
Abstract
The evolving field of persuasive and behavior change technology is increasingly targeted at influencing behavior in the area of health and wellness. This paper provides an empirical review of 16 years (85 papers) of literature on persuasive technology for health and wellness to: (1.) answer important questions regarding the effectiveness of persuasive technology for health and wellness, (2.) summarize and highlight trends in the technology design, research methods, motivational strategies, theories, and health behaviors targeted by research to date, (3.) uncover pitfalls of existing persuasive technological interventions for health and wellness, and (4.) suggest directions for future research.
Keywords
Introduction
Persuasive Technology (PT) are interactive systems designed to aid and motivate people to adopt behaviors that are beneficial to them and their community while avoiding harmful ones. The use of PT, aimed at bringing about desirable change by shaping and reinforcing behavior and/or attitude is growing in virtually all areas of health and wellness. Over the past decade, several PT have been developed targeted at impacting one or more aspects of health and wellness. These technologies can broadly be classified into two main category: PT for health promotion and prevention and PT for disease management.1,2 PT for health promotion and prevention are targeted at behaviors undertaken by individuals for the purposes of preventing illness, detecting early illness symptoms, and maintaining general wellbeing. 3 Examples include being physical activity,4–6 healthy eating,7–9 smoking cessation,10,11 avoiding risky sexual behavior and unwanted pregnancy,12,13 and dental health.14–16 PT for disease management help patients improve health-related self-management skills such as teaching them how to manage certain illnesses, helping them comply and adhere to treatment directives. 17 Each of these health behavior domains has attracted considerable attention.
There is an increasing interest and investments in developing and using technology to promote health and wellness by various stakeholders including health and wellness researchers and practitioners, technology designers, and public health and government agencies. Therefore, it is necessary to conduct an empirical review to reevaluate and uncover important trends, best practices, gaps, and opportunities for improvement. In addition, research on this topic is fragmented, using many different approaches, methods and concepts. A literature review can help bring these disparate sources together.
Thus, in this paper, we present an empirical review of 16-years (from 2000 to 2015) of PT studies across various health and wellness domains with the aim of: (1.) answering important questions regarding the effectiveness of persuasive technology for health and wellness; (2.) highlighting and summarizing emerging trends in the technological intervention design, research method, target health behavior, use of motivational strategies and behavior theories – which is important in guiding and setting roadmap for subsequent research agenda; (3.) uncovering pitfalls of existing PT interventions for health; and finally, (4.) suggesting directions for future research. This review serves as a reference for future research in this area, providing a comprehensive overview that will be a useful starting point for anyone interested in an overview of persuasive technology for health and wellness by systematically analyzing and categorizing the scattered research effort in this area under useful headings and highlighting the merging trends.
Materials and methods
As our goal is to systematically analyze persuasive technology in the health domain, we employed quantitative content analysis, a technique which enables comparison, contrast, and categorization of data according to different themes and concepts. 18 This entails collecting data in a rigorous way, paying special attention to the objectivity of the results.
For our literature search, we used the Elsevier Scopus database as our first data source with the search terms “Persuasive Health Technology”, “Persuasive Technology and Health”, “Behavior Change Technology and Health” “Persuasive Technology”, “Technology and Health Interventions”. Scopus is the largest abstract and citation database of peer-reviewed literature. 19 We also searched PubMed, EBSCOHost, Springer, the ACM Digital Library, IEEE Xplore, and Google Scholar with the same search term. This ensures good coverage of technological health interventions across various fields including Human-Computer Interaction (HCI), medical and health informatics, health information systems, and other related research field. Finally, we scanned through the reference lists of the included studies to find further potentially relevant studies. The search resulted in 1842 unique titles, of which 544 articles were deemed relevant following a title examination. After the abstracts of each article were reviewed, a total of 85 articles that were published from 2000 to 2015 are included in this analysis. We included only articles that discussed the design and evaluation of new PT for health and wellness or an evaluation of existing PT for health and wellness and are published in English. We also excluded papers describing the design and development of PT for health without an evaluation. The study identification process is as summarized in Figure 1.
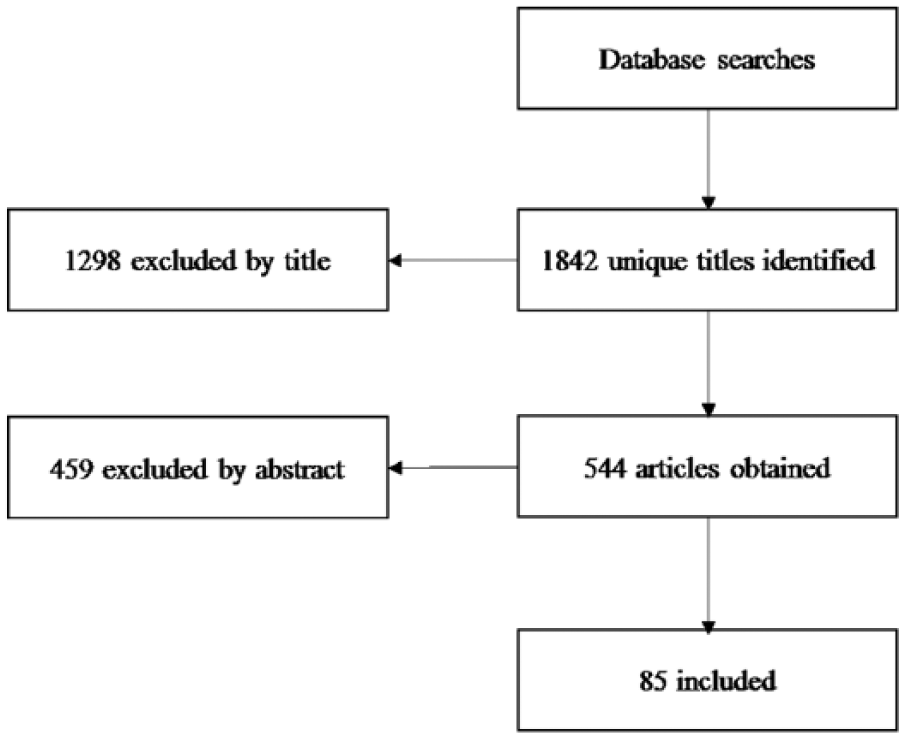
Included study identification process.
Analysis and coding scheme
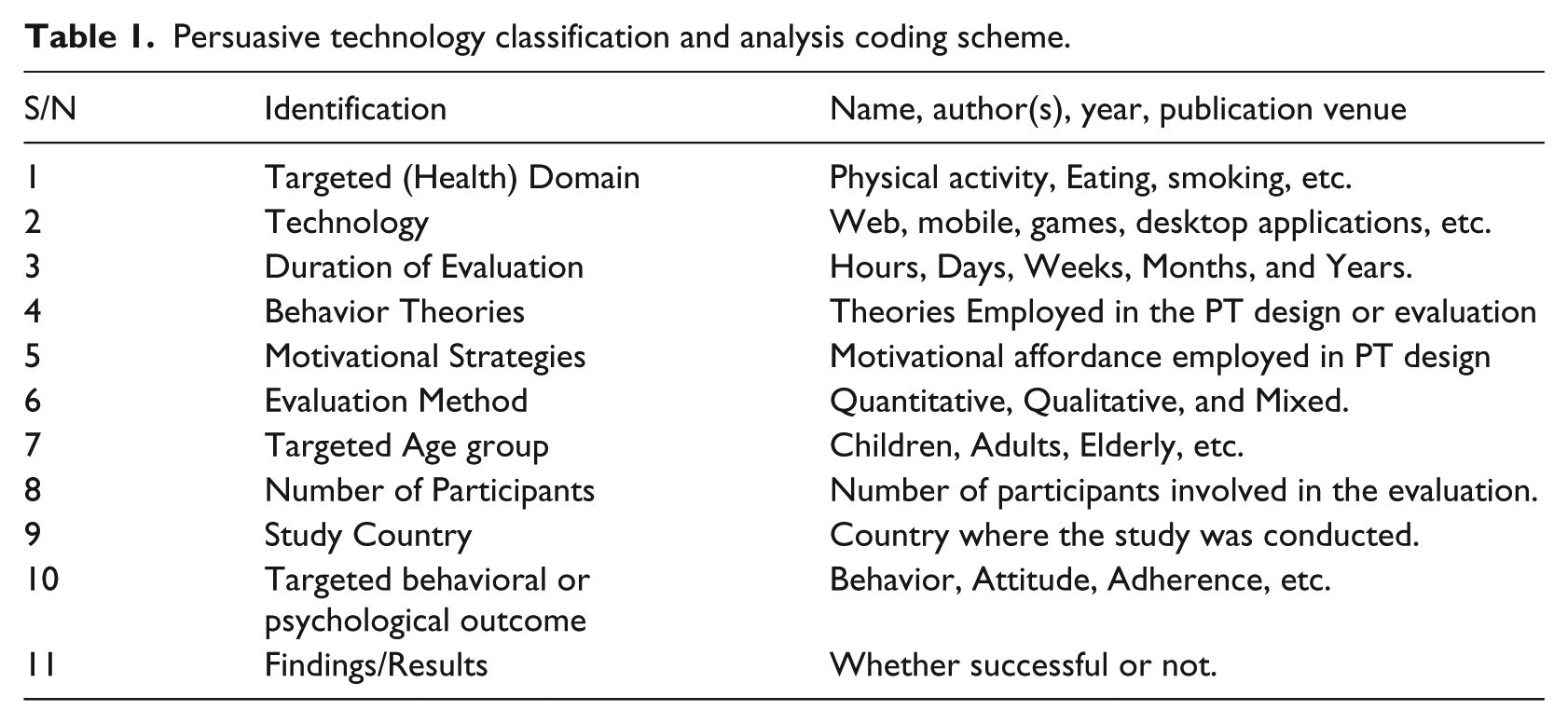
In the second stage of the review, we coded the articles. To achieve this, we iteratively developed a coding sheet for analyzing PT, see Table 1. Next, we went through each of the articles and classified their data using the coding sheet. The coding sheet included the following parts (see Table 1):
Persuasive technology classification and analysis coding scheme.
Results
The analysis of existing PT for health and wellness revealed some interesting insights and trends. Below we present our findings under various categories including: evaluation outcome, employed technology platform, persuasive and motivational strategies, behavior theories, targeted behavior domain, theory, strategy, and outcome mapping. The detailed summary of all the reviewed studies is presented in the Appendix.
Persuasive health technology by year and country
As shown in Figure 2, a relatively large proportion of empirical studies of PT for health and wellness are published after 2005 compared to before 2005. However, there was a big jump starting in 2005, and after that it has been relatively stable, despite some year to year fluctuation. It is important to highlight that although the year 2015 seems to have the least number of studies since 2005 (Figure 2), it is probably because the study was completed halfway through 2015, with many of the publications for the year still pending.
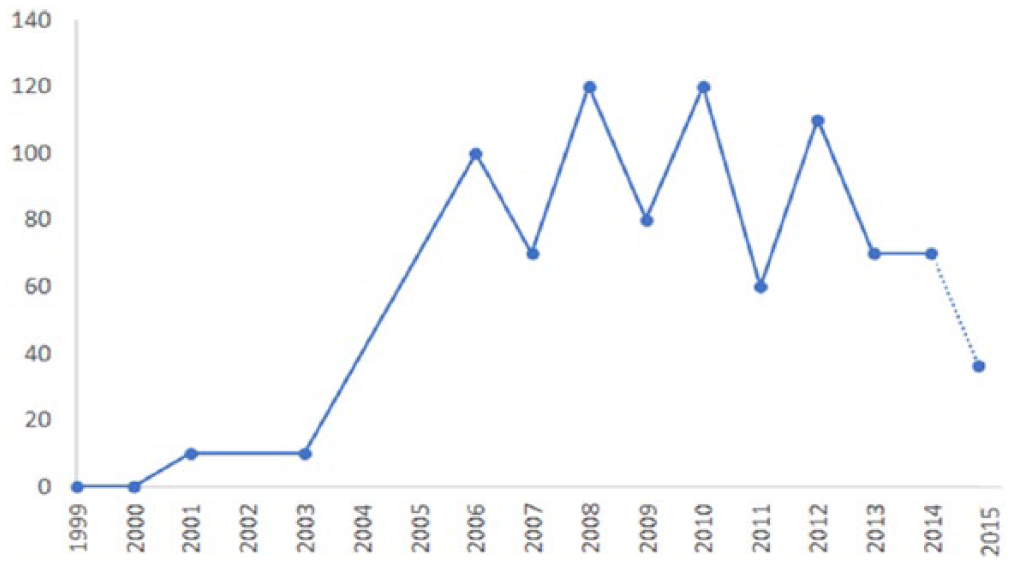
Persuasive technology for health and wellness trend by year.
As shown in Figure 3, the studies were conducted in 21 different countries with the USA leading the list with a total of 38% of all the studies. USA is followed by the Netherlands with 19%. Taiwan is in the third place with a total of 6% and Finland and Japan are the fifth place, having 5% each of all the studies.
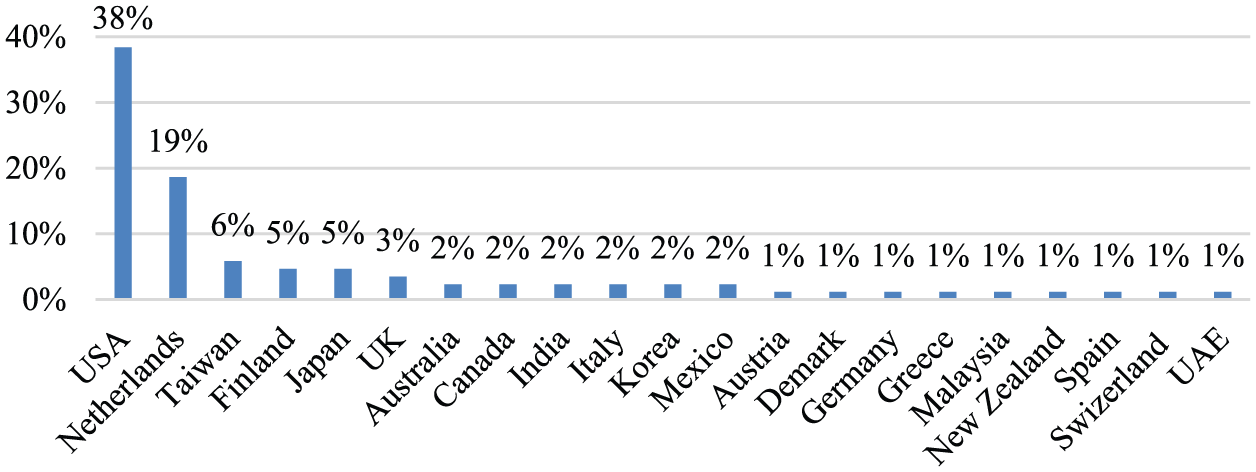
Persuasive technology for health and wellness trend by study country.
Evaluation outcome: does persuasive health technology work? Effectiveness of persuasive health technology
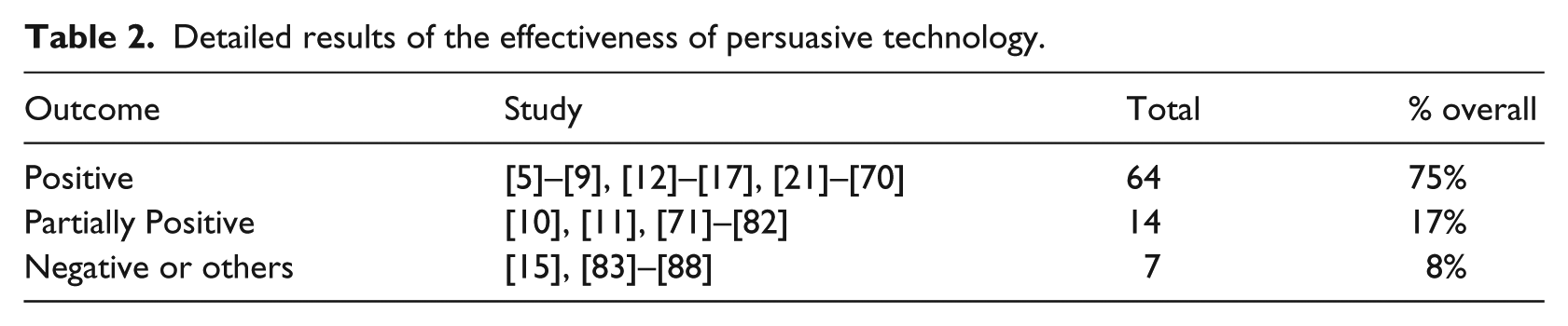
Figure 4, summarizes the reported results from the evaluation of the PT for health and wellness reviewed in this paper. Of the 85 reviewed studies, 64 (75%) reported fully positive outcome from using the PT to impact specified health behavior. Fourteen studies (17%) reported results partially positive – a combination of positive with negative or no effect results. Only 7 (8%) of all the studies were unsuccessful at achieving their intended persuasion objective – finding negative results, no positive results, or no results at all. 20 The results of the effectiveness of PT for health and wellness are detailed in Table 2.
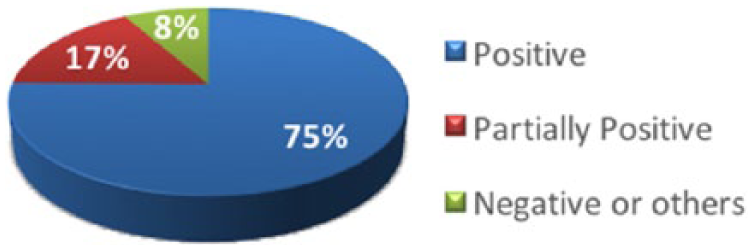
Summary results of the effectiveness of persuasive technology.
Detailed results of the effectiveness of persuasive technology.
Technology platforms for persuasive technology
Figure 5 summarizes the major technology platforms employed by PT for health and wellness designers. The most frequently employed technology platforms emerged to be mobile and handheld devices with a total of 27 (28%). It is followed by games with 16 (17%). Games category included all the studies that delivered their PT interventions in the form of games irrespective of whether the game is mobile-based, web, or runs on a stand-alone desktop. In addition, persuasive implementations on the web and social networking sites are common among the studies reviewed. Ambient and public display is the least frequently employed platform with 5(5%).
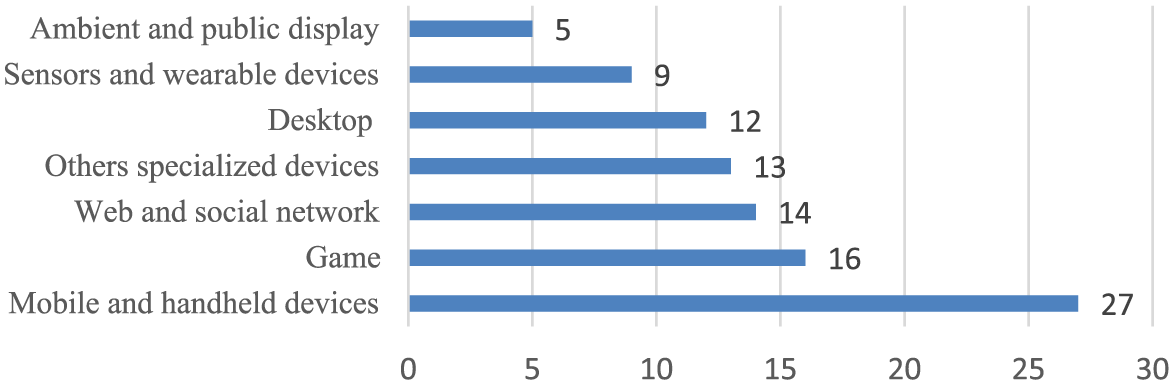
Persuasive technology platforms.
Persuasive strategies and motivational affordance employed
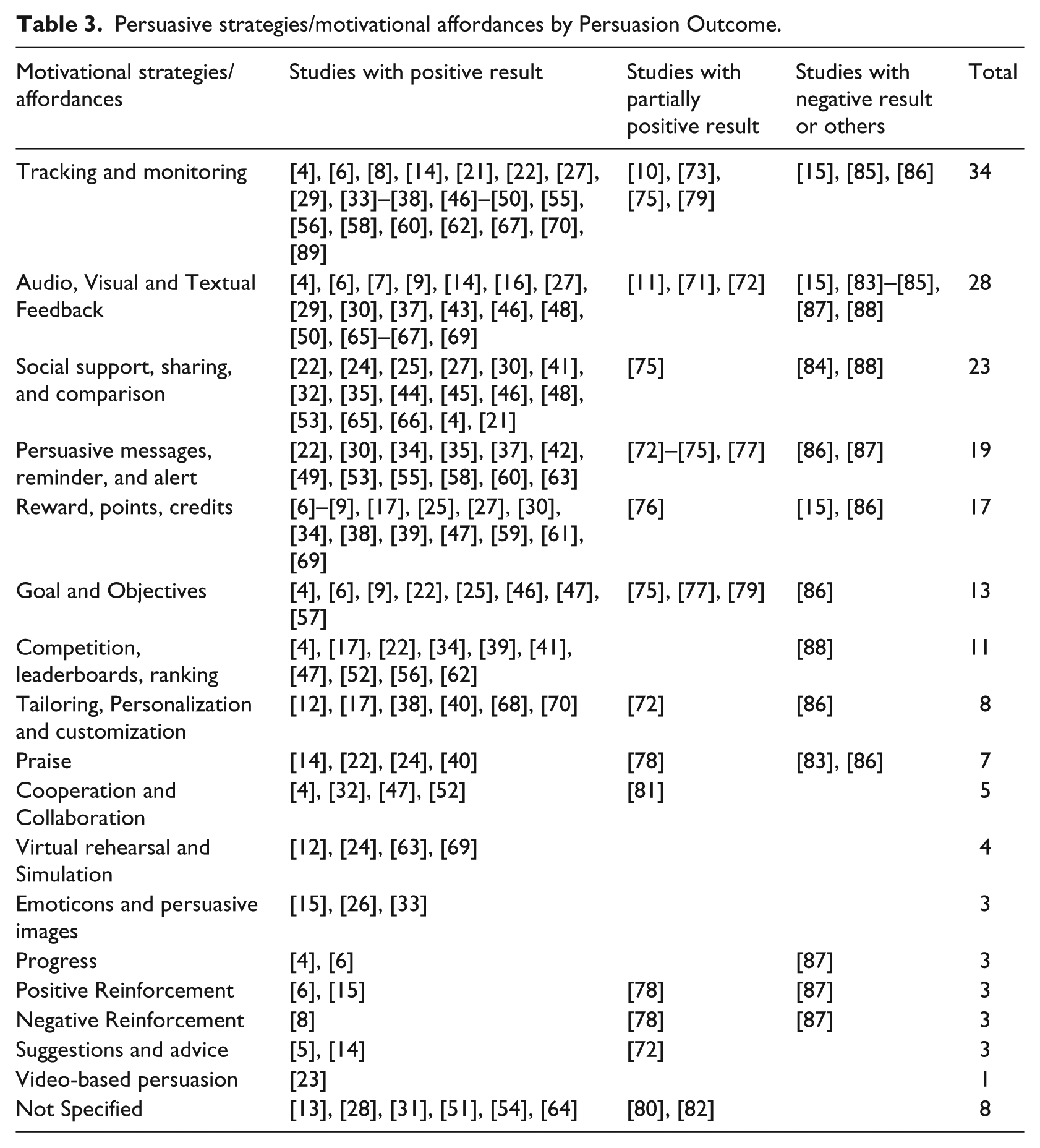
The reviewed studies employed several persuasive strategies and motivational affordances to bring about the intended persuasion outcomes. Table 3 shows the prevalent motivational affordance and persuasion outcome. Tracking and monitoring is the most frequently employed strategy (with a total of 34 studies), followed by feedback (28). It is important to note that approximately 80% of the reviewed studies employed more than one motivational strategy (see the Appendix) and are categorized accordingly. Some of the studies did not specify their strategy.
Persuasive strategies/motivational affordances by Persuasion Outcome.
Behavior theories employed
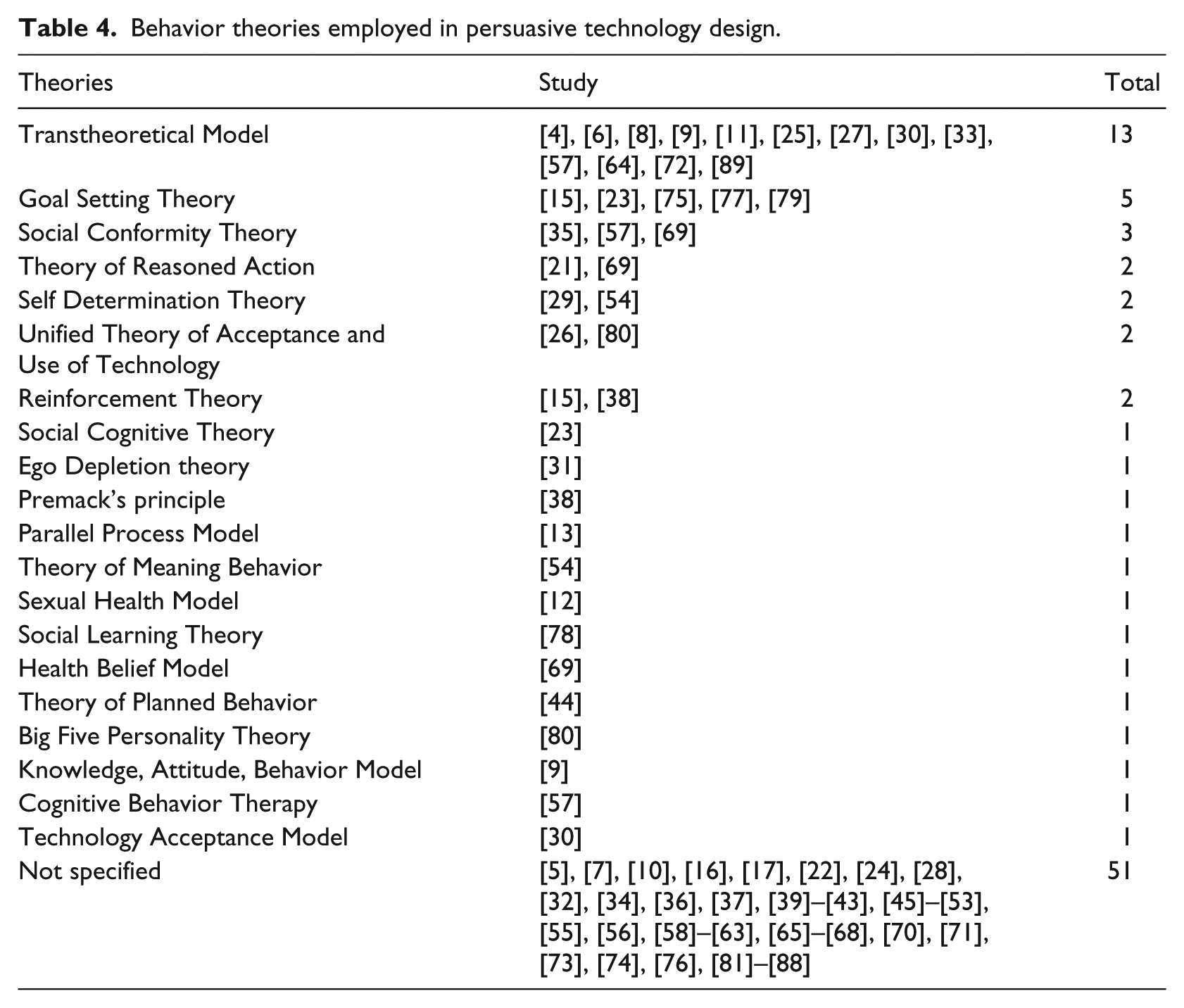
Examining behavior change theories employed reveals that more than half of all the studies reviewed (55%) are not informed by any theory or did not specify the theories that inform their PT intervention design, see Table 4. Even among the studies that specified the theories that informed their design, most of them only mentioned the theories without actually specifying how the theories informed the actual PT intervention design components and/or evaluation. Transtheoretical model of change (TTM) is the most frequently employed theory with a total of 13 (14%) studies. Most of the studies based on theories employed more than one theory or adapted constructs from more than one theory.
Behavior theories employed in persuasive technology design.
Targeted health behavior domain of persuasive technology by persuasion outcome, motivational strategies, and behavior theories
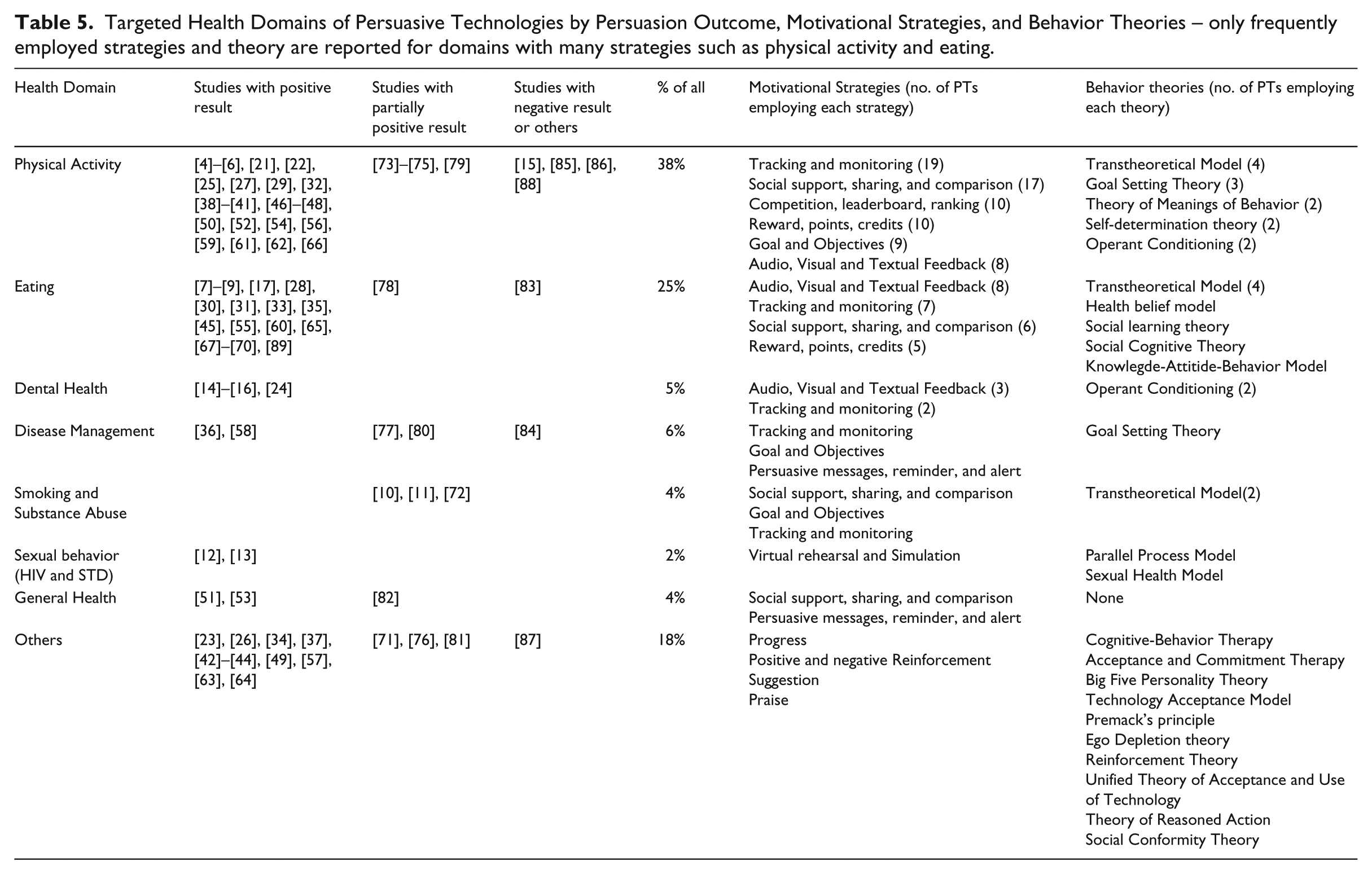
As can be seen from Figure 5 and Table 5, the PT for health and wellness reviewed in this paper fundamentally focused at imparting eight major health behavior domain, including physical activity, eating, dental health, disease management, smoking and substance use, sexual behavior, general health, and others. “Others” consists of health behaviors that appeared less frequently (in all cases, only one study looked to the behavior) such as sleeping, and depression. Physical activity has attracted the most research interest, making up 38% of all the reviewed studies, followed by healthy eating with a total of 25%.
Targeted Health Domains of Persuasive Technologies by Persuasion Outcome, Motivational Strategies, and Behavior Theories – only frequently employed strategies and theory are reported for domains with many strategies such as physical activity and eating.
Health behavior domain and persuasion outcome
With respect to the persuasion outcomes, it is difficult to speak specifically to the domain specific effectiveness of PT for health and wellness because of the variability in the number of studies from each domain included in this analysis and other domain-specific factors that could influence the effectiveness of PT including the instantiation and operationalization of the persuasive strategies and the duration of evaluation. However, based on the results from the analyzed studies, PT targeted at smoking and substance abuse related behaviors appear to be the least successful with respect to the effectiveness of PT at promoting the desirable change in the domain. All three studies (100%) on smoking and substance abuse analyzed only reported partially positive results – a combination of positive with negative or no effect results. This is followed by disease management with 60% of all the studies reporting either negative or partially positive results. On the other hand, PT targeting dental health and sexual behaviors seem to be the most successful with respect to the effectiveness of PT at promoting the desirable change in the domain. All the studies related to dental health and sexual behaviors (100%) analyzed reported positive results. For eating related behaviora, 91% of all the studies reported fully positive results while for physical activity, 75% of all the studies reported fully positive results. Similarly, 67% of all the studies related to general health reported fully positive results. Finally, for the “Others” category which consists of health behaviors that appeared less frequently in our study, 73% of all the studies reported fully positive results. Figure 6 presents the comparative effectiveness of PT by targeted health domain.
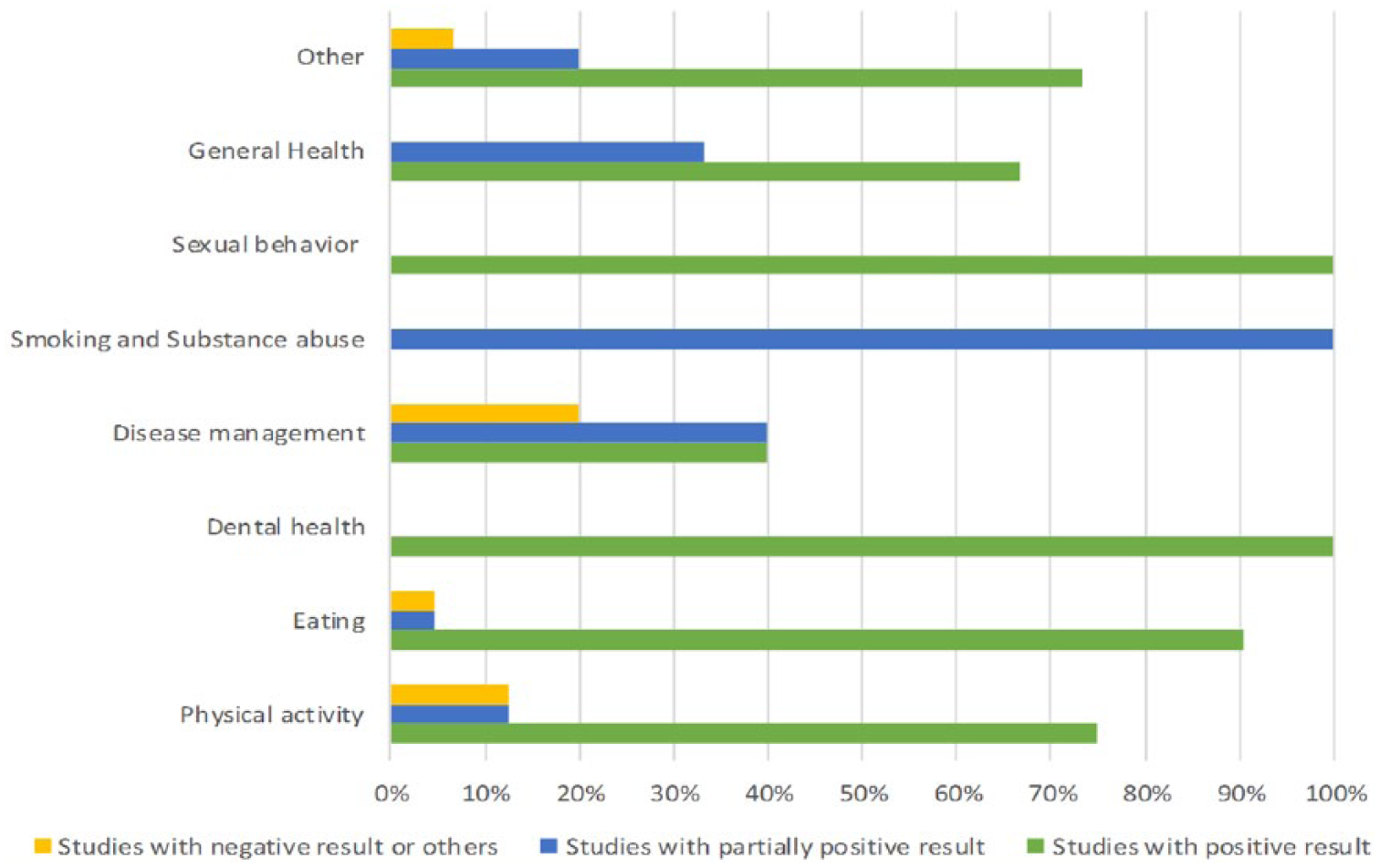
Comparative effectiveness of PT by health domain.
Health behavior domain and motivational strategies employed
Some strategies were more frequently applied in one health and wellness domain than others. For example, tracking and monitoring is a common motivational and persuasive strategy in the physical activity and eating domain. As shown in Table 5, column 6, tracking and monitoring was employed 19 times and 7 times by PT targeting physical activity and eating behaviors respectively. Similarly, simulation and rehearsal is a popular strategy in the sexual behavior domain.
On a general note, tracking and monitoring; social support, sharing, and comparison; competition, leaderboard, and ranking; and rewards, points, and credits (listed in decreasing order of frequency) emerged as the top four strategies that are commonly employed by PT interventions in the physical activity domain. Similarly, for eating behavior tracking and monitoring; audio, visual, and textual feedback; and social support, sharing, and comparison (listed in decreasing order of frequency) emerged as the top three strategies. Finally, for dental behavior, audio, visual, and textual feedback followed by tracking and monitoring were the commonly employed strategies.
The variations in the popularity of the strategies across various health and wellness intervention domain may be due to the fact that some strategies are easier to operationalize in one domain than the other. However, there is no clear relationship between the strategies or the number of strategies employed in the PT design and persuasion outcome – PT effectiveness. This is probably due to many possible factors that could mediate the effectiveness of the strategies employed in PT including differences among the target population and the need to tailor the strategies to be appropriate for the target audience. The possible variations in operationalization and instantiations of the strategies is another possible factor.
Health behavior domain and behavior theories employed
Although most analyzed studies are not based on any known behavior theories or did not specify the theories that informed the design, for those that did, some theories seem to be more popular in one health and wellness domain than the other. As can be seen from from Table 5, column 7, theories such as the Transtheoretical model is more prevalent in the smoking and substance abuse, physical activity, and health eating domain. Similarly, goal setting theory is used mostly in physical activity and disease management domain. The variations in the popularity of the theories across various health and wellness intervention domains may be due to the fact that some theories are more suitable for some domain and can be easily operationalized than others. For instance, theories such as Transtheoretical model were developed in the context of smoking cessation. Although, it has since been proven effective for developing interventions targeting other health and wellness domains, it is more popular in the smoking cessation interventions as shown by this study. However, there is no clear relationship between the theory or the number of theories used to inform the PT and the persuasion outcome – PT effectiveness.
Targeted behavioral/psychological outcomes
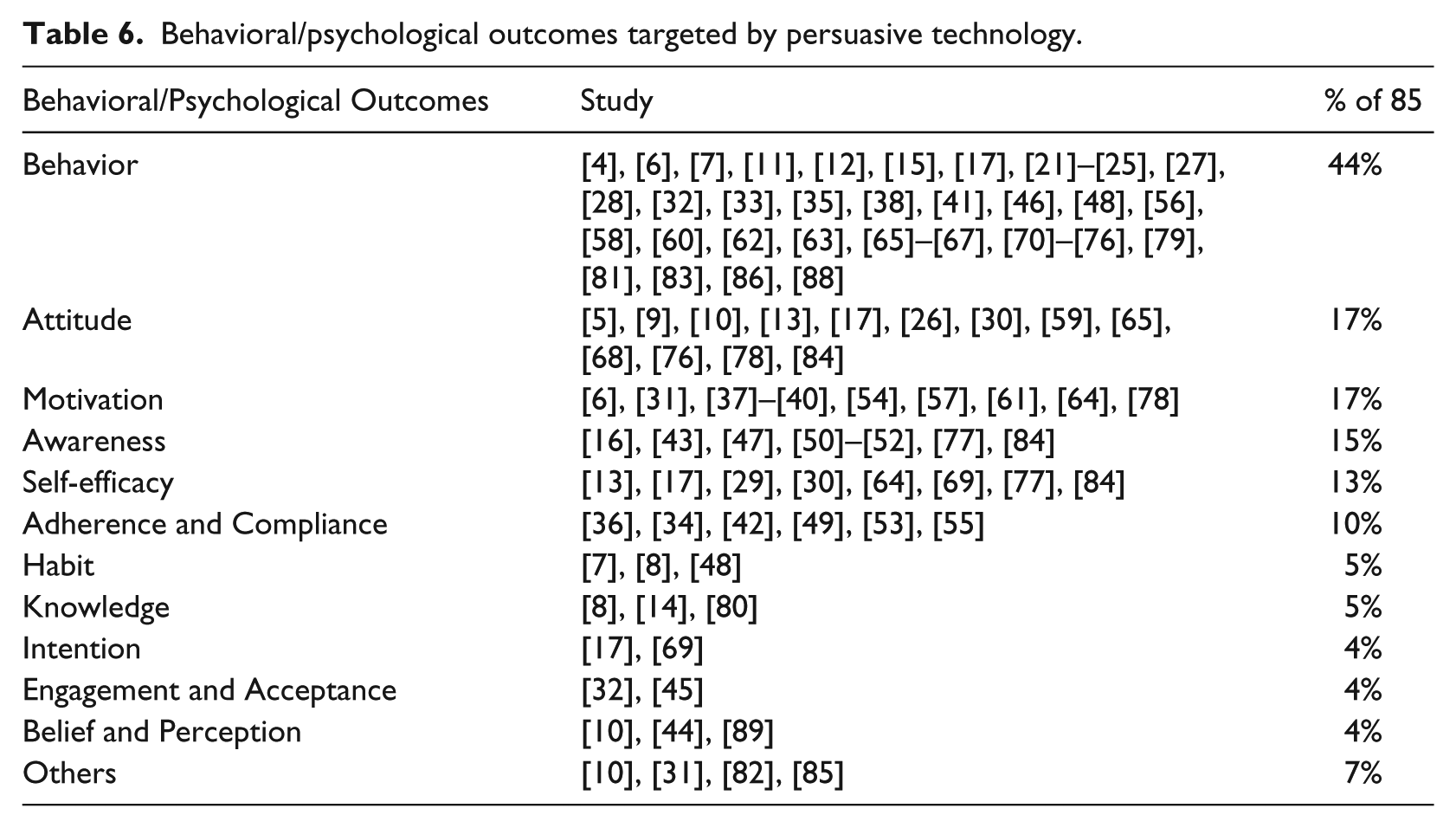
With respect to the behavioral or psychological outcome targeted, as shown in Table 6, the studies are targeted at change in 12 distinct outcomes. Nearly half of all the studies (44%) are targeted at actual Behavior change (either promoting desirable behaviors or motivating change of undesirable behaviors). Seventeen percent (17%) were targeted at Attitude change and 17% at increasing Motivation, while an additional 7% were categorized as “Other” a category housing all studies that either did not specify the targeted behavioral outcome or included a targeted outcome unrelated to behavior. Most of the studies targeted more than one behavioral outcome and hence assessed the effectiveness of their PT on more than one behavioral outcome. As a result, some studies belong to more than one category in Table 6. The behavioral outcomes were not often measured using standardized instruments; creating or reinventing measurement instruments is a common trend among reviewed studies. Again, some studies that were targeted at actual behavior ended up evaluating the effectiveness of their systems by measuring some mediating psychological outcomes such as Attitude and Motivation because of the long evaluation period needed to establish actual change in behavior.
Behavioral/psychological outcomes targeted by persuasive technology.
Study methodology used by persuasive technology
Data collection and analysis trend
Table 7 summarizes the methodology employed by the reviewed paper in evaluating their PT for health and wellness. Mixed method emerged as the dominant method. Of all the studies, 46% employed mixed method combining both quantitative and qualitative approaches in their study. This is followed by the quantitative approach, accounting for 39%. The most commonly used approach for collecting quantitative data was questionnaire/survey. A few studies (mostly physical activity motivating PT and games) collected additional quantitative data via logged data of user’s behavior and system usage.6,34,45,55–57,62,77,88–90 A fully qualitative approach is the least popular with only 15% of all the studies using the approach. The most frequently used qualitative methods are interviewing, focus-group discussion and observation of participants’ behaviors and PT use.
Study methodologies used by persuasive technology.
Regarding the data analysis methods used in the reviewed studies, frequencies, percentages, and means and standard deviations are the most popular methods. ANOVA, Regression analysis and t-tests are the commonly used as inferential techniques. Content analysis was the most used qualitative data analysis methods.
Duration of evaluation
With respect to how long the PT were evaluated, the duration of evaluation varied substantially, ranging from 15 minutes to 3 years. However, some studies did not report how long their PT evaluation lasted. Only a few studies conducted a longitudinal evaluation of their PT12,72,84 and the majority of the studies did not conduct a follow up study beyond the initial (feasibility) study. Therefore, it is difficult to establish long-term effects of PT for health and wellness from existing studies.
Study participants and sample size
Similar to the study duration, the sample size (number of participants in the evaluation of the PT) also varies greatly. The sample size ranges from 1 to 16,340 participants, with a mean sample size of 258 participants. However, one study did not report the total number of participants in their evaluation 61 and some studies are conducted in stages with the sample size and composition varying at each stage. In such cases, we report a combined sample size from all stages. Most of the study participants are recruited using a convenience sampling method and were recruited from academic communities or via online forums.
As can be seen from Figure 7, 66% of all the studies are targeted at adults, 16% involved children and teens, only 13% are targeted specifically at elderly people, and 5% of all the studies did not specify the target audience.
Targeted age demographic.
Discussion
Effectiveness of persuasive technology for health and wellness
Following from the reviewed literature, it can be concluded that persuasive technologies are effective at promoting various health and wellness related behavior with 92% of all the reviewed studies reporting some positive outcome (fully and partially positive) from PT use.
Although the majority of the studies (72%) are targeted at behavior and/or attitude change in line with the original conceptualization of PT by Fogg 91 (technology intended to change attitude and/or behavior), generally, the studies targeted and measured various other behavior-related or psychological outcomes beyond the conventional outcome of behavior and attitude. Similarly, some of the technologies are aimed at reinforcing and strengthening existing behavior (e.g., increase daily step count while others aimed at changing behavior (quitting smoking). This shows that persuasive technology has evolved over the years to encompass various practices that were not in the initial conceptualization.
The relationship between target health behavior domain (persuasion context) and persuasive technology outcome
There seem to be some variations in the effectiveness of the PT across various health and wellness domain. PT targeted at smoking and substance abuse related behaviors appear to be the least successful with respect to their overall effectiveness at promoting the desirable change in the domain. This is followed by PT targeting disease management. On the other hand, PT targeted at dental health; sexual behaviors; eating related behaviors; and physical activity (listed in decreasing order) seem to be the most successful with respect to the effectiveness of PT at promoting the desirable change in the domains. It is important to note that the effectiveness of the PT in various domains could be influenced by many factor including the operationalization of the persuasion strategies and behavior theories, the length and depth of evaluation, and the appropriateness of the PT for the target audience. Therefore, due to this methodological plurality and the heterogeneity of sample sizes and data, we are not able to draw strong conclusions about which persuasion contexts provided the most positive effects.
The relationship between behavior theory and persuasive technology outcome
Although, it is difficult to fully establish that using behavior theory to inform the design of PT influences their effectiveness due to the limited number of study in this review (85), the review results suggest that there may be some relationships. All the studies that are based on known theories but one 15 reported either fully positive or partially positive results. The study, 15 which failed employed an instantiation of negative reinforcement hence confirming that the use of any form of punishment as motivational strategy may backfire. Theories such as TTM and goal setting theory are more prevalent in the literature than others. However, the popularity of the theories vary across the domains. Theories such as TTM is common in the smoking and substance abuse, physical activity, and eating related domains.
The relationship between motivational strategies and persuasive technology outcome
Although several research efforts have been directed toward developing taxonomies for naming and classifying persuasive and motivational strategies,91,92 there still exist many inconsistencies in both naming and operationalizing strategies in persuasive systems. In some cases, the only way that one could possibly identify the actual motivational strategies employed in the PT is by studying how they work. Again, while some strategies such as monitoring/tracking, feedback, and social support seem to be more frequently used than others, it does not seem that there is a relationship between the strategy employed and the success of the PT. This is probably because of the variations in the instantiation and framing of the strategies. For instance, feedback is often instantiated in different forms, including audio, visual, or text based feedback, in various degrees of granularity, and in one of two valences – positive or negative. This variation in instantiations is likely to impact effectiveness. The choice of how to instantiate and operationalize the strategies are solely based on PT designer’s own discretion. Again, some strategies are more dominant in some health domains than the other. For example, monitoring and tracking strategy is a predominant strategy in physical activity and eating behavior motivating PT than other health wellness domains. Similarly, simulation and rehearse is a popular strategy in the sexual behavior domain.
General limitations and recommendations for future research
Based on the results of this review, we identified specific gaps in the literature and we offer suggestions for improvement and moving the field forward:
The PT literature lacks standardized approaches or tools for evaluating the effectiveness of PT and most existing evaluation approaches are based on subjective data which can be biased. Research into alternative assessment and evaluation techniques would enrich the PT community. In particular, the persuasive community would benefit greatly from research into objective evaluation approaches.
PT studies are limited in terms of effective integration of behavior theories and practice in their design. This is probably because most PT designers often lack the skills needed to translate theoretical determinants of behavior into technology design artefacts. We recommend that future research be focused on developing a comprehensive framework for translating theoretical determinants into technology design components.
Most PT employed more than one strategy in their design (see the appendix), therefore making it difficult to establish whether there is a relationship between the strategies and success of the PT. Research aimed at establishing the interactions between individual strategies and the success of PT either using sophisticated statistical techniques or by examining the effectiveness of the strategies in isolation would be vital to the community and would contribute in advancing the field.
Only a few studies have conducted longitudinal evaluations of the effectiveness of their PT.12,72,84 We stress the need for research in this direction to establish the long-term effect of PT on health and wellness.
Only a few PT involved the target audience in their design.30,79 We recommend that PT designers adopt the participatory design approach to enable the involvement of the target group(s) in deciding on the theories, strategies, and particular instantiation that will be suitable for the target audience and behavior.
Finally, there is a need for more PT to target diverse demographies such as older adults and children.
Conclusion
This paper provides a review of the effectiveness and trends of Persuasive Technology (PT) for health and wellness. The review results show that PT is a promising approach for promoting desirable behavior on a broad and heterogeneous range of health and wellness. However, lack of large-scale and longitudinal evaluations makes it impossible to establish the long-term impact of PT at promoting desirable behavior in the area of health and wellness. The review also highlighted PT trends and limitations of existing studies and suggested some improvements and future research direction.
Footnotes
Appendix
A comprehensive overview of persuasive technology for health and wellness.
| Authors | System/Project Name | Health Domain | Technology | Motivational Strategy | Behavior Theory | Country | Reference |
|---|---|---|---|---|---|---|---|
| Kim et al. (2008) | BuddyClock | Sleeping | Mobile | Feedback, status sharing | None | USA | [71] |
| Graham et al. (2006) | QuitCoach | Smoking | Web | Social support, Feedback and Advice | Transtheoretical model | Australia | [11] |
| Zwinderman et al. (2012) | Phone Row | Physical activity | Mobile game | Competition and leaderboard, feedback, and social comparison via Facebook | None | Netherlands | [88] |
| Young (2010) | Twitter Me | Physical activity | Combination of web, phone, and pedometer | Tracking and monitoring, sharing, Competition, praise, goal setting, reward, social comparison, persuasive text messaging | None | Netherlands | [22] |
| VanDeMark et al. (2010) | E-TREAT | Substance abuse | Computer-based application | Tailored persuasive messages, Individualized feedback, personalized coaching and support, suggestion | Transtheoretical model | USA | [72] |
| Van Leer and Connor (2012) | Mobile video | Voice therapy | Mobile | Video-based persuasion | Goal setting theory, social cognitive theory | USA | [23] |
| Toscos et al. (2008) | Mobile app. | Physical activity | Mobile | Social support, Persuasive text message, tracking and monitoring, sharing achievements | None | USA | [73] |
| Salam et al. (2010) | PMLE | Dental anxiety | CD ROM | Virtual Rehearsal, similarity, praise, and social learning | None | Malaysia | [24] |
| Sakai et al. (2011) | APStair | Physical activity | Publicly displayed screen | Authority, commitment, and consensus | None | Netherlands | [74] |
| Nakajima and Lehdonvirta (2013) | Persuasive Art | Physical activity | Ambient mirror | Tracking and monitoring, Reward, persuasive visual art, feedback, empathetic expressions | Goal setting theory, reinforcement theory | Japan | [15] |
| Nakajima and Lehdonvirta (2013) | Virtual Aquarium | Dental hygiene - Tooth brushing | Ambient mirror | Goal and objective, tracking and monitoring, visual feedback, positive reinforcement | Reinforcement theory, information theory | Japan | [15] |
| Mutsuddi and Connelly (2012) | Text messaging app | Physical activity | Desktop text messaging app | Goal and objective, reward, sharing testimonies | Transtheoretical model | USA | [25] |
| Munson and Consolvo (2012) | GoalPost and GoalLine | Physical activity | Mobile | Goal and objective, self-monitoring, sharing, reminder | Goal setting theory | USA | [75] |
| Mintz et al. (2012) | HANDS iProject | Autism | Mobile | Source credibility - expertise and trustworthiness, reward | None | Denmark, Sweden, Hungary, and UK | [76] |
| Looije et al. (2006) | iCat-personal assistant robot | Diabetes | Robot | Emoticons and visual expressions | Unified theory of acceptance and use of technology | Netherlands | [26] |
| Lim et al. (2011) | Pediluma | Physical activity | Physical activity tracker | Tracking and monitoring, visual feedback, reward, sharing | Transtheoretical model | USA | [27] |
| Lee et al. (2011) | Snackbot | Eating | Robot | default | None | USA | [28] |
| Lee et al. (2011) | Snack ordering site | Eating | Web | Default and Information | None | USA | [28] |
| Lacroix et al. (2009) | Activity monitor | Physical activity | Wearable device | Tracking and monitoring, visual feedback. | Self-determination | Netherlands | [29] |
| Kroes and Shahid (2013) | Powerfood | Eating | Mobile | Social Influence, feedback, comparison, reminder, points | Transtheoretical model, technology acceptance model | Netherlands | [30] |
| Kehr et al. (2012) | Chocolate Machine | Eating | Chocolate machine | Not specified | Ego depletion theory | Germany | [31] |
| Kaplan et al. (2003) | TLC-Computer-based telecommunication system | Chronic disease management | Computer-based application | Goal and objective, reminder | Goal setting theory | USA | [77] |
| Jeen et al. (2007) | Self-Diet System | Eating | Web | Source credibility, praise, negative reinforcement, social facilitation | Social learning theory | Korea | [78] |
| Foster et al. (2010) | Step Matron | Physical activity | Facebook app and pedometer | Competition, comparison | None | UK | [41] |
| Gasca et al. (2008) | pHealthNet | Eating and physical activity | Pedometer, mobile and web | Social support, collaboration, commitment | None | Mexico | [32] |
| Fabri et al. (2013) | Cooking Website | Eating | Web | Tracking and monitoring, Persuasive images | Transtheoretical model | UK | [33] |
| Consolvo et al. (2008) | UbiFit Garden | Physical activity | Mobile and activity sensor | Tracking and monitoring, visual feedback, reward, goal and objective progress display, positive reinforcement | Transtheoretical model | USA | [6] |
| Grimes et al. (2010) | OrderUp | Eating | Mobile game | Reward | Transtheoretical model | USA | [8] |
| De Oliveira et al. (2010) | MoviPill | Adherent to prescriptions | Mobile game | Tracking and monitoring, reward and point, reminder, competition | None | Spain | [34] |
| Chiu et al. (2009) | Playful bottle | Water intake (eating) | Mobile enabled Tracking and game | Tracking and monitoring, reminder, social support | Social conformity theory | Taiwan | [35] |
| Chang et al. (2008) | Playful toothbrush | Dental Hygiene - Tooth brushing | Game | Tracking and monitoring, visual and audio feedback, suggestion, praise | Teaching-learning theory | Taiwan | [14] |
| Bhatnagar et al. (2012) | Biometric system | Chronic disease management - tuberculosis | Biometric tracker | Tracking and monitoring | None | India | [36] |
| Berque et al. (2011) | Typing tracker | Healthy typing - repetitive strain injury | Computer-based application | Tracking and monitoring, reminder, visual and auditory feedback | None | USA | [37] |
| Berkovsky et al. (2012) | PLAY MATE! | Physical activity | Game | Tracking and monitoring, reward | Reinforcement theory, premack’s principle | Australia | [38] |
| Arteaga et al. (2010) | Mobile app | Physical activity | Mobile game | Competition and Reward | Theory of planned behavior, theory of meaning of behavior, personality theory | USA | [39] |
| Pollak et al. (2010) | Time to Eat! | Eating | Mobile game | Reminder, Control, positive and negative feedback | None | USA | [7] |
| Soler et al. (2009) | Molarcropolis | Dental hygiene - tooth brushing | Mobile game | Visual feedback | None | Greece | [16] |
| Khaled et al. (2009) | Smoke? | Smoking | Computer game | Tracking and monitoring | None | New Zealand | [10] |
| Eyck et al. (2006) | Cycling system | Physical activity | Virtual coach | Tailoring and personalization, tunneling, praise | None | Netherlands | [40] |
| Albaina et al. (2009) | Flowie | Physical activity | Touch-screen, photo frame and pedometer | Tracking and monitoring, commitment and consistency, goal and objective | Goal setting, classic learning theory | Netherlands | [79] |
| Rosser et al. (2010) | MINTS-II | HIV/STI | Web | Customization, tunneling, simulation | Sexual health model | USA | [12] |
| Adams et al. (2015) | Mindless plate | Eating | Sensing plate | Tracking and monitoring, Competition and leaderboard, comparison, | None | USA | [89] |
| Kientz et al. (2010) | MyPyramid Blast Off | Eating and physical activity | Computer game | Praise, visual feedback | None | USA | [83] |
| Bickmore et al. (2007) | Wrist-rest agent | Wrist rest | PDA-based social agent | Audio alert | None | USA | [42] |
| Obermair et al. (2008) | perFrame | Healthy posture | Interactive picture frame | Feedback | None | Austria | [43] |
| Parmar and Keyson (2008) | PHI | Maternal health and menses | Computer-based application | Social cues | Theory of planned behavior | India | [44] |
| Gasser et al. (2006) | Mobile app | Eating and physical activity | Mobile and web | Social facilitation | None | Switzerland | [45] |
| Fritz et al. (2014) | Activity sensor | Physical activity | Activity sensing devices | Tracking and monitoring, reward, goal, conditioning, social-sharing | None | USA | [46] |
| Sohn and Lee (2007) | UP Desk | Physical activity, smoking | PD text messaging | Tracking and monitoring, competition and leaderboard, cooperation, goal and objective, reward | None | Korea | [47] |
| Looije et al. (2010) | Robotic assistant | Diabetes self-management | Computer-based application | Not specified | Unified theory of acceptance and use of technology, five factor model | Netherlands | [80] |
| Toscos et al. (2006) | Chick Clique | Physical activity | Mobile and pedometer | Tracking and monitoring, sharing, comparison, positive feedback | None | USA | [48] |
| Goessens et al. (2006) | SPAIN pilot-study | Patient’s self-management | Computer-based application | Feedback, social support | None | Netherlands | [84] |
| McCreadie et al. (2006) | Personal Navigation tool | Physical activity | Mobile app | Tracking and monitoring, feedback | None | UK | [85] |
| Sterns and Mayhorn (2006) | PDA Pillbox | Medication adherence | PDA pillbox | Tracking and monitoring, reminder | None | USA | [49] |
| Knipscheer et al. (2006) | Persuasive story table | Loneliness and depression | Digital story telling table | Cooperation and collaboration | None | Netherlands | [81] |
| McCalley and Mertens (2007) | Pet plant | General health | Digital pet plant | Not specified | None | Netherlands | [82] |
| Chi et al. (2007) | Digital kitchen | Eating | Calorie aware kitchen | Tracking and monitoring, feedback | None | Taiwan | [50] |
| Golsteijn et al. (2008) | BLB | General well-being. | Persuasive bulbs | Not specified | None | Netherlands | [51] |
| Fujinami and Riekki (2008) | Ambient Mirror | Physical activity | Ambient mirror display | Competition, cooperation and collaboration | None | Japan | [52] |
| Harjumaa et al. (2009) | FT60 | Physical activity | Heart rate monitor | Tracking and monitoring, personalization, reduction, praise, reward, reminder, credibility, goal and objective | None | Finland | [86] |
| Munson et al. (2010) | 3GT | General well-being. | Social network | Reminder, sharing | None | USA | [53] |
| Roberto et al. (2007) | Computer-based application | Pregnancy, STD, and HIV prevention | Computer-based application | Not specified | Parallel process model | USA | [13] |
| Spruijt-Metz et al. (2008) | Get Moving! | Physical activity | Computer-based application | Not specified | Self-determination theory, theory of meanings of behavior | USA | [54] |
| Tsai et al. (2007) | PmEB mobile | Eating | Mobile app | Tracking and monitoring, reminder | None | USA | [55] |
| Fujiki et al. (2008) | NEAT-o-Games | Physical activity | Mobile game | Tracking and monitoring, competition | None | USA | [56] |
| Kaipainen et al. (2010) | GoodLife | Stress management | Web | Goal and objective, Tunneling | Goal setting theory, Transtheoretical model, cognitive behavior theory, acceptance and commitment therapy | Finland | [57] |
| Chatterjee et al. (2012) | In-home monitor | Diabetes self-management | Environmental and body-wearable sensors | Tracking and monitoring, reminder | None | USA | [58] |
| Chittaro and Sioni (2012) | LocoSnake game | Physical activity | Mobile game | Reward | None | Italy | [59] |
| Langrial and Oinas-Kukkonen (2012) | Web app | Eating | Web | Reminder, tracking | None | Finland | [60] |
| Peeters et al. (2013) | Social Stairs | Physical activity | Intelligent musical staircase | Reward | None | Netherlands | [61] |
| Burigat and Chittaro (2014) | Mobile app | Earphone use | Mobile app | Reminder, feedback, positive/negative reinforcement, progress | None | Italy | [87] |
| Chen et al. (2014) | SP-Stretch, Social Persuasion System | Physical activity | Mobile sensing and game | Tracking and monitoring, competition | None | Taiwan | [62] |
| Clinkenbeard et al. (2014) | Social network app | Physical activity | Social network | Tunneling, reduction, Suggestion | None | USA | [5] |
| Langrial et al. (2014) | Good Life Compass | Depression | Web | Reminder, rehearsal | None | Finland | [63] |
| Kopf et al. (2015) | Pakinson’s Disease related videos | Parkinson’s disease | Video | Not specified | Transtheoretical model | USA | [64] |
| Takeuchi et al. (2015) | Meal-sharing social media application | Eating | Social network | Feedbacks, sharing | None | Japan | [65] |
| Cornejo et al. (2015) | GuessMyCaption | Active ageing | Ambient casual game | Visual and audio feedbacks, sharing | None | Mexico | [66] |
| Orji et al. (2013) | LunchTime | Eating | Web | Goal and objective, reward, social influence, feedback | Transtheoretical model, knowledge- attitude-behavior theory | Canada | [9] |
| Lin et al. (2006) | Fish’n’Steps | Physical activity | Animated virtual fish | Goal and objective, tracking and monitoring, visual feedback, progress, sharing, competition, cooperation | Transtheoretical model | USA | [4] |
| Orji (2014) | JunkFood Alien | Eating | Phone-based game | Competition and Reward | None | Canada | [17] |
| Lo et al. (2007) | Playful Tray | Eating | Digital playful tray and games | Tracking and monitoring, visual feedback | None | Taiwan | [67] |
| Gerber et al. (2009) | Text messaging app | Eating and physical activity | Mobile | Personalization and tailoring | None | USA | [68] |
| Peng (2009) | RightWay Café | Eating | Computer game | Feedback, points, rehearsal | Theory of reasoned action, social cognitive theory, health belief model | USA | [69] |
| Kaptein et al. (2012) | Text messaging app | Eating - snacking | Mobile | Tracking and monitoring, liking, consensus, consistency, authority | None | Netherlands | [70] |
| Khalil and Abdallah (2013) | SET UP | Physical activity | Mobile | Tracking and monitoring, sharing | Theory of reasoned action | United Arab Emirate | [21] |
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.