
Abstract
Despite the growing attention of researchers, healthcare managers and policy makers, data gathering and information management practices are largely untheorized areas. In this work are presented and discussed some early-stage conceptualizations: patient-generated health data, observations of daily living, quantified self and personal health information management. As I shall try to demonstrate, these labels are not neutral; rather, they underpin quite different perspectives with respect to health, patient–doctor relationship and the status of data.
Keywords
Introduction
Health data production, interpretation and use have been traditionally restricted to healthcare professionals, with some notable exceptions (e.g. type 1 diabetes). The diffusion of miniaturized and easy-to-use measuring devices and the availability of consumer health applications allow patients (and laypeople) to become health information ‘prosumers’ (producer–consumer). The increasing availability of personal health information, however, depends on patients’ willingness to engage in data gathering, storing, sharing and interpreting. I shall refer to these activities as ‘patient data work’. The most notable form of patient data work goes under the label of ‘self-tracking’, defined as ‘the practice of gathering data about oneself on a regular basis and then recording and analysing the data to produce statistics and other data (such as images) relating to regular habits, behaviours and feelings’. 1 Depending on the purpose and the main beneficiaries of patient data, different modes of self-tracking have been identified.2,3
Despite the great interest, though, patient data work is still insufficiently theorized. The conceptual landscape is confused both because there are several competing labels that aim at describing patient data and because these are often used interchangeably despite their different original meanings. The purpose of this work is to present and discuss some conceptualizations that are gaining momentum in the academic debate and the policymakers’ discourses, reconstruct their genealogy and unpack their implicit assumptions. To this aim, I will focus on high-level constructs: patient-generated health data (PGHD), observations of daily living (ODLs), quantified self (QS) and personal health information management (PHIM). These constructs have been selected through an abductive analysis of existing labels in political (PGHD), scientific (ODLs and PHIM) and general public (QS) debates on patient health data management practice. None of these labels refer to specific data managing tools or practices (e.g. patient reported outcomes); rather, they provide an abstract definition of data gathered and managed by patients and the data’s relational properties. As such, their analysis allows one to consider each label as a lens through which to observe the emergence of ‘patients as data workers’ from a different angle. As I shall try to demonstrate, these labels are not neutral; rather, they underpin quite different perspectives with respect to health, the patient–doctor relationship and the status of data.
The article is structured as follows. In the next section, I will present the methodology adopted to reconstruct the genealogy of each label. In the subsequent section, I will present each label in detail, discussing its origin and the patient data work implied. In the discussion, I will show how the labels sustain three different patient–doctor reconfigurations: delegation, partnered care and self-experimentation. I will conclude this article by presenting some limitations and indications for future work.
Methodology
PGHD, ODLs, QS and PHIM are labels that describe specific kinds of patient data and/or the social practices of their production and management. These labels share some significant concepts, such as the idea that patients’ role is changing, that these data/information will become increasingly important and that these changes will affect healthcare delivery. However, these labels are sometimes used interchangeably and as synonyms of the practices and the outputs of self-tracking. The aim of this work is to reconstruct the genealogy of each label to reveal its underlying assumptions.
To this end, I’ve analysed different kinds of documents (journal articles and proceedings, governmental agencies’ papers, magazine articles and websites) to reconstruct the origin and underpinning of each label. In line with the scope of this article, I have tried to trace back the original source of each label and restricted the search and the analysis to the documents that provide a definition of the label itself. The research has been conducted by adopting the following analytical questions:
What is the origin of the label?
What kind of data does the label refer to?
What are the main motives for gathering/managing the data?
What is the role of patients/laypeople with respect to the data?
What is the role of healthcare professionals?
What are the main issues and concerns regarding the data?
Where do the data belong?
As noted before, these labels are often used as synonyms and in ways that betray their original meaning. It is out of the scope of this article to explore the current use of these labels as it would require an article in its own right. The methodological choice to refer only to foundational documents is reflected in the results, which privilege a clear-cut distinction among labels and probably underestimate their overlapping.
PGHD, ODLs, QS, PHIM: four acronyms, four approaches
PGHD
PGHD is a label coined by the Office of the National Coordinator for Health Information Technology, a position within the US Department of Health & Human Services. The most comprehensive document regarding PGHD is a white paper published in 2012, 4 and since then, the label has been widely used in official documents.5,6 Subsequently, the label has spread and has been used in several academic publications.
PGHD are defined as ‘health-related data – including health history, symptoms, biometric data, treatment history, lifestyle choices, and other information – created, recorded, gathered, or inferred by or from patients or their designees to help address a health concern’ (p. 2). 4 This definition is a result of the analysis of informal conversations with clinicians, health informatics researchers, patient advocates, health system leaders and a health law specialist. The definition of ‘data’ is broad and includes measured vital signs, self-reported lifestyle data (e.g. diet, exercise) and quality of life data (e.g. sleep quality, social contacts), and data can be ‘structured or unstructured, machine-readable or not, numeric, text, image, waveform, etc’. (p. 4). 4 Scenarios used to illustrate the potential of PGHD refer to structured data gathered through sensors (e.g. glucometers, blood pressure monitors), objectively measured by devices. However, patient record outcomes (PROs), data on patients’ health status reported directly from the patients with standardized and validated questionnaires, can also be considered a good example of PGHD.
As pointed out by the definition quoted above, patients create, record and gather data. While patients can make personal use of PGHD to measure what matters to them and facilitate a patient-defined life, 7 the main benefits are foreseen as complements to provider-directed data. 6 Providers are responsible for reviewing PGHD to assess their quality and relevance and to decide whether to discard document in the electronic medical record (EMR) or share with the care team but not document in the record. 4
PGHD pose different challenges to the healthcare system, including technical, operational, legal and others (for an overview see Petersen and DeMuro). 8 The main operational issues, the ones directly faced by healthcare professionals, are associated with the systematic use of PGHD for providers’ workflow and staffing. Despite the perceived benefits, providers anticipate that they will need more resources to ‘activate’ patients, to provide feedback and review PHGD and to identify the patient subgroups likely to be most active in the use of PGHD.
ODLs
ODLs is a vernacular introduced in Project Health Design, a US programme of the Robert Wood Johnson Foundation focused on the research concerning personal health records, patient-controlled digital tools for health data management.
9
ODLs were ‘encountered’ in the development of the project and are defined as a type of patient-defined and patient-generated data: Observations of daily living (ODLs) are the patterns and realities of daily life that have never before been considered to be part of one’s health record, such as diet, physical activity, quality and quantity of sleep, pain episodes and mood.
10
While PGHD are provider-defined and may have little or no meaning to patients, ODLs are patient-defined data, ‘deeply personal, idiosyncratic sensory and behavioural indicators for the purposes of health monitoring and behaviour modification’. 11 ODLs can be collected through sensors or self-reported information, ranging from ‘counts of nights of adequate sleep to the time frame between eating broccoli and having a bowel movement’ (p. 6). 9 Being patient-defined is the foundational feature of ODLs. As such, ODLs cannot be defined a priori but are rather discovered (e.g. when designing personal health management systems), and the key issue for researchers is not to define which data are ODLs but rather understanding what motivates people to collect them. 12
Patients do not merely collect ODLs but also decide the tools, the duration and the objectives of data collection. Patients can autonomously interpret ODLs, but also share (part of) them with providers. Healthcare professionals can assist patients in selecting ODLs and how to collect them, and play an important role in motivating patients in continuing data collection. Despite being patient-defined, patient willingness to collect ODLs depends on doctors’ willingness to consider them as valuable support to care practices by reviewing ODLs during clinical encounters. In the patient–doctor relationship, ODLs can help provide a richer picture of the patient’s daily life and cues relevant for case management. This information should be stored in the personal health record system, controlled by patients but connected with providers’ EMRs.
The main issue regarding ODLs is the increased burden on patients. Collecting health data is a time-consuming activity, and motivation may decrease fast. 12 Sensors or other forms of semi-automated ways to capture ODLs, such as leveraging online social media, 13 are being considered as solutions to this problem.
QS
The QS is a label coined in 2007 by Kevin Kelly and Gary Wolf, editors of Wired magazine, to explore and put into practice the connection between lifelogging, personal genomics, location tracking and biometrics. 14 Alongside, they founded QS meet ups, informal gatherings of people interested in sharing their lifelogging experiences. The conceptual roots of the QS movement are in self-experimentation and refer to the work of Neuringer. 15
There is no clear-cut definition of QS. Instead, several mottos (e.g. you are your data, self-knowledge through data) provide a synthesis of the spirit of the movement formulated by the founders: ‘Our mission is to support new discoveries about ourselves and our communities that are grounded in accurate observation and enlivened by a spirit of friendship’. 16
The QS movement has been popularized by local meet ups, workshops, conferences and, most notably, a famous Ted talk given by Gary Wolf. 17 The label, however, gained widespread attention not limited to the original movement, attracting scholars from different disciplines (e.g. informatics, social sciences, medicine), and for some QS has become a synonym for self-tracking. 18 QS specifically refers to practices aiming at gathering strictly quantitative data for self-knowledge. QS practices can be triggered by the need to solve a problem, 18 but also engaged for the sake of experimenting and exploring the potential of new tools.
Unlike PGHD and ODLs, QS moves beyond analysis and aims at ‘hacking the body’. The collection of multiple parameters offers the possibility to manipulate them to the desired end. ‘The cycle of experimentation, interpretation, and improvement transforms the QS into an improved “higher quality” self’. 18 The group of peers (e.g. meet ups, online forums) can support the individual in the decision of what to track and how to interpret data as well as in helping to push the existing limits of the tracking tools through hacks. 19
Clinicians have no formal role in QS. QS practices involve laypeople who assume multiple roles – project designers, data collectors and critical sense-makers, 20 leaving no room for clinical experts. However, some scholars conjecture that widespread self-tracking practices will lead to new patient-driven care models. The analysis of aggregate data gathered by individuals, for instance, could offer new opportunities for preventive medicine. 21
These scenarios require the willingness of people engaging in QS to share their data and to explore new forms of cooperation with clinical experts for analysis. 22 The main issues regarding QS are related to the intrinsically voluntary nature of data collection and the limits of existing technologies in supporting laypeople in their self-knowledge endeavour.
PHIM
Unlike the labels presented above, PHIM does not focus on a specific type of data, but rather on some social practices that ‘support consumers’ access, integration, organization, and use of their personal health information’. 23 The label has been mostly used in the academic debate, and the increasing attention it is gaining is mostly due to the success of personal health record systems; moreover, it has aimed at supporting designers by providing them descriptive and analytical tools.23,24 Most of the works are exploratory in nature and have the purpose to map a largely unknown territory in which health-related activities and daily life are inextricably intermingled.24,25
PHIM refers to the practices of managing health-related information and varies from person to person, from time to time. A non-exclusive list of motivations to perform PHIM activities includes scheduling and planning, coordinating with relatives and caregivers, decision-making, tracking and communicating with peers and healthcare professionals. To these aims, people collect and use a wide array of data and different tools to gather and share them, from family calendars to annotations on healthcare records.24,25 Despite the wide definition of PHIM, which encompasses all sorts of health-related information, many articles focus on patient-defined data and on their emergent and (medically speaking) unconventional use.
Doctors have little role in PHIM activities. Most of these activities are not acknowledged by healthcare professionals and remain invisible to them,24,26,27 unless some PHIM are explicitly required by healthcare professionals themselves. In this case, providers can instruct the patient on how to perform data management correctly. In other cases, providers may implicitly require patients to perform certain PHIM activities, such as maintaining good care of their medical records, keeping them in order and bringing them to periodic visits. 25 Inadequate PHIM by patients can lead to disruptions in the patient–doctor relationship.
Supporting these activities requires the design of patient-centred tools which are flexible enough to accommodate the diverse scopes and the changing needs of users. The main issues regarding PHIM are the additional burden caused to patients,25,26 the fragmentation of information collected from various sources 28 and the willingness of people to share with providers information they perceive to be ‘personal’. 29 Moreover, the highly personal styles and tools used in gathering data may cause difficulties in sharing the data with providers.
The changing locus of health data production and use: three perspectives – delegation, partnered care and self-experimentation
The description of the four labels provides the basis for theorizing patient data and data work. To this end, I shall refer to data work as a practice, ‘a mode, relatively stable and socially recognized, of ordering heterogeneous elements into a coherent whole’ (p. 6). 30 Health data are but one of the many ‘heterogeneous elements’ of patient data work, such as actors (patients, healthcare professionals, peers), technologies (EMR, PHR, measuring devices), knowledge (lay, professional) and so on. The analysis of the four labels illustrates how each definition points to a different set of relations.
A simple example, body weight, could help to illustrate this point. Body weight is PGHD when a doctor requires a patient with chronic heart failure to measure it every day to include the measurement in an EMR. Weight is an ODL for a diabetic patient asked by the doctor to keep track only of her glucose level, if she decides to keep her weight under control to improve her running performances and share the measurements with a her doctor during a routine visit. Measuring body weight is a QS activity for a person interested in establishing a pattern of food intake, weight and sleep quality and discussing with peers in an online forum how to improve her sleep. From a PHIM perspective, measuring and recording one’s weight is an activity that requires being fitted into the busy morning schedule of a father in charge of preparing breakfast and driving his two children to school.
Each label rejects an ontological definition of data; rather, it points to the relation between health data and other ‘heterogeneous elements’ and activities. In doing so, each label describes more than just health data and refers to the practical socio-material arrangements of patient data work. The analytical questions presented above can be reinterpreted as a way to map which are the relevant elements for each label. With the notable exception of the origin of the label, Table 1 furnishes a schematic way to identify the relevant features of the social practice called ‘patient data work’.
PGHD, ODLs, QS and PHIM.
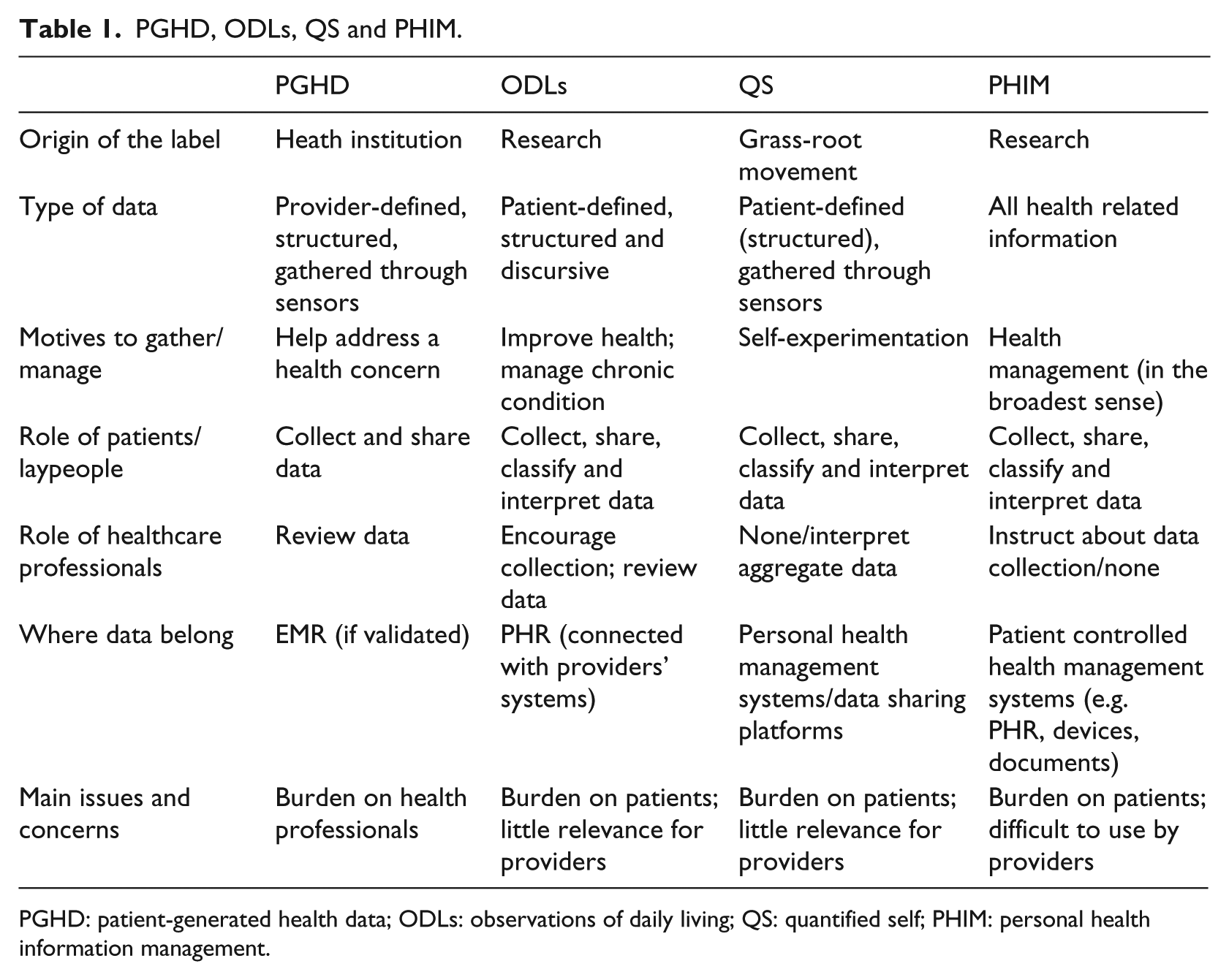
PGHD: patient-generated health data; ODLs: observations of daily living; QS: quantified self; PHIM: personal health information management.
Table 1 also allows one to unpack the implicit underpinnings of each label. PGHD, thus, is a label that conceives patient data work within a traditional frame of reference, a provider-driven care model characterized by an asymmetric patient-provider relationship. PGHD presents a future form of healthcare in which patients are trustworthy partners in health management only if their role is restricted to data-gathering activities while providers remain in charge of data analysis. In a nutshell, PGHD advocates for new technologically enhanced forms of delegation to patients.
ODLs envision a more balanced pattern of patient–provider relationships coupled with patient-defined health/wellbeing goal setting. Patient-defined data can help patients in self-managing practices, but also be of use to providers for a richer picture of patients’ health. ODLs refer to a multifaceted health management model through which patients and providers can cooperate while pursuing different goals. Should we reduce ODLs to one motto, we could say it envisions a ‘partnered care’.
QS envisions a radically different form of health management. Laypeople are considered health knowledge seekers enabled by technologies, and they may not require professional expertise. QS envisions a novel space in health management in which laypeople rely on their own judgement and the help of peers to establish connections among different data sources and perform experiments (body-hacks) to improve their quality of life. In a word, it is a self-experimentation perspective.
Finally, PHIM refers to the mundane practices of managing health information in everyday life. Boundaries between health and other spheres of activities blur as practices blend together. PHIM is used to highlight the unfinished business of personal health management and the tinkering to accommodate one’s personal life and providers’ recommendations.
PHIM is a cross-cutting concept. PHIM refers to any form of health data management, and it can be considered as a synonym for patient data work. As such, the PHIM label does not hold any given vision of a future form of healthcare.
Each of the labels presented assigns a role to healthcare professionals, laypeople and technologies and define what has to be considered as relevant knowledge. Leaving aside PHIM for the reasons highlighted above, the analysis confirms the striking differences between the other three labels (Table 2). As we move from the PHGD to ODL to QS, we witness the diminishing role of the healthcare professional, the increasing relevance of the patient and a shift from validated clinical knowledge to emerging grass-roots discovery. Not surprisingly, these shifts are well represented by the different roles of self-tracking technologies. Under the PHGD approach, technologies are considered as tools to restrict the agency of patients to data gathering, ensuring the collection of objective and clinically reliable data. At the opposite end, QS experimenters consider technologies as tools to be hacked and for gathering and interpreting data to establish new patterns.
The role of healthcare professionals, laypeople and technology in PGHD, ODLs and QS.
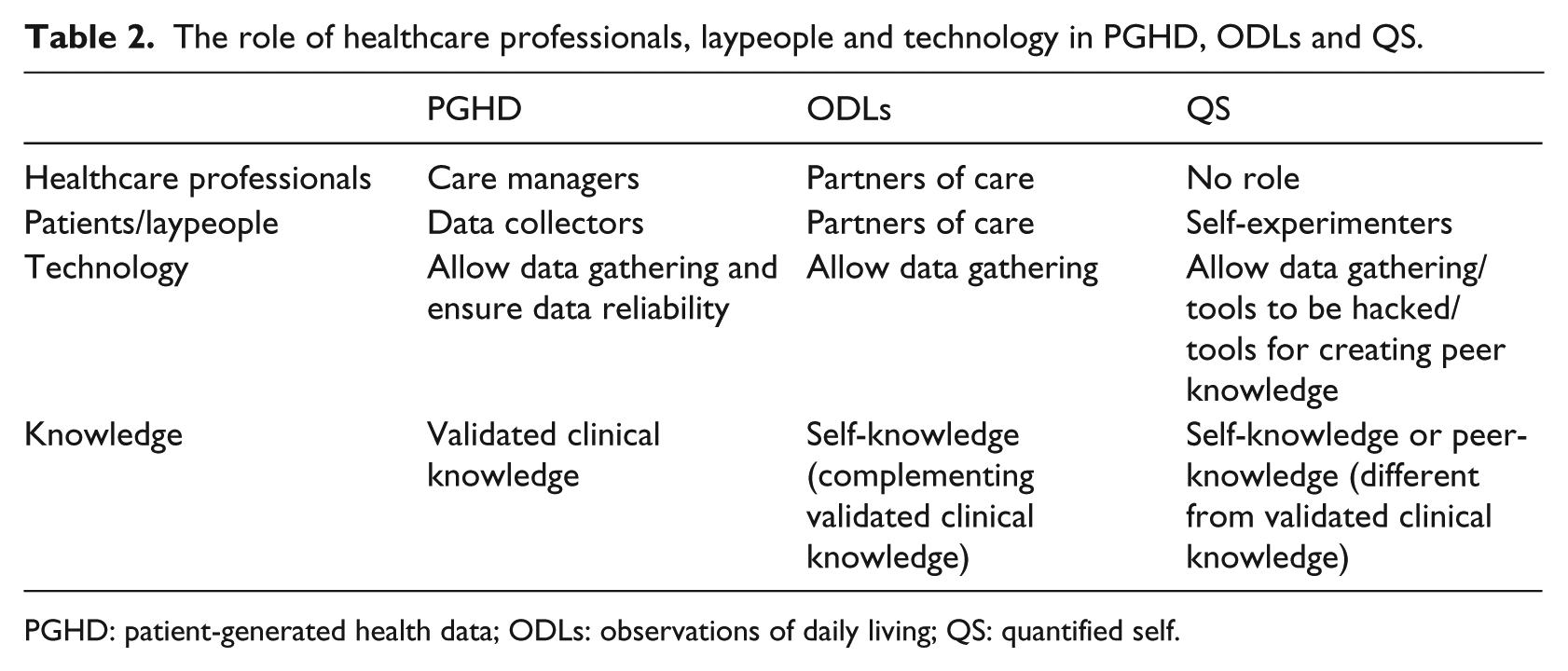
PGHD: patient-generated health data; ODLs: observations of daily living; QS: quantified self.
Conclusion
Policymakers, healthcare managers and professionals, vendors, medical informatics scholars and patients are showing growing attention towards data produced and managed outside healthcare settings. The existence of multiple stakeholders is reflected in the origins of the labels used to describe patient data work. In this article, I have reviewed four emerging conceptualizations regarding patient data work: PGHD, ODLs, QS and PHIM. While two (ODLs and PHIM) belong to the scholarly debate, the remaining labels have been coined by a government agency (PGHD) and a tech magazine (QS).
These actors have different expectations about the risks and benefits of data gathered by patients, about new forms of patient-hood and the patient–doctor relationship and about novel kinds of healthcare provision. These expectations are often implicit and hidden behind general statements.
Drawing to the end of the article, I would set aside the analytical/descriptive stance adopted in the rest of the article to reflect on the generative effects of the labels under scrutiny. The labels under analysis, thus, are not merely descriptive, but are instead political devices as they present a desired state of affairs. Each label, albeit implicitly, reveals the underlying assumption about legitimate knowledge and whose knowledge counts. Moreover, each label can be considered as an integral part of larger socio-technical desired scenarios. Each label is part of larger set of envisioned relationships, expectations regarding roles and the provision of care in the future and associated concerns. Each label represents a lens through which a relevant stakeholder defines the challenges and the possibilities offered by self-tracking technologies.
PGHD provides a government-oriented, provider-centric view of the health provision system in which only healthcare professionals possess valuable knowledge. QS offers a patient-activist perspective and a potentially disruptive patient-driven knowledge creation with no or a limited role for clinicians. ODLs envision a more collaborative scenario where validated clinical knowledge coexists with patient discovery and new forms of therapeutic alliance as well as more collaborative patient–doctor relationships. The fourth label, PHIM, is a cross-cutting concept that draws attention to the new role of patients as data ‘prosumers’ and the increasing burden of data work required to manage one’s health and wellbeing.
Footnotes
Acknowledgements
This work is part of a larger research project (TreC – Cartella Clinica del Cittadino) funded by the Department of Health and Social Politics of the Autonomous Province of Trento, Italy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.