
Abstract
The medical profession is highly specialized, demanding continuous learning, while also undergoing rapid development in the rise of data-driven healthcare. Based on clinical scenarios, this study explores how resident physicians view their roles and practices in relation to informed patients and patient-centric digital technologies. The paper illustrates how the new role of patients alters physicians’ work and use of data to learn and update their professional practice. It suggests new possibilities for developing collegial competence and using patient experiences more systematically. Drawing on the notion of flipped healthcare, we argue that there is a need for new professional competencies in everyday data work, along with a change in attitudes, newly defined roles, and better ways to identify and develop reliable online sources. Finally, the role of patients, not only as consumers but also producers of healthcare, is a rather formidable and complex cultural change to be addressed.
Keywords
Introduction
Digitalization of healthcare is mentioned in policy and research as a partial solution to global concerns about increasing costs, quality and access.1,2 It is also possible to increase quality of life. 3 This might include distance monitoring, video consultations, self-care and peer-to-peer support. Healthcare has recently undergone developments like patients’ access to electronic health records (EHR), 4 increased online support communities and physician-rating websites.5,6 These may impact patient interactions with each other, information seeking, and relationships with healthcare professionals. 7 The development is rapid, involving adaptations for patients, care organizations and professionals.
This all adds up to a changing role for patients, that is, that patients are no longer merely consumers of care, but are instead regarded as co-producers. Patient empowerment is a broader term but closely related to the concepts of patient-centered healthcare and patient participation. 8 Patients today are more informed—sometimes misinformed—due to the vast amount of online health information.9,10 Furthermore, the datafication of health and self-care practices has given rise to personalized and individualized healthcare, enabling patients to be in control and responsible for the management of their own health. 11 Patients participate as co-creators in care, self-tracking, self-managing, using social media and personal health records.12,13 The alleged desirability of shared decision-making is based on the patient’s right to be involved, informed and take an active role. However, evidence of healthcare professionals’ intentions to engage in shared decision-making is uncertain as the scientific evidence is insufficient. 14
Digitalization transforms not only healthcare and work practices, but also how physicians interact and learn at work. Many studies in health informatics and related areas have focused on the design, implementation and use of digital technologies in clinical settings (e.g. telemedicine and patient records); the technological possibilities are surely many and promising. Previous research suggests that social media can enhance knowledge sharing 15 and translation of research evidence into clinical practice. 16 The literature further points to the potential with healthcare big data, in the context of integrated electronic health records, to support physicians’ clinical decisions, while also addressing new issues related to privacy and security.17,18 A common concern among physicians is that digital technologies may interfere with the patient communication or workflow and lead to additional burden and workload.4,19 Some research results indicate that even though digitalization offers great possibilities, the potential for involving the patients, in particular, so-called expert patients, is not always embraced by health professionals.20,21
This transformation, enabled by patient-centric technologies and data analytics, has been described as a shift from “Pull” to “Push” in medicine, 22 referring to the fact that patients provide healthcare practices with data and information instead of the other way around. So healthcare is inverted or flipped, similar to the way digital technologies have been used to flip education.23,24 However, there is a lack of knowledge regarding how healthcare organizations and professionals are affected by a flipped healthcare. Is it for better or worse? As the healthcare landscape changes, there is both a need and an opportunity to broaden the scope of health informatics research.1,25–27
Thus, there is a need for a deeper understanding regarding how flipped healthcare is viewed by the health professionals. The aim of the paper is to describe how resident physicians perceive the impact of these changes on clinical practice, and the new competencies that may be required of them. The research question is: How do resident physicians view their role and practice in relation to informed patients and patient-centric technologies?
Research approach
The methodology is an interpretative qualitative study designed in the spirit of collaborative practice research. 28 Physicians working in hospitals and outpatient clinics in Western Sweden were chosen for participation in the study. They are particularly interesting as a study group because they represent the next generation of clinical practice: they work as physicians and are also still in training toward specialist competence. Three semi-structured focus group interviews were conducted with 17 participants in total (Table 1). Each focus interview lasted about 1 h and was recorded and transcribed. Informed consent was obtained according to Codex rules & guidelines. 29
Data collection and participants.
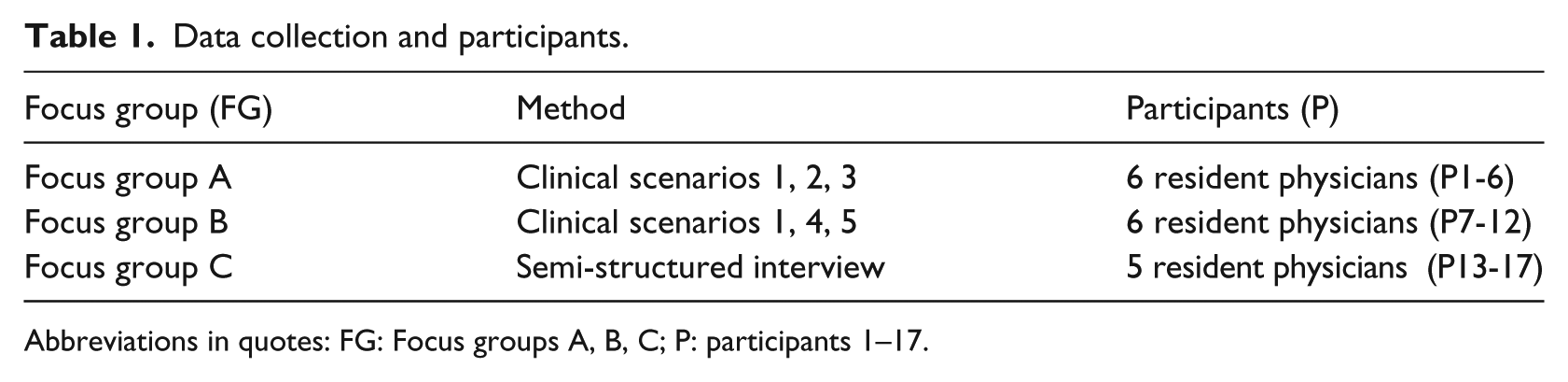
Abbreviations in quotes: FG: Focus groups A, B, C; P: participants 1–17.
This is a follow-up study to an initial semi-structured interview study with individual resident physicians. 30 The focus groups in this study were intended to further investigate and explore in depth the specific topic of emerging challenges from digital patients (i.e. patients that Google their symptoms and use consumer health or self-care technologies). Five clinical scenarios (see Appendix 1) were developed and used in focus groups A and B as a basis for discussions, to capture the resident physicians’ perceptions and attitudes as members of a group rather than individuals. An additional semi-structured focus group was conducted, guided by the themes for the scenarios but aiming for an understanding of challenges related to demands for new competencies in particular.
The analysis was conducted using qualitative methods of content analysis to summarize and systematize the material into categories, identifying relevant themes and subthemes. 31 The interviews were done in pairs with author 1 present in all, accompanied in each case by one of the coauthors. Preliminary analysis was conducted manually by the interviewing researchers. A basic coding scheme was developed with descriptions of each node, and secondary analysis was conducted by the first author supported by the qualitative data analysis software NVivo 10. 32
Findings and analysis
The results are presented and discussed according to the main themes identified in the analysis, describing how the participants viewed their professional roles and changes to professional practice in relation to informed patients, patient-centric digital technologies and demands for new competence.
A profession in transition, to be digitalized or to digitalize?
The physicians described how digital technologies—referring broadly to the use of IT, including administrative systems, clinical decision support and patient-centric technologies—have become increasingly integrated into everyday practice: “… as an equally important part of our daily work, such as our stethoscope and our intercollegiate contact …” (FG C: P14). They shared feelings of frustration arising from well-known IT-related problems, techno-optimism and top-down approaches: “I think those who develop IT really need to ask the doctors, the nurses, anyone using the system before they implement it /…/ in 2017, I do not understand that people can develop such a terrible IT system in healthcare” (FG C: P16). Nevertheless, they were optimistic about the potential of better use of patient-centric digital technologies (e.g. smartphone apps and other self-tracking devices for measuring and analyzing personal health data). Rather than focusing on technological aspects or specific systems, the participants described this as a matter of developing new work practices, norms, and behaviors, calling for a change of attitudes, for instance when it comes to patients bringing their own data: “… working for it instead of against it …” (FG B: P11).
Because of the new openness and transparency of health information and patient data, they also saw an increased need for better tools for them as physicians to aid the patient’s decisions: “… helping out, manage numbers, and explain relative risks …” (FG B: P7). The participants reflected on the transition “from textbook knowledge to free information on the Internet” (FG A, P3). They emphasized the benefits of having access to updated, real-time data and expertise, but pointed also to the risk that physicians’ knowledge might become more fragmented and “rather superficial perhaps” (FG A, P5). They highlighted that context is important for discussing patient questions and wished for more interactive information systems. They suggested functions like filtered information targeted to specific questions or the patient at hand and access to online clinical evidence and guidelines to support diagnosis and treatments: “… so you get a little summary…” (FG A: P1) along with information adapted to patients and overall better integration to get the full picture: “… integrating all that occurs during the care of a patient, and then you get to choose what you want to make use of” (FG C: P15).
New opportunities to keep updated and communicate with peers and patients were expressed as both a blessing and a burden. The participants saw the potential for example social media for everyday work purposes, such as communication, information seeking and knowledge sharing. However, they also raised concerns about information security and privacy aspects, in the physician–patient relationship, as well as collegial communication: “You often end up in uncertainty, as you mentioned earlier [refer to Internet and confidentiality]; it’s ridiculous really, that it feels safer by fax than by email …” (FG C, P13). There was also a concern among the participants about digital stress and information overload: “because we really need to be able to quickly check, so to speak, many things every so often” (FG A: P3). This can add to the workload, since the responsibility depends on discretionary activity of individuals.
In this theme, the main challenges concern data work, in terms of how physicians’ seek information and how they use data to learn and update professional practice. The new role of patients and patient-generated data, along with the introduction of social media in healthcare, provide the potential for shared learning opportunities and communication. Knowledge in this area is lacking, both on an individual level and in terms of organizational support and resources for practice, especially related to privacy and information security.
Professional role and responsibility—who should facilitate patient involvement?
The participants further discussed their concerns over boundaries regarding professional roles and responsibilities to patients. The following conversation illustrates this balancing act, expressed as a struggle between the constraints of the clinical practice setting and a sense of professional duty to provide answers to informed and uninformed patients alike: “It’s like the patients give us homework, but do we always have to do that homework?” (FG A: P3) “… well, we have a responsibility, of course, to keep updated […] not a responsibility to sit at night or in the weekends to answer patients’ questions …” (FG A: P4)
The physicians expressed mixed feelings about this development. Overall, they took responsibility for guiding or helping patients in medical matters, while in general showing ambivalence or uncertainty toward giving recommendations and advice, for instance on choosing health apps or providing technical support: “… I can tell the patient there is really good information here online [but] I’m not an Internet instructor, that’s not what I’m educated for, that’s not what I want to spend my time on …” (FG C: P13).
This was discussed as an opportunity for a new profession rather than a responsibility for the physicians: … It was a really interesting thought, the very first thing you [referring to FG C: P16] started with, about a new profession. I can see what you mean now … to have an IT-guidance of some sort, here at the healthcare center, responsible for learning and educating patients … (FG C: P13)
This issue is further accentuated in the context of digital healthcare, where patients not only Google their symptoms but also bring their own data. One physician commented: “That’s quite annoying to me when they order tests [online] and then I have to deal with that when it wasn’t even me who ordered the test” (FG A: P5). Participants talked about ethical aspects of consumer health technologies, referring to the risk for unnecessary treatments and examinations: “… medicalization or over-investigating … for things that are not illnesses” (FG B: P8). They pointed out inequities in access as to whether digital developments benefit all patients, or those already healthy and privileged: “… one must ask, is it Greta 89 that will have to wait …” (FG B: P8).
In this theme, the main challenges relate to how the new role of patients alter physicians’ work and the effects of patient-centric technologies on the clinical workplace. In particular, issues related to professional roles and responsibilities came to the fore, as previously established boundaries between public and private domains, medicine and technology, evidence-based medicine and home remedies have become increasingly blurred.
Manifestations of knowledge and expertise
Participants were well aware of the emerging new role of patients who participate in care and come prepared, knowledgeable about diagnosis and treatment options. They talked about different categories of patients within this context, as summarized by one of the physicians: … patients with issues that are obviously complete nonsense, where some newspaper scares them for example, and them we can calm down; then there are patients who come with non-medical issues, such as homeopathy, well then we can only tell them that this is not my area of expertise […] and then, there are the patients who come and are really familiar with their own illness, diabetes for example, who may have special knowledge that we don’t have, and these patients tend to themselves take responsibility because they are well aware of their disease, and in that case they know best. (FG A: P6)
The physicians expressed a generally positive attitude toward patients’ use of self-tracking and online information: “… probably these patients are more active and care about their health …” (FG B: P11), provided the information didn’t diverge much from standard medical practice. A challenge though is when there are conflicts of interest, for example regarding expensive treatments options or disagreements on how to interpret data: “… if the patient feels confident and self-diagnosis, but the healthcare doesn’t agree and resists …” (FG B: P12).
As reflected above, there is concern about the increase in “fake medical news” and misunderstandings: Whether from Internet searches or the use of self-care technologies, there is the risk of patients either trusting apps and not seeking medical advice or seeking advice based on misinterpretations of data: “… Official healthcare websites are one thing /…/ a skilled nurse, for instance, answering questions from people, but if patients would just ask each other …” (FG A: P1). The physicians expressed that they have an important role to provide an evidence-based approach: “We are like consultants, and we can only offer what we can offer, so to speak, which is our medical expertise, based on scientific thinking and proven experience” (FG A: P1).
The key challenge in this section is the emerging role of patients and how physicians balance the information patients bring against their own expertise, as well as the difference in the quality of outside information brought to the clinical setting. Clearly, there is an impact on the patient–physician relationship and traditional views of medical knowledge and expertise.
Discussion
For better or worse, flipped healthcare changes the professional practice of physicians and perceptions of professional roles and responsibilities. First, we identified a transition of the medical profession. The health informatics field is characterized by optimism about technology, contributing to mismatches between predicted and actual benefits.33,34 Besides frustrations with IT-centric approaches, our participants talked about health informatics as a dynamic facet of new work practices. IT-systems in healthcare historically were promoted as replacement for and automation of existing work tasks (e.g. scanning patient records and computerizing) intended to save time for clinicians. Similar arguments are put forward today, suggesting for example that mobile technologies may reduce time demands and strengthen the patient–physician relationship due to greater patient self-management and shared care. 35 In practice, however, the effect has often been the opposite, increasing the administrative burden instead. Participants confirmed common concerns among physicians about increased workload, ambiguity and time pressure. Our findings illustrate that new types of data work (e.g. social media and online knowledge sharing) are not considered work per se, rather as added tasks in an already busy workday. This discretionary work often occurs after attending to care work and daily practical tasks related to the patient.
It is important to distinguish between digital technologies for documentation and administration, and more exploratory technologies for finding knowledge or algorithms for treatment recommendations. The former are perceived as old-fashioned, poorly designed and a source of frustration. The physicians described digitalization and data work as beyond replacements for paper-based information. Described new benefits were support for collaboration, decision-making, continuous learning and staying current. They spoke of patient-generated health data as an underused resource and suggested digital solutions to improve general care. This suggests a change in attitude, where the benefit is now expected to exceed the risks.
Second, digitally informed and engaged patients are changing professional roles and responsibilities. The amount of medical knowledge now available was described as a dilemma for both physicians and patients, regarding how to use and prioritize different kinds of information. It is noteworthy that medical informatics and evidence-based medicine (EBM) emerged around the same time and overlap in many ways.36,37 Consistent with prior research, our findings show that physicians often encounter barriers when answering clinical questions and seeking information online.38–40 Medical information systems, for example, clinical support tools, tend to be organized by diseases, whereas information needs of physicians are focused on the patients’ symptoms. Integrating a patient-centered approach has been suggested as a solution to this mismatch. 41 Underlying aspects for patient participation, like features for shared decision-making, are uncommon today. 42 Our research also suggests a value in systematically incorporating patient experiences into tools that facilitate knowledge sharing and patient–physician collaboration. 26
In addition, social media and online networks change communication patterns among patients and physicians, enabling continuity of care beyond office visits.7,21 This brings new challenges for physicians, in terms of scope of responsibility, transparency, tone of the patient communication, and boundaries between private and professional. 43 As mentioned above, data-driven healthcare imposes new tasks on top of clinical work. Hence, as highlighted by participants in this study, there is need for new occupational roles not previously part of clinical teams such as statisticians, analysts, information professionals.44,45 These would allow healthcare professionals to focus on core tasks and patients, while acquiring new skills in practice.
As outlined in the third theme, manifestations of knowledge and expertise, established views of medical knowledge are challenged, along with the role of the physician as the expert and the evidence-based approach. The development of medical professional knowledge has traditionally been described as progressing from novice to expert per the Dreyfus model of skills acquisition. 46 In earlier research, we found that resident physicians often function as a source of updated medical as well as IT-related knowledge for senior colleagues. Thus, the more senior doctors often learn from younger colleagues. 30 Findings from this study illustrate how the nature of knowledge and expertise is challenged—or flipped—even more. Patients now enter into this equation, as they engage in discussions with peers and experts via online forums, and bring health data, lab test results and consumer apps to consultations.
While the benefits of access to updated, real-time data reduces the risk of mistreating patients, there exists the risk that over-informed patients, whether from online information or self-tracking, might reduce fairness in care to other patients and incur unnecessary treatments for themselves. Physicians are used to relying on science and proven experience. Consistent with that need, participants implied that new technologies and apps should reflect the standards of evidence-based medicine. While physicians have always had a role as interpreters of medical information, the responsibility to aid patients to a more critical appraisal of health data is increasingly important. Now they need to know the technology as well as knowing the patient.
In all, there are new opportunities for shared learning, where the physicians can inform the patients, as well as learning with and from the patients. This can actually include learning from other physicians and existing guidelines and so on through the patients. Patients may share other patients’ experiences and the advice of their respective doctors. Then the expert patient becomes a messenger or a filter for the volume of information of the kind that the physicians demand. This in turn requires that the physician trust the patient’s expertise and ability to find reliable sources. Our findings suggest that patients who manage this technique could be a rich resource and curate public medical informatics platforms. There remains a concern about what may happen if patients become more proficient than the physician. 20
Finally, revisiting the analogy between the idea of flipped healthcare and the educational notion of a flipped classroom, we find that the digital transformation in both domains connotes a more interactive relationship between patients/physicians and students/teachers. However, the effects of patient-centric technologies may—for better or worse—be more fundamental, as some patients become significantly more authoritative in their own care, whereas the flipped classroom describes a redistribution of passive and interactive elements of teaching. Consistent with previous research, we believe that it is not enough to focus on whether patient-centric technologies are used. 13 The incorporation of these technologies into complex environments like healthcare demands a reflective and critical understanding of how they integrate with everyday practice. As Lehman 47 points out, shared decision-making needs more than just knowledge; there is a need for a different mind-set among clinicians, access to tools, inclusion in medical school curricula, and a different medical culture in general.
Our findings point to increasing demands for critical thinking and ethical considerations, expressed in the interviews as a transformation of the profession, beyond individual IT skills and training in EBM. Abilities such as evaluation, negotiation and adapting knowledge to the individual patient become increasingly important. Critical appraisal and evaluation of sources was emphasized by the participants; this is now included as mandatory in the curriculum. But, pedagogical, reflective and communicative skills will grow in importance and need to be extended to include digital channels. Ethical and legal knowledge around information security and patient confidentiality is critical, both as continuous training for physicians and as expert functions in the organization. Statistics and data analysis was also highlighted by the physicians, including how to explain the “meaning of numbers” for the patients.
Findings from this study further show how different aspects of everyday digital technologies co-exist, sometimes in parallel and sometimes as conflicting perspectives. This was expressed in contradictory statements from the participants. On one hand, there was the view that IT is just as integrated in care as the doctor’s stethoscope. At the same time, they struggled with defining ethical and legal boundaries added to their responsibilities as individual physicians. It is well known that the healthcare sector is complex with a long tradition of hierarchal structures, and resistance to change. As described by Aanestad et al., 48 eHealth infrastructures have the dual character of transformative orientation toward reshaping roles and relationships, while at the same time need to control and fit the existing healthcare environment. The duality of views from the physicians’ perspective uncovers issues related to the shift in healthcare at large, beyond the immediate work practice. Patient-centric technologies thus create tensions between allowing for flexibility and ensuring patient safety and quality of care.
Conclusion
The focus of this article has been on the notion of flipped healthcare, with the aim to explore how resident physicians view their role and practice in relation to informed patients and patient-centric technologies. The paper illustrates how the new role of patients alters physicians’ work and use of data to learn and update their professional practice. It suggests new possibilities for developing collegial competence and using patient experiences more systematically.
In short, our findings show that flipped healthcare certainly has the potential to improve healthcare, but demands substantial changes and challenges for the healthcare system and professions. Training in how to use and make use of patient-centric technologies is important but not sufficient. There is a need for new professional competencies in everyday data work, along with a change in attitudes, newly defined roles, and better ways to identify and develop reliable online sources. Finally, the role of patients, not only as consumers but also producers of healthcare, is a rather formidable and complex cultural change to address.
Footnotes
Appendix 1
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.