
Abstract
This study investigated the association between care continuity and chronic conditions in relation to highly frequent use of outpatient service in order to find constructive suggestions to bring efficient, high-quality care for patients with multiple chronic conditions. The National Health Insurance database was used and 333,294 patients were identified from 2007 to 2009. The continuity of care index indicates the dispersion of a patient’s ambulatory visits among providers. Multivariate logistic regression was used to estimate adjusted odds ratios with 95 percent confidence intervals. Continuity of care index was significantly associated with age, sex, urbanization level, socioeconomic status, emergency department visits, hospitalization, psychological disorders, chronic diseases, and catastrophic illness card; those with low continuity of care index were likely to use outpatient care highly frequently. Improving continuity of care is fundamental, and the best way is to advance the practice of family medicine for primary care.
Introduction
There has been a growing demand internationally for medical care, which brings increasing challenges to healthcare systems of organizing, financing, and distributing medical resources. In Taiwan, for example, with population aging and increases in grave diseases, the average annual increase in outpatient visits was 1.51 percent from 1997 to 2011; the average number of outpatient visits per person is now around 15 and 8.06 million people visit doctors for over 15 times every year. 1 The National Health Insurance (NHI) system also helped with the increases since it made medical care more accessible.2,3
Among all patients, those with multiple chronic conditions (MCCs) are the most frequent users of medical resources. Unfortunately, MCC patients are on the rise, affecting a wide range of aspects in healthcare. Previous studies have shown that the number of a patient’s chronic conditions is positively correlated with the average number of the patient’s annual prescriptions and hospitalizations.4–6 Unfortunately, MCC patients need care services from multiple specialized departments, which, in a system that lacks integration of medical services, leads to waste of medical resources and subjects patients to problems associated with multiple medications.
Continuity of care has been shown in many studies to be associated with decreases in emergency visits7–9 and in frequency of hospitalization,10,11 as well as with favorable physician–patient relationships, patients’ satisfaction of and trust of the providers, and improved health outcomes of the patients due to the providers’ familiarity with their health conditions and emotional demands.12–14 Meanwhile, it may also encourage the patients to participate in preventive services such as cancer screening. 12 In contrast, fragmented care from multiple providers result in repeated clinical tests. 15 Since MCC patients generate an excessively high proportion of medical expenditure 4 and often go through repeated medical procedures, 6 we began to wonder whether care continuity would benefit them.
Meanwhile, Taiwan’s bureau of NHI started a counseling program in 2001 to help frequent outpatient users to rationalize their uses of medical resources in order to improve the efficiency of medical services. While the effect of counseling was still unclear, we wondered whether interventions along the line of promoting continuity of care would get us closer to rational use of medical services. We therefore started with the NHI database to investigate the relationships between care continuity and chronic conditions, how it impacted the number of outpatient visits, and risk factors of highly frequent uses. We aimed to find constructive suggestions that could help bring efficient, high-quality care for MCC patients.
Methods
Data sources
This study analyzed the nationwide population-based data derived from the National Health Insurance Research Database (NHIRD) in Taiwan. The database is maintained by the National Health Research Institute and the Bureau of NHI for research purposes and covers more than 99 percent of the population (about 23 million). We used the Longitudinal Health Insurance Database 2010 (LHID 2010) which was a subset of the NHIRD containing the information of 1,000,000 patients randomly sampled from all enrollees. The database encrypts personal information for privacy protection and provides researchers with anonymous identification numbers associated with relevant information. The Institutional Review Board (IRB) of Kaohsiung Veterans General Hospital approved this study (VGHKS15-EM10-02).
Study population
The study population comprised patients who had at least one internal medicine outpatient visit during the period from 2007 to 2009. Patients who were not continuously enrolled in the NHI program or had no internal medicine outpatient visits during the study period were excluded. Furthermore, patients with less than four outpatient visits during the continuity of care index (COCI) period (defined below) were excluded. In total, 333,294 patients were included. The index date was set as the earliest date of each patient’s outpatient visits in 2008. The previous year before the index date was the COCI period, and the year following the index date was the outcome period.
We chose the COCI by Bice and Boxerman 16 instead of other commonly used indicators, such as the usual provider continuity (UPC) index. The COCI is composed of the number of different physicians seen and the number of visits to each physician in each year during the study period. The COCI score, ranging from 0 to 1, reflects the dispersion of a patient’s ambulatory visits among providers. A higher value represents better care continuity. A COCI of 1 indicates that the patient has visited the same physician throughout the measured time; in other words, the patient had a continuous connection with one physician. This index has been widely adopted in studies using claim data sets because the index is not sensitive to the number of physician visits and suitable for studies involving a high number of outpatient visits. 1 The equation to calculate COCI is as follows
where N represents the total number of physician visits, nj is the number of visits to the same physician j, j is the given physician, and M is the number of providers.
We calculated the patients’ COCI scores during the COCI period and then categorized them into three groups according to the scores: 1 low (COCI < 0.36), moderate (0.36 ⩽ COCI ⩽ 0.99), and high (COCI = 1). The clinical characteristics, emergency department (ED) visits, number of hospitalizations and psychiatric disorders in the COCI period, as well as whether the patients had catastrophic illness cards in the past were identified. We used the codes of International Classification of Disease, Ninth Revision, Clinical Modification (ICD-9-CM) to obtain information. The Charlson comorbidity index (CCI) was calculated for each patient in the COCI period based on his or her outpatient and inpatient records. The CCI was also divided into three groups: 0, 1, and ⩾2.
Definition of outcome
All of the internal medicine outpatient visits in the outcome period were analyzed to calculate the number of outpatient visits for each individual. According to the distribution of the frequency of outpatient visits shown in our study, we defined the subjects with more than 51 visits as high users of outpatient care.
Statistical analysis
The chi-square test was used to identify the correlation between categorical variables, that is, age, sex, urbanization level, socioeconomic status, ED visits, hospitalization, psychiatric disorder, and catastrophic illness in the past year, CCI scores, and comorbidities. Multivariate logistic regression models were used to estimate adjusted odds ratios (ORs) with 95 percent confidence intervals (CIs). The statistical analyses were carried out using SAS® 9.4 (SAS Institute Inc., Cary, NC, USA). A p-value of less than 0.05 was considered to be statistically significant.
Results
The severity of increasingly frequent use of outpatient service is illustrated in Figure 1. As shown in the figure, while the total number of patients in the internal medicine outpatient department remained stable during 2006–2009 in Taiwan, the proportion of frequent users (⩾51 visits) increased steadily. These numbers speak for the necessity of this study.
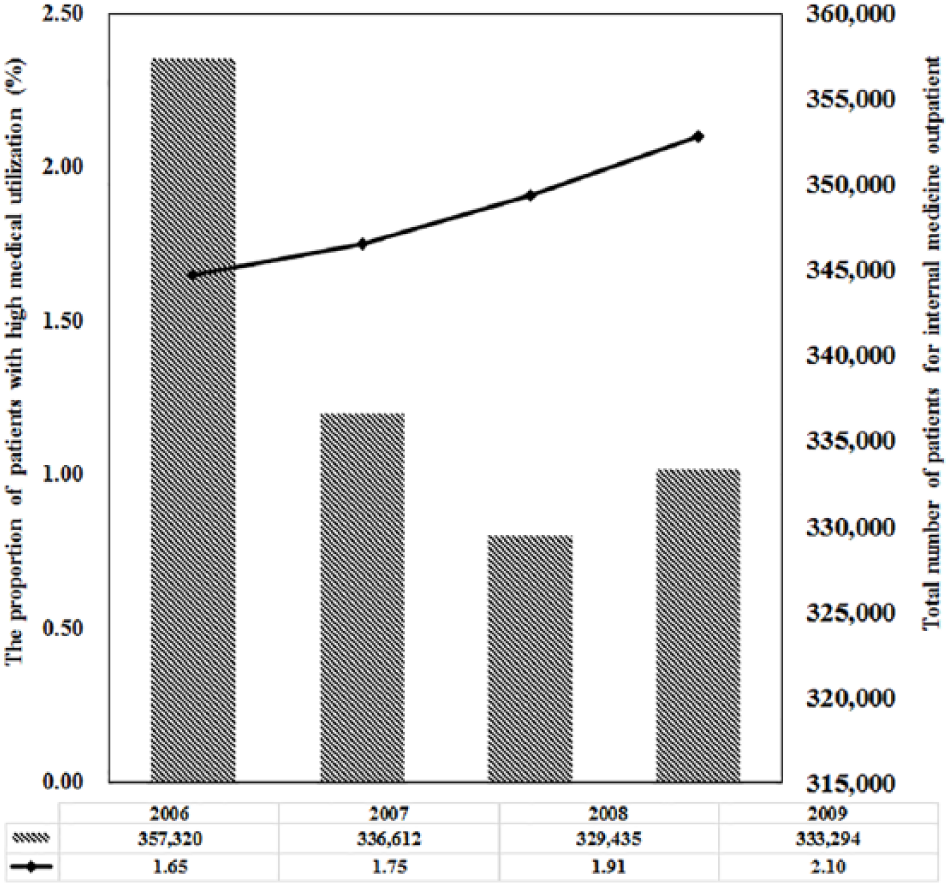
The proportion of patients with high medical utilization in outpatients care (⩾51 visits) for internal medicine outpatient during the period 2006–2009.
We identified a total of 333,294 subjects in this study, and the characteristics of them by the COCI group are shown in Table 1. There were 138,981 (41.70%), 141,791 (42.54%), and 52,522 (15.76%) subjects in the low-, moderate-, and high-level COCI groups, respectively. In the cohort, 14.30 percent of the subjects were aged below 18, 27.91 percent in the range of 18–44, 35.58 percent in the range of 45–64, and 22.22 percent were aged 65 and above. Furthermore, 52.66 percent of the subjects were female, 41.43 percent lived in suburbs, 51.40 percent had a low income, and 5.02 percent had catastrophic illness cards.
Demographic characteristics of subjects by continuity of care index group.
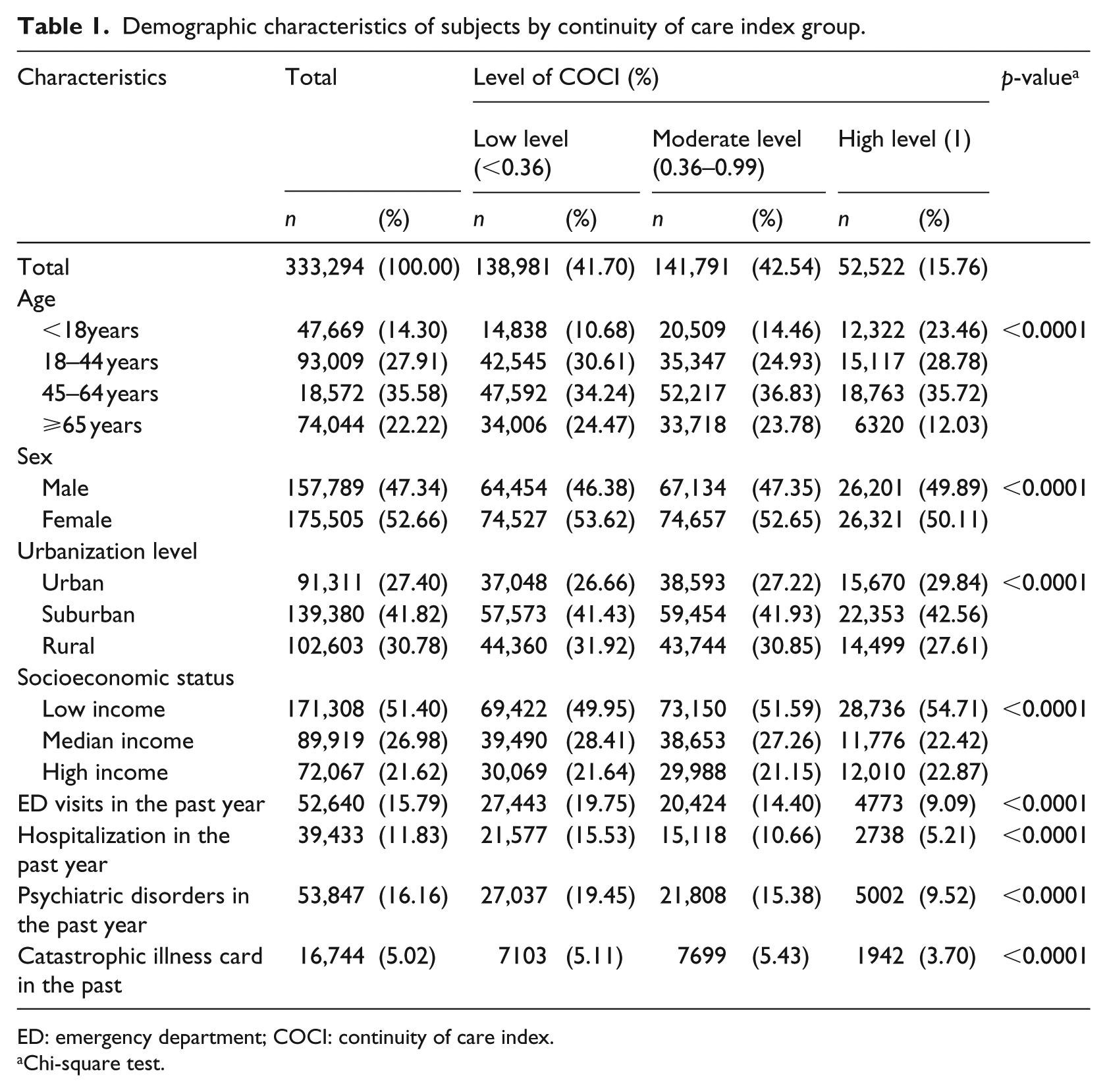
ED: emergency department; COCI: continuity of care index.
Chi-square test.
Significant correlation was found between COCI scores and age (as grouped above), sex, urbanization level, and socioeconomic status. Significant correlation was also identified between COCI scores and ED visits (9.09% visited ED in the COCI period), hospitalization (5.21% were hospitalized for at least once), psychiatric disorders (9.52% had one or more), and possession of a catastrophic illness card (3.70% had one). Regarding comorbidities (Table 2), the proportion of the patients with ⩾2 CCI scores was lower in the high COCI group than in the low and moderate COCI groups. Moreover, COCI was significantly correlated not only with CCI scores, but also with individual comorbidities.
Comorbidities of subjects by continuity of care index group.
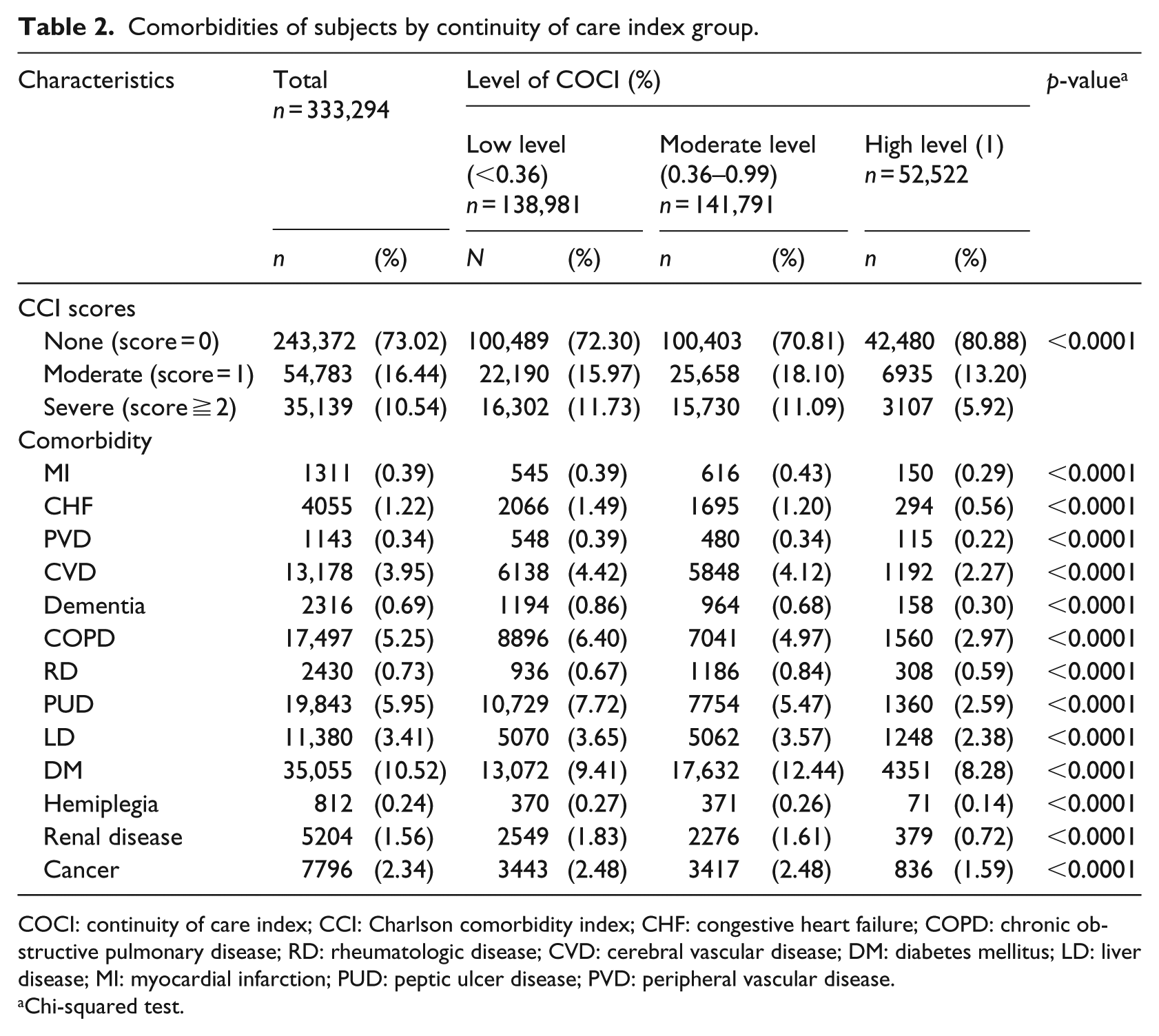
COCI: continuity of care index; CCI: Charlson comorbidity index; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease; RD: rheumatologic disease; CVD: cerebral vascular disease; DM: diabetes mellitus; LD: liver disease; MI: myocardial infarction; PUD: peptic ulcer disease; PVD: peripheral vascular disease.
Chi-squared test.
As there has been a growing trend in highly frequent use of outpatient services (Figure 1), we analyzed the above variables in order to identify the risk factors of the use. As shown in Table 3, after adjustment for all the other covariates in the table, the patients in the low and moderate COCI groups had a significantly higher risk of the use than did the patients in the high COCI group (OR = 2.38, 95% CI = 2.12–2.68 and OR = 1.96, 95% CI = 1.74–2.21, respectively). In addition, patients aged 65 and above (OR = 11.11, 95% CI = 9.08–13.59), males (OR = 1.22, 95% CI = 1.16–1.28), those who lived in rural areas (OR = 1.37, 95% CI = 1.28–1.47), those who had a low income (OR = 1.94, 95% CI = 1.76–2.13), and those who had ED visits (OR = 1.35, 95% CI = 1.28–1.44), those who were hospitalized (OR = 1.44, 95% CI = 1.36–1.53), those with psychiatric disorders (OR = 2.32, 95% CI = 2.20–2.44) in the COCI period, and those who had severe comorbidities (OR = 3.03, 95% CI = 2.84–3.23) were more likely to use outpatient care highly frequently.
Multivariable analysis of the risk of high medical utilization in outpatient care associated with each variable.
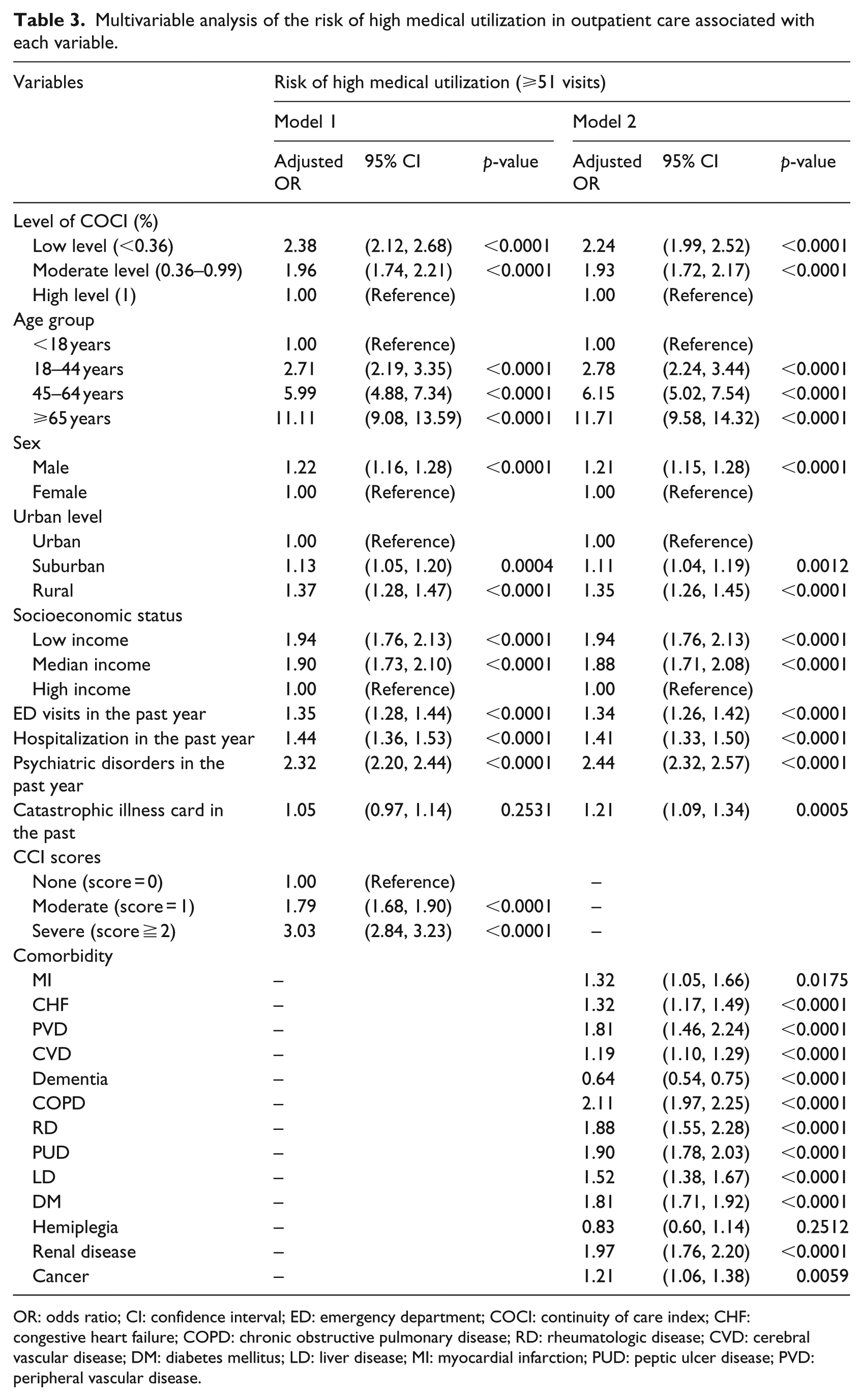
OR: odds ratio; CI: confidence interval; ED: emergency department; COCI: continuity of care index; CHF: congestive heart failure; COPD: chronic obstructive pulmonary disease; RD: rheumatologic disease; CVD: cerebral vascular disease; DM: diabetes mellitus; LD: liver disease; MI: myocardial infarction; PUD: peptic ulcer disease; PVD: peripheral vascular disease.
Furthermore, patients with any comorbidity were more likely to have highly frequent use of outpatient care except those with hemiplegia (p > 0.05) and those with dementia who had a lower risk (p < 0.0001).
Discussion
The strength of this study is that the design included an unbiased patient selection process. The key findings in our study are as follows. First, only 15.76 percent of the study population was in the high COCI group, suggesting that most patients lacked continuous care from the same providers. Given that highly frequent users of outpatient services have been on the rise, it is high time to rationalize use of medical resources. In addition, among the patients in this study, there were distinctive distributions of COCI by age, sex, urbanization level, and residential location. Second, the patients in the high COCI group had lower CCI scores than those in the moderate and low COCI groups. Third, we found a significant impact of COCI on the patients’ number of outpatient visits after all the other variables were controlled for.
Continuity of care is a centerpiece of accountable care organizations (ACOs) and patient-centered medical homes (PCMHs) and considered to be indispensable for high-quality primary care.17,18 In fact, patients in Taiwan are often criticized for their doctor-shopping behavior, since it potentially exposes the patients to misuse and duplication of medications, while it hinders information sharing or mutual trust between patients and physicians and may reduce patients’ COCI.1,19,20 It is therefore particularly important for the healthcare system in Taiwan to invest in the improvement of care continuity. Meanwhile, efficient use of medical resources has always been a centerpiece of national health policies in Taiwan as well. The NHI bureau initiated a counseling program to rationalize the use of medical resources by highly frequent hospital users in 2001, which was also aimed to improve the quality and convenience of medical services under limited budgets. 1 Unfortunately, however, whether health counseling may help rationalize the use of medical resources remains unclear. This study explored the association between continuity of care and frequent use of outpatient service in attempts to find whether the former would bring the rational use desired by policymakers.
We found that the number of highly frequent hospital users increased from 2006 to 2009, and among the more than 130,000 frequent users, nearly 85 percent lacked care continuity and only 20 percent were older people. The findings of this study may help direct efforts of rationalizing use of medical resources to the right place.
The latter finding was contradictory to the notion commonly held that only the elderly tended to use medical resources excessively, 2 and future efforts of rationalizing medical resource use should not ignore younger patients. In addition, about half of the patients in this study were of a low socioeconomic status and about 40 percent lived in suburbs. We also investigated the medical history of all the patients in the year prior to the study’s index date, including chronic obstructive pulmonary disease, psychological disorders, and hospitalizations and found that the patients with catastrophic diseases were mostly distributed in the low and moderate COCI groups. These findings of the study thus illustrated a clear picture where to invest further efforts in order to help the highly frequent users rationalize their use of medical resources.
This study also found that the patients in the high COCI group had fewer comorbidities than those in the low and moderate groups and that COCI was significantly correlated with comorbidities, which echoed the literature. Previous studies have associated fragmented care from multiple providers with duplication of services, medication, diagnostic tests, and procedures.21–23 In contrast, integrated care by a single provider or a team of providers was found to be associated with better experiences reported by patients24,25 and fewer hospitalizations.11,25,26 In fact, management of comorbidities has become a global challenge to healthcare systems, impacting national treasuries and various socioeconomic aspects around the world. Given that interactions between MCC patients and providers may involve complex medication management, it is probably more efficient to focus the efforts of improving care continuity on the provider party who prescribes essential medications for chronic conditions. 27 Meanwhile, primary care provided by family medicine may also bring improvement in the continuity of care for patients and healthcare policies may consider promoting the practice.
Our investigation identified ages higher than 65, males, residence in rural areas, low socioeconomic status, psychological disorders, and high CCIs to be significant risk factors for highly frequent use of outpatient services when confounding factors were controlled for. In addition, all the individual comorbidities were significant risk factors with only two exceptions: hemiplegia, which was not significant, and dementia, which put the patients at a significantly lower risk presumably because the disease restricted the patients from ambulatory visits. Future efforts to lower the frequency of outpatient use may target the aspects represented by these factors.
There are also limitations to this study. First, family history of diseases, life styles, and environmental information are not included in NHIRD, but they may all impact a patient’s habit of using medical resources. Next, the outcome period in this study is not very long and there is also lack of well-structured follow-up interviews with the patients. Future studies may need much longer follow-up periods.
Conclusion
We found that only a small proportion of the highly frequent users of outpatient services were 65 or above, that COCI was significantly associated with age, sex, urbanization level, socioeconomic status, ED visits, hospitalization, psychological disorders, and catastrophic illness card, that the patients with poor continuity of care were likely to visit the outpatient department highly frequently, and that a combination of age, sex, socioeconomic status, psychological disorders, chronic conditions, and care continuity could reliably predict the risk of highly frequent use of medical resources. To rationalize the use and distribution of medical resources, we propose to provide education to younger patients, those living in rural areas, those with psychological disorders, and those with MCC. In addition, improving continuity of care is also fundamental, and the best way to achieve the goal is to advance the practice of family medicine for primary care.
Footnotes
Acknowledgements
We thank BNHI and NHRI in Taiwan for providing the NHIRD as our research database. We are also grateful to the Research Center of Medical Informatics, Kaohsiung Veterans General Hospital, for data management and statistical analysis. C.W., H.-C.K., P.-L.T., and S.-F.C. contributed equally to this work.
Author’s Note
Pei Ling Tang is also affiliated with Fooyin University.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was supported by a grant (VGHKS103-G02) from Kaohsiung Veterans General Hospital, Taiwan (R.O.C.).