
Abstract
HIV medical care providers need a wide range of evidence-based clinical information resources to manage their patients’ health. We determined whether providers’ choice of information sources for HIV care and treatment are associated with their demographic and medical practice characteristics. Data used for this study were obtained from a probability sample of HIV medical care providers in 13 outpatient HIV facilities in Houston/Harris County, Texas, surveyed between June and September 2009. The mean number of information sources used by HIV medical care providers for HIV care and treatment was 5.83 (95% confidence interval: 4.90–6.75). Antiretroviral therapy guidelines (95.6%), medical journals and textbooks (82.6%), and Internet sources (69.5%) were ranked first, second, and third as sources of clinical information. At least one of the providers’ demographic or medical practice characteristics was significantly (p ⩽ 0.05) associated with six of the clinical information sources. Integration of these information resources into clinicians’ workflow may enhance efficiency of HIV care and treatment and facilitate improved patients’ care and health outcomes.
Keywords
Introduction
In recent years, the demand for proven clinically effective treatments has increased because of the need to ensure the highest quality of patient care while making the most effective use of limited resources. 1 However, the explosive increase in the amount and flow of information and data in the last few decades represents a major challenge within the health care system as well as at the provider level. Information overload has hastened the ability to improve the quality of evidence-based information used in the daily medical decision-making process and in all facets of health care. 2 Clinicians use personal clinical knowledge and a variety of information resources to solve their clinical information needs. They need to be able to access information on clinical effectiveness of treatments to improve the quality of patient care and to stay well informed on new developments, especially in the areas of diagnostic strategies, technologies, and therapies, which are constantly evolving. Consequently, medical professionals need to be able to refresh their memories and update their knowledge efficiently and effectively.
Health consumers are now more informed of their health conditions because of the explosion in Internet technology and information systems. However, this self-directed information gathering may be good and bad. In a world of open technology and easy access to information, clinicians must stay informed of the standard of care practices and current research findings, especially as some patients may come to their clinic appointments well armed with questions and/or information obtained from the Internet. However, it is unclear exactly how these changes are influencing the ways in which individuals obtain health or medical information and what patterns of trust are associated with use of different information channels.3,4
In a meta-analysis conducted by Haug, 5 it was reported that physicians generally preferred information sources from journals and textbooks, and consultation with colleagues to get answers to clinical and research questions. Similarly, family physicians caring for patients with HIV ranked clinical practice guidelines as the most important, followed by medical journals and textbooks, and other health care professionals. 6 Although clinical guidelines provide an overview of the management of a condition or the use of an intervention, they may not address uncertainties of current clinical practices and should be considered as only one strategy that can help improve the quality of care that patients receive. 7 Rapid diffusion of Internet technology and advances in information-tailoring tools and telemedicine have also broadened the reach of health care specialists beyond the constraints of the traditional office.8–11
Researchers have explored information needs, information-seeking behavior, and information sources in clinical practice with regard to a range of health professions.12–16 However, because HIV is a rapidly changing field, clinicians may find it challenging to stay up to date and therefore could benefit from efficient access to patient-focused HIV information and advice.17,18 Despite the complex treatment processes associated with HIV/AIDS, only one known study has reported the perceptions of HIV care providers sources of evidence and how those influence the clinical decision-making process. 6
No prior research has examined whether HIV Medical Care Providers’ (HMCP) preferred sources of clinical information are closely aligned with their demographic and medical practice characteristics. The objectives of this study were to identify and rank the sources of information used by HMCPs for HIV care and treatment and to determine whether HMCPs’ choices of information sources are associated with their demographic and medical practice characteristics.
Methods
Survey design and participants
Data used for this study were collected as part of the Centers for Disease Control and Prevention’s (CDCs) Medical Monitoring Project (MMP) Provider Survey conducted in 23 US states and territory from June through September 2009. The survey was administered to a nationally representative sample of HMCP who were selected to participate in the MMP. MMP is a complex cross-sectional survey designed to learn more about the experiences and needs of people living with HIV (PLWH) in the United States. Further details on MMP and the associated sampling method have been published elsewhere,19,20 while the description of MMP Provider Survey can be found in Mgbere et al. 21 and Frankel et al. 22
The Houston/Harris County, Texas component of the MMP Provider Survey data was used for this study. The survey participants consisted of a probability sample of HMCPs from 13 outpatient facilities who agreed to participate in the survey. The HMCPs eligible for this survey included physicians, physician assistants (PA), and nurse practitioners (NP) working in one of the MMP-sampled facilities and who provided care, ordered CD4 cell count or HIV RNA viral load testing, and/or prescribed antiretroviral therapy (ART) medication to individuals ⩾18 years of age with HIV infection. Interns, residents, fellows, and others in training programs were not eligible to participate in the survey. Providers who obtained CD4 cell counts and HIV RNA viral loads only for referral purposes or provided ART refill prescriptions, but did not play a more active role in managing their patients’ HIV infection, were also not eligible to participate in the survey. A total of 23 HMCPs completed the survey representing a response rate of 45 percent. The rate though considered low was higher than 42 percent rate obtained for the same survey at the national level, 23 and is typical of response rates found in other provider surveys. 6 , 24 , 25
Analytic measures
The main outcome variable was based on a structured question in which the HMCPs were asked to select all the sources of information that they used for HIV care and treatment in their clinical practice from a 12-option list. The response options included the United States Public Health Service (USPHS) and/or Infectious Diseases Society of America (IDSA) antiretroviral guidelines, medical journals and textbooks, Internet sources (i.e. Clinical Care Options, for example, Medscape, MedlinePlus, and The Body), professional colleagues (word of mouth/information from peers), international/national conferences, other HIV care guidelines, pharmaceutical representatives/pharmaceutical-sponsored meetings, national/regional AIDS education and training centers, in-services (i.e. Grand rounds), medical associations, the national HIV telephone consultation service (Warmline), and continuing medical education (CME). Participants were expected to indicate 1 (yes) or 0 (no) for each information source that they used in their practice. The total number of information sources used by each provider was then summed up and the average determined. The independent measures used in this study include providers’ demographics (type of HIV provider, age category, gender, race/ethnicity, infectious disease board certification status, years caring for patients with HIV infection, language of communication) and medical practice characteristics (facility type, number of HIV-positive patients in practice, self-rated knowledge of HIV care, sufficiency of time for patient care, referral for ART initiation). These characteristics have been described in detail in previous publications,21,26 and so, only findings relating to them in this study will be presented.
Data analysis
Based on the responses, the proportion for each information source and the corresponding 95 percent confidence interval (95% CI) were determined. The sources of information used by the HMCPs were then ranked in order of magnitude (from greatest to the least used sources). To determine whether differences existed in the average number of clinical information sources used by HMCPs by demographic and medical practice characteristics, we conducted analyses of variance and tested the means using pooled Student’s t-test and assuming equal variances. Only seven of the sources of information were selected for bivariate analyses as small cell sizes precluded the inclusion of five other sources. The chi-square test or Fisher’s exact test (when expected values were <5) were used to determine the independent associations of the seven selected sources of clinical information by provider demographic and medical practice characteristics. Characteristics within each information source that met the statistical threshold of p < 0.20 during the bivariate analysis were selected a priori and simultaneously entered in the multivariable logistic regression models. Therefore, the number of predictor variables that met the entry criteria varied slightly within the different information sources. The analysis produced estimates of adjusted odds ratios (aOR), 95 percent CI, and corresponding p-values for each characteristic within the information sources. The models’ fitness was determined using the maximum likelihood ratio test, logWorth, and R2 statistics. All tests performed were two-tailed, with a probability value of 0.05 used as the statistical significance level. The entire analyses were performed using SAS 9.4 (SAS Institute, Cary, NC, USA).
Human subjects protection
MMP was determined by the National Center for HIV, Viral Hepatitis, STD and TB Prevention’s Office of the Associate Director for Science at the CDC to be a non-research, public health surveillance activity used for disease control program or policy purposes. As such, MMP is not subject to human subjects’ regulations, including federal institutional review board (IRB) approval. As an amendment to MMP, the MMP Provider Survey was covered under the same non-research determination. All data collection was Health Insurance Portability and Accountability Act (HIPAA) compliant.
Results
Sources of clinical information
Table 1 presents the sources of information (n = 12) used in HIV care and treatment and the relative proportions of HMCP associated with each source. The USPHS and/or IDSA ART guidelines was ranked first with 95.6 percent (95% CI: 79.0–99.2) of providers indicating that this was their main source of clinical information. This was followed by medical journals and textbooks (82.6%, 95% CI: 62.9–93.0), Internet sources (69.5%, 95% CI: 49.1–84.4), and professional colleagues (65.2%, 95% CI: 44.9–81.2), which were ranked as second, third, and fourth, respectively. International/national conferences and other HIV care guidelines were tied in the fifth place (60.8%, 95% CI: 40.8–77.8), while pharmaceutical representatives/pharmaceutical-sponsored meetings (47.8%, 95% CI: 29.2–67.0) and National/regional AIDS education and training centers (34.7%, 95% CI: 18.8–55.1) were ranked sixth and seventh place. In-service (26.1%, 95% CI: 12.5–46.5) and medical associations (21.7%, 95% CI: 9.7–41.9) also serve as clinical information sources for HMCPs and were ranked eighth and ninth place. The least used sources for clinical information (ranked 10th place) were the National HIV telephone consultation service (Warmline) and CME, each represented by 8.7 percent (95% CI: 2.4–26.8) of the study participants.
Sources of clinical information used in HIV care and treatment by HMCPs—Houston Medical Monitoring Project Provider Survey, 2009.
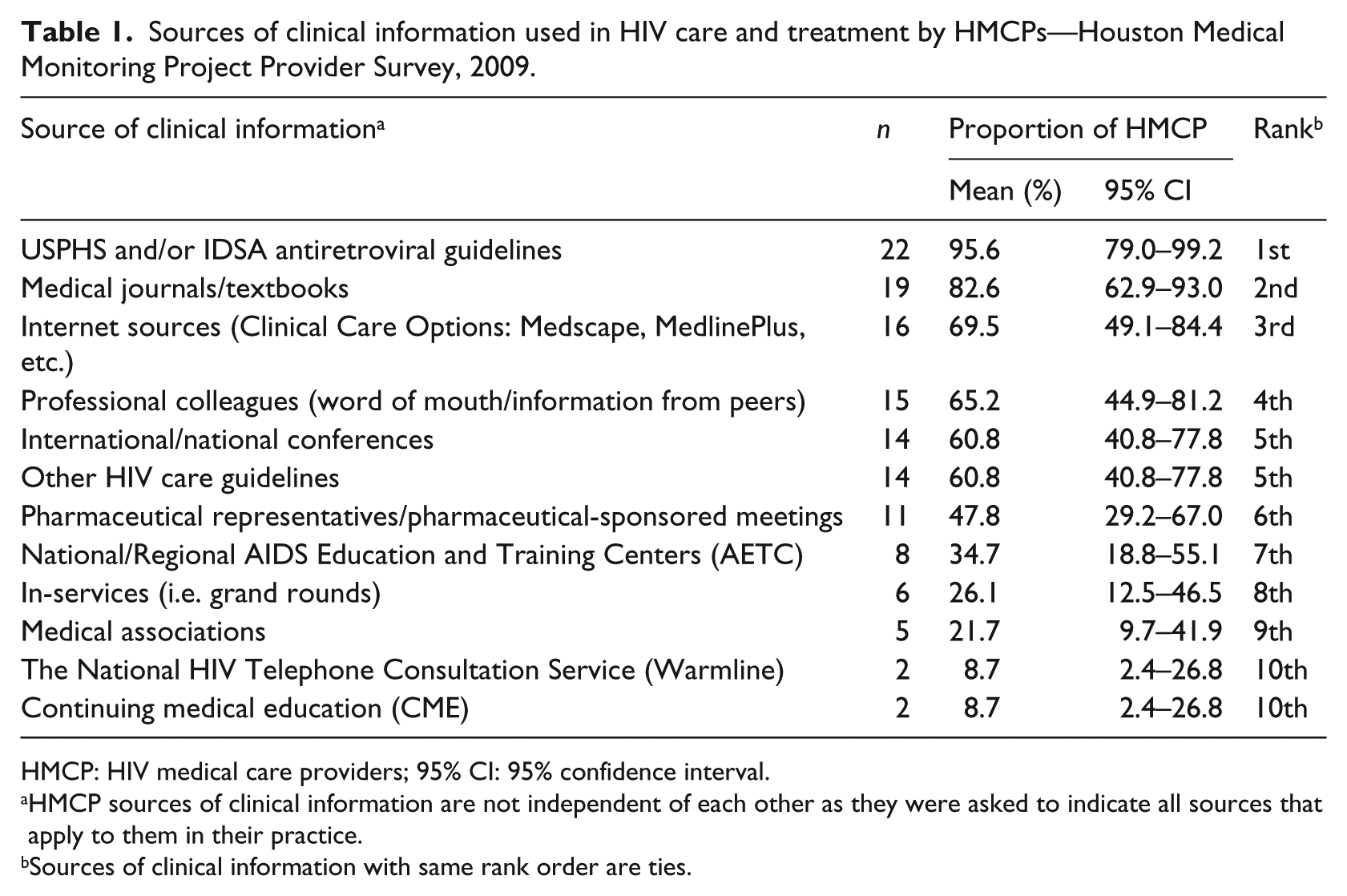
HMCP: HIV medical care providers; 95% CI: 95% confidence interval.
HMCP sources of clinical information are not independent of each other as they were asked to indicate all sources that apply to them in their practice.
Sources of clinical information with same rank order are ties.
Associations between sources of information, and providers’ demographic and medical practice characteristics
The mean number of information sources used by HMCP for HIV care and treatment was 5.83 (95% CI: 4.90–6.75), implying that more than 50% of identified sources of information (n = 12) were used by providers (Table 2). There were no statistically significant (p > 0.05) differences in the mean number of information sources used by HMCPs across their demographic and medical practice characteristics.
Mean number of sources of clinical information a used by HMCP by demographic and medical practice characteristics—Houston Medical Monitoring Project Provider Survey, 2009.
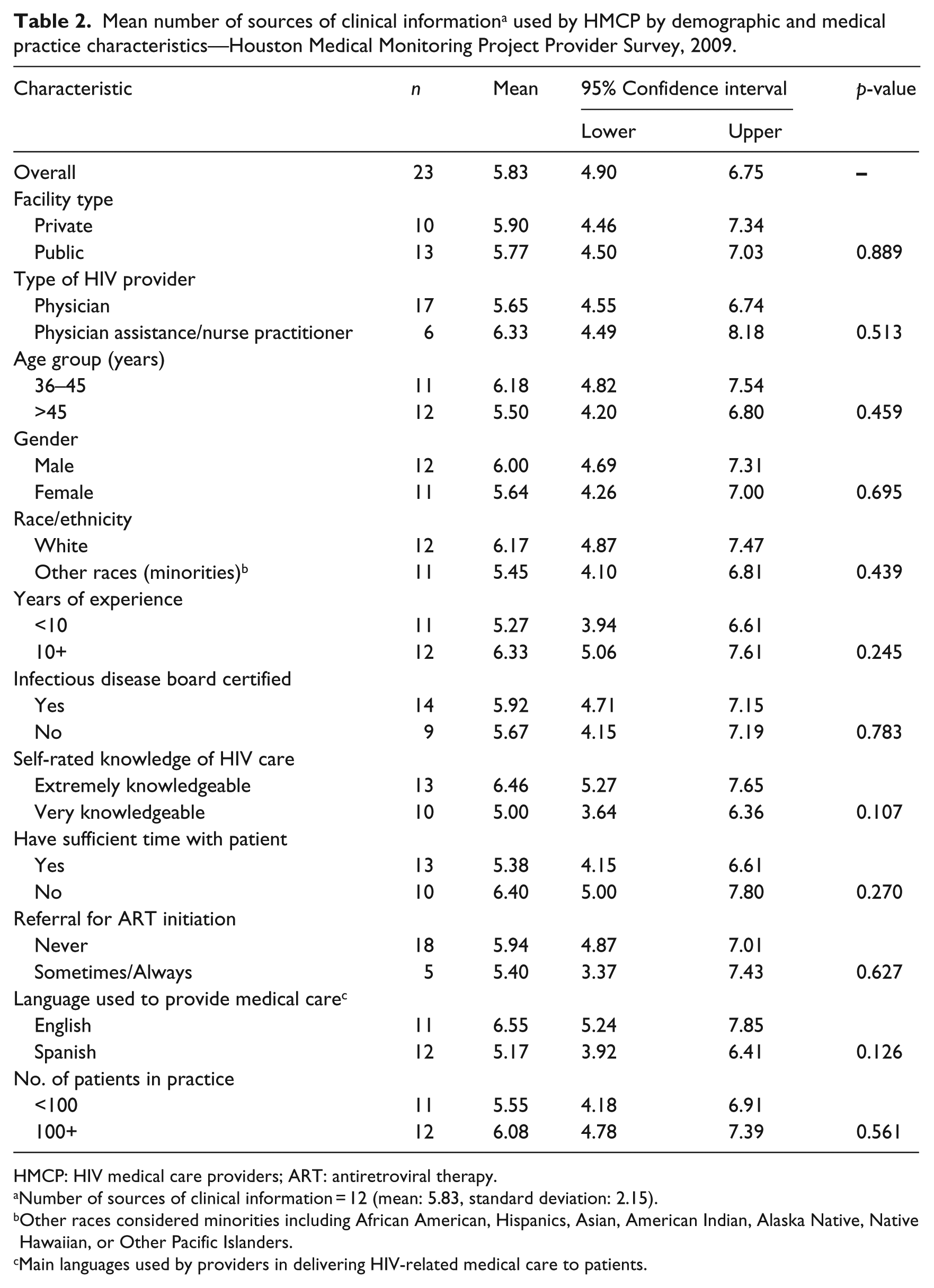
HMCP: HIV medical care providers; ART: antiretroviral therapy.
Number of sources of clinical information = 12 (mean: 5.83, standard deviation: 2.15).
Other races considered minorities including African American, Hispanics, Asian, American Indian, Alaska Native, Native Hawaiian, or Other Pacific Islanders.
Main languages used by providers in delivering HIV-related medical care to patients.
The associations of seven major sources of information used by HMCPs in HIV care and treatment with their demographic and medical practice characteristics are given in Table 3. In general, only one or two characteristics were found to have significant distinguishing associations with six of the sources. Only 18.2 percent of the HMCPs that referred their patients to other HIV specialists for ART initiation used USPHS and/or IDSA ART guidelines compared to those that did not make any referrals (81.8%, p = 0.052). Most physicians (84.2%, p = 0.014) had preference for medical journals and textbooks as one of their main sources of information for HIV care and treatment when compared to PA/NPs (15.8%, p = 0.014). Similarly, we noted significant associations (χ2 = 5.79, p = 0.016) between use of Internet services and providers’ gender with more males (68.8%) than females (31.2%) using this source for their medical information needs. Sourcing of medical information through attendance of international and national conferences ranked fifth and was significantly associated (χ2 = 3.88, p = 0.049) with providers’ age group. Most providers who were 36–45 years old (64.3%) depended more on this source for medical evidence in their practice than those who were older than 45 years (35.7%). There was significant association (χ2 = 3.88, p = 0.049) between use of other HIV treatment guidelines and the language used in providing HIV care to patients with 64.3 and 35.7 percent of the providers using English and Spanish as the medium of communication. Although ranked as the sixth main source for HIV care and treatment information, pharmaceutical representatives and pharmaceutical-sponsored meetings were significantly associated with the type of provider (χ2 = 8.86, p = 0.003) and the language used in administering care (χ2 = 5.24, p = 0.022). More PA/NPs (54.6%) than physicians (45.5%) tend to use this source for their clinical information needs.
Associations of seven major sources of clinical information used by HMCPs in HIV care and treatment and their demographic and medical practice characteristics—Houston Medical Monitoring Project Provider Survey, 2009.
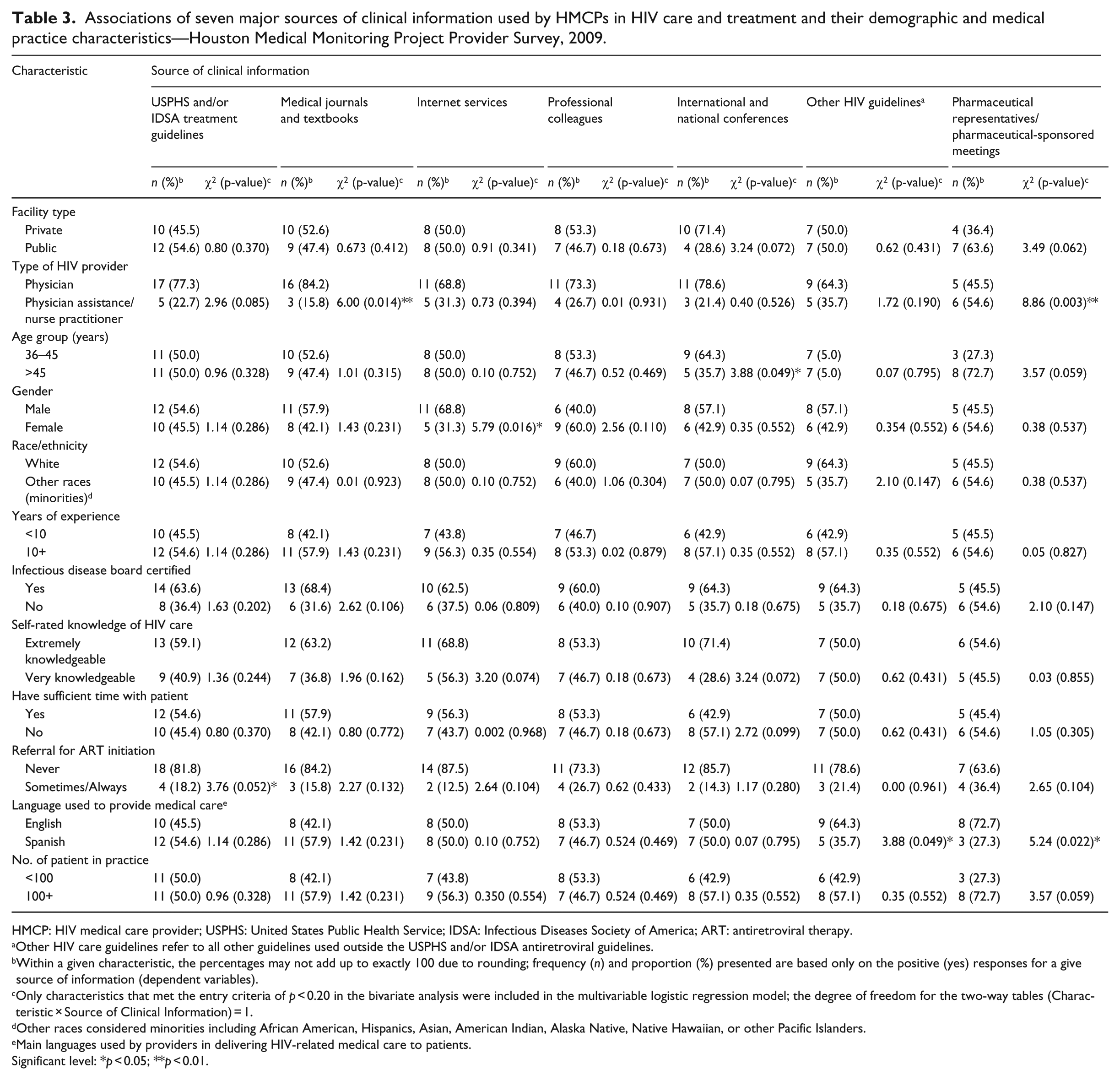
HMCP: HIV medical care provider; USPHS: United States Public Health Service; IDSA: Infectious Diseases Society of America; ART: antiretroviral therapy.
Other HIV care guidelines refer to all other guidelines used outside the USPHS and/or IDSA antiretroviral guidelines.
Within a given characteristic, the percentages may not add up to exactly 100 due to rounding; frequency (n) and proportion (%) presented are based only on the positive (yes) responses for a give source of information (dependent variables).
Only characteristics that met the entry criteria of p < 0.20 in the bivariate analysis were included in the multivariable logistic regression model; the degree of freedom for the two-way tables (Characteristic × Source of Clinical Information) = 1.
Other races considered minorities including African American, Hispanics, Asian, American Indian, Alaska Native, Native Hawaiian, or other Pacific Islanders.
Main languages used by providers in delivering HIV-related medical care to patients.
Significant level: *p < 0.05; **p < 0.01.
Multivariable logistic regression models for sources of information
Table 4 shows the summary of multivariable logistic regression models for sources of information by selected provider demographic and medical practice characteristics. Only one of the identified characteristics each distinctively tends to significantly determine the likelihood of providers’ choices of the six major sources of information for HIV care and treatment. HMCPs who did not refer their patients for ART initiation elsewhere were 23 times (adjusted odds ratio (aOR): 22.6, 95% CI: 5.19–38.46, p = 0.001) more likely to use USPHS and/or IDSA ART guidelines as the main source for clinical information in their practice than those who made referrals. Similarly, physicians were 16 times more likely to use medical journals and textbooks as their source of clinical information (aOR: 16.0, 95% CI: 10.50–34.50, p = 0.021) compared to PA/NPs. More male providers had preference for use of Internet services (aOR: 13.2, 95% CI: 1.66–28.70, p = 0.013) for HIV care and treatment information than their female counterparts. Our study further noted that providers who were 36–45 years old were 6.3 times (aOR: 6.3, 95% CI: 1.05–24.88, p = 0.044) more likely to use clinical information gathered during international and national conferences in their practice when compared to those who were about 46 years and above. There was preference for the use of other HIV care guidelines by HMCP who used Spanish language to provide HIV care compared to those who used English language in their practice. Similarly, providers who used Spanish language as the medium of communication with their patients were eight times (aOR: 8.0, 95% CI: 3.79–46.48, p = 0.019) more likely to use pharmaceutical representatives/pharmaceutical-sponsored meetings as the source for clinical information used in their practice compared to those who used English language to deliver care at their clinic (Table 4).
Summary of multivariable logistic regression models for sources of clinical information by selected provider demographic and medical practice characteristics — Houston Medical Monitoring Project Provider Survey, 2009.
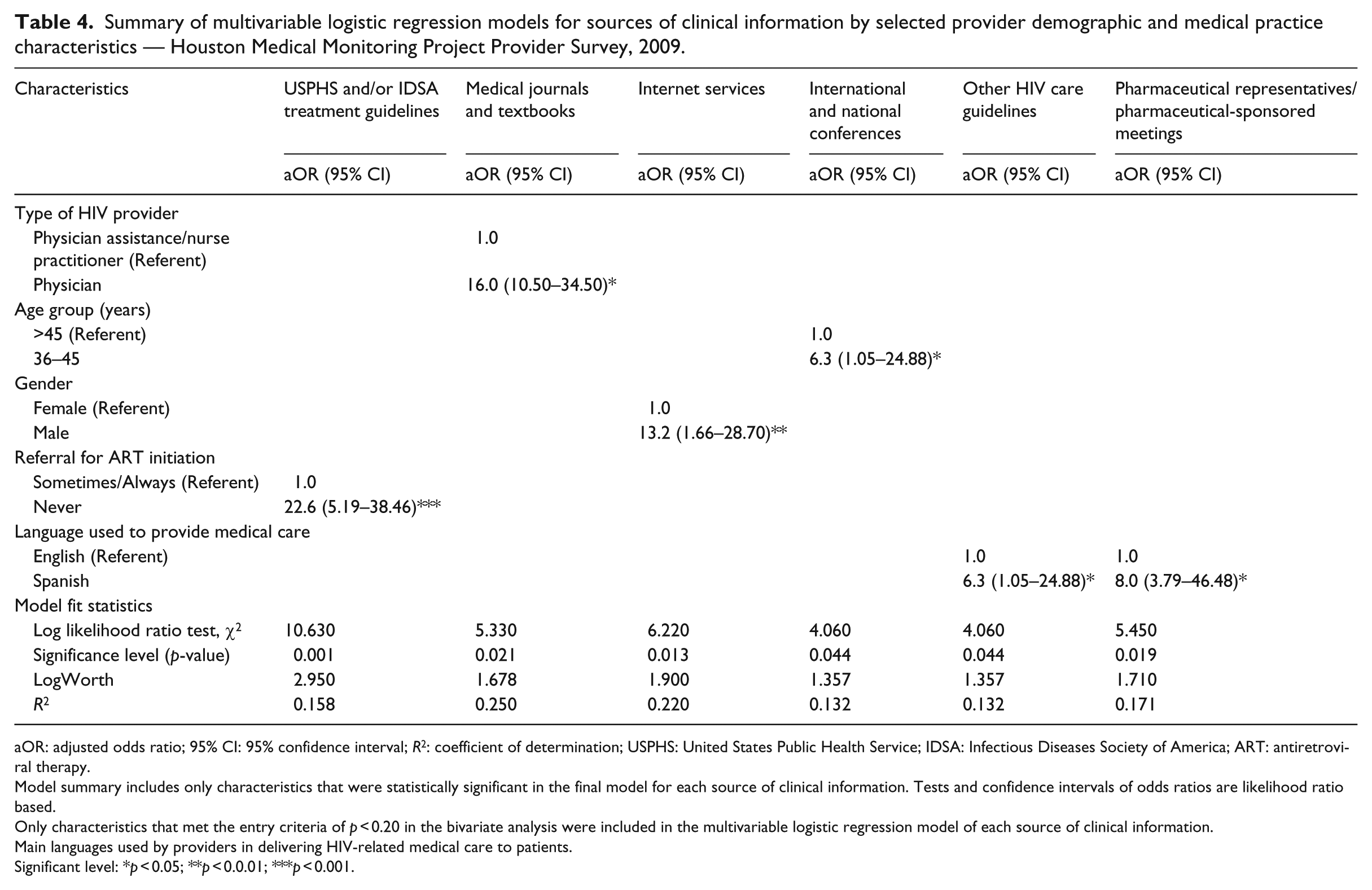
aOR: adjusted odds ratio; 95% CI: 95% confidence interval; R2: coefficient of determination; USPHS: United States Public Health Service; IDSA: Infectious Diseases Society of America; ART: antiretroviral therapy.
Model summary includes only characteristics that were statistically significant in the final model for each source of clinical information. Tests and confidence intervals of odds ratios are likelihood ratio based.
Only characteristics that met the entry criteria of p < 0.20 in the bivariate analysis were included in the multivariable logistic regression model of each source of clinical information.
Main languages used by providers in delivering HIV-related medical care to patients.
Significant level: *p < 0.05; **p < 0.0.01; ***p < 0.001.
Discussion
Variability in clinical practice may result from the use of diverse information sources to guide clinical decisions. 27 Studies suggest that there is substantial variation in the knowledge, use and perceived influence of research and different sources of evidence across health care fields.5,6,9,16,27 Our study identified seven major sources of information commonly utilized by HMCPs in their practices, some of which have been widely reported previously.5–16 The rankings indicate that ART treatment guidelines was ranked first followed by medical journals and textbooks, Internet, and professional colleagues, and these Corroborate with those reported for family physicians caring for HIV patients in a community health center setting. 6 We found that, on the average, providers in our sample used six main sources out of the 12 identified for their information needs with no significant variations noted across the demographic and medical practice characteristics.
The use of USPHS and/or IDSA ART treatment guidelines top the list with 95.6 percent of HMCPs indicating it as their main source of information for clinical practice. The Institute of Medicine defines clinical guidelines as systematically developed statements to assist practitioner and patient decisions about appropriate health care for specific clinical circumstances. 28 Clinicians, policy makers, and payers see guidelines as a tool for making care more consistent and efficient and for closing the gap between what clinicians do and what scientific evidence supports. 27 Consequently, clinical guidelines can help improve the quality of clinical decisions. Whether guidelines achieve this in daily practice is less clear because quality is often defined differently by patients, doctors, payers, and managers. 29 Providers who had never referred their patients to others for ART initiation were ardent users (aOR = 22.6) of the guidelines than those who always or sometimes made referrals. Often, HMCPs refer patients to specialists when they face a complicated or perplexing diagnosis, or one that is beyond the range or limit of their authority. Providers are also aware of the legal implications of not doing so, should a case be outside the bounds of their practice.
Medical journals and textbooks ranked second with 82.6 percent of HMCPs indicating using these resources in their practice. These resources either in print or electronic remained the most preferred source of health information as noted in previous studies.1,5,6,30 General practitioners believe that information in medical journals are more reliable than information published on the Web. 30 Of all independent factors considered in our study, only provider type significantly impacts the use of medical journals and textbooks with more physicians than PA/NPs preferring the use of these resources for their clinical information needs. Physicians were 16 times more likely than PA/NPs to use this source of evidence in their practice. This finding tends to support the conclusion reached by Stefanski et al. 6 that the background of the experts may influence their preference and epistemological commitment to a particular type of evidence. However, with the rapid rate of clinical advancements, clinicians are required to keep abreast of new and relevant publications in their specific areas and inform their practice with current research evidence. For instance, it has been reported that for general practitioners to keep up, they need to read 19 articles each day, every day of the year, 31 a feat that seems virtually impossible because of the time constraints faced by clinicians. Consequently, at best, most clinicians may read selectively from journal or textbooks by choosing what they consider important that meet their clinical information needs.
Use of the Internet among medical practitioners has increased significantly both as a means of communication and as a source for dissemination of medical and scientific information. Government and professional bodies use this resource to enable access to full-text documents and guidelines. This source was ranked third in our study with 69.5 percent of HMCP reporting its use. Our finding collaborates with those of other studies where among practitioners who use the Internet, more than 70 percent reported that the health information they find in the Web assisted in the diagnosis of patients and influences a decision about treatment.32,33 The common search engines, health-related websites, and evidence-based medicine resources accessed by medical practitioners in the Internet have been identified including Cochrane Library, UpToDate, MEDLINE/PubMed, and Clinical Evidence.12,30,34 Information obtained from these resources are intended to enable clinicians to make informed decisions about which treatments and/or prevention strategies to use for clinical conditions, but not to replace other traditional sources such as history, physical examination, availability of treatments, and local expertise.
Our study also showed that gender affects Internet use with about two-thirds of male providers and one-third of female providers indicating that they use this source to obtain HIV care and treatment information. Males were 13 times more likely than females to use this source for their clinical information needs. No other demographic or medical practice characteristics appeared to have any influence on Internet use. Our findings are similar to those reported for family practitioners’ use of the Internet for clinical information. 30 Nevertheless, it has been noted that problems of access, lack of skills, quality, readability, and applicability of information remained as barriers to effective use of the Internet as a source of health information.30,34,35 Being a moving target and depending on the search engines and websites used, changes in contents over time, and gaps in availability may have direct impacts on the quality of health information obtained from this source. Despite these barriers, the ease and convenience of accessing medical information on the Internet can help build well-informed PLWH that are open to participation in their care and clinical decision-making process with their providers. For instance, Mahroum et al. 36 in their study reported that an increase in HIV case prevalence was a strong drive for public concern in preventing HIV, leading to more HIV-related searches and interactions on the Web. The Internet therefore has the potential to be a powerful resource for meeting some of the public’s health information needs. 34
Although professional colleagues were ranked as fourth (65.2%) in the hierarchy, the ease of use and interaction among clinicians have been reported as ideal social and informal methods for gaining clinical information. 35 This source, which is often easily accessible, would provide concise, reliable, synthesized, and ready-to-use clinical information. Thus, seeking information from colleagues may provide opportunities for shared decision-making, especially as HIV remains a complicated disease. We observed no significant associations between providers’ use of this information source and their demographic or medical practice characteristics. This could indicate the existence of strong professional partnerships among clinicians at all levels that may enhance the quality, efficacy, and trust in the clinical information shared.
Although international/national conferences and other HIV care guidelines were tied in ranking to the fifth place (60.8%), they were significantly associated with provider age group and language used in administering care, respectively. Providers who were younger (36–45 years) were six times more likely than those over 45 years to attend conferences. This may be associated with the fact that younger clinicians are often more excited than older and experienced clinicians to attend conferences because they find it rejuvenating and as an excellent resource for education and camaraderie. Medicine evolves constantly and live conferences with field experts put you at the forefront of new information. 37 Attendance at national and international conferences therefore offers opportunities for providers to take a broader view of their practice in the context of the whole profession and beyond. With fast-paced changes in technology, diagnostic strategies, and therapies, conferences can alert providers to changes in patient-care guidelines and new recommendations, or identify new diagnostic and treatment possibilities coming through research. Apart from providing objectivity on one’s service and practice, 38 conferences offer opportunities for live CME, networking with colleagues, learning about new and innovative ideas for revamping tired workflows, improving patient care, and enhancing medical knowledge. HIV providers who used Spanish language in their practice were six times more likely than those who used English language to utilize other HIV care guidelines. Although guidelines are linked to evidence, it is important to note that some come at the expense of reducing individualized care for patients with special needs that may include language barriers and should be applied with discretion. Clinical guidelines developed with attention to the public good can promote distributive justice, advocating better delivery of services to those in need. 29
Pharmaceutical representatives/pharmaceutical-sponsored meeting was ranked sixth as the source of clinical information used by HMCPs (47.8%). Only provider type and language used to provide medical care were significantly associated with this source. However, model analysis indicates that language used in clinical practice was the only predictor (R2 = 0.171, p = 0.019) of this source of clinical information. Providers who use Spanish language in their practice were eight times more likely than those using English language to use this source for meeting their clinical information needs. Despite the ranking, information obtained from pharmaceutical industries generally are often less trusted because of the possibility of some level of bias toward their products and services. This is consistent with prior researches indicating that health care professionals are skeptical of the credibility of evidence obtained from the pharmaceutical industry.6,39 The National HIV telephone consultation service (Warmline) was underutilized by providers in our sample. This may be a reflection of the level of experience of the providers in our study sample as majority of them (91.3%) had 6 or more years of clinical experience. 21 The Warmline provides expert medical and clinical pharmacy guidance to clinicians caring for patients with HIV 40 and thus may help reduce the need to refer patients to specialists. HIV teleconsultation model may be particularly useful in rural and underserved communities where resources and easy access to HIV expertise may be lacking.
Study limitations
This analysis should be interpreted with some important limitations in mind. First, the provider survey participation rate of 45 percent was considered low. Our sample included mostly physicians who typically have lower survey response rates. However, our study response rate was higher than the 42–43 percent obtained for other HIV care providers-related studies at the national level.23–25 Second, although probability proportional to size sampling method was used to select participating facilities, it was not possible to weigh the providers’ self-reported responses to the survey questions because of the small sample size and this may have caused potential response bias. Therefore, our sample may not be representative of all HIV providers in Houston/Harris County, Texas. Thus, our findings may be considered as exploratory and devoid of any generalization. Finally, although the goodness-of-fit statistics obtained in our study validate our model-based analyses, the wide CIs of some adjusted odds ratios may reflect instability in the models, due to inadequate sample size and calls for cautious interpretations. Despite these limitations, the strength of our study is grounded on the fact that it provides the first comprehensive assessment of how the demographic and medical practice characteristics of HMCP influence the choice of clinical information sources they use for HIV care and treatment decision-making process. To our knowledge, little or no research has attempted to focus specifically on assessing these important relationships, which have ultimate impact on patients’ health outcomes.
Conclusion
Although the scholarly knowledge base remains one of the sources used by HMCP in their practice, our study identified the following additional ranked major resources used for their clinical information needs: USPHS and/or IDSA ART treatment guidelines, medical journal and textbooks, Internet, professional colleagues, international/national conferences, and other HIV care guidelines, among others. There is no doubt that the adoption and uptake of new technologies within the health care systems may have significant impact on the use pattern of these resources in the near future. Overall, the demographic and medical practice characteristics influenced the sources of clinical information needs of HMCPs minimally. The type of HIV provider, gender, age group, referral for ART initiation, or language used to provide medical care were the factors associated with the main information sources identified in our study. Consequently, it is important to empirically identify physicians and other health professionals’ specific information needs and information-seeking behaviors taking into consideration these characteristics. We recommend that future study should evaluate the accessibility and quality of health-related information emanating from the sources identified in our current study. User-specific differences are likely to play a role in which a particular source will be most useful in a given context. The development of tools to meet the information needs of clinicians require an understanding of the clinician and the context in which clinical decisions are being made. 41 Therefore, any integrated system intended for this purpose should provide evidence-based information in ways that reflect HIV providers’ preferences and clinical workflows. This will allow its use in specific contexts, for specific user types to answer specific questions, 42 thereby enhancing data streams quality and efficiency, and leading to improved patient care and health outcomes.
Footnotes
Acknowledgements
The authors would like to thank the HMCPs who participated in this survey; the MMP staff; members of the Community Advisory Board and Provider Advisory Board in Houston project area; the Houston Health Department; and members of the Clinical Outcomes Team in CDC’s Behavioral and Clinical Surveillance Branch of the Division of HIV/AIDS Prevention, National Center for HIV/AIDS, Viral Hepatitis, STD, and TB Prevention. O.M. conceived and designed the study, conducted the data analysis, interpreted the results, prepared the initial draft of the manuscript, and participated in the critical review and revision of the article. S.K., K.J.V., S.M.P., J.W., and E.J.E. interpreted the study findings and participated in the critical review of the article for important intellectual content concerning their specialty. All authors read and approved the final version of the article for publication. The CDC conceived the provider survey in 2009 as part of the Medical Monitoring Project, developed associated materials including data collection instrument, and provided oversight on the survey implementation in Houston/Harris County, Texas, and other participating sites. The findings and conclusions of this article are solely the responsibility of the authors and do not necessarily represent the official position of the US Centers for Disease Control and Prevention or the Houston Health Department.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship and/or publication of this article: The Medical monitoring Project (MMP) 2009 Providers’ Survey was supported by the Centers for Disease Control and Prevention (CDC) under the Cooperative agreement number PS09-937.