
Abstract
Although investment in healthcare technology is rapidly increasing, the readiness to use emerging technologies among healthcare professionals is still low. The present study relies on an integrated model derived from the unified theory of acceptance and use of technology and the diffusion of innovation model to assess the factors that predicted healthcare professionals’ intentions to use healthcare information systems. Using a cross-sectional correlational design, 105 healthcare professionals (M age = 41.06, standard deviation = 9.18; 49% consultants and General Practitioners (GPs); 56.2% females) from hospitals in England completed online structured questionnaires. One-way analysis of variance showed that there were no differences in healthcare information systems usage intentions, unified theory of acceptance and use of technology and diffusion of innovation variables between consultants/GPs and non-medical staff (i.e. nurses and administration staff). Linear regression analysis demonstrated that the integrative model predicted 78.1 per cent (adjusted R2) in intentions to use healthcare information systems, and variables from both unified theory of acceptance and use of technology and the diffusion of innovation had significant effects. Moderated regression analysis further revealed that the interaction between voluntariness and effort expectancy, and voluntariness and social influence significantly predicted usage intentions on top of the main effects of the individual predictors. This poses direct implications for both practice and theory in this field. Future research should consider the predictive validity of integrative theoretical models of technology acceptance and utilization in healthcare settings.
Keywords
Introduction
Healthcare information systems (HIS) are often portrayed as precious tools which can enable better quality and safety of healthcare and make the whole process of patient treatment more efficient. HIS are expected to collect, store, analyse, and provide information about the patient to caregivers, thus, enabling better decision-making and timely actions with respect to treatments and the provision of healthcare services. 1
Although technical expertise may present one of the barriers to technology acceptance in healthcare, a large body of research has indicated that social and psychological barriers to technology acceptance are also important.2,3 Even though technology acceptance represents a constant challenge in other business sectors, it is especially pertinent to healthcare environment.4,5 Specifically, the introduction and utilization of comprehensive HIS, dealing with the core processes of healthcare organizations can be particularly challenging 6 because it requires changes in the established patterns of behaviour, as well as the implementation of sophisticated tools and technology.
Emerging and ongoing challenges faced by the modern healthcare organizations, such as an ageing workforce, financial pressures, budgetary cuts, and staffing issues, as well as increased public demands for high-quality healthcare services, make it even harder to effectively introduce and utilize novel technologies for effective healthcare management. 7 One way of overcoming those challenges and optimizing technology acceptance and utilization is to better understand the ways employees and other stakeholders in healthcare organization perceive, evaluate, and decide to use novel technologies. Considering the extensive resources invested in Healthcare Information Technology projects8–10 and the ensuing added value for the healthcare organizations and the patients, it is very important to understand the factors driving the successful deployment of the IT in healthcare settings. To this end, behavioural and social cognitive models of technology acceptance have proven particularly useful.
Characteristics of technology introduction in healthcare environment
One of the main barriers for introducing technology in the healthcare environment is the growing complexity and variability in the process of providing health and care. 11 Unlike in some other industries where processes can be fully standardized, healthcare is characterized by high variability from case to case. In addition, specialty-specific or department-specific processes further increase the variability and heterogeneity of healthcare services and this makes it harder to map those processes into a health information system.
As Barach and Johnson noted,
12
Healthcare systems are best described as complex adaptive systems. As such, they are a collection of individuals who are free to act in ways that are not totally predictable. (p. i10)
It is also common that information systems are increasing complexity by creating additional tasks and by requiring additional skills from healthcare staff, which are often already overwhelmed with daily challenges in healthcare provision. As explained by Dekker, 13 new information networks are creating new roles and change existing human and organizational links.
As the expectations of the clinical information systems (CIS) are raised and significant financial investments are made in their development and implementation, it is not surprising that academics and practitioners are seeking to gain better understanding of what are the key factors influencing acceptance of these systems, and how they can be used to modify outcomes. The technology acceptance model (TAM) provides a sound framework for recognizing, assessing, modelling, and potentially modifying those factors.14,15
In their meta-analysis, Schepers and Wetzels 16 found that the context (e.g. type of industry) and the type of technology in question can differentiate the process of technology acceptance that is described in the TAM. Several scholars have investigated the acceptance and use of technology in the healthcare environment3,17,18 and argued that technology acceptance in this context is different from that in other contexts and types of industry.
Ketikidis et al. 18 used TAM2, a variant of the original TAM, to predict healthcare professionals’ intentions to use electronic health records and found that perceived ease of use had a stronger correlation to technology acceptance than perceived usefulness (PU). This is different from most of the findings in other industries, where PU seems to have higher impact on acceptance. Some other findings on physician population suggest that perceived ease of use was less related to the level of acceptance.19,20
Furthermore, in their review of the studies related to the physicians’ acceptance of healthcare technology, Yarbrough and Smith 19 note that due to specific professional training and work environment, physicians cannot be expected to behave in the same way as the users in other, more commercially oriented branches. Therefore, theoretical models used to predict technology acceptance in this population should be adopted accordingly and reflect the particularities of the given context.
Hennington and Janz
17
used the unified theory of acceptance and use of technology (UTAUT), a theoretical extension of the original TAM, and identified several typical barriers that could hinder adoption of the CIS: The uncertainty of financial return on EMR investment, misalignment of EMRs with existing business processes, the relationship between EMRs and improved quality of care, increased effort on the part of EMR users, the physician/payer relationship, financial resource constraints, and time constraints. (p.65)
Some of these barriers are possibly more relevant in US health environment, where the study originates, but they provide excellent illustration on types of challenges to be considered when introducing CIS. Holden and Karsh 3 also highlight specific nature of the healthcare environment and opportunities to understand better ‘… salient beliefs that clinicians have about using health IT’ (p.14).
Through an enhanced understanding of specific motivating factors and inherited beliefs of clinical staff, the models used to predict and explain acceptance of technology could become more reliable and robust, and therefore easier to adopt in relevant projects.
Although TAMs derived from the TAM tradition (e.g. TAM, TAM2, UTAUT) have provided useful insights into end-users’ readiness to adopt a new technology, still they tend to be rather static in their approach by overlooking dynamic processes and flows that may also influence technology acceptance. One such process is the influence of early adopters/users of technology on the more widespread use of a new technology in a given setting. In fact, early adoption of technology by certain individuals in an organization can influence more general perceptions of usefulness and anticipated effort among people who have not yet used the technology in question. This process is described in the diffusion of innovation (DoI) theory, which highlights the importance of early technology adopters/users leading the way for more widespread technology use in an organization.21,22
Several studies have explored the applicability of DoI in the adoption of electronic patient record,23,24 but they have done so without controlling for the variables described by the models of the TAM tradition. On the other hand, López-Nicolás et al. 25 suggested that there is a growing body of research for integrating TAM and DoI, but still with limited content in professional contexts. This is obviously a very interesting area as it could shed more light on the technology acceptance variables that could be dynamically affected by diffusion processes, like social influence and perceived benefits. Although social influence is analysed within TAM2 and UTAUT models as a measure of social acceptance and potential use of technology by others, it is still an underappreciated source of influence on technology acceptance. Finally, Lo and Weng 26 found that the so-called Bandwagon effect had a positive influence on technology adoption in hospital environment, and that positive performance experiences positively moderate adoption. These findings seem to resonate with the premises of the DoI model.
Academic Models for Technology Acceptance
Technology acceptance model
TAM is the most commonly used and researched model for technology acceptance. Davis 27 originally introduced it, with the intention to explain factors leading to users’ behavioural intention (BI) to use Information Technology. He proposed two main variables that influence this intention – perceived ease of use (PEU) and PU, as shown in Figure 1. This model is based on the psychological theory of reasoned action (TRA) which explains behaviour in wider context.28,14
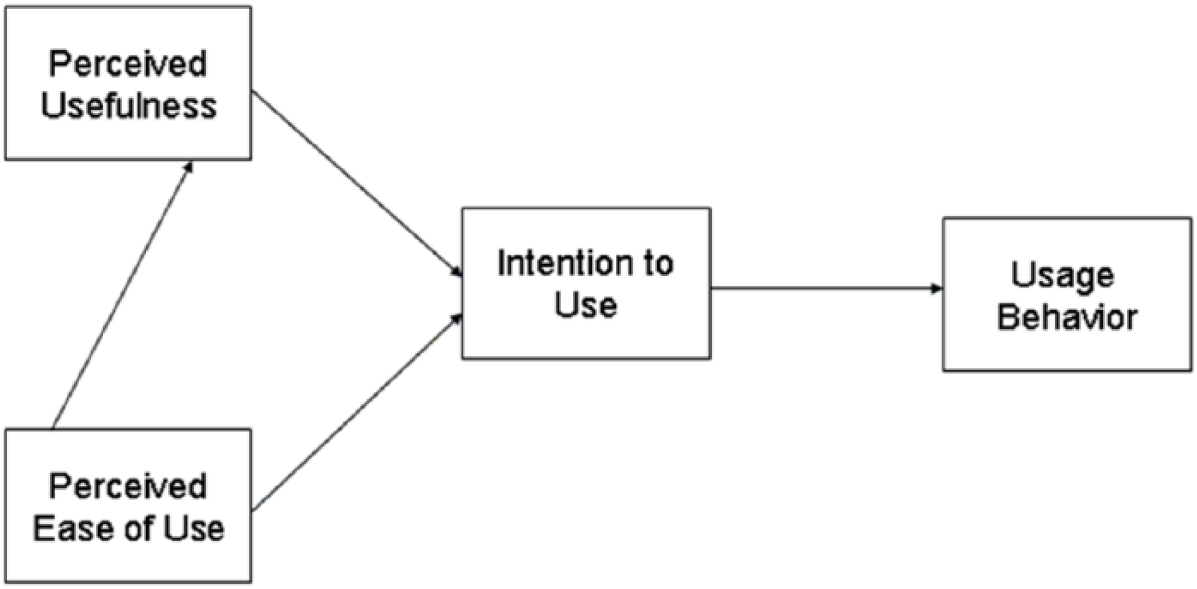
Technology acceptance model, based on Davis. 27
Davis 27 defines PU as ‘the degree to which a person believes that using a particular system would enhance his or her job performance’ (p. 320). Therefore, subjective impression on how much technology can improve results for the person or the organization. He also defines PEU as ‘the degree to which a person believes that using a particular system would be free of effort’ (p. 320). 27
Traditionally, TAM is studied through self-reported questionnaires and acceptance is understood as a stronger intention to utilize the given technology – although intentions to use technology and actual usage may not correspond, and this is one of the main criticisms of the TAM approach.15,29 Notwithstanding those limitations, a large body of research has supported the main theoretical tenets of TAM across business sectors and professional environments.14,30
Extended TAM – TAM2
As mentioned above, there were several proposals to improve the original TAM, usually by adding additional variables, but the most important update was introduced by Venkatesh and Davis, 31 known as TAM2 model. The extended model introduces two groups of variables that are influencing PU and intention to use technology in question – social influence processes and cognitive instrumental processes (Figure 2).
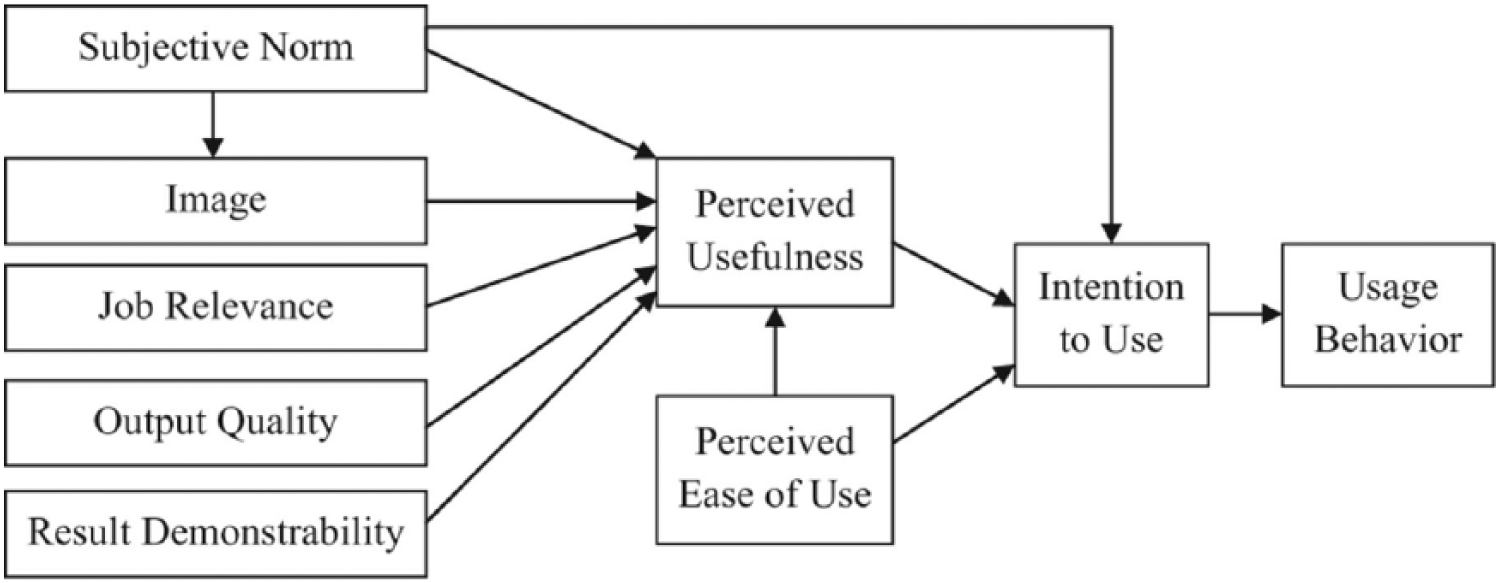
TAM2, based on Venkatesh and Davis. 31
Subjective norm is a key social influencing process, and it is defined as the theories of reasoned action and planned behaviour and reflect ‘perceived social approval of referent others for a given behaviour’ (p. 302). 32
Unified theory of acceptance and use of technology
Based on the comparison and testing of various acceptance models, Venkatesh et al. 33 proposed a new model with the idea to combine proven variables and relationship from eight different models. They named it the UTAUT.
UTAUT is based around four variables – performance expectancy, effort expectancy, social influence, and facilitating conditions. These variables, together with key moderating influences – gender, age, experience, and voluntariness of use – determine BI and actual usage of technology (Figure 3).
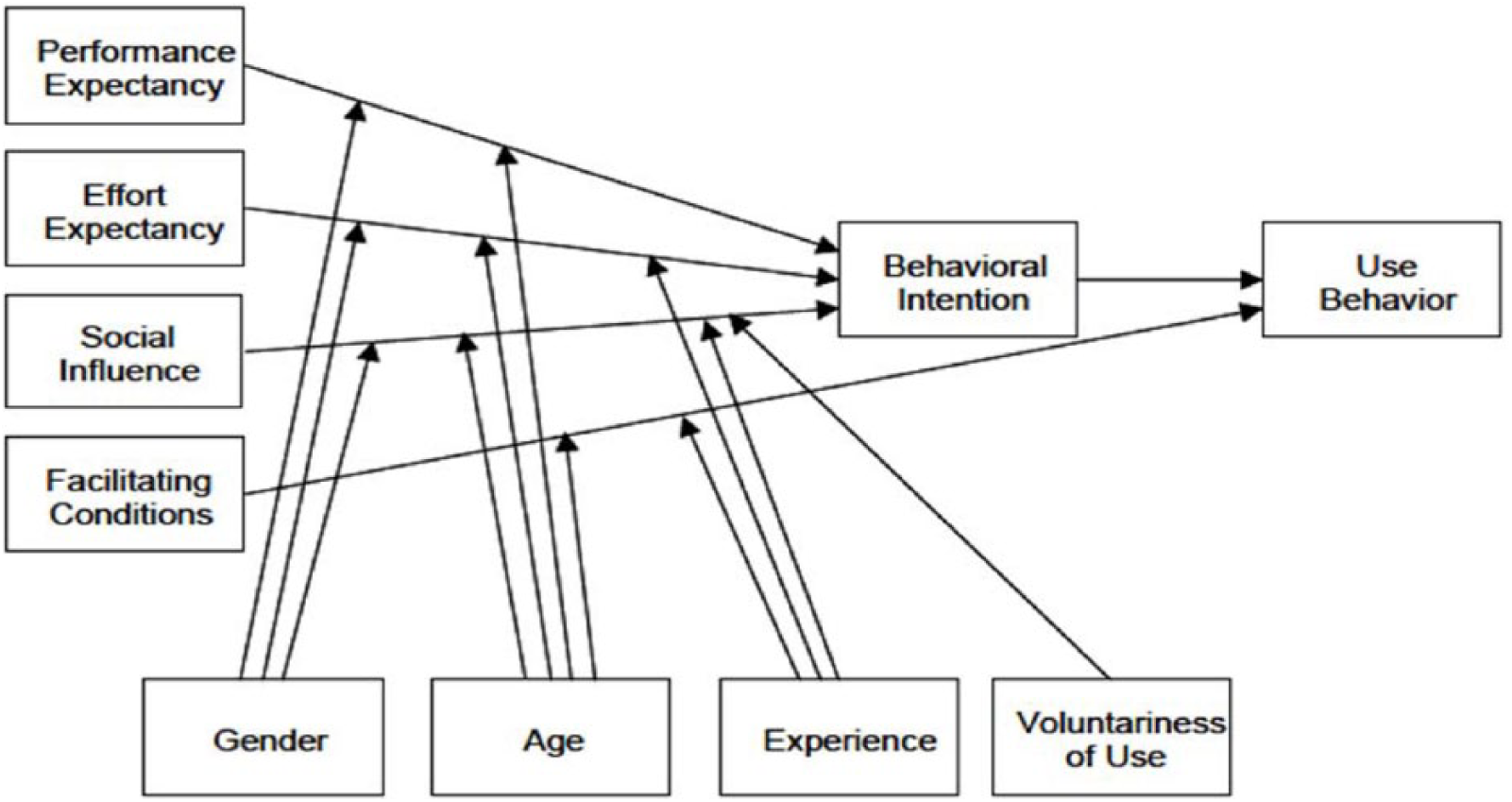
The UTAUT model. 33
Hennington and Janz 17 used the UTAUT to predict intentions and actual usage of the electronic medical records (EMRs) in a healthcare environment. Venkatesh et al. 34 have extended this model again, into the so-called UTAUT2, adding additional constructs that should reflect more closely consumer context – hedonic motivation, price value, and habit.
In a revision of the UTAUT for EMR adoption in healthcare, Venkatesh et al. 35 simplified the original structure of the model, by retaining only age as a key moderator variable of the associations between UTAUT variables and usage intentions. They argued that medical practice is characterized by a high degree of autonomy and it is difficult to impose any changes that physicians perceive as irrelevant to their work. They also noticed that the degree of disruption introduced by a new technology is important for technology acceptance. For example, the computerized physician order entry system (CPOE) has been met with less resistance, because it facilitates healthcare processes without disrupting the normal workflow. On the other hand, various decision support tools, which interfere directly with healthcare practitioners’ work, may evoke greater resistance, and, therefore, reduced technology acceptance.36,37
Diffusion of innovation theory
Almost 50 years ago, Rogers 21 introduced the DoI theory, which focuses on analysing the channels for communicating innovation among members of a given social unit. DoI is essentially considered to be a form of communication where the content is the idea/change being implemented (Figure 4).
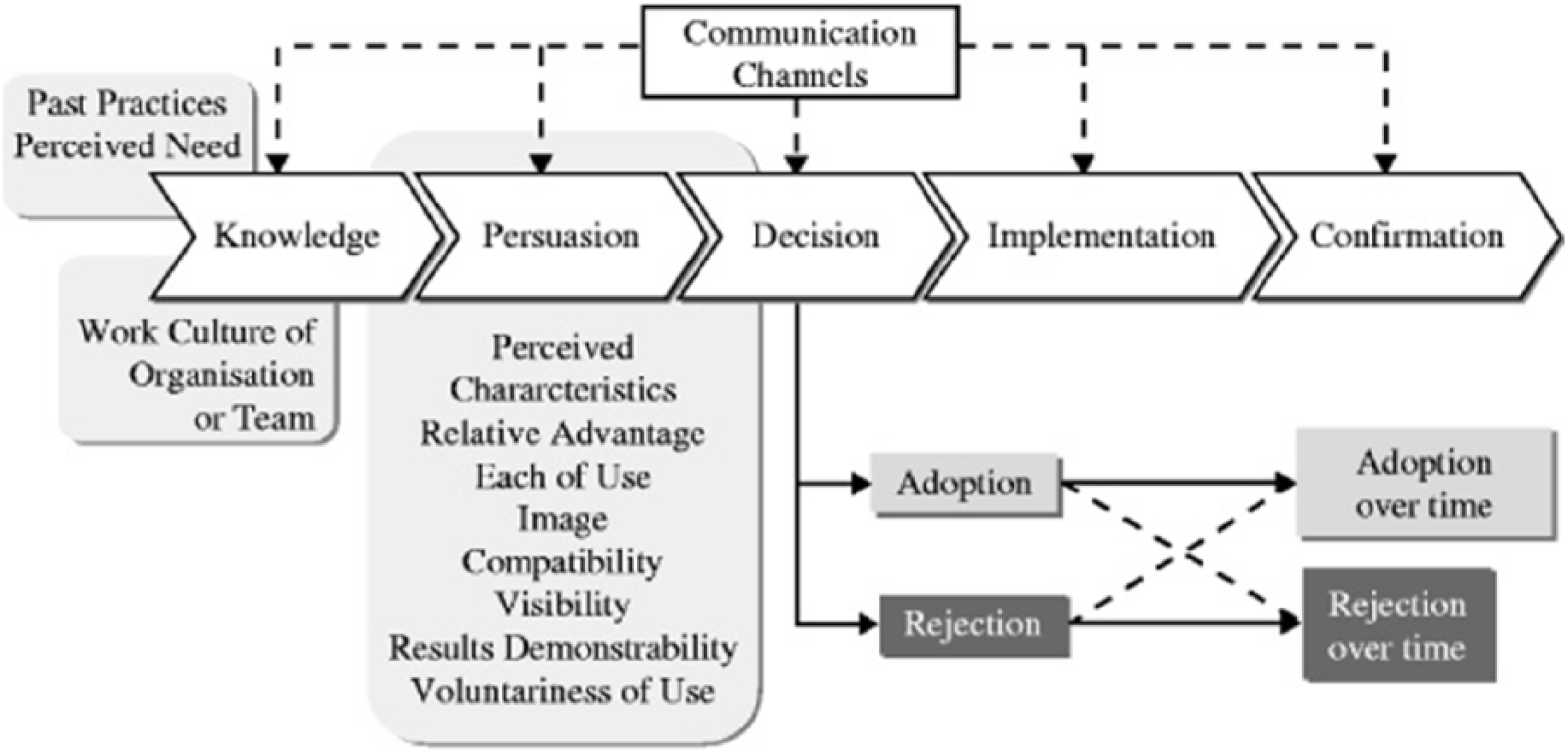
Communication steps and influencing factors in the process of innovation acceptance.
As Haider and Kreps 38 concluded, DoI analyses the interactions among four major factors, namely innovation, communication channels, social systems, and time. A large body of research has used DoI across professional contexts and innovation outputs.
Rogers 21 argued that key characteristics of the innovation that determine its adoption and value are relative advantage (how does it compare to other ideas), compatibility (is it consistent with existing processes, values, experience), complexity (how difficult is it to achieve), trial-ability (can it be tested in safe environment), and observability (will results of innovation be visible to others).
This model also brings out the factor of time and how it influences the process of the innovation, especially in the correlation with the social influences and how they change as the innovation gains traction in the target population/organizations (Figure 5).
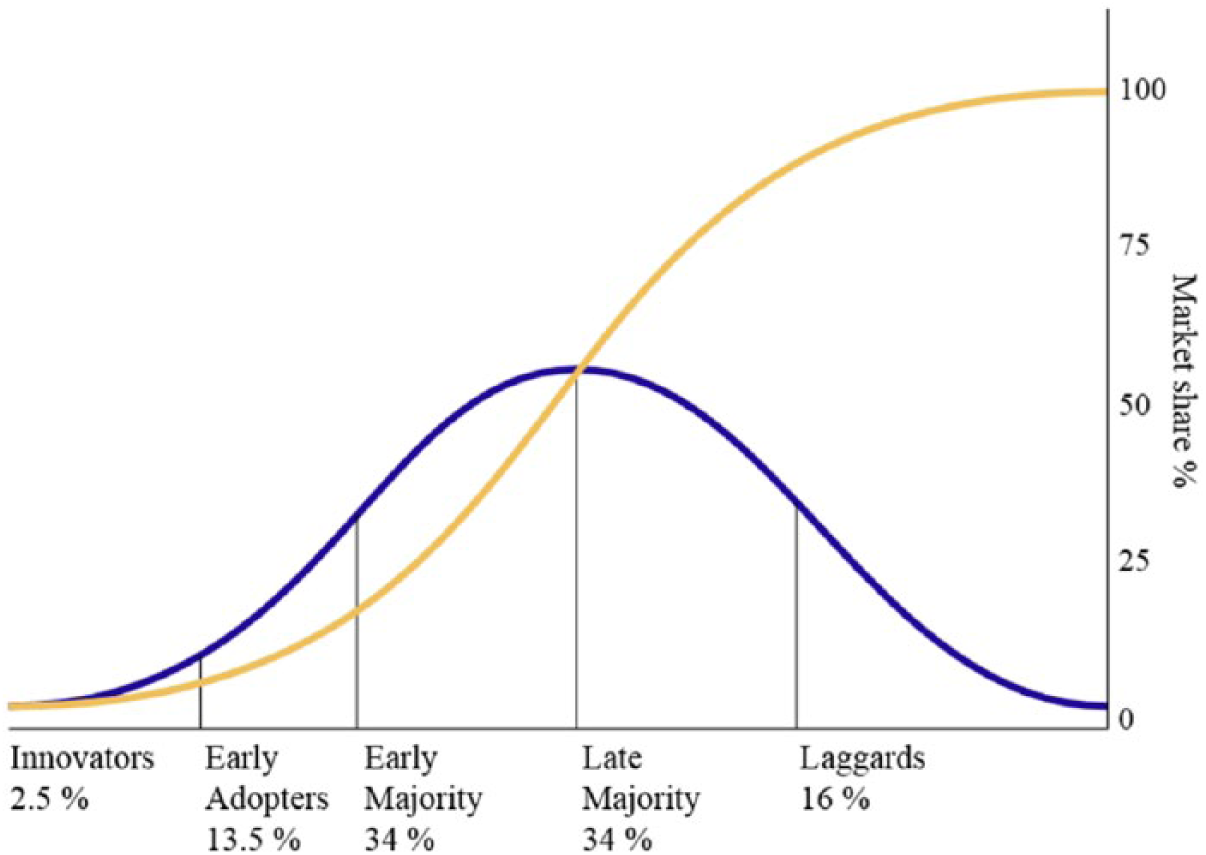
Diffusion of innovation curve. 21
Greenhalgh et al. 39 highlighted the difference between simpler, product-based innovation, where the single user of the innovation is the primary focus; and more complex, process-based innovation, where a whole team is the main focus, as illustrated in Figure 6.
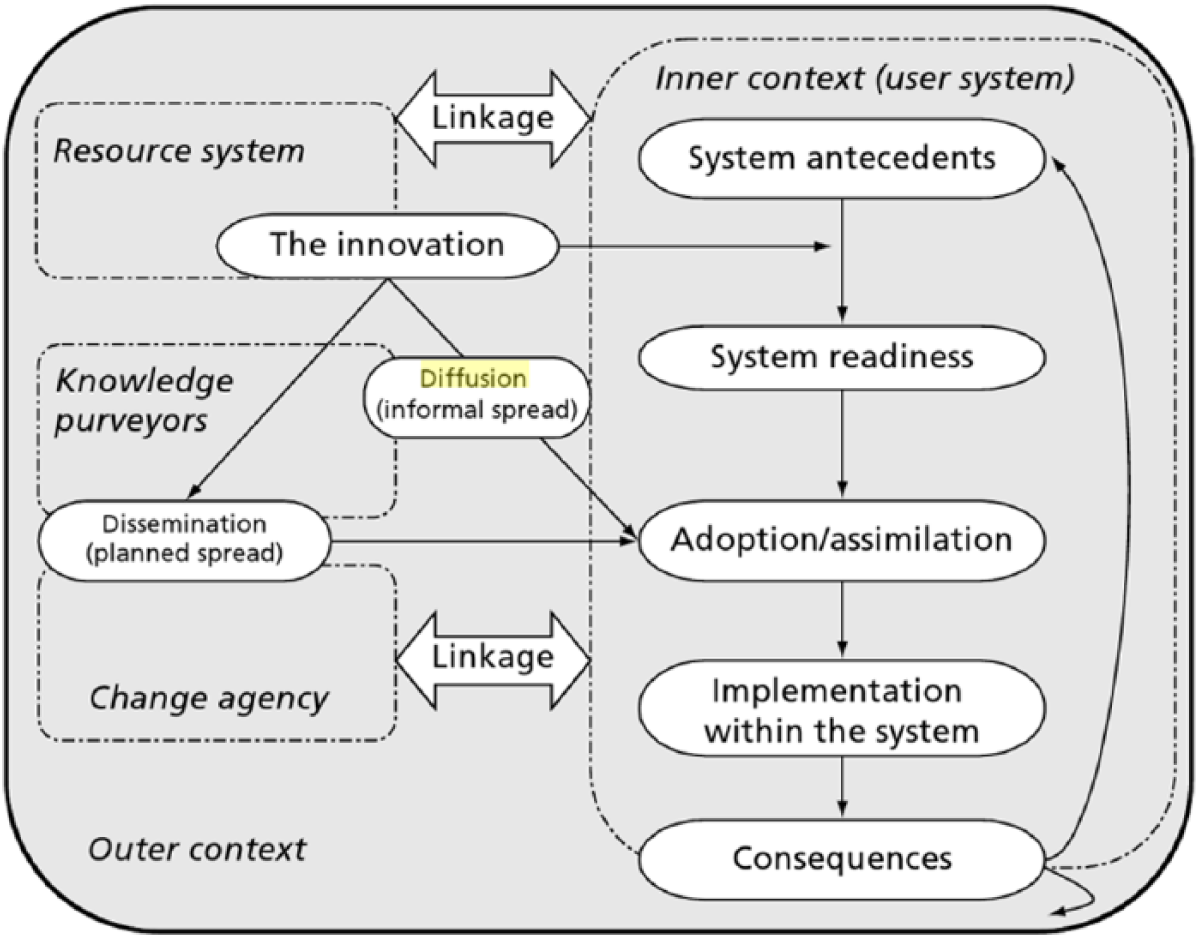
Model for determinants of diffusion of innovation in the health services. 39
On the other hand, Lyytinen and Damsgaard 40 emphasized the importance of understanding the adoption of complex and networked technologies that are becoming more prevalent. They argued that the adoption of such technologies can hardly be predicted by the processes described in the DoI alone. Therefore, more integrated approaches are needed to better understand technology adoption in specific settings and groups of users.
Rationale of the present study
Overall, currently there is a large financial investment in the development and deployment of healthcare information technologies, such as Health Information Systems (HIS), but this investment is not met by healthcare professionals’ readiness to use the said technological innovations. One way to better understand the social and behavioural drivers underlying healthcare professionals’ intentions to utilize HIS is to apply state-of-the-art TAMs, such as the modified UTAUT that applies to healthcare technologies. 35 Although the UTAUT accounts for key technology acceptance variables, such as healthcare professionals’ anticipated benefits on work performance and perceptions of effort, as well as social norms, it still overlooks the important role of more dynamic normative processes that are better described in other theories, such as the DoI. Specifically, the DoI can add to the UTAUT by increasing our understanding of the normative standards of technology use (e.g. how early adopters’ experiences with the technology are communicated and potentially influence others). The integration of UTAUT with DoI variables, therefore, can elucidate the processes of technology adoption by accounting for personal beliefs about work performance and effort, the existence of facilitating conditions, as well as experiential and normative influences relevant to using the technology in various phases (e.g. training, implementation, system use).
Stemming from previous research, which is arguing for the need to integrate TAMs with features of DoI theory25,41 for an enhanced understanding of end-users’ readiness to use emerging technologies, the present study used an integrative model to predict healthcare professionals’ intentions to use HIS (Figure 7). In this model, we anticipated that DoI variables relevant to the user experiences (e.g. training and implementation experiences around HIS) will significantly predict healthcare professionals’ intentions to use HIS, over and above the effects of the variables described in the UTAUT.
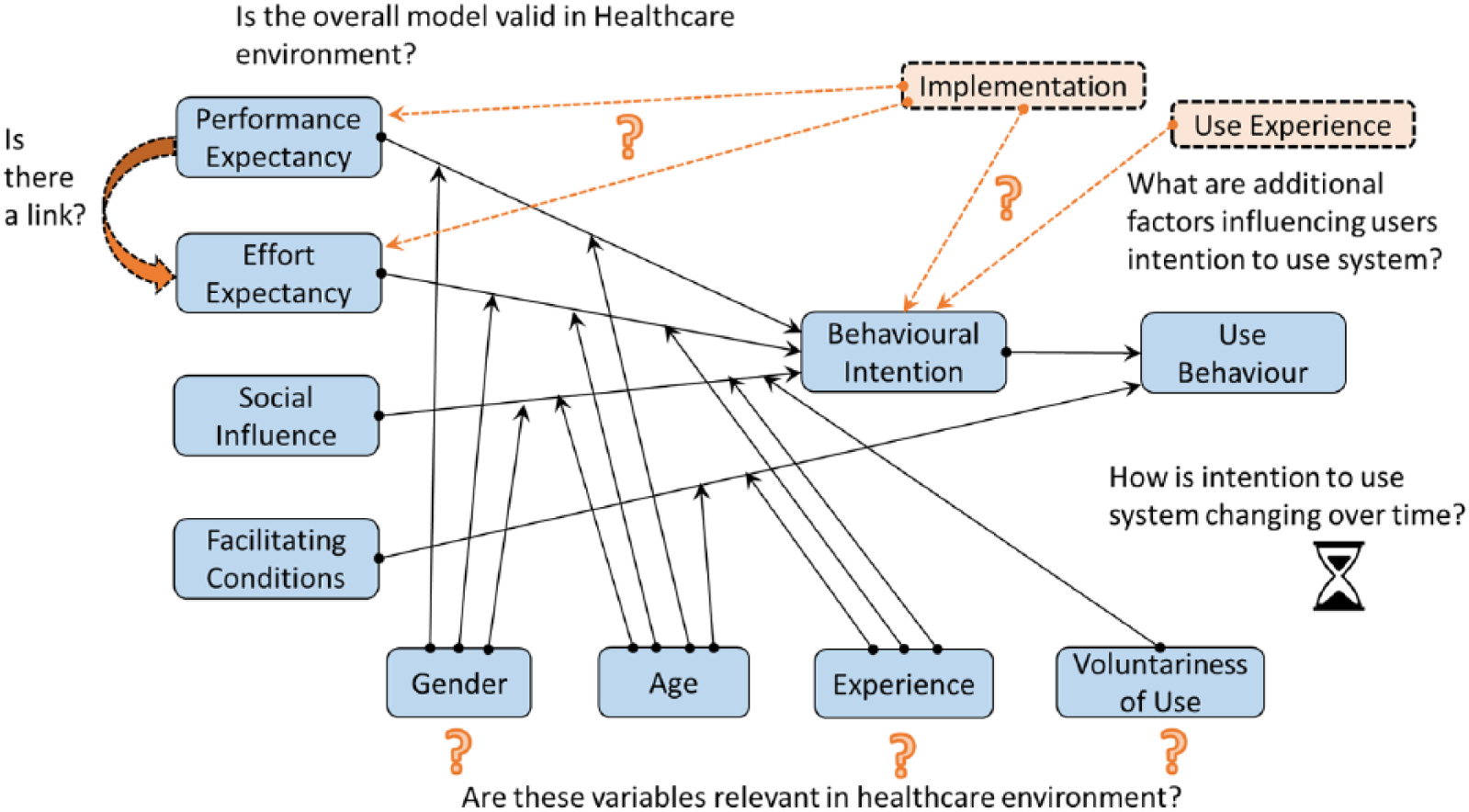
Overview of the research questions against the UTAUT and additional variants related to DOI model.
Methods
Participants/design
A cross-sectional, correlational, survey-based design was used. A two-stage cluster sampling was used to select participants. Two-stage cluster sampling allows researchers to first identify a larger sampling unit (i.e. healthcare settings in the present study) and then select participants in those settings as a second unit of assessment. In the context of the present study, this approach ensures that healthcare practitioners are derived from similar settings (i.e. healthcare providers). Because we sampled healthcare professionals from both private and public healthcare providers, our cluster sampling approach further ensures that healthcare professionals derived from the specific subsets of the first cluster (public vs private healthcare providers) are more homogeneous with respect to their experiences in using HIS. Stated differently, it is more likely that professionals coming from similar contexts will have similar experiences in technology use. It would be harder to achieve this goal by electing healthcare professionals from random settings without controlling for their professional setting/context.
At the first stage, private and National Health Service (NHS) healthcare service providers were identified and were contacted to take part in the study. At the second stage, healthcare professionals within the selected organizations were approached and requested to take part in the study. Overall, we contacted via email nearly 500 healthcare professionals, including doctors (GPs or consultants), nursing and administration support staff from private and NHS hospitals, asking them to complete an online survey about their perception towards technology use in healthcare settings. Of them, 105 provided valid responses that were used for subsequent analysis, yielding approximately 20 per cent response rate. The average age of participants was 41.06 years (standard deviation (SD) = 9.18), and 56.2 per cent (n = 59) were females. Most participants (79%, n = 83) came from the NHS, and 49 per cent (n = 51) identified as doctors/consultants and GPs (M age = 42.84 years, SD = 9.46, 64.7% males), whereas 51 per cent were identified as nursing and administration staff (M age = 39.23 years, SD = 8.68, 75.5% females). Following international ethics code for research with human subjects (Declaration of Helsinki), all participants were duly informed about the aims and purposes of the study, provided their informed consent prior to participation, and were informed about the participation rights (i.e. voluntary participation, right to withdraw without any prior notice and without any penalties, anonymity and confidentiality of the data).
Measures
Based on previous research on technology acceptance in healthcare settings18,35 and on systematic reviews of technology acceptance studies used in healthcare, 3 we developed a questionnaire comprising variables from the UTAUT and the DoI models, as well as demographic and work-related characteristics of the participants (i.e. age, gender, tenure, role in their organization).
With respect to UTAUT variables, performance expectancy was assessed with the mean of four items (e.g. ‘the system is improving my access to patient data’ and ‘using the system enables me to accomplish tasks more quickly’), and higher scores indicated higher perceived improvements/benefits in work performance using HIS. Internal consistency reliability was at acceptable levels (Cronbach’s α = .78). Effort expectancy was also measured with the mean of four items (e.g. ‘it was easy to become skilful in using the system’ and ‘using the system is clear and intuitive’), and higher scores indicated lower perceived effort needed to effectively use HIS, whereas the measure was internally consistent (Cronbach’s α = .92). Social influence was measured with the mean of three items (e.g. ‘most of my colleagues use the systems in its full capacity’ and ‘people whose opinion I value think that it is important to use the system’) and higher scores reflected more favourable social norms towards using HIS (Cronbach’s α = .86). Facilitating conditions were measured with the mean of four items reflecting the availability of resources/support to use HIS (e.g. ‘I have the necessary resources to use the system’ and ‘A specific person (or group) is available for assistance with system difficulties’). Higher scores on this measure indicated greater perceived support/facilitating conditions for using HIS (Cronbach’s α = .79). Voluntariness of use was assessed with the mean of four items reflecting personal choice in using the system (e.g. ‘If I have an option to complete a task with or without the system, I choose to use the system’), and higher scores reflected greater voluntariness (Cronbach’s α = .92). Finally, BIs (i.e. intentions to use the system) were measured with the mean of three items (e.g. ‘I intend to continue using the system in the future’ and ‘I will always try to use the system when appropriate for my work’), and higher scores indicated stronger future usage intentions (Cronbach’s α = .90).
With respect to DoI measures, implementation experience was measured with six items (e.g. ‘During the system implementation, purpose and the goals of the systems were clear’ and ‘I had ability to influence implementation decisions’), and higher scores indicated greater involvement in the process of system deployment and a more positive experience (Cronbach’s α = .74). Accordingly, system operation experience was measured with seven items (e.g. ‘System is stable and reliable in daily use’ and ‘All system related queries I had were answered clearly and timely’), and higher scores indicated a more positive and productive experience in actual system usage (Cronbach’s α = .92). Finally, training experience was measured with four items (e.g. ‘Employees were given enough time to train for using the system’ and ‘Training sessions were well organized and productive’), better experience in the process of training for system use (Cronbach’s α = .82).
Results
Group differences in UTAUT and DoI variables
One-way analysis of variance (ANOVA) was used to assess for gender differences, and differences between professional roles (medical vs non-medical staff), and type of sector (private vs NHS), in HIS usage intentions and in related variables derived from the UTAUT and the DoI. The results did not show significant differences between gender and professional roles (p > .05).
Inter-correlations among the study variables
Bivariate correlation analysis with Pearson’s r was used to estimate the association between intentions to use HIS and the other study variables. The findings showed that the system operation experience had the strongest correlation with usage intentions (r = .861, p < .001), followed by UTAUT variables, such as performance expectancy (r = .799, p < .001), facilitating conditions (r = .796, p < .001), social influence (r = .758, p < .001), training experience (r = .730, p < .001), effort expectancy (r = .633, p < .001), and implementation experience (r = .611, p < .001). The observed correlations were in the direction expected according to the main theoretical tenets of the UTAUT and the DoI, thus attesting to the construct validity of the measures used. The findings from the bivariate correlation analysis are presented in Table 1.
Inter-correlations and internal consistency reliability scores for the measures used in the study.
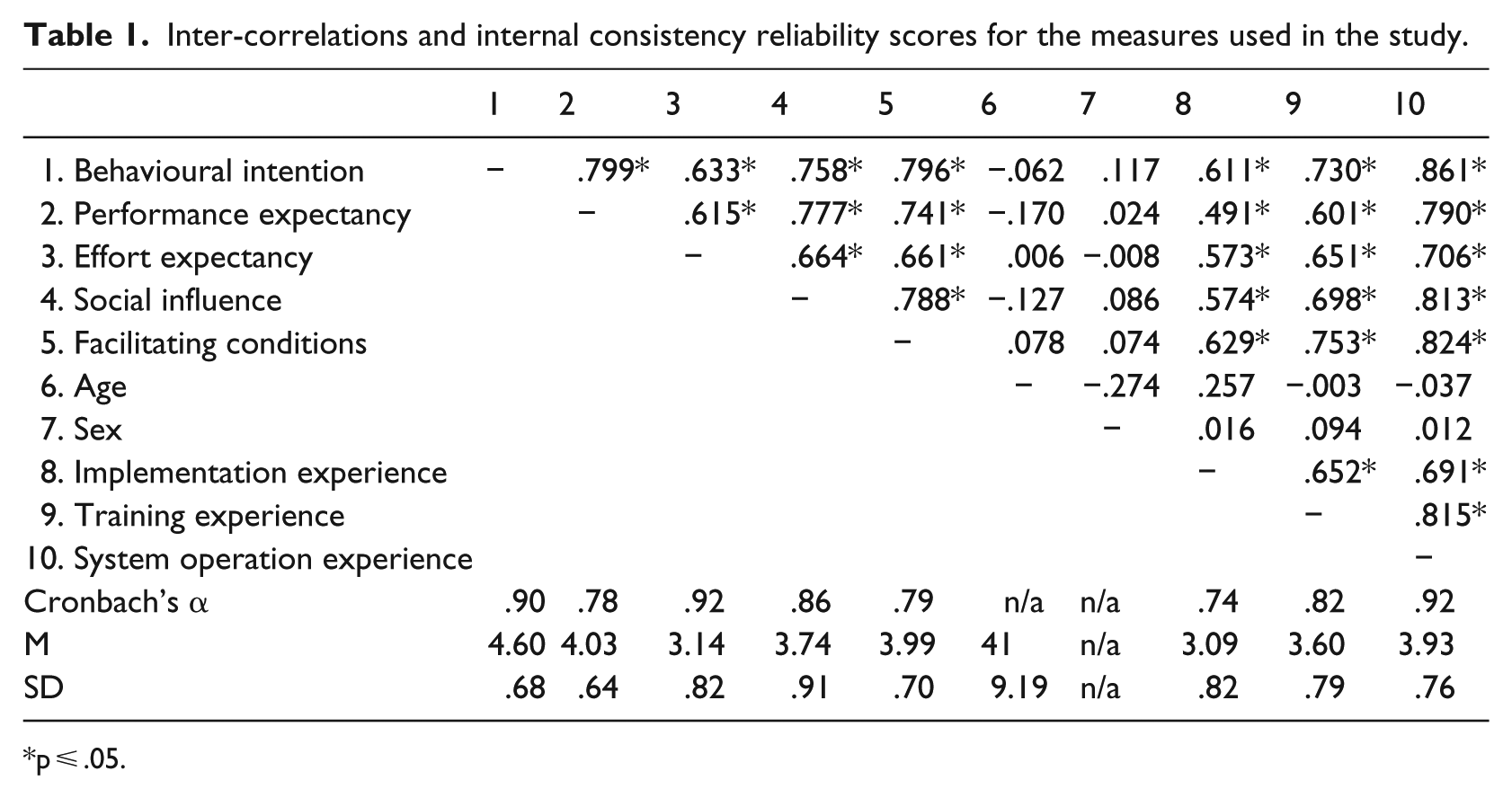
p ⩽ .05.
Direct effects of UTAUT and DoI variables on HIS usage intentions
Hierarchical linear regression and moderated regression analysis were used to assess the moderation effects of the tested variable. Specifically, based on the tenets of the UTAUT, it was expected that performance expectancy, effort expectancy, social influence, and facilitating conditions would directly predict intentions. Second, it was expected that integrating variables from the DoI model to the UTAUT will significantly improve predicted variance in intentions. A two-step model was used to test these expectations. The first step included variables derived from the UTAUT (performance expectancy, effort expectancy, social influence, and facilitating conditions). The second step included variables derived from the DoI model (i.e. training experience, implementation experience, and system operation experience). The overall model was statistically significant (F = 42.18, p < .001) and predicted 78.1 per cent (adjusted R2) of the variance in future intentions to use HIS. The variance inflation rate (VIF) was below 10 for all predictor variables, thus, indicting low collinearity among the predictors. Standardized beta values (β) were used to denote the relative strength of each predictor variable, and unstandardized beta coefficients (B) with 95% confidence intervals (CIs) were used to indicate the expected change in intentions if the predictor variable changed by one unit, holding all other variables constant. The 95% CIs were used to help in estimating the true relevance of the predictor variables, in addition to the p-values. For example, 95% CIs containing zero values probably indicate a non-significant effect, or an effect that should be treated with caution, even if the respective p-value is lower than .05. 42
In the first step of the analysis, significant predictors included performance expectancy (β = .407, p < .001) and facilitating condition (β = .348, p = .001). In the second step of the analysis, the inclusion of DoI model variables increased predicted variance significantly (ΔR2 = 5.6%, p < .001), performance expectancy retained its significant effect, but the effect of facilitating condition turned non-significant. Among the DoI variables, only system operation experience significantly predicted intentions (β = .451, p < .001). The results of the regression analysis are presented in Table 2.
UTAUT and DoI predictors of intention to use HIS.
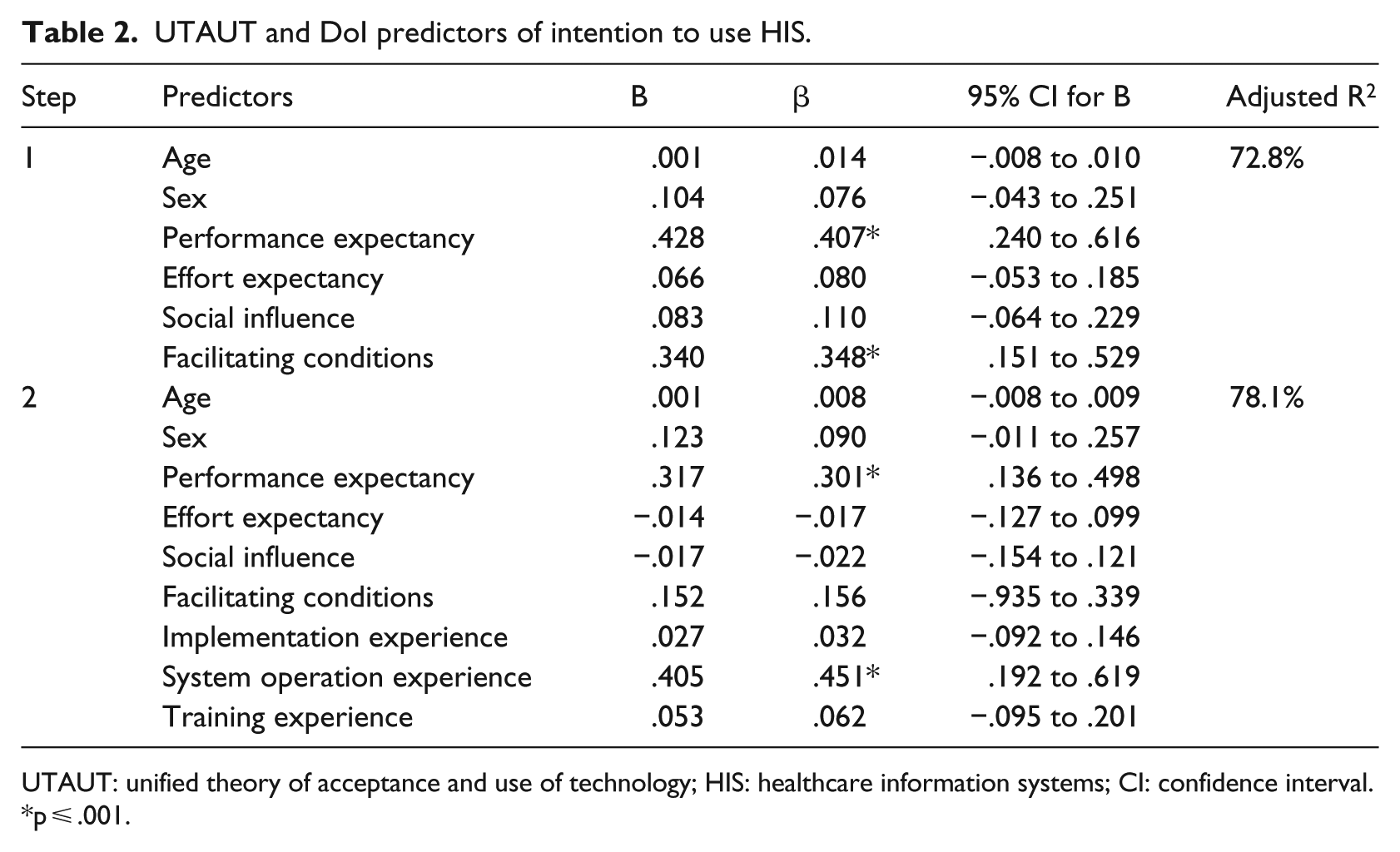
UTAUT: unified theory of acceptance and use of technology; HIS: healthcare information systems; CI: confidence interval.
p ⩽ .001.
Interaction between UTAUT variables in predicting HIS usage intentions
In addition, based on the UTAUT, it was expected that the effects of performance expectancy on intentions would be moderated by demographic variables (gender and age); the effects of effort expectancy on intentions would be moderated by demographic variables (age and gender), and previous experience with using CIS; the effects of social influence on intentions would be moderated by demographic variables (age and gender) and previous experience with using HIS; the effects of facilitating conditions on intentions would be moderated by age and experience. Ten moderated regression models were respectively developed to test each of the potential moderation effects. The predictor variables were standardized (z scores) to avoid multicollinearity, and an interaction term was computed denoting the product of (predictor × moderator) in each model.
The results showed that voluntariness of use significantly interacted with effort expectancy in predicting future usage intentions of HIS (B effort expectancy × voluntariness = –.249, β = –.415, p < .001, 95% CI for B = –.313 to –.186), so that the association between effort expectancy and usage intentions is stronger when voluntariness scores are lower; this possibly means that when users of technology are willing to use the given system or application, effort expectancies become less influential on intentions to use the system. Furthermore, the analysis showed that voluntariness of use significantly interacted with social influence, so that the association between social influence and usage intentions was weaker when voluntariness was higher (B social influence × voluntariness = –.193, β = –.403, p < .001, 95% CI for B = –.247 to –.139); this finding potentially indicates that favourable social norms become less relevant in predicting intentions to use HIS when end-users are personally willing to use HIS.
Discussion
Overview of the key findings
The present study assessed the predictors of intentions to use Health Information Systems (HIS) among healthcare professionals in England, using a TAM that incorporated variables from the UTAUT and the DoI models. The results showed that certain UTAUT and DoI variables predicted HIS usage intentions in our sample. More specifically, performance expectancy (i.e. expectations that using the HIS in question will improve work performance) and system operation experience accounted for the variance in intentions to use HIS, whereas other variables pertaining to ease of use (i.e. effort expectancy), social norms, facilitating conditions, and training did not have a significant effect on intentions. These findings are in line with other studies of TAM/UTAUT applications in healthcare3,19 where Performance Expectancy and not Effort Expectancy significantly predicted intentions. However, other studies have found different results. 18 The variability in research findings reflects the heterogeneity and variability in healthcare services.
Furthermore, variables related to DoI model, like experience during implementation, training, and system usage, were associated with future intention to use the technology (see Table 1), but only system operation experience predicted intentions to use HIS when other predictors were controlled for. This finding highlights the importance of the initial stages of system usage for the future sustainability. Adoption or rejection over time will be influenced by these experiences, so they need to be managed carefully by practitioners and understood better by academics.
Within the respondents’ profile, those that had some role in the decision for the system purchase or implementation show significantly more positive intention towards using the system. No other significant differences were found between different groups of respondents in this sample.
Limitations of study
Overall, the size and variety of the sample, as well as the relatively low response rate, indicate that this article’s findings would benefit from further supporting evidence. Some very strong relations found with BI values are challenged by the fact that the values are significantly skewed to the right, indicating overall high usage intention. This is likely due to combination of these three factors:
Response bias - with relatively low response percentage, it is possible that the survey had more responses from those with more positive attitude toward the systems in question (i.e. self-selection bias).
Low sensitivity of the questions related to the BI to detect small variations in the variable. This may be because many of the respondents are already users of the systems, and this is one of their main tools in daily work; thus, the intention for future use is positively influenced by their current role rather their personal attitude.
Respondents are working with different systems and indifferent stages of deployment and maturity, so their responses may also be influenced by this fact, making cross-comparison somewhat less reliable. Generalization of these findings to any other environment is limited, due to the specific nature of test environment here, and limited size and response in the research.
In addition, the definition of PU and the other constructs derived from the UTAUT were largely based on published studies and the recommendations of the UTAUT founders. As such, the items have largely focused on usefulness for the user (in our case doctors) without really addressing the interpersonal nature of the specific profession (i.e. patient welfare). This is something to be studied further by future research on this topic.
Recommendations for future research
Some findings presented could potentially have implications for practice, so further research to test those may be valuable. The link between operational experience of the system use and BI could be significant for practitioners and this should be investigated in further research. In addition, any link between users taking part in selection and implementation and use intention should be evaluated further as it could be used within the process of selection and implementation.
In addition, general indirect influence of the process of implementation and system operations on some key UTAUT variables and use intention could be significant for further evaluation. Longitudinal study with matched samples of respondents, which can be surveyed within different stages of deployment of system, would be the optimal approach to gathering data. This would exclude many variations related to the system, environment, time, and so on, and possibly, more importantly, it could test dynamic development of BI depending on value of various variables.
Generally, there is a quite limited body of evidence for informational technology acceptance within healthcare environment. Considering importance and unpredictability of this process, not only from organizational and economical perspective, but also from the perspective of patient safety and treatment outcomes, further research in this whole area is highly recommended by authors. Finally, it could also be valuable to test significance of DoI model within this environment and if it could compliment UTAUT. This could be especially relevant for the dynamic development of the BI and which are the factors that can be useful for practitioners to influence it.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.