/without assistance).
Objectives and guiding questions for a feasibility study
Due to the design of this study, we considered the “objectives and guiding questions for a feasibility study,” referring to a work by Orsmond and Cohn. 28 In their work, the authors present five objectives, again concretized by guiding questions 28 as key considerations for planning and performing a feasibility study: Objective 1: Evaluation of recruitment capability and resulting sample characteristics. Objective 2: Evaluation and refinement of data collection procedures and outcome measures. Objective 3: Evaluation of acceptability and suitability of intervention and study procedures. Objective 4: Evaluation of resources and ability to manage and implement the study and intervention. Objective 5: Preliminary evaluation of participant responses to intervention.
Statistical analyses
IBM’s Statistical Package of the Social Sciences (SPSS) Statistics for Windows, Version 22.0. (IBM Corp., Armonk, NY, USA) was used for statistical analyses. Since we conducted a feasibility study, only descriptive analyses were conducted. Group comparisons of demographic and other variables were performed using t-test and Mann–Whitney U test.
Results
Group 1
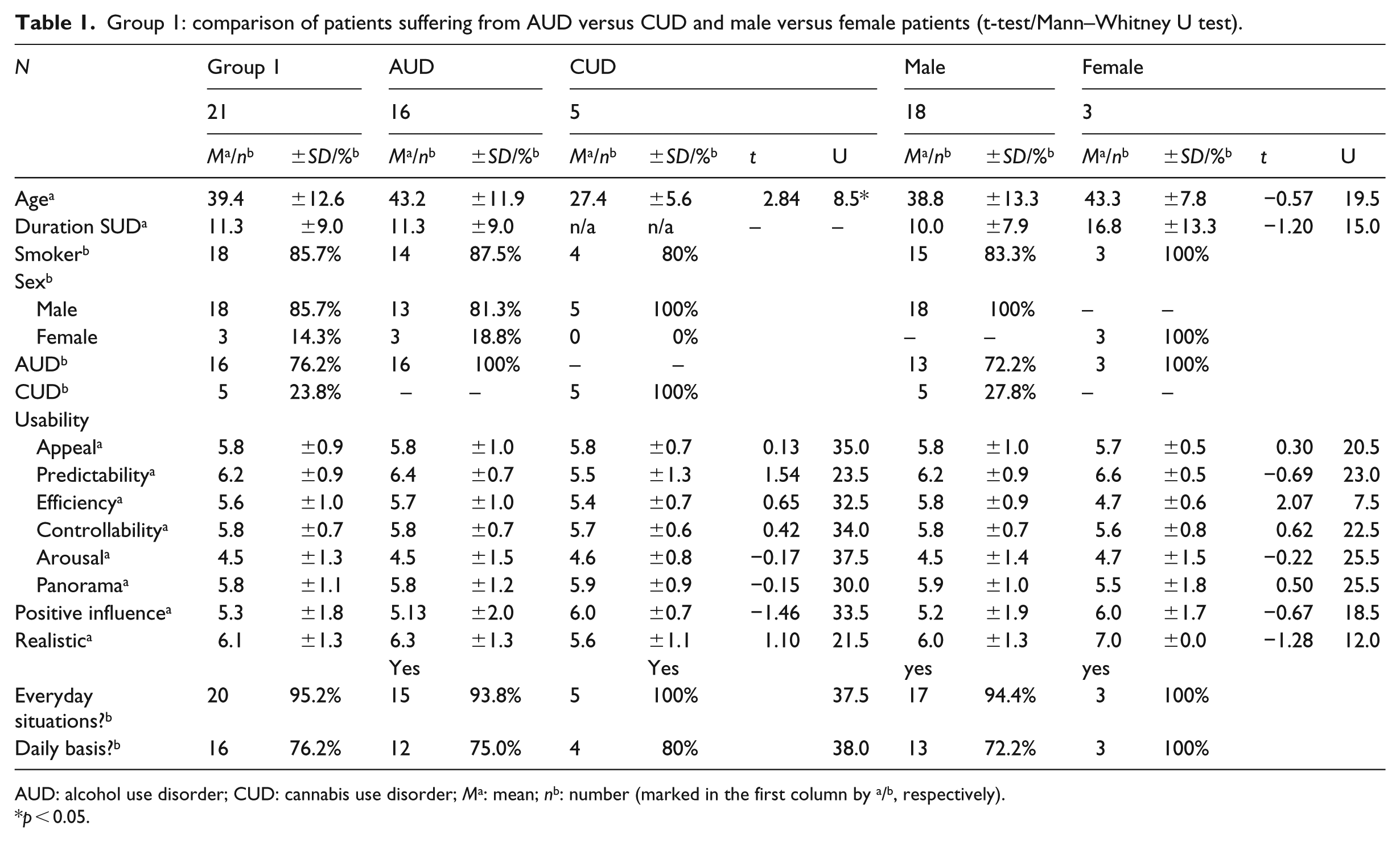
The overall ratings by the patients were very positive (see Table 1). The usability categories have reached arithmetic averages of 5.81 ± 0.90 in appeal (i.e. mean rating of items 8, 10, 14, 15), 6.22 ± 0.90 in predictability (i.e. mean ratings of items 1, 2, 13), 5.64 ± 0.95 in efficiency (i.e. mean ratings of items 6, 9), 5.78 ± 0.66 in controllability (i.e. mean ratings of items 5, 7, 12), and 4.51 ± 1.34 in arousal (i.e. mean ratings of items 3, 4, 11). Regarding the panorama navigation, the arithmetic average of 5.80 ± 1.11 was reached (i.e. mean ratings of items 16 a and b). Surprisingly, the panorama control was even well accepted by patients who use a computer on not more than 1 day per week (N = 8, 6.13 ± 1.19), intriguingly representing almost one-third of the patients (28%). Likewise, approximately one-third does not have any (“never”) or almost any (<1 day/week) experience with playing video games (for more details see Supplemental material). Nevertheless, 76 percent of the patients (only AUD) can imagine playing the game on a daily basis, and 93 percent stated that the game included everyday situations (for more details see Supplemental Figure 1).
Group 1: comparison of patients suffering from AUD versus CUD and male versus female patients (t-test/Mann–Whitney U test).
AUD: alcohol use disorder; CUD: cannabis use disorder; Ma: mean; nb: number (marked in the first column by a/b, respectively).
p < 0.05.
The game situation was seen as mostly realistic (6.14 ± 1.28), and the perceived influence of periodic training on the success of the treatment was positively evaluated (5.33 ± 1.83).
Group 2
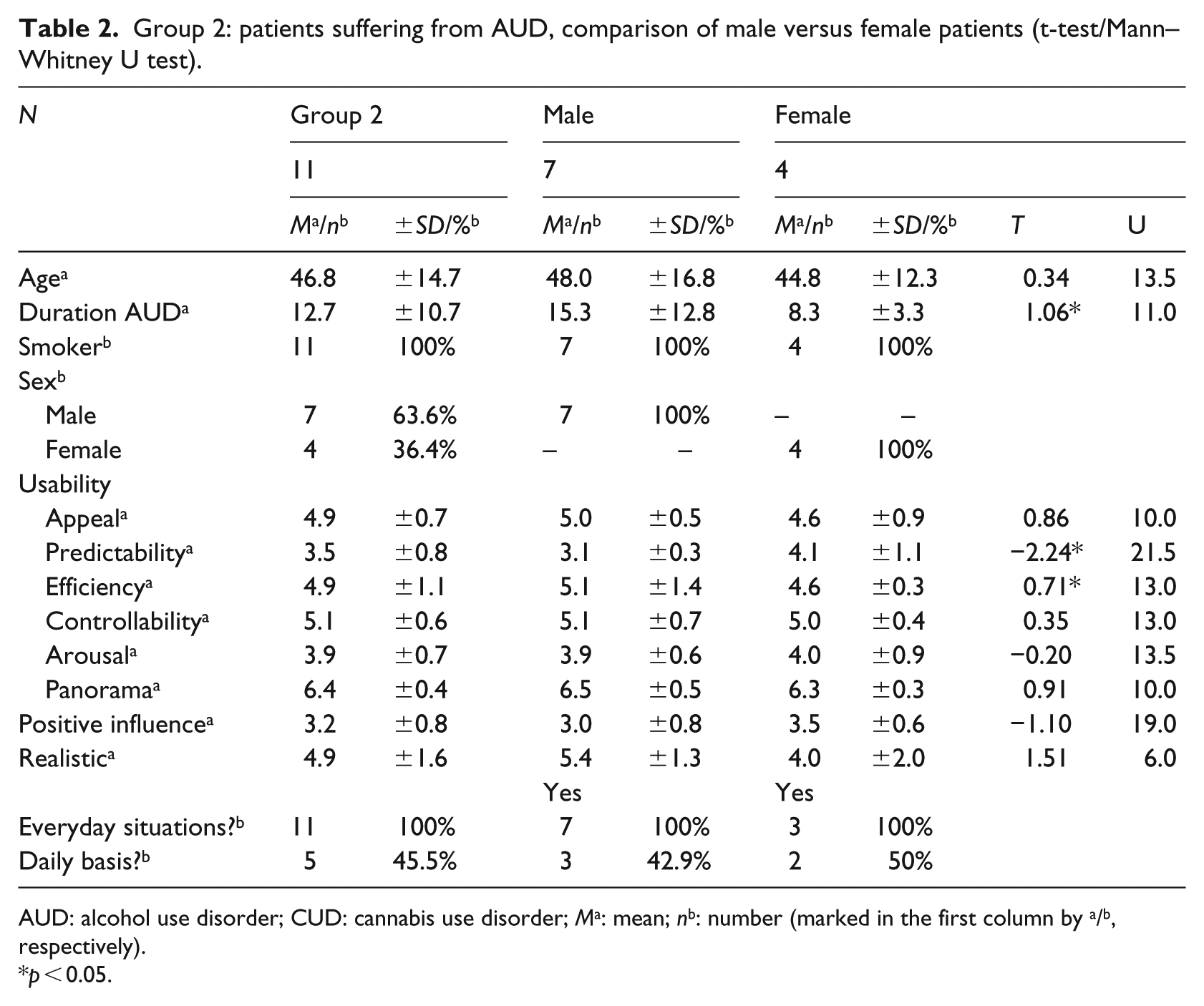
The overall ratings by Group 2 were very positive as well (see Table 2). The usability categories reached arithmetic averages of 4.86 ± 0.68 in appeal (i.e. mean rating of items 8, 10, 14, 15), 3.48 ± 0.79 in predictability (i.e. mean ratings of items 1, 2, 13), 4.95 ± 1.13 in efficiency (i.e. mean ratings of items 6, 9), 5.09 ± 0.62 in controllability (i.e. mean ratings of items 5, 7, 12), and 3.94 ± 0.73 in arousal (i.e. mean ratings of items 3, 4, 11). Regarding the panorama navigation, the arithmetic average of 6.41 ± 0.44 was reached (i.e. mean ratings of items 16 a and b). Surprisingly, the panorama control was even well accepted by patients who use a computer on not more than 1 day per week (N = 4, 6.38 ± 0.48), intriguingly representing almost one-third of the patients (36%). Likewise, 18 percent (N = 2) does not have any (“never”) or almost any (<1 day/week) experience with playing video games (for more details see Supplemental material). Nevertheless, half of the patients (N = 5) can imagine playing the game on a daily basis, and all patients stated that the game included everyday situations.
Group 2: patients suffering from AUD, comparison of male versus female patients (t-test/Mann–Whitney U test).
AUD: alcohol use disorder; CUD: cannabis use disorder; Ma: mean; nb: number (marked in the first column by a/b, respectively).
p < 0.05.
The game situation was seen as mostly realistic (4.91 ± 1.64), and the perceived influence of periodic training on the success of the treatment was positively evaluated (3.18 ± 0.75). Craving before did not differ significantly compared with craving after playing the serious game. However, descriptively a trend toward a reduced craving after using SALIENCE was revealed (AUQ: p = 0.086 one-sided; VAS: p = 0.056 one-sided). We hypothesize that it might have been possible to detect statistically significant differences if the patients would have played SALIENCE on a daily basis instead of playing it only once. Mean reaction times were 1762 ± 724 ms, ranging from 931 to 3079 ms.
Group comparisons
Group 2 rated the following aspects: appeal, predictability, and controllability, realistic and positive influence (p < 0.05) significantly lower than Group 1. However, the overall usability ratings were high and the game was also very well perceived in Group 2. No statistically significant differences were revealed for efficiency, arousal, and panorama.
Objectives and guiding questions for a feasibility study
For both groups, it became apparent that inclusion and exclusion criteria were chosen adequately, making it possible to recruit enough participants and performing the experiments in a timely manner (objectives 1 and 4). 28 In line with this, the study procedures and intervention were suitable for and acceptable to participants (see feasibility and usability results for both the groups). In addition, not one of the patients quit the game before finishing the tasks and due to the design of the game, it fits with the daily life activities of the patients, at least if they have access to a web browser (objectives 2 and 3). It was revealed that the game was very well received, participants understood the tasks, and they were not overstrained by game’s requirements (objectives 2 and 3). As discussed in one of the following sections, we are confident that the intervention is relevant to the intended population (objective 1).
Taking into account that Orsmond and Cohn 28 suggest an iterative process, performing a feasibility study, for Group 2, we included an “outcome measure” and also captured “craving” before and after playing the game (objective 2). Since craving is one of the diagnostic criteria of an AUD, frequently causing relapse, craving is a sensitive and very suitable measure in this context (objective 2). Finally, the preliminary analyses of the data suggest that the intervention is likely to be successful (considering the descriptive reduction of craving and the qualitative feedback of the participants; objective 5).
Discussion
This investigation was aimed at creating a web-based training game for the therapy of patients with AUD. As treatment settings regarding SUDs, such as AUD and CUD, have been changing to include shorter inpatient treatment times, the integration of technical approaches into standard treatment appears to be promising.
To the best of our knowledge, this is one of the first studies to combine CET with VR cues as a treatment approach in AUD, 29 without adding an aversive stimulation. 30 The major finding of this feasibility study is that the SALIENCE game was well accepted by patients. Usability ratings were high, and the game was evaluated as realistic. However, it remains to be determined whether there is a generalizable treatment effect of decreasing relapse rates, time to relapse, as well as drug-associated behavior such as drinking days and standard drinks following the training.
Several researchers have demonstrated that CET is effective with a medium effect for alcohol consumption outcomes when compared with treatment as usual, 31 as well as with relaxation/meditation treatments.32–34 Moreover, CET may be particularly effective in the long term, 35 favoring a long-term use to reduce heavy drinking days, 31 and relapse risks. 35 Nevertheless, there has also been some criticism that exposure-based substance use interventions may not be effective, since it may be difficult to generalize the learning from the therapeutic setting into real-world high-risk settings which are associated with the risk for relapse. 36 There are several phenomena following extinction that may contribute to this hypothesis. For example, it has been shown that an extinguished conditioned reaction may recover spontaneously. 37 In addition, the extinguished conditioned reaction may diminish following subsequent exposures to the unconditioned stimulus after extinction, a phenomenon which is called reinstatement. 38 Finally, the extinguished conditioned reaction may be renewed when the conditioned stimulus is presented in a context that is different from the extinction context. 39 To overcome these shortcomings, it was hypothesized to include retrieval cues (e.g. a neutral and novel stimulus) originally employed as a conditioned inhibitor, which could be presented after training to reduce spontaneous recovery in the original extinction training context. 6 Moreover, it has been highlighted that extinction learning about the drug-associated cues may be generalized from the therapy contexts to the more naturalistic “home” and high-risk setting. 36 Consequently, current behavioral therapies use CET facilitating learning and cognitive reinforcement of new behavior and suppress craving while adding VR elements to practice new skills and enhance the ecological validity and generalizability of this treatment. 10
Up to now, several studies assessed craving induced by substance-related stimuli in VR settings. Most of them were conducted in tobacco use disorder, demonstrating consistently that (1) VR increased craving for smoking-related compared with neutral cues, 10 (2) VR cues are superior in inducing craving over simple pictures, 40 and (3) craving might be induced in smokers but not in non-smokers. 41 Culbertson et al. 42 and Ryan et al. 43 were able to replicate these findings in methamphetamine users and in binge drinking college students.
As a next step, some researchers combined CET and VR in AUD 30 and tobacco use disorder (for review see 10 ). This approach was able to decrease alcohol craving after 10 sessions when paired with an aversive stimulation. 30 While some studies showed beneficial effects of VR in the context of CET for tobacco use disorder, 10 others did not detect a decrease in tobacco craving after treatment. 10
In addition, it has been shown that decision-making deficits are associated with substance consumption and relapse risk. 22 Therefore, we also added a decision-making training component to the SALIENCE game. The participants were confronted with VR alcohol cues they are used to from everyday life and then had to choose between an alcoholic and a non-alcoholic drink. At this point, the actual augmented CET started by presenting patients with familiar images from which the non-alcoholic beverages should be chosen. Recently, it has been demonstrated that a “simple” cognitive-bias modification (CBM) intervention improves treatment outcome in AUD. More specifically, patients were trained to make avoidance movements (pushing a joystick) in response to pictures of alcohol. 44 The same group replicated this preliminary finding in a further study comprising more patients. 24 Performing a randomized controlled trial, it was demonstrated that patients receiving CBM developed alcohol-avoidance behavior and reported significantly lower relapse rates at 1-year follow-ups, compared with patients receiving treatment as usual. 24 Intriguingly, moderation analyses revealed that older patients and patients with a strong approach bias at pretest benefited most from CBM. It appears that six training sessions may be sufficient, yet the authors stated that many patients might profit from continuing the training. 45 It has to be emphasized that only static pictures were used, and a relatively simple action task had to be performed in these studies.
To sum up, CET applications and their enhancement using VR cues may be suitable, easy, inexpensive, non-stigmatizing tools, which can be integrated into the patients’ everyday lives, even if they have an employment. At best, most applications are funny, realistic, and engaging. If this is achieved, it may be assumed that starting the training with SALIENCE in a clinic and continuing it in the naturalistic context will decrease the craving and relapse risk.
Limitations
A limitation of this study is its small sample size. Moreover, due to the fact that the study was designed as a feasibility study, we included both patients suffering from AUD and CUD despite the fact that the game was initially designed for AUD patients. This might have influenced the presented results. Nevertheless, our analyses did not reveal significant differences between both the groups concerning usability ratings. Further versions of the application will include much more stories and levels and players will be able to add personal content in terms of preferred drugs, individual high-risk situations, individual contexts, and risky interpersonal processes (by adding VR social interactions). As a consequence, the application will be independent of age, gender, race, and religion. In the actual pilot version of the software, we did not log the individual reaction times and choices. However, according to the experimenters’ perception, participants chose non-alcoholic beverages in more than 95 percent of the cases. In addition, it has to be highlighted that VR cues may also cause relapses during gaming because of the realistic scenarios, or may induce cyber sickness, including sensations of vertigo or nausea during or after VR exposure. 46
Outlook
Technological innovations for the treatment of substance use disorders must be simple, brief, and applicable across diverse substances and substance users. 6 Again, it has to be highlighted that the main challenge is to generalize the training effect and to prepare the patient for his confrontation in an outpatient setting. It may be noted that our approach represents a reasonable add-on to standard treatment since it is inexpensive and engaging. It can be used practically anywhere, at least as long as the patient has access to the Internet. For the future, an offline version or a mobile application may be created to increase accessibility and both seem to be reasonable objectives. Although interventions designed to reduce substance use via cue exposure have demonstrated little efficacy as stand-alone interventions, we suggest using them as an add-on to the usual treatment. Because of its simple structure, new content, for example, trainings with regard to other SUDs, “patient-specific” situations, as well as other substances of abuse such as cannabis can be implemented easily with our SALIENCE software. Editable photos, stories, and even avatars can be used to facilitate a personalized and state-dependent treatment. Furthermore, implementing more and different environments may be useful to avoid a renewal effect and facilitate the generalization of extinction responses. 11 Apart from the addition of avatars, it is also conceivable to augment VR cues by implementing other sensory qualities such as auditory stimuli.
Supplemental Material
Supplementary_Material_(1) – Supplemental material for The training game SALIENCE for the therapy of alcohol use disorder
Supplemental material, Supplementary_Material_(1) for The training game SALIENCE for the therapy of alcohol use disorder by Sabine Vollstädt-Klein, Philip Mildner, Jan Malte Bumb, Damian Karl, Christoph Ueberle, Yury Shevchenko, Falk Kiefer and Wolfgang Effelsberg in Health Informatics Journal
Footnotes
Acknowledgements
The authors thank Yury Shevchenko and Thomas Wiegand for their valuable contributions to the design and implementation of SALIENCE and Sarah Gerhardt for her assistance in the data collection. They also thank Fabian Thalmann for the recruitment and assessment of participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.