
Abstract
Persuasive technologies are tools for motivating behaviour change using persuasive strategies. socially-driven persuasive technologies employ three common socially-oriented persuasive strategies in many health domains: competition, social comparison, and cooperation. Research has shown the possibilities for socially-driven persuasive interventions to backfire by demotivating behaviour, but we lack knowledge about how the interventions could motivate or demotivate behaviours. To close this gap, we studied 1898 participants, specifically Socially-oriented strategies and their comparative effectiveness in socially-driven persuasive health interventions that motivate healthy behaviour change. The results of a thematic analysis of 278 pages of qualitative data reveal important strengths and weaknesses of the individual socially-oriented strategies that could facilitate or hinder their effectiveness at motivating behaviour change. These include their tendency to simplify behaviours and make them fun, challenge people and make them accountable, give a sense of accomplishment and their tendency to jeopardize user’s privacy and relationships, creates unnecessary tension, and reduce self-confidence and self-esteem, and provoke a health disorder and body shaming, respectively. We contribute to the health informatics community by developing 15 design guidelines for operationalizing the strategies in persuasive health intervention to amplify their strengths and overcome their weaknesses.
Keywords
Introduction
There is growing evidence that persuasive technologies (PTs) are effective tools for motivating behaviour change, influencing people, and promoting learning using various persuasive strategies.1–3 PTs for health – which are designed as interventions with the primary purpose of changing a user’s behaviour or attitude without using coercion or deception4,5 – have attracted the attention of researchers, physicians, and health practitioners as a novel approach for motivating desirable health behaviour using various persuasive strategies. Research has shown that PTs can be strategically designed to motivate desirable behaviour change, for example, to help people overcome addictive behaviours such as substance abuse,6–8 to promote personal wellness, to manage diseases, to engage in preventive behaviours,5,9,10 and to avoid risky behaviours.6,7,11,12
A fundamental feature of PT intervention is persuasion, an attempt to influence or reinforce behaviours, attitudes, feelings, or thoughts.4,13 Persuasion can be achieved using persuasive strategies. Socially-oriented persuasive strategies (competition, social comparison, and cooperation) are the most widely and frequently employed strategies both in persuasive health technologies and other online support interventions because of their ability to leverage social influence to motivate behaviour change. Socially-driven PTs are PTs that employ the socially-oriented strategies, competition, social comparison, and cooperation to motivate behaviour change. Studies have shown that these socially-driven PTs can be effective for motivating health behaviour change. As a result, researchers have applied them for motivating behaviour change across several health domains, including binge drinking prevention,6–8 drug and substance use prevention, HIV and sexually transmitted disease (STD) prevention and treatment, 14 smoking cessation,15,16 being physically active,17,18 and healthy eating.19–21 They have also been applied in the area of disease management, including in teaching skills for self-management of type 1 diabetes 22 and asthma. 23
Despite the wide application of the socially-driven PTs across many persuasive health domains as an intervention, there have been mixed findings regarding their effectiveness at motivating the desired behaviour change. Although there are many stories of successful socially-driven persuasive interventions with respect to their effectiveness at motivating healthy behaviour change,19,20,24–26 research has also shown that using socially-driven persuasive intervention as a tool to motivate behaviour change could be counterproductive.20,27–30 For example, Palinkas et al. 31 in their evaluation of a socially-driven intervention for primary and secondary prevention of drug and alcohol use among multiethnic female adolescents found that the intervention was largely ineffective and mainly counterproductive as the prevalence of alcohol and drug use increased significantly over the intervention period.
There is still a gap in knowledge on how and why the socially-oriented strategies (competition, social comparison, and cooperation which are the driving forces of the socially-driven persuasive interventions) could influence behaviour either positively or negatively and the mechanisms through which they motivate or demotivate behaviours. This is essential for effective operationalization of the strategies in intervention design and the success of socially-oriented persuasive health intervention in general.
To advance research in this area, we conducted two large-scale studies of 1108 and 790 (a total of 1898) participants to investigate the strengths and weaknesses of the three socially-oriented strategies (competition, comparison, and cooperation) that are widely used in persuasive health interventions design. We investigated these strategies in the context of PTs for promoting healthy eating behaviour (study 1) and PTs for motivating change in risky health behaviours such as binge drinking (study 2). Investigating two different health domains allows us to uncover a wide range of strengths and weaknesses that could be generalized across other domains. As a secondary objective, we validated the persuasiveness of the strategies and showed their comparative persuasiveness with respect to their ability to motivate healthy behaviour change.
We used prototype persuasive implementation of the individual strategies that has been validated in other studies.13,32 The results of a thematic analysis of 278 pages of qualitative data reveal important strengths and weaknesses of individual strategies that could facilitate or hinder their effectiveness at motivating desirable behaviour changes. Specifically, we found that because each of the socially-oriented strategies harnesses the principle and the power of social influence to motivate behaviour change, they share some common strengths (such as their tendency to make behaviours
However, because each of the strategies differs in their operationalization of the social influence principle, some strengths and weaknesses are unique to the individual strategies or subsets of the strategies. Some of the strengths are as follows:
Our findings also reveal that the three socially-oriented strategies differ significantly with respect to their overall persuasiveness, with the social comparison being the most persuasive of the strategies.
Our findings advance existing knowledge in the area of persuasive health intervention design by offering five main contributions. First, we provide insights into the mechanism through which socially-driven persuasive health interventions could motivate or demotivate health behaviours by revealing the strengths and weaknesses of the individual strategies that should be taken into account by PT for health designers when employing each of the strategies. Second, we provide a comparative analysis of the mechanism through which the three strategies could influence behaviour positively and negatively by comparing and mapping the strengths and weaknesses of individual strategies. Third, based on our findings, we offer 15 design guidelines on how to operationalize/implement the strategies in persuasive health intervention design to amplify their strengths and overcome their weaknesses. Fourth, we validate and compare the perceived effectiveness of individual socially-oriented strategies and show that they differ significantly in their overall persuasiveness via a large-scale study. Finally, we provide an extensive review of existing socially-driven persuasive health interventions (classifying them into interventions for health promotion and prevention and interventions for disease management). We also deconstruct how existing interventions operationalized the three socially-oriented strategies.
These contributions build on and extend our previous work 33 where we only reported a few of the strengths and weaknesses and six design recommendations based on a preliminary analysis. Besides, this study is based on a larger data set of 1898 participants and an in-depth analysis of 278 pages of qualitative data which allows us to uncover more details and provide more insights, 15 design guidelines, and extensive discussions of design implication for persuasive health intervention by situating them within the context of existing knowledge.
Related work
In this section, we present a brief overview of socially-oriented persuasive strategies and socially-driven persuasive health interventions employing the strategies.
Socially-oriented persuasive strategies
A fundamental feature of PT intervention is persuasion, an attempt to influence or reinforce behaviours, attitudes, feelings, or thoughts.4,13 Persuasion is often achieved using various persuasive strategies. Persuasive strategies are techniques that can be used in PT intervention design to promote desirable behaviours or attitudes. 32 Over the past few decades, a number of persuasive strategies have been developed. For example, Fogg 4 developed seven persuasive strategies, and Oinas-Kukkonen and Harjumaa 34 built on Fogg’s strategies to develop 28 persuasive system design strategies.
Among all the strategies, socially-oriented persuasive strategies (competition, social comparison, and cooperation adopted from Oinas-Kukkonen and Fogg4,34) have been widely employed in PT intervention for health designs and other online health support systems.3,32,35 The major distinction between socially-oriented strategies and other persuasive strategies is their ability to leverage the power of social influence to motivate behaviour change. 34
Social influence is a term used to explain the effect that other people have on us – our behaviours, beliefs, and attitudes. 36 Social influence occurs when an individual’s behaviour or attitude is affected by others. Almost all our behaviours can be shaped by the power of social influence. According to Berger, 37 ‘without our realizing it, other people’s behaviours have a huge influence on everything we do at every moment of our lives, from the mundane to the momentous occasion. Even strangers have a startling impact on our judgments and decisions’. As a result, research has applied the principle of social impact to influence behaviours in many domains including marketing, 38 education, 39 transportation, 40 environmental sustainability, 41 energy and water conservation,42,43 and of course health.17,18 For a typical example of an application of social influence principle in the marketing domain, see Amazon.com. 38 Amazon.com employed the power of social influence in their e-commerce website to motivate customers to purchase products and hence increase sales using the customers who bought this also bought that concept and the product rating tactics. Similarly, in the area of energy conservation, Gustafsson and Svahn 42 described a mobile application called Power Explorer which allows teenagers to compete with their peers on who used the less energy as a way of saving energy. With respect to education, Christy and Fox 39 investigated the impact of social influence on students’ educational performances using a leader board which allows the students to view and compare their performance with that of others. In the health domain, Toscos et al. 17 developed a mobile health application that leverages the power of social influence to motivate teenage girls to exercise by comparing their activity levels. This is in contrast with the Fish ‘n’ Step 18 which employed the self-monitoring strategy to motivate physical activity by allowing users to track their own behaviours.
Considering this increasing application of social influence principle to affect individual’s behaviours in various domains, recent research efforts have focused on developing systematic approaches for operationalizing the principle in various application domains. In the field of PTs, Oinas-Kukkonen 44 proposed three socially-oriented strategies – competition, social comparison, and cooperation:
For a detailed discussion of these strategies, see the work by Oinas-Kukkonen and Harjumaa. 34
Among all the domains of applications, the use of socially-driven PTs (which employ these strategies) in the health domain has received special attention,45,46 likely due to the importance of maintaining good health and wellness. Therefore, this study will focus on socially-driven PTs for health and wellness with special emphasis on socially-driven PTs for promoting healthy eating and socially-driven PTs for motivating change in risky health behaviour (risky alcohol behaviour change).
Socially-driven persuasive health interventions
PTs aim to bring about desirable change in attitude and/or behaviour without using coercion or deception. 4 Socially-driven PTs are PTs that employ the power of social influence (via the three socially-oriented strategies: competition, comparison, and cooperation) to motivate behaviour change. Studies have shown that these socially-driven PTs can be effective for motivating desirable behaviour change.15–21,47 As a result, researchers have employed these strategies in persuasive health technologies for motivating behaviour change in many health domains, including binge drinking prevention,6–8 drug and substance use prevention,6,31,48 HIV and STD prevention and treatment, 14 smoking cessation,15,16 being physically active,17,18 and healthy eating.19–21,49
In general, socially-driven persuasive health technologies can broadly be categorized into two main areas: socially-driven persuasive health technologies for health promotion and prevention and socially-driven persuasive health technologies for disease management.
Socially-driven persuasive health interventions for health promotion and prevention
Preventive health behaviours are behaviours that are undertaken to prevent sicknesses, detect early signs of sickness, and maintain general health and well-being. 50 Examples include smoking cessation,15,16 being physically active,17,18 healthy eating,19–21 and binge drinking prevention.6–8 Several socially-driven PTs have been developed for health promotion and prevention.
For example, National Mindless Eating Challenge (NMEC) is a mobile phone–based persuasive health intervention aimed at promoting healthy eating behaviour. 21 NMEC employs the social comparison strategy to motivate behaviour change. NMEC users are required to care for virtual pets or plants and that entails them following some healthy eating recommendations. At the beginning of the application, users are assigned tasks that are relevant to their healthy eating goals and are given the opportunity to view and compare their performance with the performance of others (social comparison). Similarly, LunchTime is a persuasive application for motivating healthy eating. 19 LunchTime employs the competition and comparison strategies to motivate behaviour change. Users assume the roles of restaurant customers, and their goals are to choose the healthiest food from a list of food choices. Each user is allowed to compare his or her performance with that of other users (competition and comparison). Finally, RightWay Café is a game-based persuasive health intervention that employs competition to promote healthy eating and physical activity. 51 At the beginning of the game, the users create a personified avatar using their own personal characteristics, such as height, gender, body frame, name, physical activity, weight, and age. Users are tasked with managing the daily activity of their avatar (such as calorie consumption and physical activity) to enable them to reach a healthy weight. The user who is most successful at managing his or her avatar’s daily diet and physical activity in a healthy way wins (competition).
Typical examples of socially-driven persuasive intervention in the area of physical activity are NEAT-o-Games, 52 Phone Row, 53 Fish ‘n’ Step, 54 and Chick Clique. 17 NEAT-o-Games 52 is a persuasive game-based intervention that employed competition and comparison to promote physical activity. The virtual racing game requires users to race with other users in their mobile network. The user’s physical activity (monitored using wearable accelerometers) is used as input to control the speed of his or her avatar in the race. At the end of every day, players’ activity points are compared and winners are announced (competition and comparison). Similarly, NEAT-o-Games and Phone Row 53 employed the competition and comparison to motivate moderate intensity physical activity by requiring users to control the movement of a smartphone racing boat using their body movement. Users compete and compare their performance with the performance of other users (competition and comparison). Fish ‘n’ Step, 54 employs competition and cooperation to promote physical activity. A user’s daily step count is associated with the growth and flourishing of a virtual fish in a tank. A user’s fish tank includes other users’ fish, thereby fostering both cooperation and competition. Users could compete with one another (competition) as an individual or as part of a team (cooperation) and are provided feedback regarding their calories burned, personal progress, and ranking. Chick Clique 17 is a persuasive mobile health application that leverages competition and comparison strategies to motivate teenage girls to exercise. Chick Clique allows up to four friends to engage in a friendly competition where the group’s walking statistics are tracked, ranked (competition), and compared with the other members (comparison).
Several PTs have also employed the socially-oriented strategies highlighted above to motivate risky health behaviour change. For example, N-Squad Web Adventure 8 is a socially-driven PT which employed the cooperation to impart knowledge about the consequences of alcohol consumption and hence discourage risky drinking behaviours. The application simulated the impact of unhealthy alcohol intake on an individual’s body including the circulatory, digestive, and nervous systems. It requires that users work as part of a group to resolve some challenges about risky drinking behaviours embedded in the application (cooperation). Similarly, Thinking Not Drinking: A SODAS City Adventure 48 is a game-based persuasive intervention for preventing unhealthy alcohol use. Thinking Not Drinking employs the social comparison to motivate behaviour change. Each game session begins with skill-specific goals that a user must accomplish. The game trains players on how to overcome peer pressure (social comparison) and avoid alcohol abuse. For a review of applications of persuasive strategies to motivate changes in alcohol and other risky health behaviours, see the work by Lehto and Oinas-Kukkonen. 35
Socially-driven persuasive health interventions for disease management
PTs have also been employed to impart disease-specific knowledge and self-management skills on patients. These include educating patients on how to manage certain illnesses, helping them conform to treatment directives by providing relevant health information, providing timely reminders to the patients, simulating health behaviour, and providing opportunities for users to rehearse health behaviours that are related to their specific illness.32,55 Persuasive interventions for disease management are mainly targeted at people who identified themselves ill and the overarching objective is to help them manage their illness or get well with the aid of the PTs.
For example, Packy and Marlon is a persuasive health intervention that helps children and teenagers self-manage their type 1 diabetes. 22 Users are tasked with keeping their virtual characters’ diabetes under control by monitoring the avatar’s vital body signs, administering insulin, and other drugs as may be necessary. 22 Packy and Marlon simulates various real-life diabetes challenges. To win, each one of the two users, Packy and Marlon, must effectively manage their characters’ diabetes and insulin intake; therefore, they must support each other (cooperation). Similarly, Bronkie the Bronchiasaurus is a persuasive health intervention aimed at imparting asthmatic children with asthma self-management skills. 23 The persuasive application simulates good and bad real-world asthma self-management skills to impart self-monitoring skills to kids with asthma. The application presents two virtual characters (Bronkie and Trakie), and users are required to help the characters control their asthma. To achieve this, users have to avoid triggers such as dust and smoke that have the tendency of impacting their asthma negatively while they go on their mission. They also need to measure and monitor breath strength, take medications, and use the inhaler as required. The user’s health decisions are determined by the character’s health outcome and a good health outcome is required to win (competition). This review is by no means exhaustive; however, it is a good representation of common practice in the area of socially-driven persuasive health technologies design.
This review shows that the socially-oriented strategies have been widely employed in PTs to motivate behaviour change across various health domains. The evaluated persuasive health interventions reported varying degrees of success at achieving the intended health objectives and mixed findings with respect to the effectiveness of the socially-oriented strategies.18,21,30,32 However, there is a lack of research into the mechanism through which the strategies could motivate or demotivate behaviours; why they may work in one context and fail in another. Revealing the strengths and weaknesses of the individual strategies would shed light on the mechanism through which these socially-oriented strategies could motivate or demotivate behaviours and suggest ways of operationalizing them to reduce their weaknesses and amplify their strengths. It will also shed light on why many persuasive interventions record varying degrees of success, mixed findings, and even failures. 28 Again, because the socially-oriented persuasive strategies are often employed en masse, there is little knowledge on their comparative efficacy.
Study design and method
In this section, we focus on the purpose of our study, the study instruments, and data collection method which were presented in a previous study. 33
Purpose
In our study, we set out to address two important issues in persuasive health intervention research: (1) investigation of the perceived persuasiveness of three socially-oriented persuasive strategies (competition, comparison, and cooperation) with respect to their ability to motivate changes in healthy behaviours and (2) investigation of the mechanism through which these three strategies could motivate or demotivate the adoption of healthy behaviours by examining their strengths and weaknesses. Specifically, we focus on two common application domains of persuasive health interventions to ensure uniformity and generalizability. They include (1) PTs for encouraging healthy eating behaviour and (2) PTs for motivating change of risky healthy behaviour (risky alcohol behaviour change).
Measurement instrument
To achieve the aims of our study, we conducted two separate empirical studies. The first study focuses on PTs for motivating healthy eating behaviours, while the second study focuses on PTs for motivating a change of risky alcohol behaviours. To gather the required data for both empirical studies, we used prototype PT implementation of each of the socially-oriented strategies. The study instruments have been validated in previous studies.13,32 Specifically, in each study, we represented each of the three socially-oriented strategies in different storyboards. In study 1, the storyboards focus on PTs for encouraging healthy eating, while, in study 2, the storyboards focus on PTs for promoting change of risky alcohol behaviours. All of the storyboards were designed by an artist following the recommended storyboard design guidelines proposed by Truong et al. 56 Storyboards, in general, provide a common visual language, which individuals from different socio-cultural backgrounds can easily read and understand. 57 Moreover, in previous research works,32,58,59 they have been found to be an effective way of evaluating and depicting persuasive strategies to users of a persuasive intervention to elicit the right responses, which will eventually inform the intervention design. In our studies, the storyboards portray a character, which represents the user (or a study participant), and his or her interactions with simulated PTs for motivating the respective health behaviour change – illustrating the individual socially-oriented strategies. For example, in Figure 1, the user is the character (in blue dress and red hair) interacting with the computer.
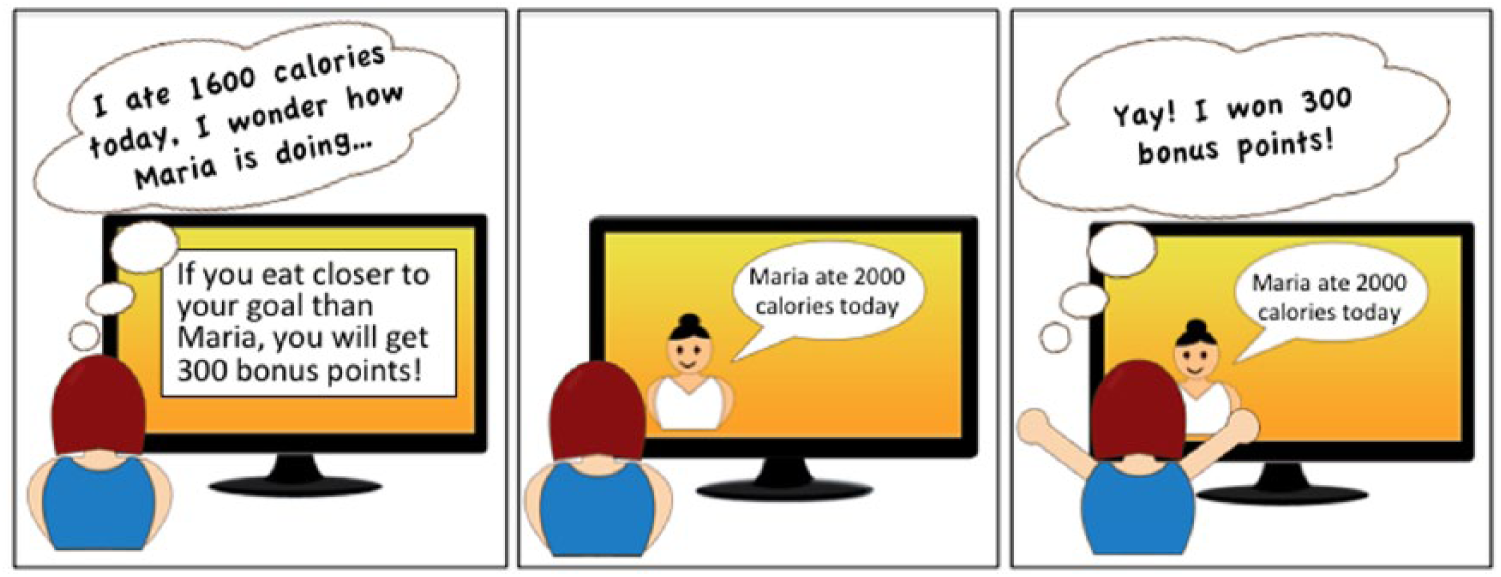
Storyboard illustrating the Competition persuasive strategies in the context of persuasive technology for motivating healthy eating behaviour – adapted from Orji et al. 32
In designing the study instruments for both of our studies, a number of steps were followed.
First, we evaluated and iteratively refined the storyboards by taking into consideration recommendations from domain experts, with whom we interacted. Upon completing the expert evaluations, we proceeded to carry out the initial online user evaluations with the sole purpose of ensuring that our storyboards accurately depicted the respective strategies. Figure 1 shows an example of a storyboard which illustrates the competition strategy in the context of PT for motivating healthy eating, while Figure 2 shows competition in the context of risky alcohol behaviour change.
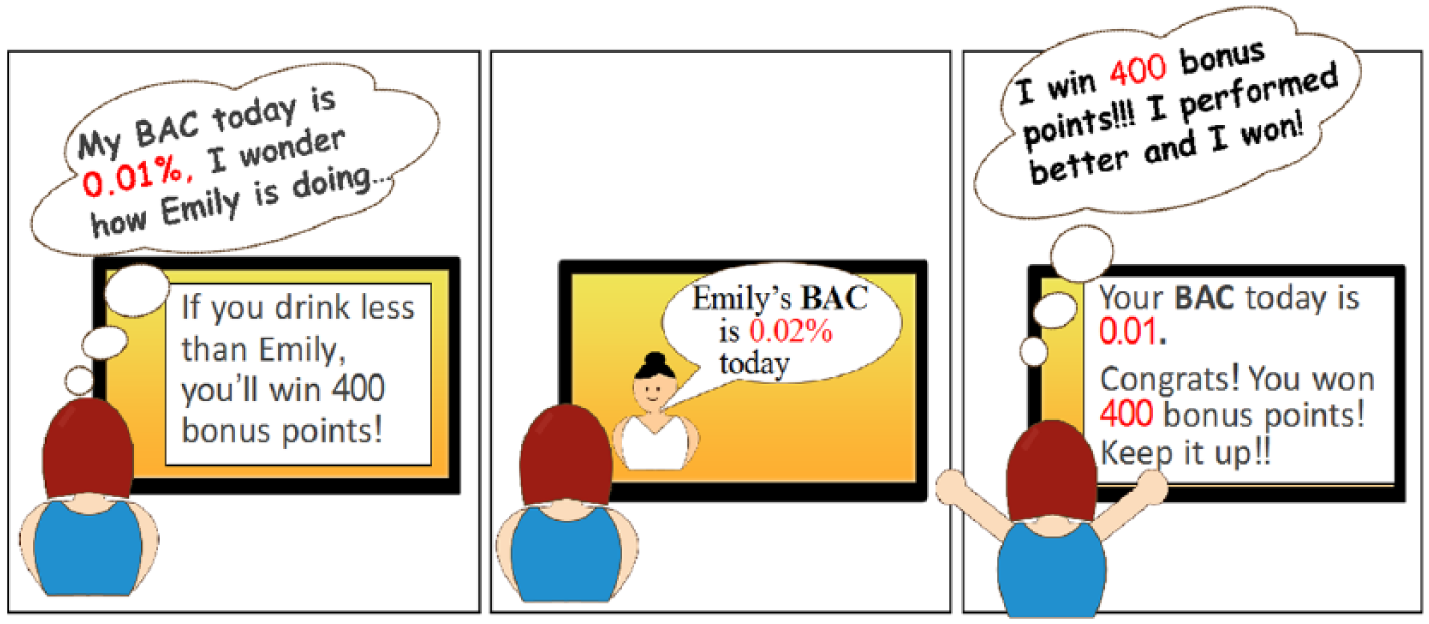
Storyboard illustrating the Competition persuasive strategies in the context of persuasive technology for motivating risky alcohol behaviour change – adapted from Orji et al. 13
Second, following each storyboard, we presented to participants a validated scale for assessing the perceived persuasiveness of each socially-oriented persuasive strategy to elicit quantitative feedback on its effectiveness. The scale was adapted from Orji et al.
32
and has been used by a number of studies.13,60,61 Specifically, we asked participants the following questions: “Imagine that you are using the system presented in the storyboard above to track your daily eating (or alcohol intake in study 2), on a scale of 1 to 7 (1-Strongly disagree to 7-Strongly agree), to what extent do you agree with the following statements: a) The system would influence me. b) The system would be convincing. c) The system would be personally relevant for me. d) The system would make me reconsider my eating (or alcohol drinking) habits.”
Third, each strategy was followed with an open-ended question. The open-ended questions allow participants to provide qualitative feedback (comments) on the strategy represented in each storyboard and how they would use the persuasive system. Furthermore, the comments allowed them to justify their ratings of each strategy with respect to its effectiveness (i.e. strengths and weaknesses). Prior to assessing the persuasiveness of each strategy, we ensured that the participants understood the strategy illustrated in the storyboard. We achieved this by asking them two comprehension questions. In the first question, we asked the participants to identify the illustrated strategy on the storyboard from a list of strategies (‘What strategy does this storyboard represent?’). In the second question, we asked them to describe what is happening in the storyboard in their own words (‘In your own words, please describe what is happening in this storyboard’). Responses from participants who answered both comprehension questions incorrectly were discarded. Together with the responses from participants who gave correct answers to the two comprehension questions, we also retained responses from participants who answered one of the comprehension questions correctly. Moreover, we asked them questions about their eating and drinking behaviours as well as demographic information.
Data collection
Study 1 was approved by the University of Saskatchewan’s ethics board, while study 2 was approved by the University of Waterloo. Afterwards, we recruited participants for the studies using Amazon Mechanical Turk (AMT): an online recruitment platform, which allows access to a global audience at a relatively low cost and ensures efficient survey distribution and reliable results.62,63
We used SurveyMonkey to design our questionnaires. To eliminate possible bias due to a fixed ordering of the storyboards, we used the page randomization functionality provided by SurveyMonkey. This randomized the positions of the storyboards (and their associated questions) by varying their ordering for each participant.
Prior to conducting the main study, we carried out two pilot studies. The first pilot study (which focused on healthy eating) consisted of 30 participants (15 were recruited from AMT and 15 from a university in Canada). The second pilot study (which focused on binge drinking behaviour change) comprised 20 participants (10 were recruited from AMT and 10 from a university in Canada). The preliminary evaluation of the pilot studies confirmed the suitability and understandability of our study instruments.
Participants’ demographic information
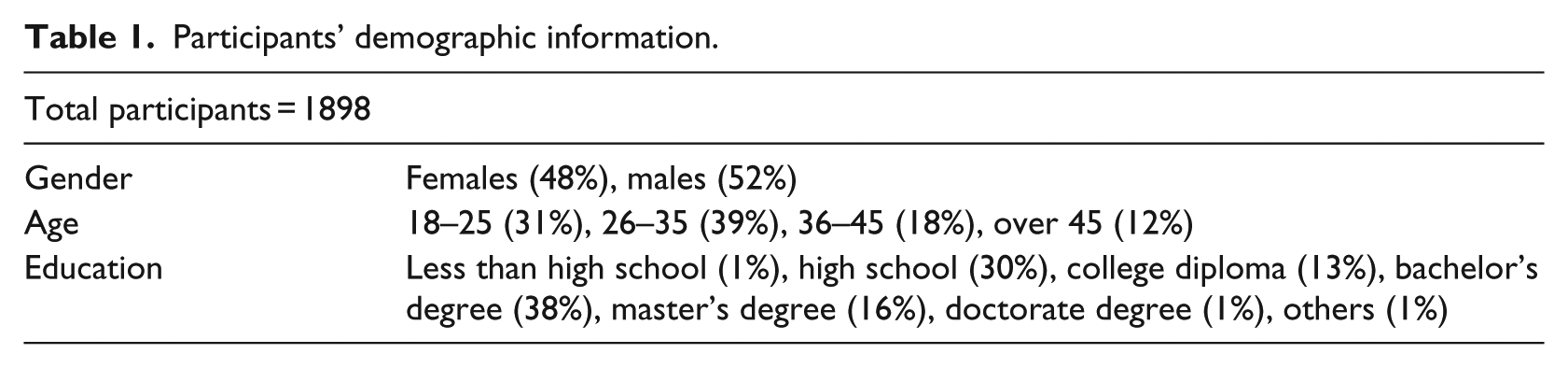
A total of 1898 valid responses were included in our analysis after filtering out incomplete and incorrect responses to comprehension and attention-determining questions. In all, 1108 of these responses came from study 1 and 790 responses from study 2. In appreciation of their time, participants received US$2 as compensation. Moreover, our participants were at least 18 years of age at the time of data collection; they also read and understood English well. Finally, specifically for study 2, participants were those who consumed alcohol often or had consumed alcohol at least once. In general, we have a relatively diverse population in terms of gender, age, and education level attained (see Table 1). Our sample in each study was relatively diverse, as there were participants from different continents and countries, such as the United States, India, Canada, Mexico, and other countries of the world.
Participants’ demographic information.
Data analysis
The two main aims of this article are as follows: (1) to examine the persuasiveness of the three socially-oriented strategies that are commonly employed in persuasive health intervention design and (2) to investigate the mechanism through which these strategies could motivate or demotivate healthy behaviour by investigating the strengths and weaknesses of the individual strategies. To achieve this, we used several well-known analytical tools and procedures. We summarize the various steps taken to analyse our data in this section:
We validated that our storyboards accurately depicted the intended socially-oriented strategy by running the chi-square test. 59
We ascertained the appropriateness of our data for analysis using the Kaiser–Meyer–Olkin (KMO) sampling adequacies and the Bartlett test of sphericity. 64
To evaluate and compare the persuasiveness of the socially-oriented strategies, we calculated the average score for each strategy and conducted a repeated measures analysis of variance (RM-ANOVA) followed by pairwise comparison. The analysis was conducted after validating for the ANOVA assumptions.
We also used notched box plot to visualize the persuasiveness of the strategies (see Figure 3).
To tease out the strengths and weaknesses of the individual socially-oriented persuasive strategies, we conducted a thematic analysis 65 of 278 pages of qualitative participants’ comments from our participants about the individual strategies.
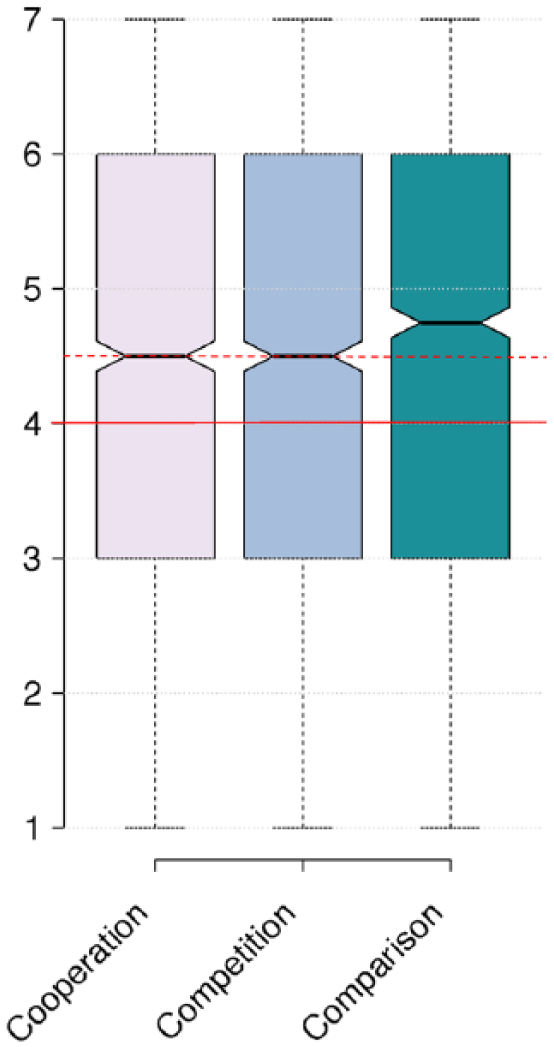
A box plot showing the overall persuasiveness (y-axis) of the strategies on a scale ranging from 1 to 7. The thick horizontal line indicates a neutral rating of 4. The notches represent the 95 per cent confidence interval for each median. The non-overlapping notches (as shown by the dotted red line) give 95 per cent confidence that Comparison differs from Competition and Cooperation.
Storyboard validation
To ensure that participants understood the socially-oriented strategy illustrated in each of the storyboards, we ran chi-square tests on the participants’ responses to the multiple choice questions that asked them to identify the strategy represented in each of the storyboards. The results for all of the three socially-oriented strategies were significant at p < 0.01. This shows that our participants understood the storyboards and that the storyboards effectively illustrated the intended socially-oriented persuasive strategies. 32
Measurement validation
We determined the suitability of our data for further analysis using the KMO sampling adequacies and the Bartlett’s test of sphericity. Our results showed that the KMO was 0.733, well above the recommended value of 0.6. The Bartlett test of sphericity was statistically significant (χ2(3) = 3148.392, p < 0.0001). These results demonstrate that our data were appropriate for more advanced analysis.28,32,66
Results
In this section, first, we show and compare the results of the overall persuasiveness of the socially-oriented strategies, which is followed by the results of the thematic analysis of the qualitative data that shows, maps, and compares the strengths and weaknesses of the three strategies.
Comparing the persuasiveness of the strategies overall
The results of the ANOVA show significant main effects of strategy type (F(1.93, 3667.470) = 10.325, p = 0.000) on persuasiveness. This means that overall there are significant differences between the three socially-oriented strategies with respect to their persuasiveness. Generally, social comparison emerged as the most persuasive of all the three strategies (significantly different from Competition and Cooperation as shown by the Bonferroni-corrected pairwise comparisons). Figure 3 shows the notch box plots of the strategies. The notch represents the 95 percent confidence interval of the median. The non-overlapping notches (as shown by the dotted red line) give 95 percent confidence that social comparison differs from competition and cooperation. In general, our participants perceive the three socially-oriented strategies as persuasive, with persuasiveness scores significantly higher than the neutral median rating of 4 (p < 0.0001), indicated by the thick horizontal red line in Figure 3.
Thematic analysis
To tease out the strengths and weaknesses of individual socially-oriented persuasive strategies, we conducted a thematic analysis 65 of 278 pages of qualitative comments about the strategies from our participants. Iteratively, we analysed the comments to identify the central themes within them and their relationship until it seemed that no further ideas were emerging from them. We classify the themes into strengths and weaknesses. We report here the themes that transpire from the analysis.
The strengths and weaknesses of socially-oriented strategies
The result of the analysis uncovered 10 major strengths and 8 weaknesses of the socially-oriented strategies. One of the strengths is common to the three strategies: They make health behaviours
In this section, we present and compare the strengths and weaknesses of the socially-oriented strategies and their corresponding supporting participants’ comments. We also map each of the strengths and weaknesses and their corresponding comments to the individual socially-oriented strategies – competition, comparison, and cooperation (Table 2 and 3).
The mapping of the strengths of the socially-oriented persuasive strategies with some sample participants’ comments.
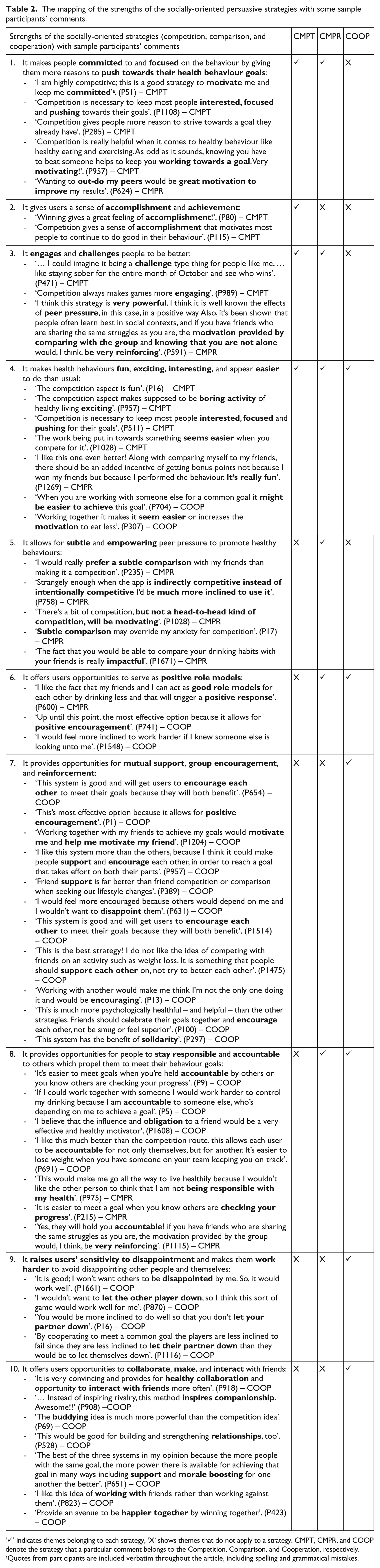
‘✓’ indicates themes belonging to each strategy, ‘X’ shows themes that do not apply to a strategy. CMPT, CMPR, and COOP denote the strategy that a particular comment belongs to the Competition, Comparison, and Cooperation, respectively.
Quotes from participants are included verbatim throughout the article, including spelling and grammatical mistakes.
Discussion
In this section, we discuss the design implications of our findings and highlight design opportunities for employing our results to inform the design of socially-driven persuasive health interventions.
Design implications of the findings: socially-oriented strategies
Socially-oriented persuasive strategies (competition, social comparison, and cooperation), which tap into the power of social influence to motivate behaviour change, have been widely employed in PTs designs. So far, research has shown some mixed findings with regard to their effectiveness at motivating behaviour change.18,20,27–29,31 Hence, there is a need for researchers and designers to understand their persuasive mechanisms, including their possible strengths and weaknesses, to ensure a more effective operationalization in future PT health interventions.
The common strengths of the socially-oriented strategies
Our findings reveal that the socially-oriented strategies share some common strengths and weaknesses (as a group) as well as some unique strengths and weaknesses (that are specific to the individual strategies). These strengths and weaknesses could facilitate or hinder their effectiveness, respectively.
Specifically, because each of the strategies explores the principle and the power of social influence to motivate behaviour, they share one strength of making behaviours
They have the tendency of making people
They
These findings suggest that PT health intervention designers could employ either the competition or the comparison strategy in their design to
Similarly, the cooperation and comparison strategies share two additional strengths in common:
They offer users opportunities to serve as
They provide opportunities for people to
These findings suggest that, apart from their tendency to make the process of adopting healthy behaviours
On the other hand, the cooperation and competition strategies are very distinct with respect to the mechanism through which they motivate behaviour change. They share no additional strengths in common apart from that shared by the three socially-oriented strategies.
The unique strengths of the socially-oriented strategies
With respect to their unique strengths, although each of the strategies explores the principle and the power of social influence to promote healthy behaviour change, they differ in their operationalization of the principle. As a result, there are some unique strengths that are specific to each of the strategies that designers need to take into consideration when employing the individual strategies.
●It gives users a sense of
This unique strength of the competition strategy could be harnessed in many ways to motivate healthy behaviour change. For example, because of the intangible and long-term oriented nature of the benefit of accomplishing healthy behaviours, many people may not derive a sense of personal accomplishment and immediate gratification directly from performing the health behaviour. According to Hartney, 68 lack of the feeling of personal accomplishment could lead people to make negative judgements of their competence and achievements and promote the feeling of insufficiency and low self-esteem and hence easily discouraged.
Adopting healthy behaviour lacks the immediate feeling of what we call healthy behaviour performance accomplishment (coined from Bandura
69
), which could be a major motivator for many people. Employing the competition strategy in PT health interventions has the tendency of filling this gap by providing individuals a sense of accomplishment derived from being able to win (by performing the desired health behaviours). Therefore, we
Participatory design approach could be adopted to understand the target audience and what is hindering them from adopting healthy behaviour and hence uncover important behavioural determinants. This would inform PT health intervention designers on the right persuasive strategies to employ to target the identified determinants and motivate behaviour change.
●It allows for
The major difference between the comparison and the other two socially-oriented strategies (competition and cooperation) is that comparison often does not involve an obvious and direct interaction with the others (peer group), which often introduces some levels of “Strangely enough, when the app is indirectly competitive instead of intentionally competitive I’d be much more inclined to use it.” (P758) – CMPR “There’s a bit of competition, but “This would also “It can create
The mapping of the weaknesses of the socially-oriented persuasive strategies with some sample participants’ comments.
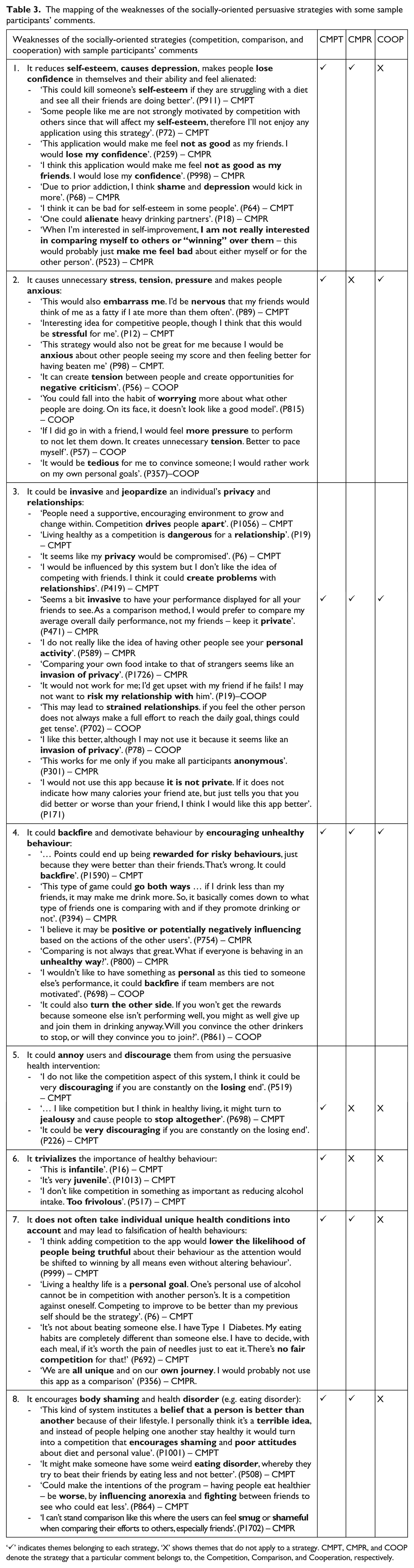
‘✓’ indicates themes belonging to each strategy, ‘X’ shows themes that do not apply to a strategy. CMPT, CMPR, and COOP denote the strategy that a particular comment belongs to, the Competition, Comparison, and Cooperation, respectively.
Therefore,
It offers opportunities to
It
It provides opportunities for
The main distinguishing factor between cooperation and the other two socially-oriented strategies (competition and comparison) is that cooperation motivates people to change together and win together by offering opportunities for collaboration, mutual support, and group reinforcement. This distinguishes it from the competition and comparison strategies which tend to focus on individual achievement. For certain behaviours, such as the health behaviours, the healthier we are as a community, the better. It is not a mutually exclusive achievement. This is supported by the participants’ comments: This is much more psychologically healthful–and helpful–than the other strategies. “ “Friend
Therefore,
Again, the unique strengths of the cooperation strategy also suggest that it may be more appropriate for designing PT health interventions targeted at people who are high in extraversion. Extraversion personality types are known for their love for making and interacting with friends.13,71 The cooperation strategy provides a unique opportunity for them to achieve that. Therefore,
Similarly, the unique strength of raising users’
Summary of the strengths of the socially-oriented persuasive strategies
In summary, the socially-oriented strategies possess 10 major strengths that shed light on the mechanisms through which they motivate behaviour change in general. Individually speaking, the competition strategy has four major strengths. They include its tendency to make
people
give a sense of
make behaviours
Similarly, the comparison strategy possesses six major strengths that provide insight into the mechanism through which it can motivate health behaviour change. They include its tendency to make
people
allow for
make behaviours
offer opportunity to serve as a
provide opportunities for people to
Finally, the cooperation strategy possesses six major strengths, which include its tendency to
make behaviours
offer an opportunity for users to serve as
provide opportunities for mutual support, group encouragement, and reinforcement;
provide opportunities for people to
offer opportunities to
With respect to the relation between the three socially-oriented strategies, the competition and the cooperation strategies are the most distinct of all. They share only one strength of making behaviours
On the other hand, competition and comparison and cooperation and comparison strategies seem equally related. Each of the pairs shares two strengths in common.
Finally, if a PT health intervention aims to promote the adoption of healthy behaviour by making the behaviour
The common weaknesses of the socially-oriented strategies
Our findings reveal that the socially-oriented strategies share some common weaknesses as well as some unique weaknesses (that are specific to the individual strategies). The weaknesses shed light on the mechanism through which the strategies could hinder the effectiveness of any PT health intervention at motivating the desired behaviour change.
The three socially-oriented strategies share two main weaknesses in common:
They could be
They could backfire and encourage unhealthy behaviour.
This means that PT health intervention designers should plan adequate mechanisms to deal with these weaknesses and we propose some mechanisms in Table 4.
Summary of the design guidelines for socially-driven persuasive health intervention design, not in any particular order.

In addition to the weaknesses shared by the three strategies, the competition and comparison share three weaknesses in common:
They could reduce
They do not often take individual unique conditions into account and may lead to falsification of behaviour.
They encourage
The findings suggest that designers employing the competition or the comparison strategies in PT health intervention design should devise approaches to overcome the loss of self-confidence and self-esteem often associated with these strategies. Therefore,
To avoid creating opportunities for body shaming when employing the competition and comparison strategies,
Similarly, the competition and cooperation strategies share only one additional weakness in common:
They could cause unnecessary
This finding suggests that the direct involvement and engagement with other people, inherent in the operationalization of the competition and cooperation strategies, is probably what causes anxiety and stress since that is the major difference between the competition and cooperation strategies and the comparison strategy. Comparison strategy tends to involve indirect peer pressure. This is supported by the following participants’ comments about the cooperation strategy: “If I did go in with a friend, I would feel “It can create
Therefore,
On the other hand, the cooperation and comparison strategies are very distinct with respect to their weaknesses. They share no additional weaknesses in common apart from that shared by the three socially-oriented strategies.
The unique weaknesses of the socially-oriented strategies
There are some weaknesses that are specific to some of the strategies that designers need to take into consideration when employing the strategies:
It could
It
Some of our participants reported that the competition strategy could trivialize the importance of health behaviour and discourage them. This is captured in the following sample comments: “I do not like the competition aspect of this system, I think it could be very “Living a healthy life is a “I don’t like competition in something as important as reducing alcohol intake.
The first comment suggests that people get discouraged when they are constantly losing in a competition not necessarily because of their inability to perform the desired behaviour but their inability to outperform the other party and win the competition. This is mostly because competition allows only one winner at a time in most cases irrespective of each individual’s performance. Therefore,
Summary of the weaknesses of the socially-oriented persuasive strategies
In summary, the socially-oriented strategies possess eight major weaknesses that shed light on the reasons they may not work as expected in some PT health interventions in general. Individually, the competition strategy is associated with all of the eight weaknesses listed in Table 3.
On the other hand, the comparison strategy possesses five major weaknesses, which include its tendency to
reduce
be
encourages
not often take individual unique conditions into account and may lead to
Finally, the cooperation strategy possesses only three major weaknesses including its tendency to
be
cause unnecessary
Summary of design guidelines
Although each of the socially-oriented strategies harnesses the principle and the power of social influence to motivate behaviour, they differ in their operationalization of the principle. As a result, there are some common strengths and weaknesses that are shared by the strategies and, at the same time, some unique strengths and weaknesses that are specific to each of the strategies. Designers need to take these strengths and weaknesses into consideration when employing the strategies as they would impact the success of the socially-driven persuasive health interventions. Therefore, we have developed some design guidelines based on our findings to guide the design of socially-driven persuasive health interventions employing the competition, social comparison, and the cooperation strategies. Since most of the design recommendations are already discussed in the ‘Discussion’ section, Table 4 presents only a summary of some guidelines. The guidelines are by no means comprehensive or exhaustive; many other guidelines can be generated from the mapping of the strengths and weaknesses of the strategies presented in Tables 2 and 3, respectively.
Limitations
First, we report the perceived persuasiveness of the socially-oriented strategies implemented in storyboards; the actual persuasiveness may differ when implemented in a specific socially-driven persuasive health intervention and evaluated in real-world. Therefore, in future work, we plan to examine the persuasiveness of the strategies along with their strengths and weaknesses in an actual PT health intervention. Second, our work has benefitted from the large-scale exploratory studies of the strategies with respect to unhealthy alcohol behaviour change and healthy eating behaviour and we can claim applicability in other health behaviour domains (because of the high-level nature of the storyboard depicting the strategies); however, our results may not generalize to other behaviour domains. Therefore, the results should be applied with caution to other health behaviour domains. Finally, it is possible that the study population distribution may differ across the two studies.
Summary and conclusion
Socially-driven persuasive health interventions have recorded some mixed findings regarding their effectiveness at motivating health behaviours. The socially-oriented persuasive strategies (competition, social comparison, and cooperation) are the major components of socially-driven persuasive health interventions and have been widely employed. In this study, we investigated the mechanism through which the three socially-oriented strategies could influence health behaviours either positively or negatively by exploring their strengths and weaknesses via a large-scale study of 1898 participants. The findings show that because each of the strategies harnesses the principle and the power of social influence to motivate behaviour change, they share some common strengths (such as their tendency to make health behaviours
However, because of the differences in the operationalization of the social influence principle across the three strategies, some strengths and weaknesses are unique to the individual strategies or subsets of the strategies. Some of the strengths are as follows: competition makes one
As a secondary objective, we validated the persuasiveness of the strategies and showed their comparative persuasiveness with respect to their ability to motivate the desired healthy behaviour change. Our findings show that, in general, the socially-oriented strategies are perceived as persuasive with the social comparison strategy being the most persuasive of all.
Based on the findings, we developed 15 design guidelines for implementing the socially-oriented persuasive strategies in health interventions to overcome their weaknesses and amplify their strengths.
Footnotes
Acknowledgements
R.O. held the NSERC Vanier Canada Graduate Scholarship and NSERC Banting Fellowship while conducting the studies reported in this paper. The authors thank the reviewers for their insightful comments and their study participants.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.