
Abstract
User characteristics should be considered when designing features for e-health or m-health applications, as the developed solution should aim to support this specific target group. This study explores the effect of user characteristics (personality, health state, stress/recovery state, leadership behavior) on the interest and likelihood of using an app for health promotion activities at the workplace. Leaders are a key factor for the success of workplace health promotion; therefore, the target group of this study are leaders. The data of 412 leaders were collected in an online study. Hierarchical multiple linear regression analyses were conducted for four outcome criteria (“personal health,” “contacting,” “leadership feedback” and “corporate key figures”). The findings showed that neuroticism, physical health and health-promoting leadership were important predictors for using an app for monitoring personal health and getting in social contact about health issues. The stress/recovery state was significantly related to the feature of getting in social contact.
Introduction
Identifying the target market of a web-platform or app in health promotion is a vital step in the creation and marketing of successful tools in e-health (electronic health) and m-health (mobile health). Health promotion “is the process of enabling people to increase control over, and to improve, their health” (Ottawa Charter, 1986 1 ). Using e-health and m-health tools to support health promotion has big potential, and currently a large number of these tools are available in different areas of health promotion (e.g. in the areas of sports, weight reduction and healthy nutrition 2 as well as in the areas of stress/burnout reduction 3 ). Gaining an understanding of the future users of e-health and m-health-tools will have a major impact on the tool’s development and advertising methods. In addition, individuals are easier to motivate to participate in web- and app-based programs if the developed app meets the requirement of the target audience and the advertising of the apps is in concordance to the users’ needs so the probability of the usage could be raised.
The majority of the studies in the field of web- and app-based health promotion focus on the technical features, layout and feedback characteristics of the program.4,5 With the exception of gender and age,6,7 users’ characteristics and how they affect the usage of e-health and m-health tools are investigated in only a few studies; and there are even less studies combining different user characteristics for a comprehensive target group analysis (see, for example, Reinwand et al. 8 ).
This study explores the effect of various characteristics of users on the interest and likelihood of using an app for health promotion. These user characteristics consist of fixed (personality; measured with the Big-Five) and modifiable (individual health state, stress and recovery state, leadership behavior) characteristics. We especially focus on health promotion activities that can be combined with workplace health promotion programs, as e-health programs at the workplace are usually not in the focus of e-health research.9,10 Therefore, this study focuses on the characteristics of leaders, as leaders are usually seen as a key factor when it comes to health promotion activities at the workplace. 11 Leaders who engage in health promotion activities themselves are able to positively influence participation levels of their employees and encourage healthy behavior.12,13 In this study, leaders are defined as persons who assume responsibility for one or more employees in a lower hierarchy. As we investigate leaders, we do not solely investigate the view of “traditional” health tools in workplace health promotion (e.g. to enhance physical activity), but in addition investigate the view of leadership-specific tools for workplace health promotion. These tools could aim to improve own leadership skills by getting repeated feedback on their leadership behavior from their subordinates 14 or aim to support leaders in monitoring their subordinates’ health and satisfaction.
Theoretical background
User characteristics and e-health interventions
Designing e-health or m-health applications with target consumers is crucial, especially if the developed solution aims to support a specific group. 15 Including the users in the design process is a common approach in human-centered design studies. 16
In their Internet intervention model, Ritterband et al. 17 identify different characteristics that lead to a high probability of using e-health or m-health interventions. For the likelihood of using these tools, several characteristics are defined, such as user characteristics, the individual’s environment, website characteristics and features of support. Especially the user characteristics are viewed as complicated, as they can be very diverse and most of them are fixed and cannot be manipulated (e.g. gender, age, personality). Others can be modified, such as intentions, interests or abilities. In the Internet intervention model, 17 user characteristics include disease, demographics, personality traits, cognitive factors, beliefs and attitudes, physiological factors and skills.
In this study, the target group are leaders, as leaders can positively influence the success of workplace health promotion programs with their actions. 11 Leaders are important key factors in workplace health promotion; therefore, the specific characteristics of leaders have to be analyzed. Leaders as a specific target group for e- and m-health tools are addressed in the practical field, where a large number of apps in the field of leadership assistance and development can be found in the app stores. Interestingly, the view of leaders for using apps in workplace health promotion has not been adequately studied in research (exceptions can be found by Ly et al. 18 and Dunkl and Jiménez 19 ).
Research about the leaders’ user characteristics for using e- and m-health tools are sparse, but this important target group has to be addressed in research about e- and m-health tools for workplace health promotion. For the development of our research question and hypotheses, research findings about general user characteristics for using e- and m-health tools were investigated.
In the next sections, research findings about the most common user characteristics in e-health and m-health research (personality, health) as well as less investigated user characteristics (stress, recovery, leadership) which could be important for health promotion at the workplace are presented. The next sections focus on research about online behavior and tool usage (e.g. smartphone usage) in the area of e-health and m-health tools. We are interested in investigating user characteristics of leaders for e-health and m-health tools. We focus on investigating predictors for using the channels Internet and smartphone (app) for health promotion. This includes both the frequency of using these channels and the behavior while using these channels.
Personality
In the Internet intervention model, 17 personality is an important factor for the probability of using e-health or m-health interventions. Research in this field especially focused on neuroticism and extraversion of the Big-Five framework 20 as important predictors of mobile phone and Internet usage.21 –23 In almost every study including the Big-Five, neurotic individuals are found to prefer and use the Internet and smartphone apps to a greater extent.21 –23 Extraverts are found to be more likely to own a smartphone,22,24 but introverts use the Internet more often and prefer online communication over traditional communication forms.21,25 It seems that the anonymity experienced on the web benefits neurotic and/or introverted individuals, as the social contact in “real life” is much more difficult for individuals with a neurotic and/or introverted personality. 21 As for neurotic individuals, higher levels of neuroticism are positively related to social media use, as neuroticism is related to loneliness and social media are an easy way to seek company and avoiding face-to-face contact at the same time. 26
Similar results can be found for e-health and m-health interventions. In the study of Halko and Kientz, 27 people with different personality patterns were asked about the perceptions and opinions of new technologies in health promotion. Their findings indicate that especially neurotic and introverted individuals rated e-health technologies as something that they would enjoy. Introverted individuals consider e-health technologies as more helpful to achieve their own health goals and are more likely to use them. The following hypotheses are stated:
H1. Neurotic leaders are more likely to use an app in workplace health promotion than non-neurotic leaders.
H2. Introverted leaders are more likely to use an app in workplace health promotion than extraverted leaders.
Physical and mental health
Previous studies in the field of (workplace) health promotion repeatedly showed that people with healthier lifestyles are more likely to participate in health promotion programs and are more likely to proceed and finish the program.28–30 In contrast to these findings, research in the field of e-health and m-health indicates that the participation in web- or app-based health promotion activities seems to be the opposite. In the study of Arning and Ziefle, 31 the majority of the participants stated that they would not use e-health programs until a poor health condition would require them to use such a program. In further studies, unhealthier people are more likely to start a web-based health program,32,33 and participants with low intention to be physically active rather chose to participate in a web-based intervention than in a traditional health intervention. 34 Similar results can be found for mental health: BinDhim et al. 35 found in their study that participants with a higher risk score in depression more often use an app that gives feedback about their mental state. A possible reason why web- and app-based health interventions seem to be more attractive for unhealthier individuals might lie in the perceived anonymity of the tools. 26 People with a lower health status might not feel comfortable to share their problems and behaviors in traditional social networks. 36 In line with this assumption, we state the following hypotheses:
H3. Leaders with a lower physical health status are more likely to use an app in workplace health promotion than leaders with a higher physical health status.
H4. Leaders with a lower mental health status are more likely to use an app in workplace health promotion than leaders with a higher mental health status.
Stress and recovery
The aspects of stress and recovery are especially important in the work-related context. Using an app-based health intervention at the workplace could be related to the users’ perceived stress and recovery at work—similar to the results found for the users’ own health status. In the study of Ferdous et al., 37 a high self-reported stress level is positively correlated to the usage of smartphone apps at work. However, in their study stressed individuals mainly use apps that can be used in the work context, such as calendar, note taking app, calculator, voice-to-text app and other utility apps. In another study specifically related to e-health interventions, the individuals’ baseline stress level could not predict the participation in an online stress management intervention. 38 The same result was found for students, where using mental health support via the Internet was not predicted by stress. 39 In the work context, the participation in a web-based stress management program at the workplace was not related to the employees’ stress level. 40 These studies indicate that the individual stress state seems to be a poor predictor for e-health and m-health interventions. Mental health is an important predictor for using mental health apps, though. Higher risk scores in depression are related to a more frequent use of apps specifically designed for depression, as depressed individuals can overcome their inhibitions easier when they can use an app anonymously. 35 The same might apply for highly stressed individuals in the working context. Seeking help in the working context is more likely if employees can remain anonymous. Therefore, we assume that highly stressed employees would benefit from an e-health or m-health intervention and state the following hypothesis:
H5. Leaders with a higher stress state are more likely to use an app in workplace health promotion than leaders with a lower stress state.
In contrary to stress and app usage, research of recovery in this field is relatively sparse. As mentioned before, participation in e-health and m-health interventions seems to be correlated with a lower health status. Therefore, it would be plausible that employees with a lower recovery state should be more interested participating in e-health and m-health interventions.
H6. Leaders with a lower recovery state are more likely to use an app in workplace health promotion than leaders with a higher recovery state.
Leadership
Leadership is one of the most important factors for successful workplace health promotion. Leaders are actively involved in decision-making processes and are responsible for the consequences of any change at the workplace. Furthermore, participation levels in of a workplace health promotion program can be positively influenced by the commitment of leaders. 13 Therefore, successful workplace health promotion programs require commitment of the management. 41 However, in the study of Dunkl and Jiménez, 42 leadership experience was not significantly related to a higher usage of e-tools in workplace health promotion. Next to leadership experience, another important aspect is the factor of health-promoting leadership. Health-promoting leadership basically means to directly or indirectly support employee health with leadership behavior. 43 Leaders who engage in such a leadership style are usually also more interested in their own health status and are healthier themselves. 44 In line with this assumption, we propose the following hypothesis:
H7. Leaders with a higher score in health-promoting leadership are more likely to use an app in workplace health promotion than leaders with a lower score in health-promoting leadership.
Methods
Recruitment and selection
In cooperation with a German market research company, Austrian and German leaders were invited to participate in an online study by sending out e-mails. The e-mails were sent out by the market research company. The participants had to fulfill the requirement of currently having an official leading position at their company; otherwise they were excluded at the beginning of the survey. In all, 461 participants began to fill in the questionnaires of the survey. Out of this sample, 49 (10.6%) participants canceled their participation after answering only a few questions. A sample of 412 leaders who filled in all questionnaires could be used for the analyses. The whole survey lasted approx. 20 min. A complete participation was rewarded with a small financial incentive (2 Euro).
Participants
In this sample of 412 leaders, 49.3 percent were working in Germany and 50.7 percent were working in Austria; 31.6 percent were female and 68.4 percent were male. On average, the participants were 43 years old (mean = 43.2, standard deviation (SD) = 9.83) and worked in different business sectors, mostly in the business sectors service/consulting (16.3%), manufacturing (15.5%), commerce (12.1%), public sector (9.2%) health care (7.5%) and insurance (6.1%). The leaders worked in lower management (63.1%), middle management (28.9%) and top management (8.0%). Most of the leaders (35.8%) had their leading position for longer than 10 years, 29.2 percent had their leading position for 5–10 years, 20.9 percent for 2–5 years and 14.1 percent less than 2 years. The number of direct subordinates varied, ranging from only 1 subordinate (8.0%), 2–5 subordinates (33.1%), 6–10 subordinates (22.6%) and more than 10 subordinates (36.3%).
Almost every participant (90.5%) had a smartphone and 80.3 percent used it up to 3 h/day; 19.7 percent even used it more than 3 h/day. The smartphone users used their device for making telephone calls or sending short messages (92.2%), sending e-mails (71.9%), surfing in the Internet (55.1%), using social media (37.8%), using apps (26.5%), listening to music (25.4%) and playing games (20.8%). Almost a third (32.1%) stated to use technical equipment (e.g. smartphone apps, chest belts, GPS watches) for physical exercises.
Measurements
Neuroticism and extraversion
To assess neuroticism and extraversion, the short version of the Big Five Inventory was used in this study. 45 Neuroticism and extraversion are measured with two items, respectively. One example item for neuroticism is “I see myself as someone who … gets nervous easily.” Answer scale ranges from 1 (I strongly disagree) to 5 (I strongly agree).
Physical and mental health
Physical and mental health were measured with the 12-item Short Form Health Survey (SF-12). 46 The SF-12 is a subjective evaluation of the individual’s physical and mental health and higher values indicate being healthier. The 12 items can be calculated into two scores: (1) physical health and (2) mental health. One example item for the SF-12 is “Thinking about the past four weeks, have you accomplished less than you would like as a result of your physical health?” Each of the 12 items has a different scale format.
Stress and recovery
The RESTQ-Work 47 addresses different aspects of stress and recovery activities and states in the past 7 days/nights. In this study, the version RESTQ-Work-27 with 27 items was used. The items can be assigned to total scores of stress and recovery. One example item for a stress-related item is “In the past 7 days/nights … I felt frustrated through my work” and for a recovery-related item “In the past 7 days/nights … I was able to relax during my breaks.” The items can be answered on a 7-point-Likert scale ranging from 0 (never) to 6 (always).
Health-promoting leadership
Health-promoting leadership was measured with the Health-Promoting Leadership Conditions Questionnaire (HPLC). 43 In this study, the self-assessment version was used, where leaders are asked to rate themselves regarding their health-promoting leadership. The 21 items of the HPLC can be categorized into seven dimensions (health awareness, workload, control, reward, community, fairness and value-fit) and one total score of health-promoting leadership. One example item for the dimension health awareness is “In the last four weeks, as a leader I took care that … all employees are motivated to take care of their health.” The items can be answered on a 7-point Likert scale ranging from 0 (never) to 6 (always).
Next to these questionnaires, the likelihood of using an app for health promotion and the interest in apps specifically designed for leadership tasks were measured with scales previously developed for this study. All items are listed in Table 1.
Questions used in the study.
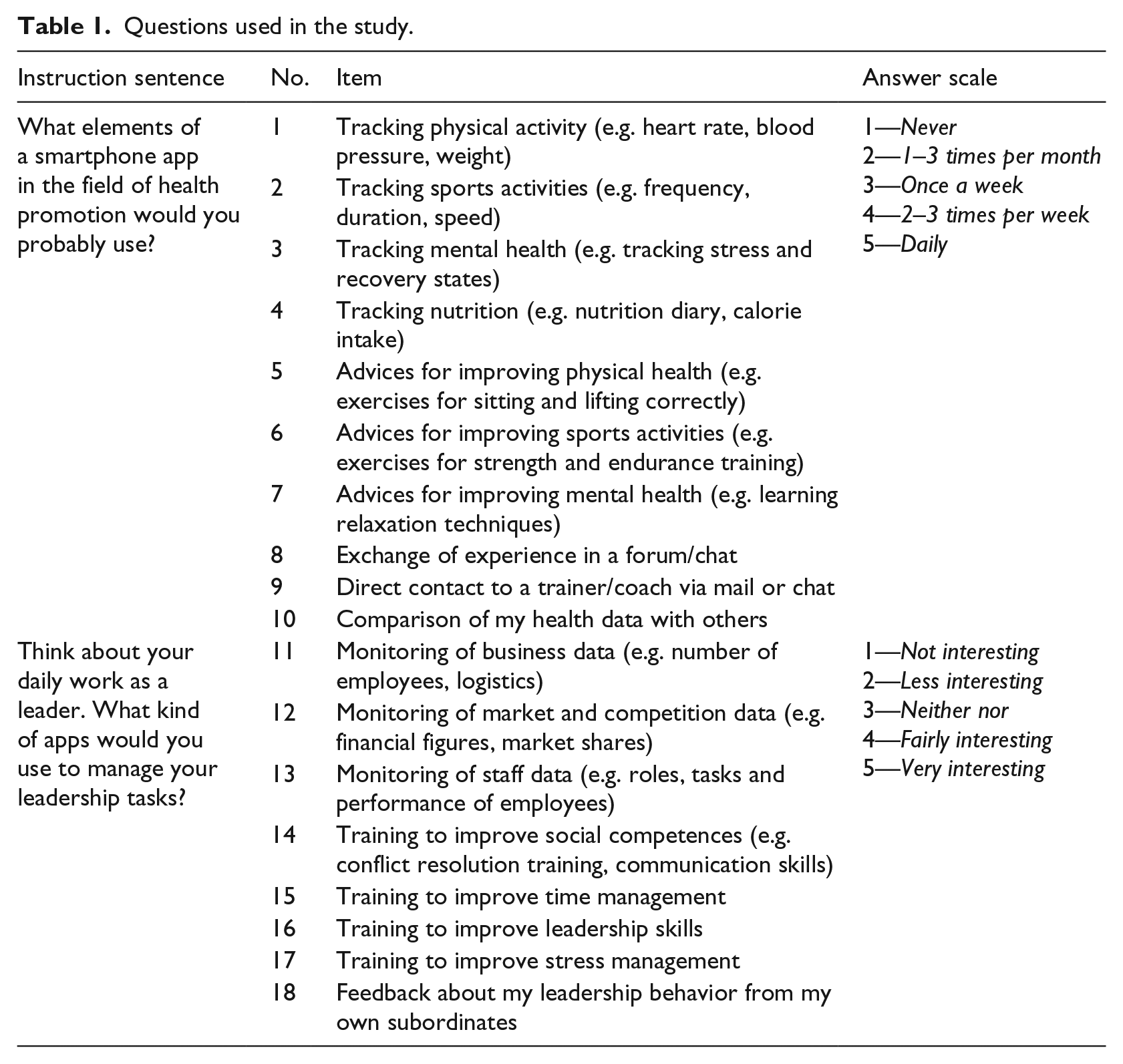
The likelihood of using an app for health promotion was measured with newly developed items. The instruction sentence “What elements of a smartphone app in the field of health promotion would you probably use?” was followed by 10 possible contents for a health promotion app (Table 1). The possible contents could be rated on a 5-point Likert scale from 1 (never) to 5 (daily).
The interest of using an app for leadership tasks was measured with eight items. After reading the instruction sentence “Think about your daily work as a leader. What kind of apps would you use to manage your leadership tasks?” the participants were asked to rate five possible contents for a leadership app (Table 1). The possible contents could be rated on a 5-point Likert scale from 1 (not interesting) to 5 (very interesting).
Results
Descriptive statistics
The means, SDs, internal consistencies and correlations of the dimensions can be found in Table 2.
Means, standard deviations and correlations between all study scales.
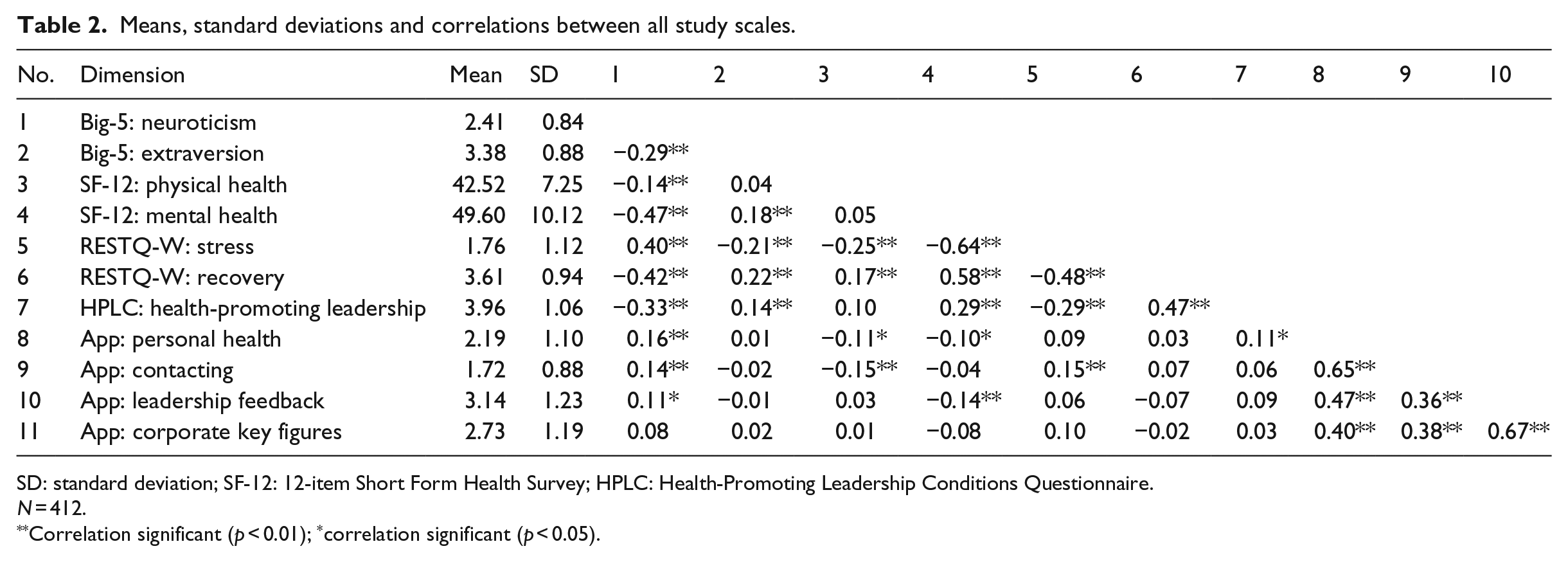
SD: standard deviation; SF-12: 12-item Short Form Health Survey; HPLC: Health-Promoting Leadership Conditions Questionnaire.
N = 412.
Correlation significant (p < 0.01); *correlation significant (p < 0.05).
Exploratory factor analysis
Exploratory factor analyses using principal component axis factoring and oblimin rotation were performed for the items of the newly developed questionnaires (“likelihood of using an app for health promotion” and “interest of using an app for leadership tasks”). For the scale “likelihood of using an app for health promotion,” the analyses showed a two-factor solution with eigenvalues of 6.08 (factor 1) and 1.04 (factor 2) explaining 64.22 percent of total variance (Kaiser–Meyer–Olkin (KMO) = 0.92, χ2(45) = 2829.840, p < 0.001). The scale “interest of using an app for leadership tasks” showed a two-factor solution with eigenvalues of 5.68 (factor 1) and 1.07 (factor 2) explaining 79.37 percent of total variance (KMO = 0.92, χ2(28) = 3170.222, p < 0.001). The four factors were named “personal health” (using an app to track personal health), “contacting” (using an app to get in contact with others), “leadership feedback” (using an app to improve leadership skills) and “corporate key figures” (using an app to track corporate key figures). The factorial solutions and their reliabilities (Cronbach’s alpha) are presented in Tables 3 and 4. Descriptive statistics for the factors as well as correlations with the other study variables are shown in Table 2.
Factor solution with oblimin rotation for the items of the scale “app for health promotion” (factor loadings < 0.30 are suppressed in this table).
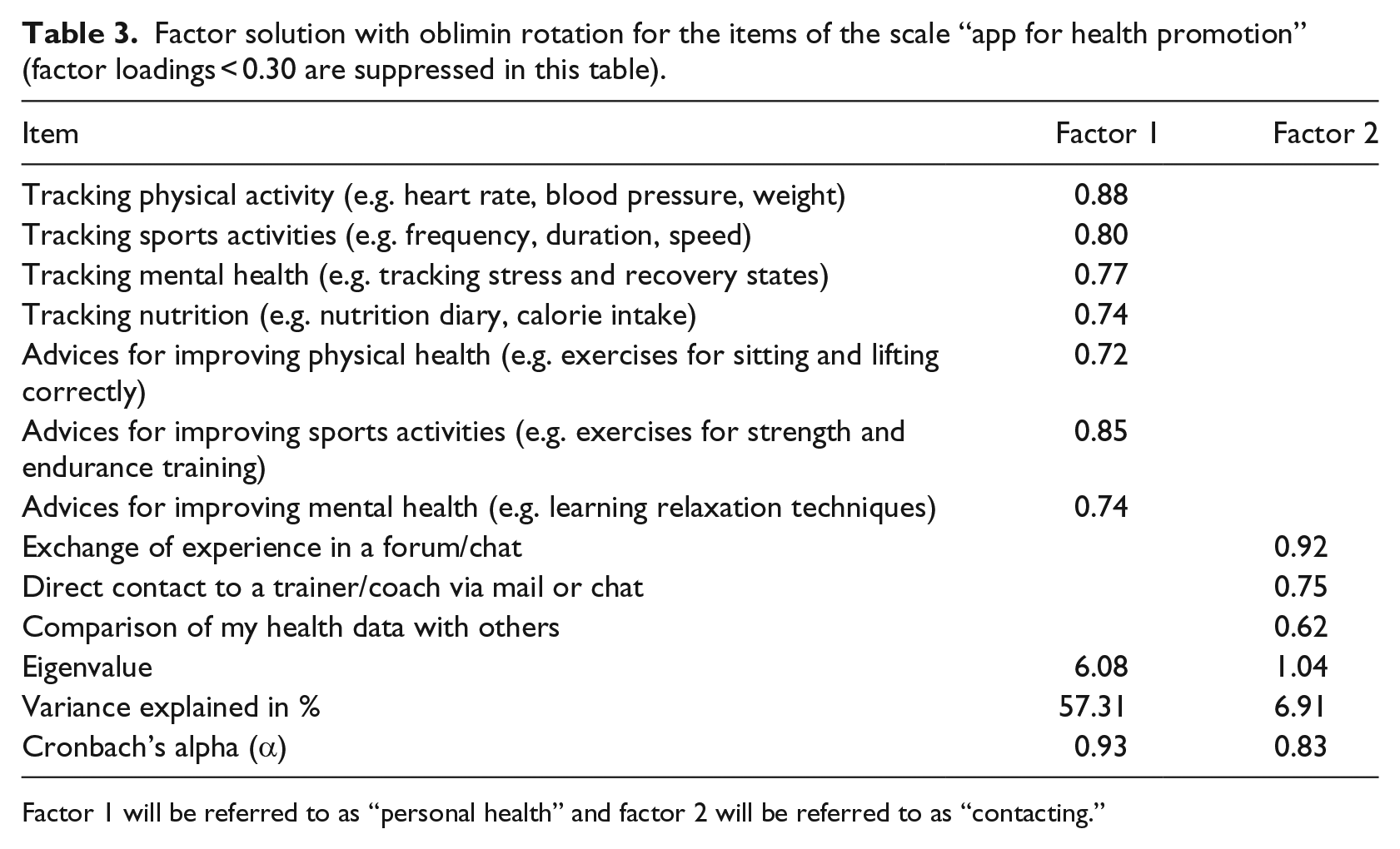
Factor 1 will be referred to as “personal health” and factor 2 will be referred to as “contacting.”
Factor solution with oblimin rotation for the items of the scale “app for leadership tasks” (factor loadings < 0.30 are suppressed in this table).
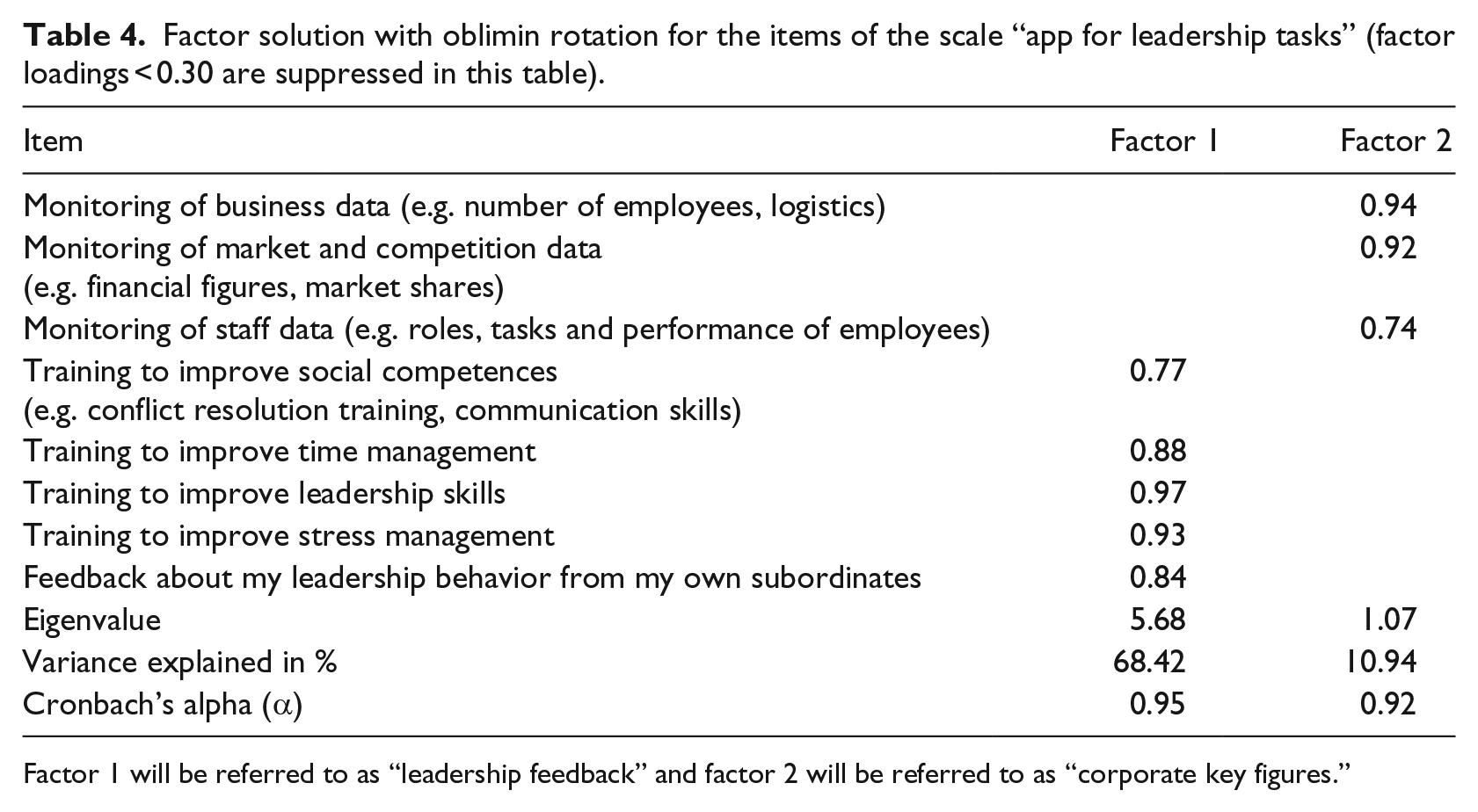
Factor 1 will be referred to as “leadership feedback” and factor 2 will be referred to as “corporate key figures.”
Hypothesis testing
Hierarchical multiple linear regression analysis was conducted separately for all outcome criteria (“personal health,” “contacting,” “leadership feedback” and “corporate key figures”). Table 5 presents the four steps of the analysis with their respective adjusted R2 (ΔR2). The ΔR2 for each step indicates how well the data of the entered variable fit to the model.
Results of the multiple regression analyses (standardized regression coefficients from the last step).
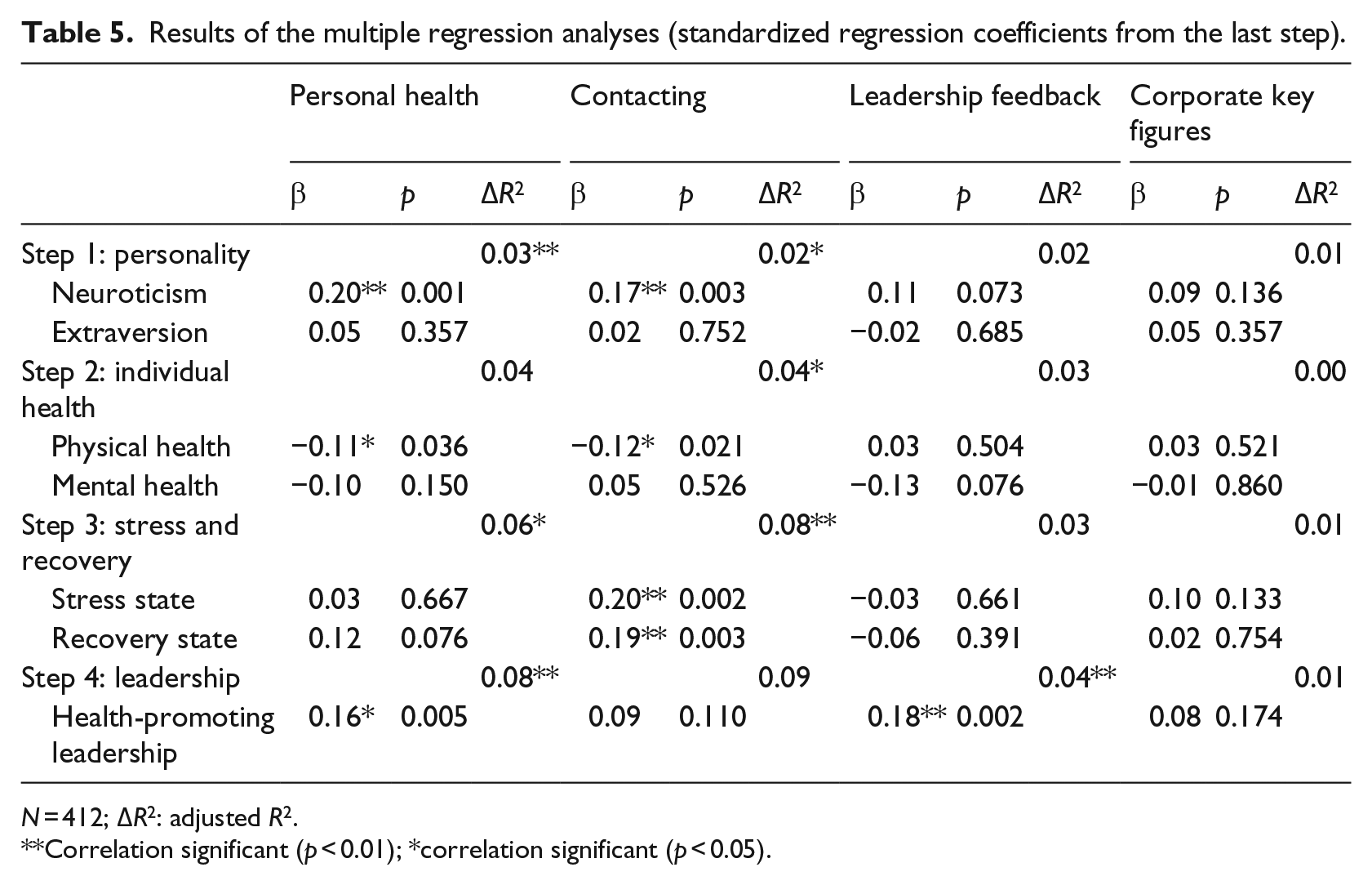
N = 412; ΔR2: adjusted R2.
Correlation significant (p < 0.01); * correlation significant (p < 0.05).
The predictors neuroticism and extraversion were stepped into the equation first. This step was significant for the outcomes “personal health” and “contacting.” The second comprised factors about health; this step was significant for the outcome “contacting.” Stress and recovery were entered in the third step. This step was significant for “personal health” and “contacting.” The extent of health-promoting leadership was entered in the regression at the last step and significantly accounted for an additional variance for “personal health” and “leadership feedback.” For the outcome “corporate key figures,” all steps showed non-significant results.
Neuroticism, physical health and health-promoting leadership were the most important predictors. As assumed in Hypothesis 1, neuroticism was positively associated with app usage (“personal health” and “contacting”). Hypothesis 2 could not be supported, as extraversion did not show a significant relation with all four outcomes. As for the health indicators, physical health was negatively associated with app usage for personal health and for getting in contact with others (Hypothesis 3), whereas mental health did not show any significant relationships (Hypothesis 4). Stress state and recovery state were both positively related to “contacting” (Hypotheses 5 and 6). As assumed in Hypothesis 7, health-promoting leadership is positively related to app usage (“personal health” and “leadership feedback”).
In Table 5, the standardized regression coefficients as well as p-values and adjusted R2 from the last step are presented.
Discussion
In this article, we aimed to identify leaders’ characteristics that could predict the participation in app-based health promotion activities. Four possible components of an app in health promotion could be identified: monitoring health behavior such as physical activity, nutrition or mental health (“personal health”), connecting with others and sharing health-relevant issues (“contacting”), using an app to monitor and improve leadership skills (“leadership feedback”) and using an app to track corporate key figures (“corporate key figures”). The user characteristics personality, health, work-related stress and recovery and extent of health-promoting leadership were analyzed for these four app components.
In past research, neurotic and introverted individuals are found to be more interested in using e-health and m-health applications. 27 We could support these findings only for neuroticism but not for extraversion. Neurotic leaders especially would use an app for monitoring of personal health and to get in social contact with others. This is in line with recent studies indicating that neurotic individuals benefit from the anonymity on the web and can get in contact with others without exposing themselves. 26 For extraversion, no significant results were found, which is surprising as many studies found introverts to use the Internet and its possibilities to a greater extent.21,27 An explanation for this result could lie in our specific sample of leaders. Research found that extraversion is the most important trait of leadership, indicating that extraverted persons are more likely to inherit a leadership position. 48 In our sample, the mean of extraversion is quite high, which means that our group of leaders consists of only a few introverts. Therefore, the non-significant results could be effects of a homogeneous group.
Physical health but not mental health of leaders is shown to be related to the likelihood of using apps for health promotion. As assumed, lower physical health is positively related to app usage, especially for monitoring of personal health and getting in social contact. Unhealthier individuals might benefit from e-health and m-health applications as this is a more comfortable way to monitor and share health problems. We expected the same for mental health, but this could not be confirmed with our findings. The reason for this non-significant result could lie in the construction of items. The items mainly focus on physical activity and less on psychological activities suited for people with mental health problems (e.g. training of self-efficacy or self-confidence). As for the app “leadership feedback” (which includes psychological activities such as “improving social competences” or “improving stress management”), a tendency that mentally unhealthier leaders would use a leadership app could be found. This supports the assumption that when focusing more on app content for psychological problems, significant differences should be found.
For work-related stress, we postulated that leaders with higher stress are more likely to use an app in health promotion. Significant results could only be found for the component “contacting.” Highly stressed leaders would seek help from others using an app. Similar to the results found for neuroticism, anonymity plays a major role. Addressing health-relevant problems at the workplace is challenging and sharing them with others is even more difficult. Anonymity provided via e-health and m-health solutions could support stressed leaders without exposing them to colleagues and thus avoiding embarrassment.
Regarding work-related recovery, leaders with higher recovery are more interested in using an app to get in contact with others regarding health-relevant issues. This seems to be contradictory to the previous finding regarding stress. However, having high stress and high recovery at the same time is not contradictory, as stress and recovery are not seen as opposites but as parallel processes. 49 Having high stress could be described with having a very demanding job, but at the same time it is possible having enough resources to feel recovered.
As our sample consists of leaders, leadership behavior in the form of health-promoting leadership was assumed to be positively related to using apps in health promotion. This assumption was confirmed for the app components “personal health” and “leadership feedback.” Leaders who engage in health-promoting leadership behavior to support employees’ health are more likely to use a leadership app to improve their leadership behavior and are more likely to monitor their own health behavior.
The app content “corporate key figures” did not show any relationships with our proposed predictors. It seems that compared to the other possible app components, leaders are less interested in this form of feedback. Actually, tracking corporate figures is not a strong component of workplace health promotion. Therefore, it might be possible that we did not include more relevant predictors for this outcome in our study.
Some limitations have to be addressed. Looking at the results, only small effects could be found, having low—although significant—adjusted R2. As we were able to collect a large sample of leaders in this study, we can benefit from this advantage and also see these small effects. The participants were recruited with an online panel, which on one hand has the advantage of reaching a large number of participants. On the other hand, a selection bias could occur as our sample consists of leaders having more affinity for technology and mobile communications. In our sample, almost every participant had a smartphone and a third uses technical equipment for physical exercises.
Conclusion
The findings showed that some characteristics of leaders on the interest and likelihood of using an app for health promotion at the workplace could be identified. Leaders with high neuroticism, high skills in health-promoting leadership and lower physical health are more interested in and are more likely to use an app at the workplace. They would especially use an app for monitoring personal health and to get in social contact about health-relevant issues. Other important factors are higher stress and higher recovery for the feature of getting in social contact via an app. Although we could not find one major predictor that influences the likelihood of using an app in health promotion, we suggest investigating other user characteristics next to the most common ones (e.g. demographics, personality) to get a clearer insight in the area of new tools in workplace health promotion. These predictors can further support in the advertising of e-health and m-health tools to raise the probability of using these tools. Furthermore, it would be interesting to investigate the usage of activity trackers in addition to smartphone apps, as activity trackers might be more suitable for monitoring health behavior than only using smartphone apps.
Footnotes
Acknowledgements
The authors want to thank the company Mikropis Holding, d.o.o, a partner in the project “24alife,” for sponsoring the recruiting of participants via the market research company.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.