
Abstract
Many studies have highlighted the patient safety risks in intravenous medication administration, and various technological solutions have been proposed to mitigate those risks, including ‘smart pumps’ and closed-loop systems. Few studies describe these implementations in detail. In this article, we report on a sociotechnical investigation of a closed-loop documentation system linked with smart pumps for intravenous infusion administration on an intensive care unit. The smart pumps are ‘mapped’ to an electronic prescribing and medication administration system, allowing infusion rates, volumes and boluses of intravenous medication to be monitored in real time. Ethnographic observations were conducted over 37 h, including direct observation of infusion administration (n = 23 infusions), discussions with clinical staff and semi-structured interviews with intensive care unit managers (n = 2). Analysis was based on the Distributed Cognition for Teamwork (DiCoT) method to understand how information is processed across individuals, teams and technologies. We report on how the system works in context, and identify contributions and compromises to patient safety with new risks that need to be managed at bedside and intensive care unit level.
Introduction
Intravenous (IV) medication administration errors have been widely recognized as a threat to patient safety. 1 Various technological solutions have been proposed to reduce IV medication administration errors, one of the most widely reported being ‘smart’ IV pumps which incorporate a drug library and dose error reduction software 2 to prevent the administration of medications when the dose is outside a predetermined safe range. Other advances to reduce errors in patient identification, communication and transcribing include electronic prescribing (sometimes called computerized provider order entry systems), electronic prescribing and medication administration (EPMA) systems and more advanced systems where several systems (e.g. EPMA systems and infusion pumps) are interoperable and information transferred automatically between them. While these new developments bring potential benefits in patient safety, they introduce new patterns of working, in terms of interactions among hardware, software and ‘people-ware’, 3 that also have an impact on patient safety. Few previous studies have explored the details of the implementation of such systems and how they shape behaviour and consequent safety.
One technological variant that lacks detailed study is a closed-loop documentation system linking smart pumps and EPMA on medication administration. This is intended to improve patient safety through real-time, accurate documentation of what medications a patient is receiving. This is potentially important in clinical contexts where medications are intentionally written to permit variability in medication administrations and to enable nurses to respond to changes in the clinical status of critically ill patients (e.g. in an intensive care unit (ICU)). This contrasts with practices in most other clinical contexts where the medication order defines a specific medication regimen. This difference in clinical practice reflects the particular needs of ICU patients, but brings with it particular safety risks, particularly around maintaining an accurate record of what has been administered so as to inform future medication administration decisions, which the closed-loop system was intended to mitigate.
Our objective was to gain an in-depth understanding of the patterns of working that had evolved in an ICU where a closed-loop IV medication administration documentation system had been implemented and of the consequent effects on patient safety.
Background
This study took place within the context of a larger study investigating patient safety in IV medication administration and the role of technology design and deployment. The larger study comprised two main sub-studies: a point prevalence study across 3–5 clinical areas in 16 hospitals, adapted from the initial design applied by Husch et al. 1 and a set of in-depth observational studies on two clinical areas in five of the participating hospitals, selected to focus on areas of particular interest. 4 Previous articles from this larger study have focused on general findings across all participating hospitals;5,6 this is the first to report on the detailed findings from one clinical setting. The observational study in an ICU in which a closed-loop documentation system had been implemented was selected for in-depth reporting because it exploits a particular innovative technology (closed-loop documentation) that is not yet widely used in UK hospitals and for which there are no detailed studies from a safety or informatics perspective.
Next, we briefly review prior work on patient safety related to medication administration in ICU, the implementation of closed-loop systems supporting IV medication administration and background on Distributed Cognition for Teamwork (DiCoT), which is the theory-based methodology applied in this study.
Patient safety relating to medication administration in ICU
Few previous studies of patient safety relating to IV medication administration in ICUs have been reported, and most previous studies have taken a quantitative approach to assessing error rates; for example, Calabrese et al. 7 conducted a point prevalence study focusing on IV medication administration errors in five ICUs in the United States. In common with other point prevalence studies that have reported on multiple clinical areas,1,5,8 the focus is on quantification of errors and harm, and the details of system implementations in different areas and at different sites are not discussed.
Rothschild et al. 9 report on a prospective, randomized time-series trial, in which ‘smart’ features were turned on or off for standalone pumps for IV medication administrations across 744 admissions in an ICU, but found no significant difference in the medication error rates across the two conditions. They attribute this, in part, to poor compliance and note that ‘although smart pumps have great promise, technological and nursing behavioral factors must be addressed if these pumps are to achieve their potential for improving medication safety’. The details of the system implementation and the ways it was used are well described, as are the interventions that were proposed following this study; these included education, changing the pump configurations and similar. However, nursing behaviours were only described at a high level (e.g. bypassing the drug library), with no account of the causal factors that shape those behaviours.
Two descriptive approaches have been applied to understand aspects of medication work in ICUs: the Systems Engineering Initiative for Patient Safety (SEIPS) and DiCoT. Carayon 10 presents the SEIPS approach to analysing healthcare quality and patient safety from a sociotechnical perspective and summarizes various studies that have applied the SEIPS approach in ICUs. These studies focus on proactive risk assessment, particularly around medication administration, and on identifying performance obstacles experienced by ICU nurses that have an impact on the quality of care delivery. Rajkomar and Blandford 11 applied a Distributed Cognition (DCog) approach (DiCoT, as summarized below) to describe activities in an ICU including, but not limited to, IV medication administration. These approaches have not yet been used to study closed-loop system implementations, which is our focus here.
Closed-loop systems
As noted above, closed-loop systems that automate steps in the complex process of medication delivery 12 have the potential to improve patient safety by removing some potentially error-prone steps in the process.13,14 Types of closed-loop systems for medication administration include the following:
Control systems where a controller monitors one or more patient variables and automatically adjusts medication delivery based on predefined rules and algorithms. 15 Examples include glucose control, 16 perioperative fluid administration control 15 and hypnosis and sedation control.17–19
Medicines administration systems involving technologies to confirm the identity of the patient and/or medication and that this matches what was prescribed. These can include EPMA, barcode medication administration, infusion pumps and automated dispensing cabinets.20,21,12 In some cases, the infusion pump receives programming information from the EPMA system; the nurse’s role is then to check these details and start the infusion, rather than programming the pump manually.
Supply systems feeding back information to stock control and procurement systems, ensuring that adequate supplies are maintained without needing to manually monitor and enter these data.
Documentation systems that automate steps in the documentation of administration; for example, details of the infusion pump’s rate, volume and any bolus doses are ‘mapped’ to a drug in the patient’s record on the EPMA system, so that nurses do not need to manually enter these data after administration.
The study reported here focuses on the last of these types of system, which is particularly well suited to ICUs where medication administration can change without necessarily requiring a change in the medication order.
DCog and DiCoT
Given the nature of the system being studied, which replaces manual communication between clinicians and the patient record by automated communication, we adopted an approach that focuses on the processing of information across individuals, teams and technologies – namely, DCog. In particular, we adopted the DiCoT approach to data gathering and analysis.
DCog22,23 has been widely used in healthcare to understand the work of distributed teams and how technology design shapes that work. It is a theory that accounts for the way that information flows around a system and is shared and transformed in the process of doing work. DiCoT24,25 was developed as a method of applying DCog theory in practice, focusing principally on team working and how the design and configuration of artefacts support work.
Conducting a DiCoT analysis involves four main phases, which are interleaved and iterative:
Data gathering (observation and interviews, shaped by the analyst’s goals);
Model construction (based on the models outlined below);
Application of the DCog principles to the models;
Reasoning about implications (for design and deployment, for understanding work etc.).
The first models that are commonly developed are information flow model, models of artefacts and models of physical configuration. The information flow model captures the important information flows between actors in the system, where an actor can be an individual, an artefact or a group that acts together to perform a function. The information flow is shaped by the designs of artefacts and the physical configuration of the system. Together, these three kinds of models represent how information is distributed materially.
Further models can be added to analyse how information is distributed temporally and socially. Two further models are presented in the analysis below: an evolutionary model shows how technology use evolves over time (including likely evolution into the future), while a social structures model shows how social structures align with the goals and structures of the ‘work’ of the sociotechnical system.
Each model represents a different perspective on the work being studied. A collection of DCog principles, with prompts, are associated with the models.24,25 For example, the DCog principle that information moves around a system prompts questions such as, ‘How does particular information move?’ and ‘Are there risks of communication breakdown (e.g. due to poor communication bandwidth, diverted attention, or misinterpretation)?’. Similarly, the DCog principle that spatial representations can support cognition prompts questions about the quality of the mapping between spatial layout and cognitive structures. Further examples are included in the analysis presented below.
Methods
Study design
We conducted in-depth qualitative observations and interviews to investigate infusion administration and documentation practices, focusing on a closed-loop documentation system in an ICU setting. The study was approved by National Health Service (NHS) Research Ethics Committee (10/H0715/13).
Study setting
The ICU was part of a district general hospital in England. The unit had 12 beds and about 750 admissions a year. There was generally one nurse per patient, and doctors were routinely present. The unit had smart infusion pumps, that is, both volumetric pumps and syringe drivers had a drug library for different drug profiles. These pumps sent data to an ICU-specific EPMA system, which monitored and recorded in real time which drugs were being given, at what volume and what rate.
Data collection
Observations focused on infusion administration and documentation and how these activities were embedded in and influenced by the wider ICU context. Preparation was also observed where possible. Infusions via volumetric pumps, syringe drivers and patient controlled analgesia (PCA) pumps were observed. Manual bolus doses were also included. Written consent to observe on the ward was provided by the ward manager, and staff were asked for informed verbal consent before observations. Patients were not asked for individual informed consent because their behaviour in itself was not the focus of the study, but were verbally asked for permission to observe their treatment where appropriate. Data collection included the following:
Observations of infusion administrations, plus their preparation where possible;
Observing the general ebb and flow of ICU work;
Talking to staff on the unit between infusions and other tasks;
Two semi-structured interviews with ICU staff that focused on infusion practice in the context of ICU. An interview with an ICU consultant was planned and conducted prior to the observations to help familiarize the observer to the unit’s activities. An interview with a matron was conducted towards the end of the observations to help reflect on the emerging findings.
DiCoT themes and principles informed data collection. The first author (D.F.), who has expertise in fieldwork and DCog, collected all data and kept extensive field notes of the context, observations and interviews.
As part of the wider study, 4 a further eight interviews with managerial staff and five interviews with patients in ICU were conducted. These added to the general picture of infusion administration at the trust, but were excluded from the focus of the current analysis.
Data analysis
Field notes were transcribed and coded by D.F. Interviews were transcribed and anonymized. Data were coded deductively against the five DiCoT models and associated principles outlined above. NVivo 11 qualitative data analysis software was used to aid this process. The DiCoT models and principles provided focus for developing narratives and diagrams to describe how information is transformed and propagated around IV infusion administration on the ICU; issues and strengths of the current system configuration were also noted.
Results
Observations were conducted for a total of 37 h on the unit, over 5 days in September 2017 and October 2017. This included 23 direct observations of infusion administration. In this section, we present our findings from the five DiCoT models outlined above: artefact, information flow, social structures, physical layout and evolution (of systems and practices).
Findings from the artefact model
Different tools and artefacts were brought into coordination to perform infusion administration, from drugs, needles and tubing to labels and stickers, trays and trolleys. We focus on three central artefacts involved in the EPMA/smart pump system.
Smart pump and docking station
Smart pumps have a drug library. Along with having hard and soft limits for different drugs, this library also specifies bolus limits for certain drugs. This is meant to enhance safety, for example, if a drug is mis-programmed the pump will prevent or alert the user to the error. The drug library on the ICU was relatively small, so not all drugs had a corresponding entry. The drug library was also outdated and introduced some hazards. For example, propofol is provided at a concentration of 10 mg/mL and displayed as milligrams per hour on the smart pump. However, nurses are used to dealing with infusion rates expressed as mL per hour; this is what is displayed in the infusion pumps for all drugs except propofol. So, if nurses want 10 mL per hour the pump should display 100 and not 10. Due to problems in updating the drug library, nurses were therefore asked not to use the propofol entry to reduce the potential for error. Both of these issues (missing and non-standard drug library entries) meant that nurses could not consistently rely on the smart features of the pump when programming it, creating scope for error. Conversely, nurses remarked that when a drug library entry is used the pump displays the name of the drug, making it easier to spot when dealing with multiple pumps and reducing the likelihood of adjusting the wrong pump when changing medication parameters.
At a larger scale, one patient may require multiple volumetric pumps and syringe drivers. Docking stations can house up to eight pumps. This keeps the pumps organized, provides them with power rather than having lots of individual power supplies and has the hardwire link to the EPMA mapping technology (the ‘closed-loop’) connected to it. However, patients on more than 8 pumps do not have all of their pumps mapped, so the administration has to be recorded manually. Some nurses reported plugs having bent pins where they have been disconnected and reconnected, so the docking station can no longer physically connect to the EPMA. While the closed-loop technology improves patient safety by automatically recording medication administrations to the EPMA for up to eight pumps (if the docking station is functioning correctly), there is a higher variability in workload where some medications are and are not mapped and a risk that nurses overlook doing manual recording in the cases where it is required. We return to the theme of mapping and recording when discussing information flow below.
EPMA system by the bedside
Each ICU bed had a computer beside it through which the EPMA system could be accessed. The EPMA system drew issues to the nurse’s attention in two main ways. Red was used to highlight where doctors had recently changed the medication order – useful when doctors (anecdotally) change medication orders without telling the nurses. Nurses also had to acknowledge each individual change before proceeding to another task, to ensure these were not overlooked. Yellow was used to highlight administration details that did not correspond to the medication order or that were outside safe parameters – similar to the soft limits of the smart pumps (except that the EPMA system cannot control the pump, so there was no alert at the pump’s interface).
The matron reported that in the future the EPMA system could do more intelligent automated checks. The matron referred to two near misses where piperacillin/tazobactam had been prescribed to a patient with a penicillin allergy, but the nurses caught the prescribing error before administering it using their own expertise and safety checks. It is thought that the prescribing error was at least partly due to the penicillin being prescribed by brand name (Tazocin) which reduced its salience as a penicillin. The EPMA system was due an upgrade to include more advanced decision support, for example, checking if a medication order conflicts with a patient’s known allergies. This external support should help protect patients and nurses downstream from prescribing errors and make the system less reliant on individuals’ memory and situation awareness.
Nurses were also able to access a workplan tab on the EPMA system that gave them a chronological list of tasks that needed to be completed. This had potential to reduce dose omissions (compared to lengthy paper medication charts that are divided into multiple sections which can make finding the next dose to give more challenging). 27 Also, an electronic infusion guide could be accessed within a few clicks on the computer system, switching from the EPMA system to the intranet, if information on how to administer drugs was required; this gave nurses quick access to information that could contribute to patient safety.
EPMA system in the doctors’ central hub
The main place to access the EPMA away from the bedside was the doctors’ central hub, which had a number of desktop computers for doctors to access as well as a large screen giving an overview of ICU and patient status (Figure 1). For each bed number, there was a structured display showing patient details and patient status, for example, Figure 2 shows the extent and length of IV access, whether the patient was ventilated and on inotropes and their status in relation to the FAST HUG mnemonic (Feeding, Analgesia, Sedation, Thromboembolic prophylaxis, Head-of-bed elevation, stress Ulcer prevention and Glucose control). This shared artefact provided a method to improve the situation awareness of health care practitioners in the unit. The main overview screen could also be used to display scans and graphs so that medical staff could discuss them collectively. Both of these displays have the potential to improve patient safety through situation awareness and shared understanding.
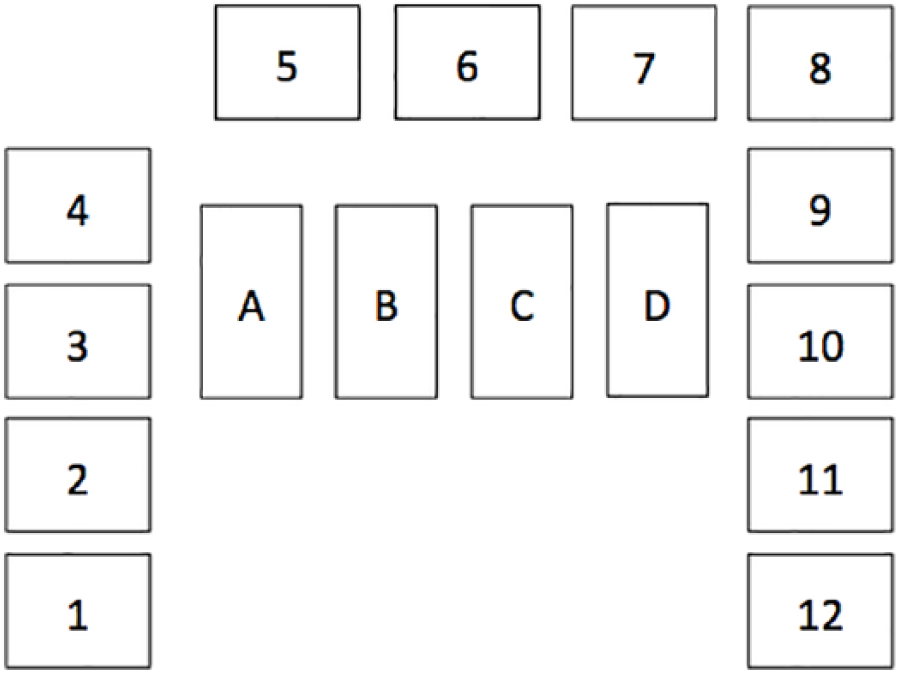
Schematic of the overview screen showing beds 1–12. Boxes A to D: (A) bed occupancy out of 12, (B) how many patients are ventilated out of 12, (C) how many patients are isolated due to infection control out of 12 and (D) patients on antibiotics out of 12.
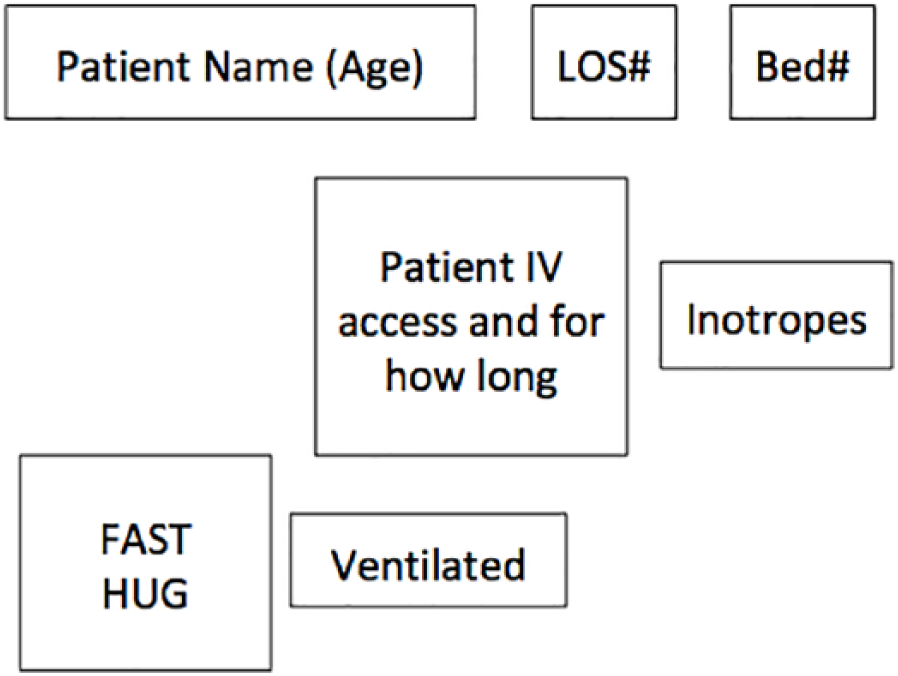
Schematic of patient information in main overview screen showing name and age, length of stay (LOS), bed number and icons to do with patient status. The colour of the border indicates how many organs are receiving artificial support, that is, black for no support, amber for a single intervention and red for multiple interventions.
These artefacts, central to information flow, are described next.
Findings from the information flow model
The ICU receives patients in a critical state; this has implications for information processing on the unit:
Sensemaking is critical. Patients’ prognoses may be uncertain, meaning that doctors must stabilize the patient, monitor their trajectory so as to be alert to further issues that need to be investigated and make rational interventions based on developing hypotheses about the patient’s condition.
Timeframes are tight. Patients’ conditions change over minutes and hours, meaning short timeframes for diagnosing, monitoring and responding to treatment.
Close coordination is needed. Doctors and nurses have close cycles of coordination to aid timely feedback and action in this complex environment.
Two important information processing activities that contribute to patient safety are facilitated by the closed-loop documentation system; these are doctors’ sensemaking and nurses administering drugs and fluids.
Doctors’ sensemaking
The doctors’ handover from the nightshift happens at about 8:00 am at the central doctors’ hub. The large overview screen (Figures 1 and 2) immediately gives a summary of the status of the ward and the patients within it, enhancing their situation awareness on the unit. A doctor from the nightshift summarizes the night’s events as they discuss each patient in turn, and the lead consultant for the day shift makes an initial plan for the day with input from the other doctors. Blue slips of paper that summarize the plan for each patient are completed. These slips are given to the nurses to provide instructions before the main doctors’ ward round at about 10:30 am, which enhances team coordination.
Doctors have electronic access to patient records, vital signs and drug administration records while discussing each patient in the central doctors’ hub. Drug administration records are particularly important because nurses titrate drugs to keep the patient stable, so patient vital signs may appear stable but increasing and decreasing doses can indicate changing patient conditions; that is, stable patient vital signs might be a false indicator.
The ability for doctors to monitor drug administration, blood tests and vital signs away from the bedside made spotting trends easier over different periods of time. For example, the computer system enabled doctors to track trends in drug administrations and vital signs side by side and work out the fluid balance of the patient. However, doctors learned, and needed to be mindful of what could and could not be trusted. For example, nurses would use their common sense to omit outliers from patient records when documenting results manually, but the computer system would just record measures without this filtering process so a patient yawning or being moved at the time a measurement was taken could lead to a spurious measure being recorded. The computer system also did not allow for fluid being lost through breathing and sweat in its calculations, which could also lead to spurious results and inappropriate interventions if this was not known. Doctors were also mindful that administration records might be inaccurate for reasons explained below. They must internally compensate for the limitations of the extra external support. Doctors need to be trained in, and mindful of, all these sources of variability and unreliable data to ensure that patients are treated safely.
Nurses administering drugs and fluids
Drugs were standardized so that the variety to be prescribed and administered is reduced. Doctors reported being able to prescribe an ‘admission order set’ in a few clicks on the computer system so that common drugs were prescribed to the patient on admission to the unit. Doctors would also give ‘mission goals’ to nurses (e.g. get blood pressure up to X using these drugs) so that nurses could act flexibly and autonomously. This flexibility meant that an accurate record of the administration was critical.
The process of administration was facilitated by the EPMA system, for example, through the red and yellow highlighting previously described. The nurse would then collect the materials and drugs needed for the administration, get a double check from a colleague and administer the drug. If the smart pump had an appropriate drug library entry used correctly, additional external checks were introduced by that.
When the nurse sets up an infusion, they also need to ‘map’ the pump to the patient’s EPMA record so that the rate can be documented against the relevant drug. As noted above, pumps are placed in a docking station that is linked to the EPMA system. If the pumps are mapped to the patient’s EPMA record correctly, the EPMA system monitors what the pumps are doing in terms of the rate, volume and any bolus doses. It will highlight alerts on-screen in yellow if a drug is being infused too quickly or slowly, or does not match a drug on the electronic medication for that patient. As noted above, the mapping made recording medication administration easier for nurses; for example, in manual systems, nurses have to record the infused volume for each pump and reset their counters every hour or at 00:00 each day. 11 Manual medication boluses and fast infusions that are not mapped could be recorded by ticking a box on the EPMA system to record their administration.
The mapping process does not always work as intended. For example, one nurse reported that a nurse on the previous shift had changed a drug in a pump but did not change the mapping, so the patient was receiving the correct drug, but the EPMA system was recording that rate and volume on the patient’s record as a different drug. Sometimes, the software did not work, for example, there was an ICU-wide mapping problem during the observation period that was caused by the need to upgrade the Windows operating system. Also, sometimes the mapping function was unintentionally forgotten or intentionally not used, for example, a nurse might prefer to tick a box for a fast infusion to record it has been administered rather than map it for such a short period of time. These oversights, technology failures and workarounds all compromise patient safety in situations where the mapping function is relied on.
Findings from the social structures model
In practice, many different professionals contributed to the work of the unit, including medical staff, nurses, cleaners, receptionists, research nurses, pharmacists, porters and physiotherapists. Different networks of staff organized around different functions, collectively these contribute to patient safety on the unit. We highlight three examples below (see Figure 3):
Direct care team network. We have already referred to the close coordination between medical and nursing staff and the flexibility of nurses in trying to accomplish ‘mission goals’.
EPMA technical support network. The closed-loop documentation system is supported by an onsite technician who troubleshoots technical issues and maintains the system. Offsite support for more challenging issues was provided by a remote technical team. These support structures were essential for maintaining the functionality of the system, enabling it to contribute to patient safety. More informally, an ICU consultant contributed to resolving a problem with the EPMA system, which required all the bedside computers to be restarted to receive a major operating system update to resolve the issue.
Nursing safety management network. One function of this network was to manage safety reporting and learning. Senior nurses would write reports on incidents and near misses, with learning filtered to nurses and other staff on the ICU. The matron supported this process and would need to report up to board level at the trust.
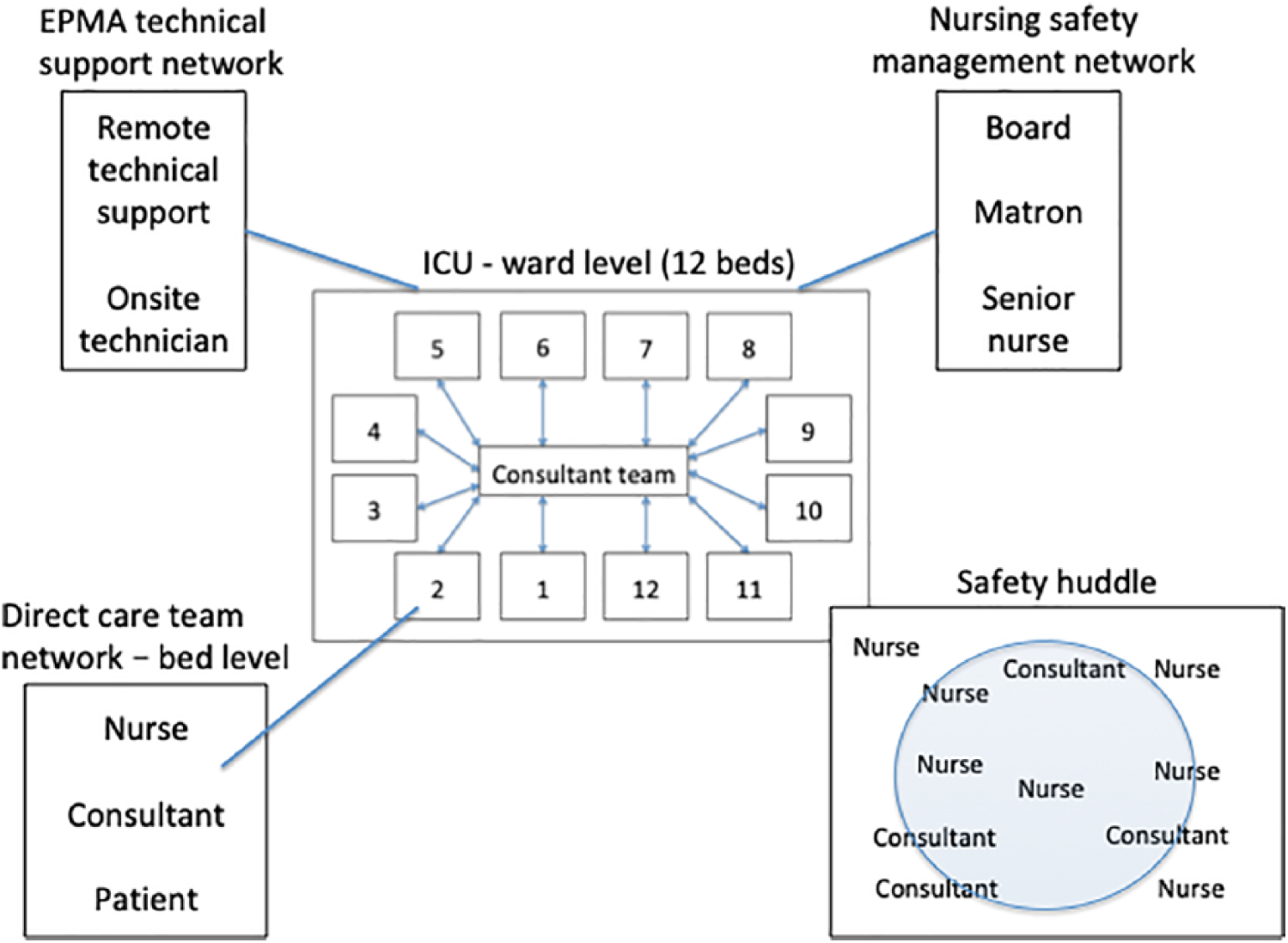
Schematic of different social structures involved in patient safety in ICU.
At a higher level of abstraction, not related exclusively to the closed-loop system, the unit had introduced safety huddles that brought together doctors and nurses to talk about demand and capacity on the unit, incidents, near misses and any other issues pertinent to the safety and performance of the group (see Figure 3). In one observation someone alerted the group to a warning issued by pharmacy who could not track a batch of gentamicin in the hospital that could increase the chance of an allergic reaction when administered to patients due to a manufacturing issue. Some staff on the ICU had previously been aware of this while others had not. In the discussion, they highlighted patients who could be vulnerable to this issue to ensure that their safety was not compromised.
Findings from the physical layout model
We present the physical layout of the ICU first in terms of overall layout and then in terms of the layout of key areas (a patient bay and the central doctors’ hub).
ICU layout
Figure 4 shows the layout of the ward. It has two wings with a reception and a central doctors’ hub area in the middle. Beds at the extremities of the ward are some distance from the central hub area, which makes access to live information discussed in the central hub (Figure 6) more important. The two medication areas hold stocks of drugs and medical equipment; however, they contain different drugs and equipment and so gathering materials for medication administration can involve nurses going back and forth. This absorbs time that might otherwise be spent on direct patient care.
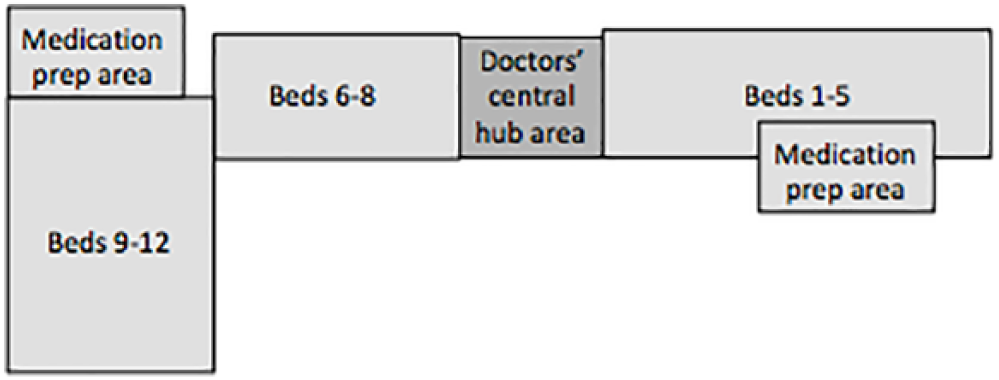
Physical layout of the ward.
Patient bay layout
Figure 5 shows a typical layout of a patient bay. The trolley, table and EPMA system table are used as surfaces for infusion preparation. Space around the bed was limited for infusion administration, especially where extra pumps go beyond a single docking station – meaning more standalone individual pumps or an additional docking station. This could make it difficult for clinical staff to access all resources in a streamlined way, distracting them from direct patient care.
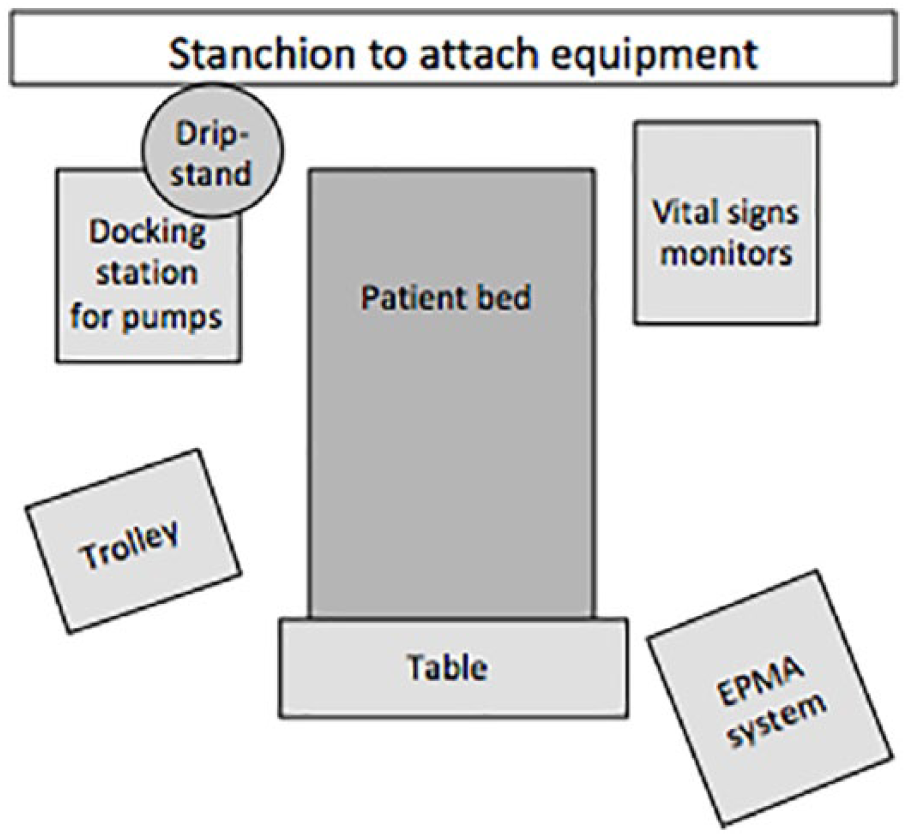
Typical layout of a patient bay.
Central doctors’ hub
Figure 6 shows the layout of the central doctors’ hub. This has four desktop computers at the centre where doctors can sit and access patient records and the EPMA system. The overview screen provides a summary of the ward’s and patients’ statuses, and it can also be used as a shared screen to discuss graphs and scans together. There are two vital sign monitors away from the desk for all patients on the ward. If an alarm goes off, doctors can make an initial assessment about its importance and urgency from where they are sat by looking at the vital sign monitors to see what is going on, viewing overview information on the big screen and accessing patient records and the EPMA system if necessary. This enables an informed response, rather than running down the corridor to every alarm or ignoring potentially important events, which has an impact on patient safety.
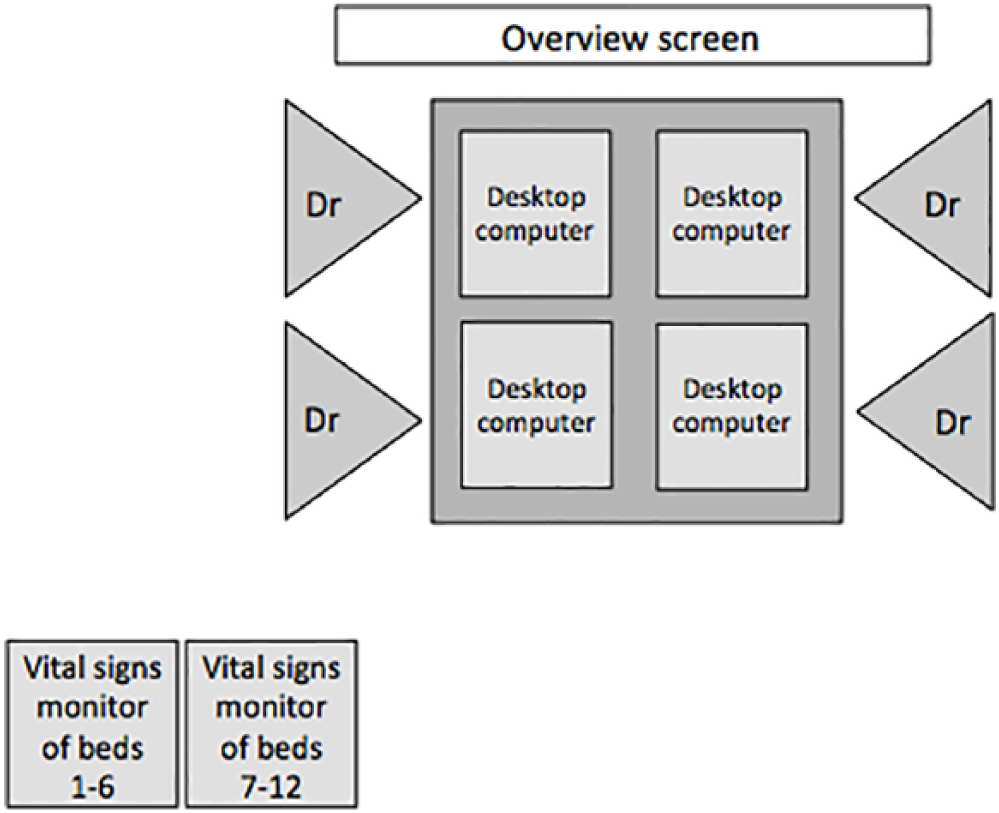
Schematic of central doctors’ hub area. Four doctors can sit at desktop computers, with a shared overview screen and vital sign monitors slightly away from the main desk.
Findings from the evolutionary model
The smart infusion pumps had been in place for about 10 years on the unit, and we have already described how the drug libraries had become outdated. The matron stressed that updating the library needed to be easier because medication practices change, and there can be problems with supply that alter the way drugs are given. Drug libraries need to be adaptable to these changes. The matron questioned the ongoing contribution of the dated drug libraries, especially as the EPMA system has the ability to draw nurses’ attention to administration discrepancies in real time. Also, future advances in the EPMA’s pharmacological intelligence and its access to more information (compared to standalone smart pumps) could facilitate more sophisticated checks at the medication and administration stages, for example, drug limits could vary based on weight, age, fluid balance figures, glucose levels and other clinical markers.
The EPMA system had been on the unit for about 5 years. The smart pumps were compatible with the linked EPMA system. Some nurses commented that their math skills were used less due to the dose calculation support of the EPMA system, so it might deskill nurses in the longer term. The matron was also keen to test that nurses had not become over reliant on it in an emergency. The EPMA system was due a major upgrade that would provide more advanced pharmacological intelligence and error checking. While the systems were taken offline for the upgrade, the matron was planning a surprise exercise to test how staff would cope if the system failed. Back-up systems would print EPMA information to be used at the bedside, which staff had been trained on, but this opportunity would test the unit’s resilience if the EPMA system failed. Here, the matron is anticipating and responding to patient safety risks evolving over long periods of time (i.e. months and years, rather than days and weeks).
Discussion
The design of informatics on ICU impacts patient safety. Furthermore, novel technologies afford new ways to gather, process and represent information that changes the landscape of what can be automated and achieved. This is the first sociotechnical analysis of a closed-loop documentation system for IV infusion administration on ICU, which has revealed contributions and compromises to patient safety. It is likely that every ICU has different technology support, so this is one example from a range of possibilities. For example, there are marked differences from the description of IV infusion administration on ICU described by Rajkomar and Blandford, 11 arising specifically from the closed-loop documentation system:
Nurses did not have to go through the laborious process of recording the volume infused into the EPMA system and resetting infusion pump volume counters every hour;
The EPMA system can draw nurses’ attention to infusion discrepancies that either do not match a medication order or are being administered outside expected parameter values in real time;
Doctors can monitor drug administration data against patient vital signs in real time.
Observations of these technologies enhance understanding of how they do (and do not) improve patient safety. For example, we have referred to the effects on doctors’ sensemaking and situational awareness, which is critical to patient care. Further, nurses’ thinking and productivity are augmented through dose calculations, easy access to an IV medication guide, guided attention through red and yellow highlighting and efficiency gains through not having to record and reset infusion volume counters every hour (which gives nurses more time for other aspects of patient care). Overall, where other types of closed-loop systems attempt to reduce error by taking the human thinking out of the loop, this closed-loop system augments the cognitive tasks across individuals, teams and technology on the unit.
However, these new practices also introduce new risks that require awareness and management. For example, doctors are mindful that they cannot always trust what the computer system says, and nurses are mindful of error-inducing structures that they need to work around in some instances, for example, not using the propofol entry in the smart pump drug library. The matron was mindful that there needed to be effective back-up plans in place should the computer systems fail, which could be tested.
Going beyond quantitative studies that focus on the frequency and prevalence of IV infusion error,1,8 this detailed qualitative analysis highlights opportunities to further evolve the design and configuration of these systems. Examples include changing the name for piperacillin/tazobactam and/or doing automatic allergy checks on the EPMA system, having functionality for pharmacy to design a just-in-time alert for certain drugs (e.g. so that a message could be given to all staff prescribing and administering gentamycin as they use the system, rather than issuing a memo that reaches some people and not others) and streamlining access to the IV infusion guide so that one click in the EPMA system opens the right page in the guide, rather than switching manually between the EPMA and the intranet. This semi-structured analysis based on DiCoT has helped to focus attention on incremental design ideas such as these. 26
DiCoT also helps to move from analysis to consider more revolutionary design ideas. 26 For example, much of the current literature is focused on evaluating the relative contribution of smart pumps to IV infusion safety. 9 However, this study challenges the model of putting more intelligence into the pumps. For ICU, where there is always a computer by the bedside, traditional (rather than smart) pumps mapped to a smart EPMA system on the bedside computer might deliver a better solution in terms of providing real-time alerts and allowing updates to be more easily managed.
Strengths and weaknesses
We have studied a specific closed-loop documentation system, which involves particular configurations of an EPMA system and smart pump technology. A strength of this study is that it explores the realities of a system used in practice. However, this might also limit its generalizability because the observations are grounded in the details of this particular context and system set up. Further research might encounter different ways these systems work together, including the EPMA system initiating hard stops for pumps similar to breaching a hard limit on a smart pump.
The system comprises an EPMA system, smart pump technology and the link between the two; some issues and insights might relate to standalone systems, rather than how they work together. For example, the closed-loop documentation system helps nurses keep track of fluctuating infusions and boluses without manually recording infusion volumes, but highlighting changes to medications for nurses might be applicable to standalone EPMA systems. This study has focused on an implementation of the system in ICU; the technology might address the requirements of other areas of the hospital less well.
Conclusion
Informatics in critical care continues to evolve and can contribute to (or compromise) patient safety in new ways. The technical potential and feasibility of advanced informatics systems are only part of the story; the sociotechnical implications also have to be investigated across individuals, teams and technologies. By describing how the system is configured and embedded in ICU IV infusion practice, we have identified a number of benefits that are specific to the closed-loop documentation system, as well as evidence of how it helps enhance properties of DCog for staff on ICU. However, the study has also highlighted ways in which these new ways of working bring new issues and vulnerabilities that need to be managed. By taking a particular instantiation of technology and social practices, this study has highlighted the importance of such details and demonstrated one approach (based on DiCoT) to reasoning about details at different levels of abstraction.
Footnotes
Acknowledgements
The authors thank the NHS staff who contributed to the study, and the critical care research staff who helped organise access and data collection.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work is supported by the National Institute for Health Research (NIHR) grant [12/209/27], from the Health Services and Delivery Research (HS&DR) stream. This research is also supported by the NIHR Imperial Patient Safety Translational Research Centre. The views expressed are those of the authors and not necessarily those of the NHS, the NIHR or the Department of Health.