
Abstract
Healthcare professionals are increasingly working with data in their care delivery practices. However, there is limited understanding of how data work is enabling novel practices. This study focuses on novel nursing practices emerging in the context of remote monitoring of chronic patients. Specifically, we analyze how personalization of care is achieved in practice through data work. The study is based on a case of a pilot center in Norway where nurses provide remote care to patients by using a specialized system. We examine the practices of the nurses and how data in the form of graphs, alerts, questionnaires and messages are used to personalize care. We identify three main practices of data work for personalization: preparatory work, continuous adjustment and question fine-tuning. Finally, we discuss the pivotal role of nurses’ data work for personalized care in remote care.
Introduction
Advanced IT solutions enable healthcare professionals to generate, access, manage and analyze large amounts of data, making data work a substantial element of contemporary care delivery practices. 1 However, there is yet limited understanding of how this novel work is changing care practices and professions. 2 For instance, the use of remote monitoring systems and IoT devices allows healthcare professionals to capture datasets of patients’ vital signs and monitor them at a distance, but limited research has investigated the implication of these practices on the work of professionals involved in the monitoring of patients, as, for instance, tele-nurses.
Remote patient monitoring systems have gained increasing popularity in recent years. This is due to their potential to improve medical services by providing more affordable, timely and accessible care. The use of telemonitoring systems has also been shown to increase the frequency of interactions between patients and health providers,3,4 and number of systematic reviews of research studies suggests that telemonitoring benefits patients by promoting their engagement in care practices.5,6 However, while the benefits of allowing patients to live at home are well recognized (e.g. increased quality of life and well-being), there is a preoccupation that with telemonitoring technologies patients are neglected. These systems are introduced as solutions for the shortage of healthcare professionals in the face of a growing population of older people with chronic diseases, and they allow health professionals to increase the number of patients they care for. 7 From a patient perspective, this means less dedicated time on the part of professionals. This preoccupation concerns also the risk of losing human contact and the personalized quality of care practices. Nursing literature emphasizes how expert nurses work from a holistic understanding of health conditions tuned to each individual patient and his or her specific situation, and it is not straightforward how personalized care practices can be delivered remotely. In addition, these systems generate new types of data, increase the volume of data, and change the frequency and mode of data collection and usage. It is also unclear how these new types of data impact the health service provision, and which types of data work emerge around it.
In this study, we therefore examine how tele-nurses perform data work, and we are interested in understanding how data work can be supportive of personalized care in the context of remote care. Specifically, in this article, we want to understand what type of data work is required from nurses in remote care and how data work is involved in the delivery of personalized care. We ask how is personalization in remote care achieved in practice through data work? To address this research question, we studied a case of tele-nursing practices in the context of a pilot telemonitoring center for patients with chronic conditions in Norway. The center provides technology-mediated care to patients at home, who use various digital measuring devices to record vital signs (e.g. blood pressure, pulse and glucose) and transmit this data electronically. At the center, nurses interact with and provide care to patients by using Dignio Prevent, an information system for remote patient monitoring and nurse–patient communication. Dignio Prevent collects data from patients’ digital measuring devices and visualize them in form of dashboards, graphs and tables. It also offers a number of functionalities for patient–nurse interaction such as messaging and a questionnaire. Nurses provide care at a distance by using the data to identify signs of exacerbation, intervene based on these signs, and prevent emergency care visits and hospital admissions. They also proactively guide patients into behavioral changes toward healthier living habits.
Research methodology
Research context and research design
The research presented in this article has been conducted as a case study on the early experiences with telemonitoring in primary care in Norway. The case study was conducted in Dignio, a private company which develops a telecare cloud-based software system, Dignio Prevent, and runs a telemonitoring center on contract for a small Norwegian municipality. The center is staffed with three nurses, and the patients are assigned to the center by the municipal care services. The center started in October 2016, offers remote care for patient with the following chronic conditions: diabetes, chronic obstructive pulmonary disease (COPD) and heart failures and had at the time of the study (October 2017) ca 145 patients. The nurses use Dignio Prevent as a patient journal and decision aid system, as well as communication platform. Patients are given a set of digital measuring devices according to their condition and a tablet with an App called MyDignio. For instance, a patient with diabetes would normally use a device for measuring blood glucose levels and a digital scale for measuring body weight. In MyDignio, the patient has full access to his or her results, records and journal and he or she can communicate with the health care personnel with messages which are also included in the record. When they use the devices, the measurements are displayed in the patient app on their tablet. Nurses access the measurements through the web interface. Patients and nurses communicate with each other via ad hoc and weekly messages and questionnaires, occasionally via phone.
The focus of the case study has been on how the new service is organized and offered to patients and what role technology plays in the nurse–patient relation. Specifically, we have studied the practices of nurses, how they care for patients remotely through a digital infrastructure, and how they deliver personal care. As our research question has guided us toward the work nurses do to fulfill their profession’s goal of delivering personalized care, patients’ perspectives on whether they experience remote care to be personalized is not within this article’s scope. Other research has, however, studied patients’ experiences in the same empirical case. Preliminary results from this research point to patients reporting of increased “follow-up, control over their own health situations and experience of personal safety and understanding of the body’s signals (our translation).” 8
Data collection and data analysis
Fieldwork was conducted from August 2016 to October 2017. Data were collected through interviews, observations of work practices and attendance of meetings. Informal conversations have also contributed to our understanding of the case and guided further data collection. 9 The study was conducted in cooperation with the key actors in Dignio, and one of the authors is the head nurse in the center. From August to December 2016, we have collected data on the Norwegian eHealth and telecare context at large by reading of policy document, project reports and research reports. From January to October 2017, the first two authors conducted a period of data collection in the company which included 10 interviews and 15 h of observation of work practices at the remote monitoring center. We have interviewed the nurses working in the center about their experiences as a nurse in home care or hospital and as “telenurse” working with remote care. We have also interviewed the management team about their vision and approach to primary care services, and the IT team of the company about how the software has been designed, developed and updated, and how users’ feedback was considered. Interviews were recorded and transcribed verbatim. During observation sessions, we sat next to the nurses working in the center. We have paid attention to how nurses interact with patients, navigate the system, reply to patients and assess patients’ conditions. During observations, we were allowed to ask nurses to explain what they were doing. We also paid attention to the ongoing conversations in the room. For example, nurses would often ask each other for advice on complex cases. Finally, we also attended meetings of the nurses’ team where they discussed current challenges and how the service could be improved. We took detailed notes which were transcribed soon after these sessions.
Given the emerging nature of nurses’ data work, we have chosen an interpretative approach. 10 Data interpretation has been guided by our interest in understanding how nurses assessed a patient’s condition and how they followed up on the vital sign readings. We have been struck by how much time the nurses in the center spent on refining comments and questions to each patient, and on assessing and re-assessing the patient’s condition. The concept of personalized care emerged as a central concept in our data and guided the identification of the three practices of data work.
Findings
In this section, we present the findings from our study. We have identified three main practices of data work supporting personalization: preparatory work, continuous adjustment and assisting the patient in creating routines for producing relevant data by fine-tuning questions.
Preparatory work: identifying the core health issues
A prerequisite for delivering personalized care is to understand which health issues are most pressing for each patient. It is critical that the nurses understand how the condition might develop for each patient to be able to monitor relevant values, and thus be able to intervene and prevent emergency situations. To decide which values should be monitored, which data should be collected and how often, nurses at the center engage in preparatory work in collaboration with the municipal care services and the patient. The collaboration with the municipal care services starts when a patient is assigned to the center, and the coordinator at the municipality informs the nurses about the patient: diagnosis, current condition and abilities and housing and family situation. Afterward, one of the nurses from the center visits the patient at home to meet him or her in person. At this point, patients receive a standard package of devices according to their diagnosis at that point. The nurse explains how to use the devices and the tablet and explains what kind of service is offered by the center and what kind of support the patient should expect from the nurses.
The patient follow-up is guided by a standard pathway defined by the medical team of the company. The pathway sets milestones and phases during the first year as a user of the telemonitoring service, and includes an objective for the service and a screening of life style habits and personal motivational factors. These are then adapted to the needs of each patient. For instance, the first 2 weeks are dedicated to teaching patients the correct use of the devices and of the tablet. This period can be extended if the patient needs more time to learn to handle the devices. Afterward, the nurses discuss and agree with patients on how often they should take measurements with their devices (e.g. twice per day) and how often they should interact. The frequency is often modified as it depends on the patient’s health conditions which vary over time. For instance, a patient who has just been discharged from the hospital may need to be monitored more frequently than what was agreed upon at the start. For the nurses, it is important that patients take an active part in these decisions, and they commit to the agreements. For instance, if data do not flow in the patient record in Prevent as agreed, this is considered a signal that a patient is struggling. In these cases, the nurses try to get a picture of the whole situation of the patient, his or her lifestyle and everyday practices and challenges. And they may, for instance, use the weekly messages to the patient to remind and encourage him to take the measurements as agreed.
Other parameters can also be set up to personal needs. For instance, in a case of a patient who took measurements very seldom and not as requested, a nurse explained that this patient lives in two different places and often forgets to take the tablet and the devices with him when moving from one location to the other. The nurse also suggested that they could give him or her a smaller tablet if this helped with carrying it around. They try to find ad hoc solutions that fit with the personal habits of patients. The flexibility of the system, of the devices and of the pathway, allows nurses to configure the data flow, the patient–nurses’ interaction via messages, and the progression of the patient, according to the patient’s specific needs. In addition, the patient is involved in co-deciding how the service is personalized to his needs. The personalization of the telemonitoring service is done according to both the needs of patients (what to monitor and how often), and the data needs of nurses (how to get the right data to be able to understand and intervene).
Continuous adjustment: understanding how to monitor what is relevant
We have mentioned that the frequency of the interaction is modified and adjusted according to the variations in patients’ health condition and personal situation. The continuous adjustment of telemonitoring also includes more specific types of adjustment. Each measurement from the personal devices is automatically sent to the record of each patient in Dignio Prevent. The nurses always set a threshold value for each measurement/vital sign for each patient. For instance, the blood pressure may become critical at different thresholds depending on body weight and other factors. If the measurement is surpassing the threshold value, it will be displayed in Dignio Prevent in form of an alert message and color coded in yellow or red. The alert guides the nurses to attend to those patients with measurements that may indicate signs of exacerbating health condition. The threshold is set but continuously adjusted, filtering measurements according to the variations in the health condition of the patient. The notes from observation describe the following: A nurse is working on the weekly message; she spends substantial amount of the time looking through the general list of alerts from the measuring devices. She typically selects and opens alerts that are coded in red, she looks through the history of alerts, and adjusts the threshold. She says that they need to adjust the threshold many times; patients are different, and they need to identify what is a normal threshold for each specific patient.
In Prevent, thresholds can be adjusted by the nurses and consequently the incoming values are color coded accordingly.
When working with the data, nurses need to make sense and interrelate different data sets. For instance, when a measurement is out of the acceptable range, the nurse needs to understand what has happened. Usually they start by examining the trends displayed in the graphs for the past weeks. Dignio Prevent allows to zoom in and out of the graph by selecting different time intervals (see Figure 1). Then they check the recent answers to the questionnaire, and other relevant messages the patient may have sent. Thus, when a measurement is out of range, nurses do not call the patient right away to ask for an explanation. They say that there is not a direct correspondence between receiving an unacceptable value and intervene with a phone call to the patient. One of the nurses explains, One thing is the measurements and the devices and that is simple, it is pure technical, they measure, but health personnel must know, what to do when the measurement departs (from the usual value), it is not enough to just make a call, you have to know what it means.
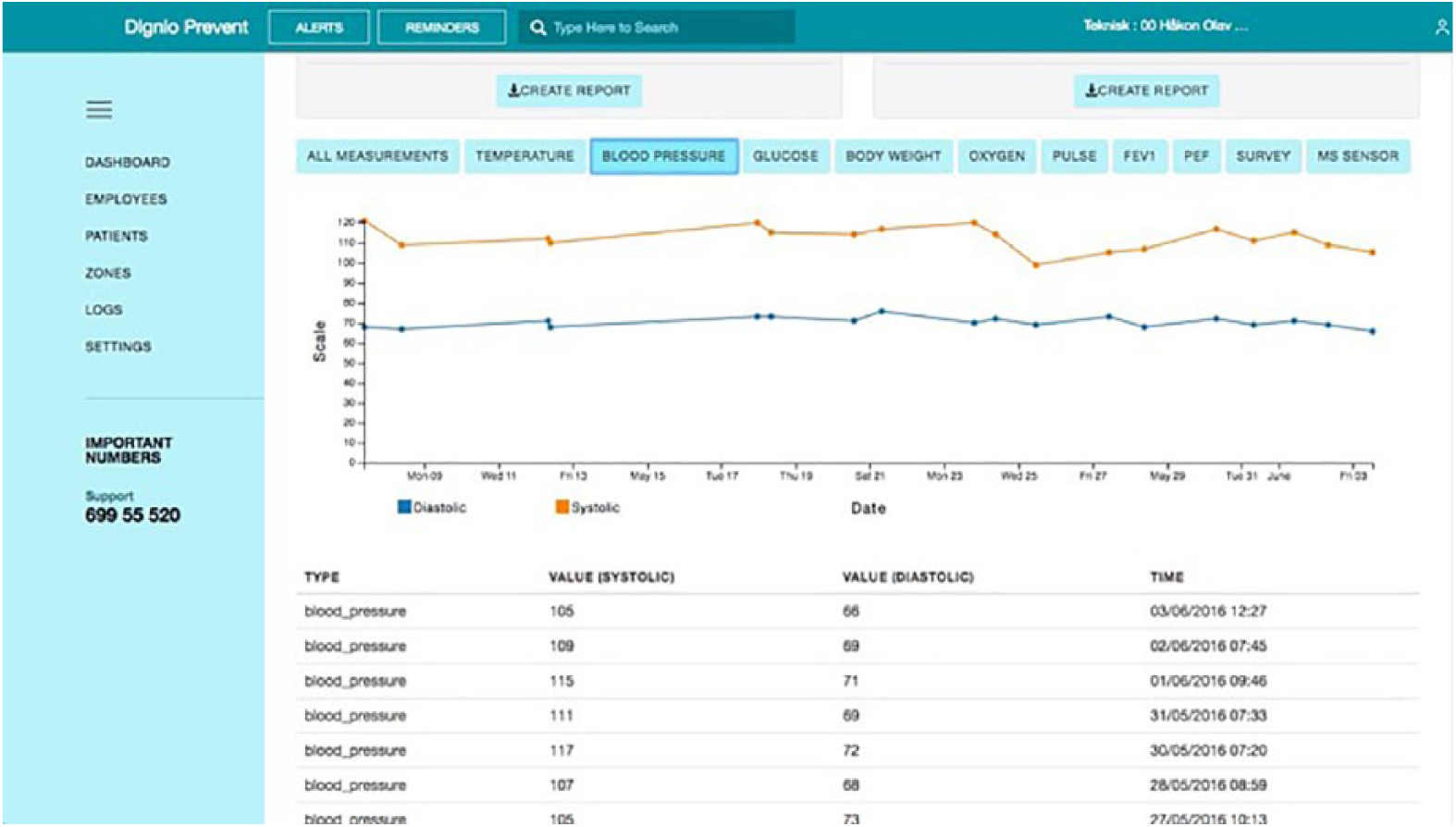
The graph of measurements in Dignio Prevent.
The personalization of the threshold facilitates and enables nurses to make sense of each measured value in relation to the rest of the accumulated data and in relation to their knowledge about the patient.
Fine-tuning of questions
The patients receiving telemonitoring have different co-morbidities, clinical histories, different lifestyles and personal issues. For the same condition, signs of exacerbation can manifest themselves in different ways. Thus, for each patient, specific values must be monitored more carefully than other values. The monitoring practice requires more than reading the incoming measurements from the personal devices. Measurements and their variations need to be contextualized for each patient. The questionnaire in Prevent is used with the aim to ask patients questions about their daily routines and experience of their vital signs, to get a more complete picture beyond the measurements (see Figure 2). For each condition, a standard set of themes are covered in the questionnaire. For COPD patients, for example, breathing experience and exercise routines are central. Given the themes, nurses select which of them are more relevant for each patient and they also formulate differently the questions within these themes, their order and the type of answer requested (e.g. yes/no, or different scales). By formulating personalized questions and by posing them in a personalized sequence, nurses try to capture contextual information on the critical factors for each patient.
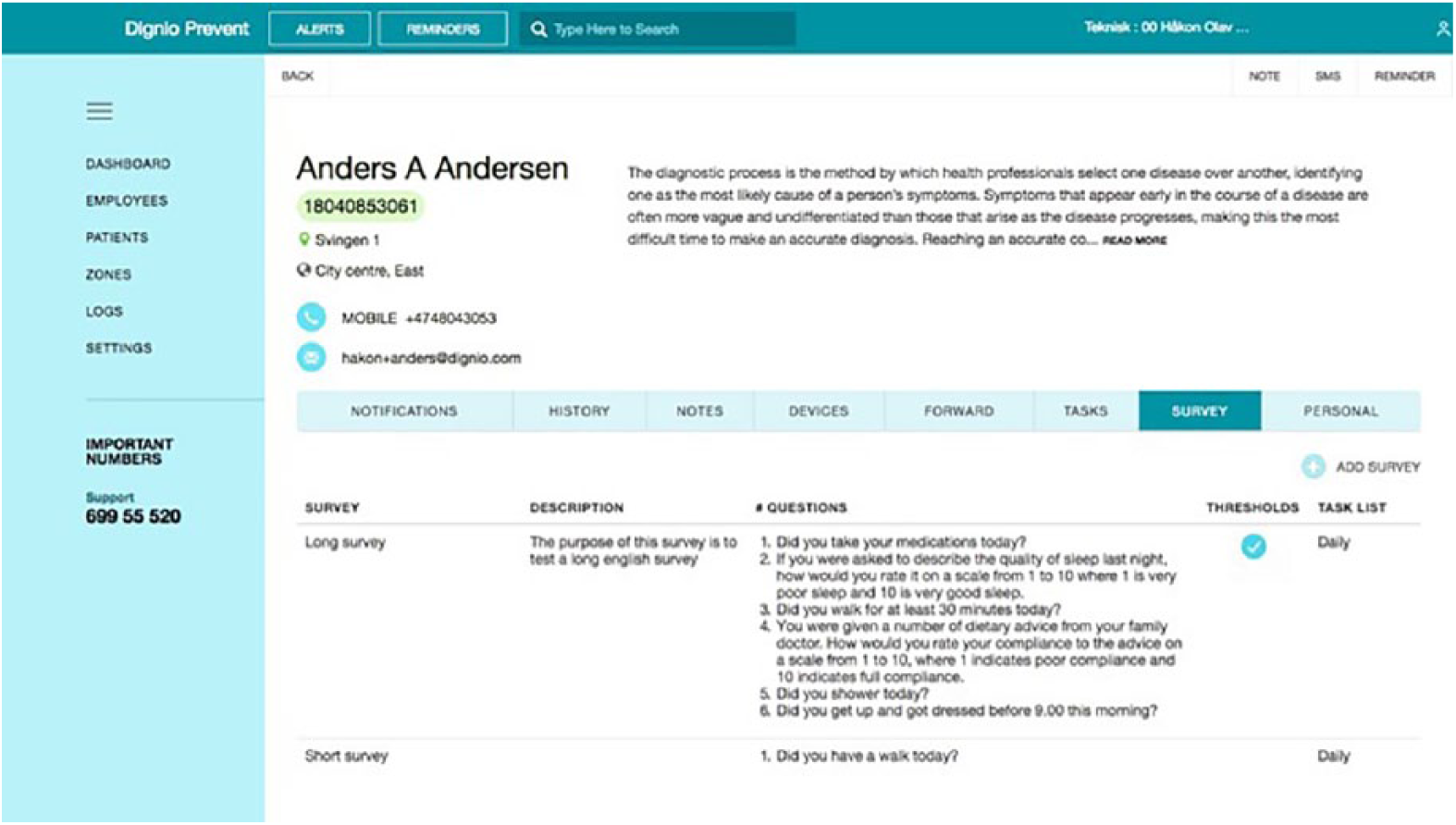
The patient questionnaire in Dignio Prevent.
Understanding this level of personalization for each patient is not straightforward. A nurse explains how the different patients’ needs make it difficult to define a standard routine for the follow up of COPD patients: you cannot define fixed routines, for instance for you, which symptoms would you develop first? You cough a lot for example. How do you track that? Is it in combination with fever? Is it in combination with when you blow in your spirometer, then the measurement falls a bit?
It can be difficult to understand which symptoms become traceable first, and how they relate to each other. The combination of personalized parameters and personalized questions tries to address this complexity.
A nurse describes how the questionnaire is used to address the individualization of the risk factors for COPD patients: some of (the patients) start to cough, but one of our patient said, no, the first thing I notice is that my breathing gets heavier, then I start coughing, and then comes the fever. Then one should know that the most important thing with this patient is, not temperature but to capture when he starts to feel his breathing is getting heavier, and then you should formulate a question “do you think that you have heavy breathing today?”
The questions should then address the critical individual risk factors and also be formulated in a way that is easy to make sense of from the patient’s perspective. The additional aim with asking personalized questions is to guide patients to understand their conditions. By reading and answering the questions, the patient in the example is also reminded to pay attention to the quality of his breathing and to learn to understand how his body experiences exacerbation.
The nurses in the center spend a considerable amount of time working on defining the right formulation for the questions. For instance, in another case a nurse was examining the data of a patient whose critical factor was body weight. The patient had explicitly said that one of his goals was to lose weight. Accordingly, the nurse needed to monitor closely his eating habits and understand them beyond the bare measurement of the weight from the digital scale. In one conversation in the center, the nurse discussed with the other nurse in the room how to ask a patient about “eating habits” in the questionnaire. One nurse suggested to formulate the question in terms of intervals, for instance, asking, “Do you eat every three hours?” or “Do you eat at fixed times?” In these formulations, the nurse stresses that for some patients it is important to be specific, and to pose questions that are easy to answer in relation to their cognitive abilities. For instance, asking about “eating habits” would be too general and too vague, thus difficult to answer.
Discussion and conclusion
In this study, we asked, “How is personalization achieved in practice through data work in remote care?” We approached this question by investigating nurses’ data work practices and examining how they support personalized care in the context of telemonitoring. We identified three different practices related to how data are sorted out, selected and generated to support personalized care: preparatory work (using data to identify the core health issues), continuous adjustment (to understand how to monitor what is relevant) and fine-tuning of questions (to engage patients in generating relevant data). Specifically, we found that personalization is achieved by working with selecting which data are relevant and meaningful to nurses (e.g. by deciding for each patient the type and frequency of data collection), working on data by interpreting and cross-analyzing data from different sources (e.g. from the devices and the questions) and working on enriching device-generated data by collecting additional data on specific issues (e.g. by asking specific follow-up questions to each patient). Data both constrain and enable the nurses to provide a service that is “fit-for-purpose.” 11 However, being able to provide a service that “fits” the specific needs of each patient requires also the work to understand how relevant data should be generated by each patient, both for responding to urgent situations and for attending to the long-term issues caused by the chronic condition. Thus, the ability of nurses to provide personalized care to patients is based on the data work of sorting out, directing attention to and generating relevant data.
Nurses’ work is driven by data as they collect, make sense of, use and act upon data. In remote care, data play an even more central role than in traditional settings. Prior research on novel telecare services has analyzed the effect on patients,5,6 but less attention has been directed to understanding to what extent and in which way data work is pivotal to remote care. By focusing on how personalization is achieved in remote care, we show how data work is not only about analyzing the data elements accumulated in the system but also includes the work of deciding what is relevant data, and discerning which incoming data signal a follow up action for each specific patient. While the technology—through the variety of available health sensors and the flexibility of the software—potentially can be used to collect vast amounts of signals from the patients, nurses do not collect all possible data. Rather they selectively orient their work toward defining what are relevant data and values, as well as guiding the patients into co-producing these data.
Nurses have novel roles in telemonitoring and these change the way they work requiring specific knowledge and skill. 5 Telecare technologies depend on specially trained nurses dedicated to read and interpret monitoring data. 12 As we have shown, the organization of work traditionally based on pre-established plans needs to accommodate the personalized needs of patients. 13 We hope that our research contributes to a better understanding of the emerging practices of “telenursing,” and that future research will investigate implications for nursing education.
Footnotes
Author’s note
Miria Grisot is also affilaited to Department of Technology, Kristiania University College, Oslo, Norway.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The research is part of the Center for Connected Care, funded by the Norwegian Research Council, grant no. 213143.