
Abstract
The usage of mobile health (mHealth) applications is rapidly increasing. This research has been aimed mostly at reviewing existing mHealth apps and their functionality. However, studies from users’ perspectives are rather scarce. This exploratory study addresses that gap and, using cross-sectional survey data, seeks to reveal the socio-demographic and individual characteristics of users who utilize specific functions of mHealth apps. The data were collected via an online survey through websites oriented toward eating habits, exercising, dieting, and weight loss. From the original sample (1002 users; M = 24.8, standard deviation = 6.9; 81.6% females), the final sub-sample of 406 participants aged from 13 to 39 years (M = 23.8, standard deviation = 5.3, 86.9% females) who reported usage of mHealth apps was examined. The analyses revealed demographic and individual differences in predicting usage of various functions of mHealth apps. The drive for thinness was associated with functions for weight monitoring and planning functions. Excessive exercise was associated with weight monitoring, socializing functions, and functions for planning and monitoring goals. These findings imply that mHealth apps should be individually tailored to incorporate components such as risk-specific warnings or the provision of information related to seeking professional help for at-risk audiences.
Keywords
Introduction
Presently, the use of mobile health (mHealth) applications on smartphones, tablets, and wearable devices is rapidly increasing. 1 There are thousands of apps which can be used for various purposes: disease prevention and healthy lifestyles, finding a healthcare professional, health diagnoses, filling prescriptions, health compliance, and the education and management of chronic ailments such as diabetes. 1 Concerning the current usage of mHealth apps, a study of the Health Information National Trends Survey revealed that 35.9 percent of US adults were using an mHealth application. 2 However, research up to this point has been focused mostly on reviews of existing mHealth apps and their functionality, feasibility, clinical utility, disease prevention, and monitoring of diseases.3–5 There is a very limited number of studies on the users of mHealth apps, with most focusing on the prevalence of mHealth apps’ use and the demographic characteristics of the app users.2,6,7 To our knowledge, there is no study that focuses on the details of the functions of mHealth applications from the user’s perspective that takes into account the individual characteristics of users. This information is important for the future development of mHealth apps, especially as it relates to the individual tailoring of the apps based on user profiles.
In this article, we use the term “functions” of apps to describe various app features which enable their users to select among a range of capabilities such as monitoring, setting goals, planning, providing feedback on performance, and communicating with other users. It should be noted that different authors use different terms when speaking about this range of capabilities, such as app functionalities, app characteristics, and app features.2,6–8 We opted for the use of the term “functions” as an overarching term throughout this article.
To date, functions of mHealth apps have been researched primarily by analyzing existing health-related software applications. In one study, 167 top-ranked apps for physical activity were evaluated with respect to which behavior-change techniques were being used by these applications. The study revealed the following functions of apps: instruction on how to perform exercises, modeling how to perform exercises, providing feedback on performance, goal-setting, planning, and social support. 9 Another study was focused on apps for weight management and it reviewed 393 apps. 5 The study found that self-monitoring was the most common function of the apps (35.3% of apps had this function). The second most common function was physical activity support (27.5%), followed by weight assessment (25.4%), healthy eating support (23.2%), and goal-setting (21.4%). Less prevalent functions of the apps were motivational strategies (7.1%), social support (5.3%), and personalized feedback (1.8%). According to Bhargava and Tanghetti, 10 the main functions of mHealth apps are to inform, advise, communicate, measure, monitor, and motivate users. The outcomes of these three studies (all relevant to our research) were subsequently used to frame the group of mHealth app functions utilized in our study.5,9,10
Currently, there are few studies focused specifically on the users of mHealth applications. In nationally representative studies of US adults, estimates of how many users report using mHealth apps range from 22.7 percent to 35.9 percent.2,7 In another study involving a sample recruited from an online panel and through online advertisements, it was reported that 58.2 percent of mobile phone users in their sample had downloaded a health-related mobile app. 6 Concerning the characteristics of mHealth app users, the studies suggest that they tend to be younger, white, have an educational level greater than high school, have a higher income, are employed, have insurance coverage, live in urban areas, are not current smokers, are more often obese, and report excellent health.2,6,7 A recent study revealed that mHealth app users are more likely to report intentions to improve fruit and vegetable consumption, physical activity, weight loss, and to meet recommendations for physical activity. 7 In contrast, a study in Germany involving a population-based sample of adults 35 years and older failed to find any significant differences between mHealth apps’ users and non-users based on gender, employment, education, smoking habits, diet, and health-related quality of life. 8
Regarding the functions of mHealth apps, the following three themes emerged from a study which asked participants an open-ended question about which app features they would potentially use: food intake, physical activity, and/or weight management features. 6 The participants mentioned that they wanted apps to provide specific and personalized recommendations regarding exercise and diet. A study of US adults asked whether mHealth apps’ users use functions which help achieve a health-related goal, such as quitting smoking, losing weight, or increasing physical activity. 2 From those app users, 60.4 percent used apps to achieve health-related goals. Users of these functions were more often younger as well as obese. This study also asked about functions for helping with medical care decision-making, which were utilized by 34.6 percent of the users of mHealth apps. These functions were more often used by 35- to 45-year-olds, who engaged them more than younger users, as well as smokers, who used it more than non-smokers. More than a third of mHealth app users (37.7%) also used functions to ask a physician questions or to seek a second opinion. 2 Users from the German study reported planning (51%) as the most commonly used function, followed by reminding (36%), prompting motivation (34%), providing information (34%), and feedback or monitoring (18.0). 8 App users using more functions for planning and feedback or monitoring were more likely to engage in physical activity.
Aims of the study
This study was carried out in the Czech Republic where the penetration of smartphones is high (64% of mobile phone users). 11 Among individuals older than 15 years, Internet usage is 79 percent. 12 Of Internet users, 41 percent use mobile phones to access the Internet and 78 percent say they sometimes search for health information online. Given that fitness and nutrition are typically the most common categories for mHealth app usage 6 and that research from the European Commission suggests that nearly three-quarters of Europeans look for health information online (specifically for lifestyle choices, such as diet, nutrition, or physical activity), 13 in this study we focus on the functions of mHealth apps which are related mainly to eating behavior and exercise. Specifically, we aim to reveal the socio-demographic and individual characteristics of users who use these specific functions of mHealth apps. We include user characteristics such as excessive exercise, drive for thinness, and weight status, due to their potential to facilitate a negative impact on app users, which is—to our knowledge—the first study of its kind. Increasingly, there have been calls to investigate the functions of mHealth apps in greater detail 8 as a result of the growing focus integrating technology into healthcare and the need for more evidence supporting the role of health-related apps for health and wellness promotion. 7 Evidence from this study may aid in the development of mHealth apps which are individually tailored to app user profiles. For example, it is known that high scores in drive for thinness and excessive exercise may be related to problems with eating disorders.14,15 It is important to understand which functions of mHealth apps are associated with possibly risky dispositional factors or problematic health behaviors so that risk management features might be implemented (e.g. the provision of warning messages in line with public health standards).
Methods
The present exploratory study utilizes data from visitors of websites focused on nutrition, weight loss, and exercise which were collected as part of a project on eating behaviors in the context of Internet and technology use, having been approved by the university Research Ethics Committee. The study has a cross-sectional design: the data were collected via an online survey between May and October 2016. For participant recruitment, Czech websites oriented toward eating habits, exercising, dieting, and weight loss were asked to publish an invitation for participation and 49 of them subsequently did so. On average, the completion of the survey took approximately 15 min. Participants were motivated by the chance to win one of five vouchers for an e-shop in the amount of 40 Euros each.
The online survey was initiated by 1143 visitors who provided at least some data on the first page of the questionnaire. However, we excluded data from 141 visitors in the process of data cleaning, yielding the base sample of 1002 users aged 13–62 years (M = 24.8 years, standard deviation (SD) = 6.9 years; 81.6% females). From this sample, we excluded 274 participants who did not fill out the whole questionnaire and 26 participants who were 40 years and older because this group was under-represented in our sample and did not allow for sufficient analyses. From the remaining sample of 702 participants, 406 participants (57.8%) reported the usage of mHealth apps, which comprised our final sample.
Among the participants aged 13–39 years (M = 23.8 years, SD = 5.3 years), 86.9 percent were female (N = 353). In our sample, 0.2 percent of participants had completed primary education, 40.5 percent secondary education, and 59.2 percent tertiary education. The participants primarily used smartphones daily (89.7%), with 8.1 percent reporting almost daily usage, and 2.2 percent reporting weekly usage or less. There were no significant differences between the users of mHealth apps and non-users according to age, income, or education. The app users were more often women, who reported using smartphones more often and rating their smartphone skills as better, while simultaneously reporting slightly lower body mass index (BMI). These differences were reported in a separate article. 16
Measures
Predictors
We collected basic socio-demographic information about gender and age. Smartphone usage was measured by the question “How often do you use a smartphone?” (1 = Never, 2 = Several times a month, 3 = Several times a week, 4 = Almost daily, 5 = Daily; M = 4.89, SD = 0.35). The Advanced usage of smartphone was measured by a newly developed item, “How advanced a user are you of smartphones?” on a scale from 1 (Beginner) to 8 (Expert), M = 6.21, SD = 1.17.
Education
We inquired into the level of the respondents’ own education and about the highest educational achievement of their parents (the highest degree of education achieved in the family, be it the father or the mother). For those aged 26 years and younger, the parents’ education level was used as an indicator of education, except for the cases in which respondents aged 18–26 years had attained a higher level of education than their parents.
Drive for thinness
Seven items from the subscale Drive for thinness from the Eating Disorder Inventory-3 (EDI-3) 15 answered on a 6-point scale ranging from 1 = Never to 6 = Always were used. The scale was computed by averaging the items; M = 3.34, SD = 1.15, α = 0.84.
Excessive exercise
Five items from the subscale Excessive exercise from the Eating Pathology Symptoms Inventory Scales (EPSI) 17 answered on a 5-point scale ranging from 1 = Never to 5 = Very often were used. The scale was computed by averaging the items; M = 3.21, SD = 0.88, α = 0.84.
Weight status (BMI)
The respondents reported their current height (in cm, M = 168.71, SD = 7.39) and weight (in kg, M = 68.11, SD = 22.11). BMI was computed as follows: weight/(height/100);2 M = 22.79, SD = 3.99.
Criteria
First, we aimed to create groups of functions of mHealth apps which are typically combined. Functions were grouped according to theoretical perspectives which are based on research analyzing mHealth apps.5,9,10 Consequently, scales for the following groups of functions were created. The responses for each of the functions were as follows: Never (=1), Several times a month (=2), Several times a week (=3), Almost daily (=4), and Daily (=5).
Functions for monitoring weight
This scale was created as an average score of four items—monitoring weight, monitoring BMI, monitoring calorie usage, and monitoring calorie intake. M = 1.91, SD = 0.94, α = 0.77
Functions for monitoring health features
This scale was created as an average score of four items—counting steps, sleep monitoring, monitoring heart rate, and monitoring health status. M = 1.59, SD = 0.85, α = 0.71
Functions for planning and monitoring of goals
This scale was created as an average score of three items—planning and monitoring the goal of the targets in weight loss, planning and monitoring the goal of the targets in gaining weight, and planning and monitoring the goal of the targets in sport or exercise. M = 1.70, SD = 0.83, α = 0.65
Socializing functions
This scale was created as an average score of two items: communicating with people who are using this application and comparing my results (in sport, nutrition, etc.) with people using the given application. M = 1.54, SD = 0.93, α = 0.72
IBM SPSS Statistics version 22 was used for the data analyses. Descriptive statistics were calculated to show distributions of mHealth apps’ usage. Four hierarchical linear regressions were conducted to examine the effects of demographic and individual characteristics for usage in four distinct groups of mHealth apps’ functions. Figure 1 shows the analytic model for the linear regressions. In the separate regression models, socio-demographic variables were entered into the first block, and individual characteristics of apps users were entered into the second block.
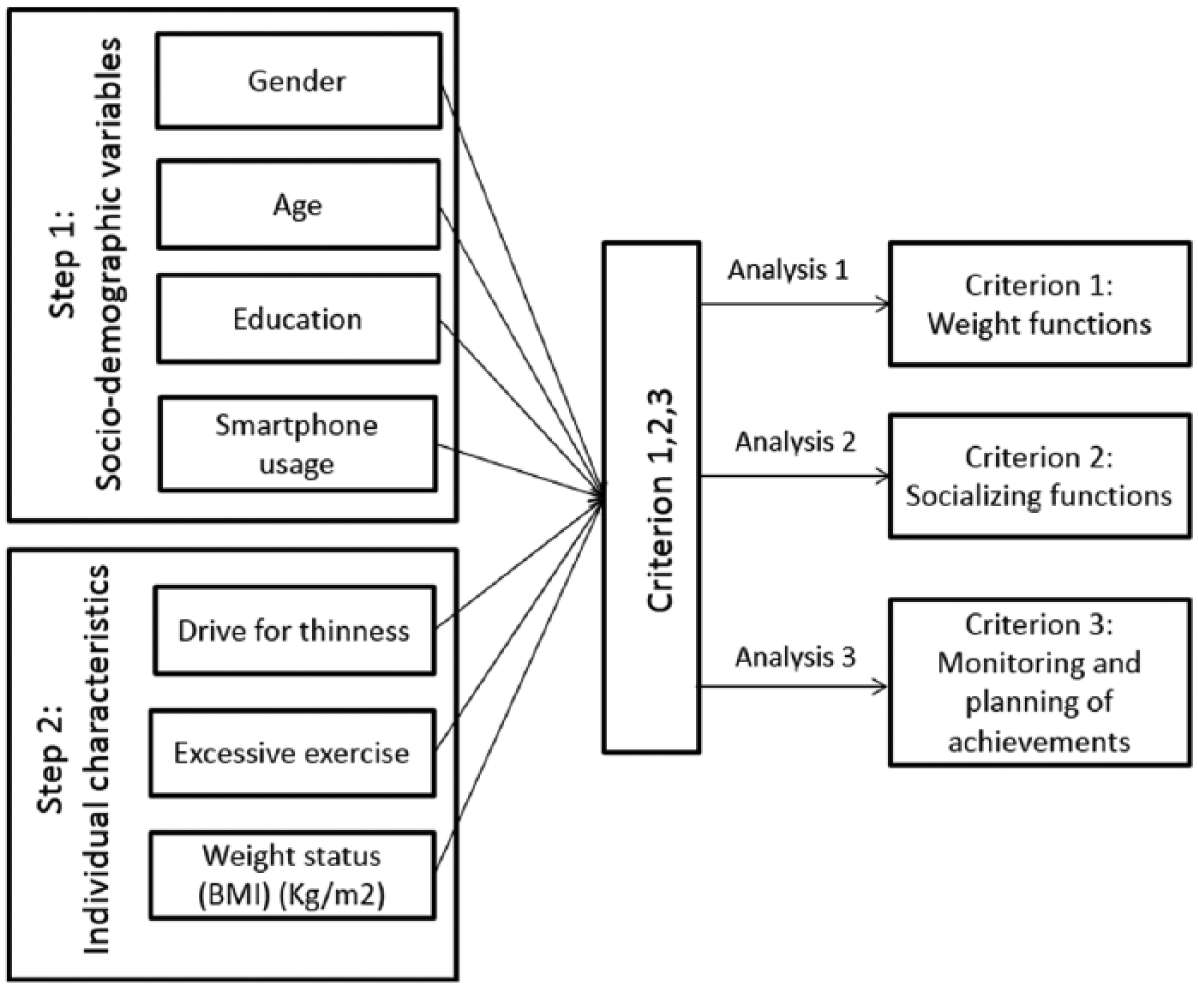
Analytic model for two-step linear regression.
Results
Descriptive analyses of mHealth apps’ functions
Table 1 displays the frequency of usage of all app functions. In the first group Functions for weight monitoring, the most often used functions were monitoring calorie intake and calorie usage, with more than half of mHealth apps users using these functions at least monthly. Monitoring of calories are also the most often used functions among all functions of applications. Among Functions for monitoring health features, the most often used function was counting steps which is another very frequently used function overall. Among Functions for planning and monitoring of goals, the most often used function was planning and monitoring of targets in sport or exercise, with more than half of users utilizing this function at least monthly. The Socializing functions are used less often, with about a fifth of the users communicating at least monthly with other users through the mHealth apps and about a third of the users comparing their results with others in the applications.
Functions of mHealth apps: percent of users of the given apps’ function.
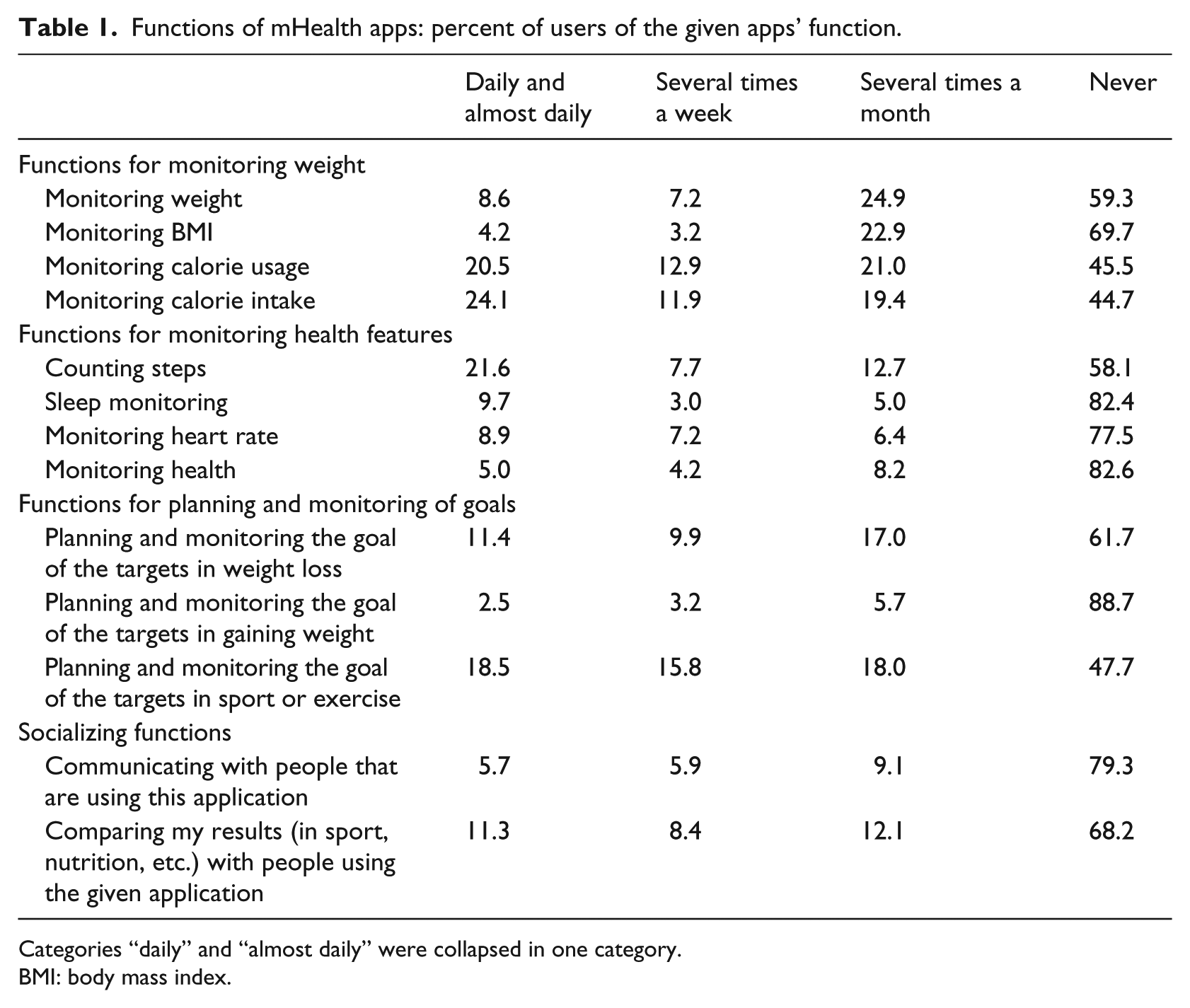
Categories “daily” and “almost daily” were collapsed in one category.
BMI: body mass index.
We also analyzed usage across the entire set of functions and show that 71.2 percent of mHealth app users utilize at least one of the Functions for weight monitoring, 55.4 percent at least one of the Functions for monitoring of health features, 37.2 percent at least one of the Socializing functions, and 60.6 percent deploy at least one of the Functions for monitoring and planning of goals.
Regression models: predicting mHealth app functions
The results of the hierarchical linear regression analyses are shown in Table 2, with the exception of the model for Functions for monitoring health features, which was not significant (p > 0.05). The model for Weight functions explained 14.5 percent of the variance (p < 0.001), the model for Socializing functions explained 7.5 percent of the variance (p < 0.001), and the model for Functions for planning and monitoring explained 11.3 percent of the variance (p < 0.001).
Hierarchical linear regression predicting functions of mHealth apps: weight monitoring functions, socializing functions, functions for planning and monitoring of goals.
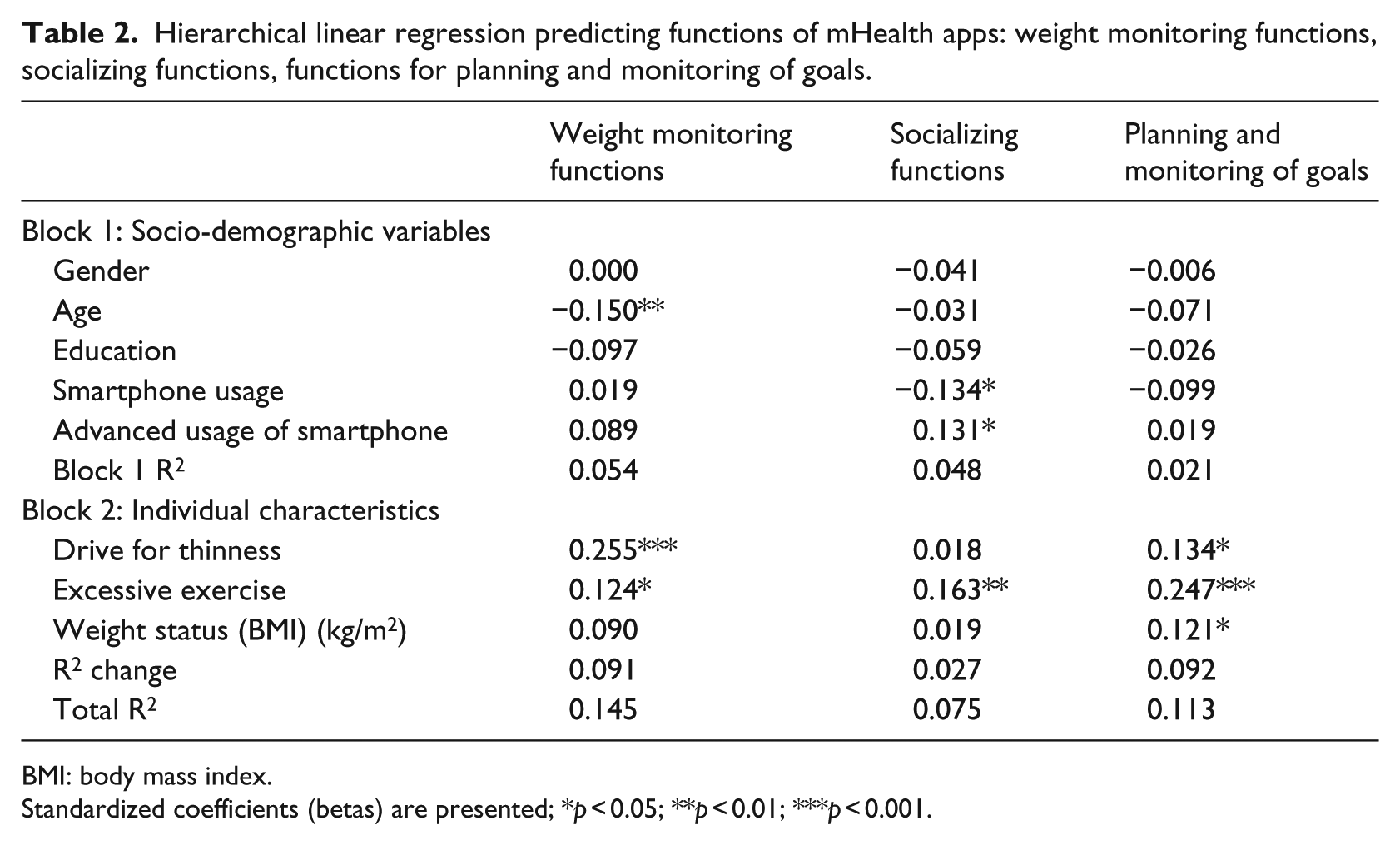
BMI: body mass index.
Standardized coefficients (betas) are presented; *p < 0.05; **p < 0.01; ***p < 0.001.
In the significant models, from the demographic factors, age was negatively associated with usage of Weight functions such that younger app users tended to use Weight functions more often. The amount of usage of smartphones was negatively, yet moderately, related to usage of Socializing functions (beta = −0.134). On the other hand, the usage of Socializing functions was moderately positively related to the advanced usage of smartphones (beta = 0.131).
Concerning individual characteristics, excessive exercise was positively related to all three groups of functions: Weight functions, Socializing functions, and Functions for planning and monitoring of goals. The largest effect was found for Functions for planning and monitoring of goals (beta = 0.247). Drive for thinness was associated with usage of Weight functions (beta = 0.255) and Functions for planning and monitoring of goals (beta = 0.134). The usage of Functions for planning and monitoring of goals was also associated with BMI, such that respondents with higher BMI were using these functions more often.
The model for Functions for monitoring health features was not statistically significant. Therefore, separate analyses for each function from this group were run. We created dichotomized variables for using versus not using each of the functions and used a t-test to analyze differences between users and non-users. We tested the same variables as in the regression models. For the functions Counting steps and Sleep monitoring, we found no significant differences (p > 0.05). For the function Monitoring the state of health, users with higher drive for thinness (p = 0.033) and with higher BMI (p < 0.001) reported using this function more often. For the function Monitoring heart rate, we found that users with higher excessive exercise patterns are using this function more often (p = 0.009).
Discussion and conclusion
Descriptive characteristics of usage of mHealth app functions
In this article, we analyzed in detail which functions of mHealth apps are used and what are the demographic and individual characteristics of its users. We found that among the most often used are weight-related functions, with the most frequent usage being monitoring calorie intake and calorie usage. This is in line with the study by Krebs and Duncan 6 where participants reported they would potentially use the food intake and weight management features of mHealth apps most often. In our study, 60.3 percent of users reported using Functions for planning and monitoring of goals, which is in line with the study by Bhuyan et al. 2 where 60.4 percent of app users reported using apps for achieving health-related goals. Also, German users reported planning as the most commonly used function of apps (51%) in another study. 8 Given the differences between these three samples (whereas our study targeted a sample of users of health-related websites), it is interesting that the number of people reporting using these functions is quite similar. It is therefore possible that the net share of users of these functions is stable across different populations of mHealth users.
From Functions on monitoring health features, users reported the usage of counting steps most frequently, which was among the most often used functions overall. The Socializing functions of apps were less often used, with users more often comparing results with others and fewer people reporting communicating with others within the application. It may be that Socializing functions are being utilized more through the Internet within online communities and not directly within the applications, which should perhaps be investigated further and specifically in future research.
Importantly, our study brings new findings to the field in that it describes a broader range of functions and usage patterns, including counting steps, sleep monitoring, monitoring BMI, monitoring calories, and setting different goals, in comparison to previous studies. This additional information can prove useful to software developers as well as researchers planning future studies involving mHealth apps.
Predicting usage of mHealth app functions by demographic characteristics
Concerning the predictors of different usage of functions, we found no gender and education differences, which is in line with the study by Bhuyan et al. 2 and also the study by Ernsting et al. 8 Younger age was associated only with higher usage of Weight functions, probably relating to the fact that dieting behavior is also more prevalent at a younger age. 18 In contrast, while the study by Bhuyan et al. found associations between age and functions for planning goals, we found no such association in our study, potentially due to the restricted age range in our study. Importantly, our study contributes to the field in finding that levels of smartphone usage and an advanced knowledge of smartphones were associated with Socializing functions of mHealth applications. Interestingly, the level of smartphone usage was negatively related to Socializing functions. It may be that more advanced users of mobile phones generally communicate more through mobile phones with usage of other communication platforms rather than through Socializing functions of mHealth apps. These results could be interpreted in relation to theories linked to digital literacy or the “uses and gratifications theory,” such as to clarify these associations between technology usage, digital literacy, and using of apps’ functions. 19
Predicting usage of mHealth app functions by individual characteristics
The present results describe new associations between the functions of apps and specific individual characteristics of users, the drive for thinness, excessive exercise, and weight status. Our study is the first exploratory study in this area. Future research should pursue approaches with a focus on theory testing, including setting a priori hypotheses about potential mediators of apps usage and health impact, and analytical approaches such as mediation analyses. For example, it could be useful to test the role of different app functions as mediators between individual characteristics (such as drive for thinness) and the impact of apps on users.
The drive for thinness was associated with Functions for weight monitoring and Functions for monitoring and planning and monitoring of goals, with the largest effect present within Weight monitoring functions. Such relations can indicate that some people can use mHealth apps potentially in a harmful way because the drive for thinness is associated with eating disorders.12,14 The possible pathological usage of mHealth applications can be indicated also by associations between excessive exercise (assessed as part of the Eating Pathology Symptoms Inventory) and functions for Weight monitoring, Socializing functions, and Functions for planning and monitoring of goals. Both observed associations may indicate that some app users are at risk for eating disorders. Such findings have several practical implications as we discuss below. It is also interesting that only excessive exercise and not the drive for thinness was linked to the Socializing functions. The possible pathological usage of Socializing functions should be investigated in detail in future research.
The Functions for planning and monitoring of goals were associated also with higher BMI, suggesting that more obese individuals tended to use these functions more frequently. This is in line with the study by Bhuyan et al. 2 who found that obese respondents were using more functions for achieving health behavior goals. Unfortunately, our study did not include enough underweight people, precluding comparative analyses for this group. This is a challenge for future research. But we can state based on these new results that people with higher BMI were not using more Weight monitoring functions and Socializing functions. Future research should investigate which app functions may be most impactful for overweight people.
Concerning the Functions for monitoring of health features, we found no differences between people who use or do not use the function for counting steps, one of the most widespread functions of mHealth apps. As this function was not associated with the scores for drive for thinness and excessive exercise, we can hypothesize that the counting steps’ function is not only popular and useful, but that it presents no potential harm or risk with respect to eating disorders, which is an important finding also from an app developers’ perspective.
Limitations and practical implications
This study used a specific sample of respondents visiting websites focused on nutrition, weight loss, and exercise, which led to (among other things) a very high proportion of women in our study. The sample in our study is specific and the generalization of our findings is limited. We also investigated a specific group of mHealth functions which were focused on weight monitoring and exercise; however, other and new functions in mHealth applications remain worthy of further study. We were also focused only on a particular set of individual factors which are related to usage of specific app functions. Future studies should ensure more a representative sampling of the populations of app users and app functions, as well as individual difference characteristics as a way to overcome these limitations.
There are also practical implications stemming from this study. We demonstrated that individual characteristics such as the drive for thinness or excessive exercise are related to the higher usage of some functions of mHealth apps, which may put users at risk for problematic eating behaviors. Designers of mHealth apps should attend to this in the process of app development and aim to create individually tailored apps with respect to these risks. Any new app features should be evidence-based and consistent with public health standards for dieting and exercise to ensure safety of users of mHealth apps.20,21 In the development of future apps, the implementation of such features could lead to more advanced education functions or risk stratification functions where warnings could be indicated for users “at risk” for maladaptive app usage based on profiles of their individual characteristics. Individual tailoring of mHealth apps could then incorporate components such as risk-specific warnings or the provision of risk-specific information as to seeking professional help. Our results also indicate that tailoring mHealth apps in relation to risks of problematic eating behavior is relevant only for some, not all, app functions, specifically for Functions for monitoring weight and also for Functions for planning and monitoring goals.
On a positive note, our findings show that individuals with higher BMI are also more frequent users of Functions for planning and monitoring of goals. This suggests that app designers should specifically target obese individuals with features focused on the planning of eating behavior. Further research on user characteristics and mHealth app usage is needed to facilitate the development of the more effective tailoring of mHealth apps and their specific functions.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: The authors acknowledge the support of the Czech Science Foundation (GA15-05696S) and the Masaryk University.