
Abstract
This study identified specific types of online health-related activities that may promote preventive dietary behaviors. Two cycles (Cycles 1 and 3) of the Health Information National Trends Survey 4 were analyzed (N = 2606 and 2284, respectively; Internet users only). Similar types of activities were grouped to create three types of online activities: information seeking, engagement in health information technology, and social media use. In both cycles, online health information seeking and the engagement in health information technology were positively associated with two dietary behaviors (fruit/vegetable consumption and using menu information on calories) but not with soda consumption. Individuals may be exposed to new information or become more aware of their current health status through information seeking or health information technology engagement. However, social media use for health was not related to any of the dietary behavior. The results suggest that “how we use the Internet” may make a difference in health outcomes.
Keywords
Introduction
The Internet is the first source of health information for 70 percent of American adults. 1 People use the Internet not only to seek health information but also to engage in diverse activities that the Internet enables. 2 Prestin et al. 1 divided various online health-related activities (OHAs) into three categories. First is health information seeking, which refers to the purposeful search of specific health information. 3 According to the Pew Research Center, most Internet users in the United States (72%) use search engines to seek health information and others use professional websites such as WebMD. 2 Second is the engagement in health information technology (HIT). HIT is a tool to manage individual health, and HIT engagement includes use of online patient portals, computer-mediated communication with healthcare professionals, and mobile health device use. 4 Third is the use of social media, referred to as peer-to-peer healthcare. 2 The use of social media in the health context means the use (both posting and reading) of user-generated content from blogs, social networking sites, online support groups, or forums,1,5,6 where individuals share their opinions and seek those who have similar health problems. 2
Most previous studies have focused on how many people engage in OHAs or what sociodemographic factors are associated with such activities. For example, Prestin et al. 1 examined the percentage of US adults participating in several OHAs and found that social media use for health is still not common (less than 5%). Thackeray et al. 6 investigated two types of social media use (social networking and online reviews or rankings). Consulting online rankings or reviews regarding medical topics was predicted by chronic disease and higher income. Those with lower education and of the male gender were less likely to read online rankings and reviews. Older age and male gender predicted the use of social networking sites for health. Higher socioeconomic status (SES; measured by education and income), female gender, and having a chronic disease are consistent and positive predictors of HIT use and online health information seeking.4,5
However, little research has examined the associations between various OHAs and health outcomes. According to uses and gratification theory, 7 individuals actively select sources of information that can gratify their needs and expose themselves to such sources. Media effects can be partly seen as individuals’ choice to be influenced by the media. 8 Thus, the goals of individuals who choose social media for health information may differ from the goals of individuals who select professional health-related websites or communication with healthcare professionals. In other words, the difference in health-related goals causes the difference in media use, which may lead to differences in health outcomes. Previous health communication studies have supported this assumption. Lee and Chae 9 showed that only online health information seeking is negatively related to fatalistic beliefs about cancer prevention, while social media use or purchase of health products was not. Chae and Quick 10 found that mothers’ health information exposure regarding children’s health through a professional health-related website is different from exposure through an online community; the former is associated with positive health beliefs while the latter is not. These studies were conducted in specific contexts such as cancer and children’s health.
This study sought to examine the association between various OHAs and health outcomes in a general public health context: preventive dietary behaviors. Preventive dietary behaviors represent a health topic that applies to everyone. Fruit and vegetable intake provides nutrients and even reduces the risk of cancer and other chronic diseases. 11 The consumption of sugar-sweetened beverage can increase obesity and related disease. 12 Using calorie information posted on a menu also can decrease calorie intake and thus can contribute to weight loss.13,14 These behaviors can reflect a choice of lifestyle to maintain a nutritious diet and healthy weight. To date, most studies have considered demographic, socioeconomic, or psychological predictors of preventive dietary behaviors. For example, being a female, education, income, exercise frequency, and self-efficacy are positively associated with the intake of fruits/vegetables.15–17 In contrast, consumption of sweetened beverages is predicted by low SES, low self-efficacy, and less physical activity.18–20 Similarly, those with higher education and income tend to check calories on a menu for weight management. 13 However, the role of the Internet in promoting a healthy diet, despite its importance, has not been fully explored. Cancer-related information seeking increases the intake of fruits and vegetables among both cancer patients 21 and the general public aged 40–70 years, 22 but these studies did not consider OHAs and measured cancer information seeking from any source.
Thus, combining the two unanswered questions (i.e. the effect of OHA on health outcome and the role of OHA in healthy diet), the goal of this study was to identify specific types of OHAs that have potential to promote preventive dietary behaviors with nationally representative data. To achieve this aim, this study used two cycles (Cycles 1 and 3) of the Health Information Trends Survey (HINTS) 4, conducted by the National Cancer Institute. Among four cycles of HINTS 4, only these two cycles covered both various OHA items and dietary behaviors. The two cycles had different respondents and can be seen as two separate national surveys with similar items. Importantly, the analysis in this study included only Internet users among respondents. Because the Internet has a positive effects on health such as increased knowledge and informed decision-making, 23 this study sought to test whether engagement in OHAs can make further difference beyond the effect of the Internet.
Methods
Participants and procedures
HINTS is a nationally representative survey via mail among US adults. The Cycle 1 survey (N = 3959) was conducted from October 2011 through February 2012 and Cycle 3 (N = 3185) from September through December 2013. The overall response rate was 37.91 percent and 35.19 percent, respectively, based on the American Association for Public Opinion Research response rate 2 (RR2) formula. For more information, see the HINTS homepage (http://hints.cancer.gov). A total of 3959 people completed the Cycle 1 questionnaire. Cycle 1 had both a long-form and a short-form questionnaire. Deleting the short forms, which did not cover OHAs, left 3516 cases. Then, to the question “Do you ever go online to access the Internet or World Wide Web, or to send and receive e-mail?,” those who replied with “yes” were included (Internet users). Ultimately, 2606 cases were included. In the same way, Cycle 3 originally had 3185 responses, but 2284 cases were included. For descriptive statistics of two cycles, see Table 1.
Descriptive statistics (Cycle 1, N = 2606; Cycle 3, N = 2284).
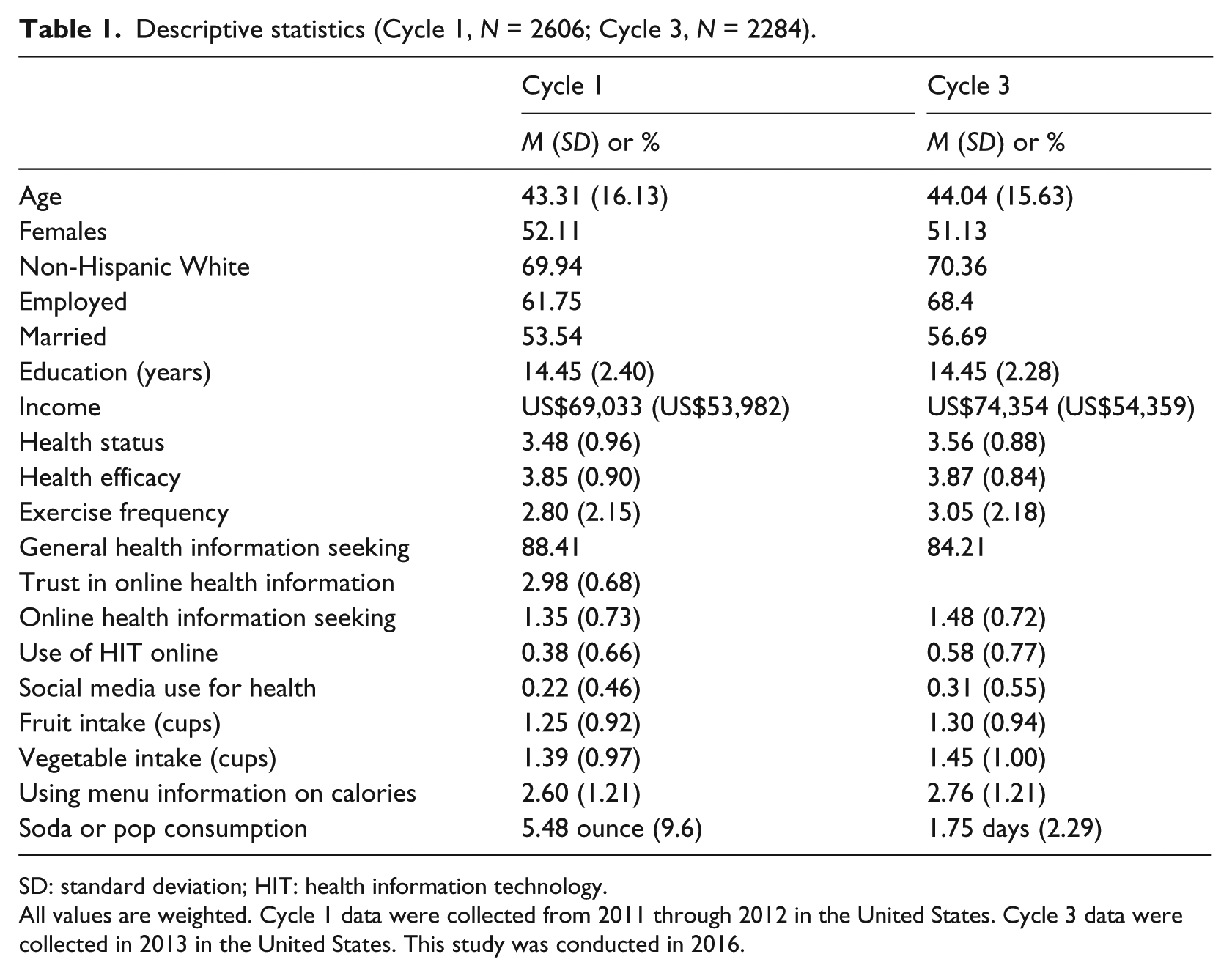
SD: standard deviation; HIT: health information technology.
All values are weighted. Cycle 1 data were collected from 2011 through 2012 in the United States. Cycle 3 data were collected in 2013 in the United States. This study was conducted in 2016.
Measures
OHAs
Each cycle had variations in OHA items, and this study used the same items across the two cycles to maintain consistency. Among all possible OHA items that HINTS provides, only items that are (1) common to both cycles, (2) potentially related to dietary behavior, and (3) have more than one similar item (to create an index) were chosen. Finally, the following eight OHA items were chosen: (a) looked for health or medical information for yourself; (b) looked for health or medical information for someone else; (c) looked for a healthcare provider; (d) downloaded health information to a mobile device, such as a cell phone, tablet computer, or electronic book device; (e) kept track of personal health information such as care received, test results, or upcoming medical appointments; (f) used email or the Internet to communicate with a doctor or a doctor’s office; (g) shared health information on social networking sites, such as Facebook or Twitter; and (h) participated in an online forum or support group for people with a similar health or medical issue. All eight items were recoded (1 = yes, 0 = no).
To create indices of OHAs, an exploratory factor analysis (EFA) was conducted via Mplus 7.11. In principle, these OHAs are not appropriate for EFA. Muthén and Muthén 24 stated that EFA should be performed with variables developed to measure certain domains. HINTS items do not form a scale to measure one construct. They are the list of various OHAs. It is possible for an individual to engage in one behavior but not in other behaviors in the list. Thus, EFA in this study was used just to identify a set of items that are more strongly correlated with each other than other items, but not to identify dimensionality of a latent variable. An EFA with eight items in Cycle 3 was performed. Based on Hu and Bentler’s 25 criterion, which suggests that a good model should have a root mean square error of approximation (RMSEA) of ≤0.06, a comparative fit index (CFI) of ≥0.95, and a standardized root mean square residual (SRMR) < 0.08, the three-factor model showed an excellent fit: χ2(7) = 5.089, p > 0.05, RMSEA = 0.00, CFI = 1.00, and SRMR = 0.02. An examination of factor loading (geomin rotation) and factor structure showed that the first factor consisted of two information seeking items (a and b), the second factor consisted of tracking personal health information and e-communicating with providers (e and f), and the third factor consisted of two social media items (g and h). However, c (0.34 and 0.34) and d (0.39 and 0.38) almost equally loaded on both the first and the second factor.
When conducting the same analysis with Cycle 1, a three-factor model was not identified but a four-factor model showed a perfect fit: χ2(2) = 0.567, p > 0.05, RMSEA = 0.00, CFI = 1.00, and SRMR = 0.01. The results were almost the same. The aforementioned three factors were clearly differentiated, but c and d again showed a problem; (c) loaded on the same factor with information seeking items (a and b), and (d) alone loaded on another fourth factor. Based on the results, the study identified three types of OHAs: independent health information seeking (not from providers), use of HIT, and social media use. Information seeking for oneself (a) and someone else (b) represent a traditional information seeking activity, a purposive and non-routine information acquisition, outside of normal exposure to information sources. 3 Tracking personal health information and e-communicating with providers (e and f) are about management of one’s health using HIT, and these two same items were used in Jackson et al. 4 as HIT engagement. Sharing health information on social media and participation in online support groups (g and h) are clearly social media use. Thus, each of the three categories consisted of the sum of two dichotomized items. Downloading information (d) and looking for a provider (c) were excluded, because they showed inconsistent results in both cycles. In this way, the categorization based on EFA was consistent with the result of correlation analysis (i.e. each item was coupled with another activity most strongly correlated with it in the bivariate correlation) as well as previous studies.4,6
Fruit and vegetable intake
Fruit and vegetable intake was measured in the same way in the two cycles: how many cups of fruits and vegetables (including 100% juice) participants eat or drink each day (0 = none to 6 = 4 or more cups). The item was originally measured on an ordinal scale and transformed to a ratio scale variable to meet the assumptions of ordinary least squares (OLS) regression. Each response option was replaced with the mean value of that interval. For example, 0 (= one) was still 0, but 1–2 cups was recoded as 1.5 cups. Regarding the lowest and highest options (i.e. 1 = ½ cup or less and 6 = 4 or more cups), the upper bound and the lower bound were used (i.e. 1 = ½ cup and 6 = 4 cups). Fruit intake and vegetable intake were averaged.
Sugar-sweetened beverage consumption
Participants reported the amount of sugar-sweetened soda or pop they drank each day. The response was measured on a 6-point scale in Cycle 1 (0 = none to 5 = more than 48 ounces) and on another 6-point scale in Cycle 3 (1 = none to 6 = every day). Responses were recoded to represent the actual amount or actual frequency. For example, option 2 (13–24 ounces) was recoded as 18, the mean value. Option 6 in Cycle 3 was recoded as 7 (days). Due to the difference in the scales, the two variables were standardized to be consistent across the two cycles.
Calorie check
Calorie checking behavior was measured by asking the frequency of using menu information on calories before ordering food (0 = never to 5 = always).
Covariates
The same covariates were adopted in both cycles. First, demographics and SES factors were adjusted: age, gender (1 = female, 0 = male), race/ethnicity (1 = non-Hispanic White, 0 = other), education, income, marital status (1 = married, 0 = not married), and employment status (1 = employed, 0 = not employed). Education and income were based on an ordinal scale and transformed in the same method used to recode fruit and vegetable consumption. Education was recoded as years of formal education and income as the actual amount of money. For example, college graduates (= 6) were coded as 16 (years). Among them, age, gender, race/ethnicity, income, education, employment, and marital status influence OHAs.9,26,27 Gender, race/ethnicity, education, and income are important predictors of fruit and vegetable consumption28,29 and soda intake. 20 Education and income influence calorie checking behavior. 13 Second, as health-related variables, health status (1 = poor to 5 = excellent), exercise frequency (0 = none to 7 = 7 days per week), and health efficacy (1 = not confident at all to 5 = completely confident) were chosen. These variables are the significant predictors of fruit and vegetable intake.15,16 Third, this study also controlled for information-related variables associated with OHAs. General health information seeking from any source (1 = yes, 0 = no) was included because it should be positively associated with online health information seeking. Trust in the online health information was used because it influences online health information seeking. 9
Statistical analyses
OLS regression was performed via STATA 14, which can reflect two types of weights in HINTS: a full-sample weight (for population estimates) and a set of 50 replicate weights (for standard errors of the estimates). Thus, all numbers are weighted values. For each cycle, three regression analyses were conducted, each having fruit/vegetable consumption, soda consumption, and calorie checking, respectively, as dependent variables (DVs). Three types of OHAs and covariates were entered in the regression equation.
Results
Cycle 1
Before conducting the main analysis with Internet users only, to confirm a difference between Internet users and non-users, a t-test was performed as a preliminary analysis. For all three DVs, a significant difference existed between Internet users and non-users. Non-users were less likely to consume fruits and vegetables (t (3433) = −3.12, p < 0.01), more likely to drink soda (t (3442) = 2.31, p < .05), and less likely to check calorie information (t (3452) = 7.23, p < .001) than Internet users. Then, to see if OHAs can make a further difference among Internet users, regression analysis was performed.
The first model had fruit/vegetable consumption as the DV. The model was significant and explained 14.87 percent of the variance in the DV. Those who used online HIT consumed more fruits and vegetables. Female gender, health status, health efficacy, and exercise frequency were significant predictors. The second model used calorie checking as the DV and accounted for 10.7 percent of the variance in the DV. Online health information seeking was positively associated with the DV, as were age, female gender, exercise frequency, and general health information seeking. The third model had soda consumption as the DV (R2 = 12.56%). Those with younger age, male gender, low education, and low income were more likely to drink soda, but OHA was not a significant predictor. Social media use was not associated with any preventive behavior. For unstandardized coefficients and jackknife standard errors, see Table 2.
The results in Cycle 1 (N = 2606).
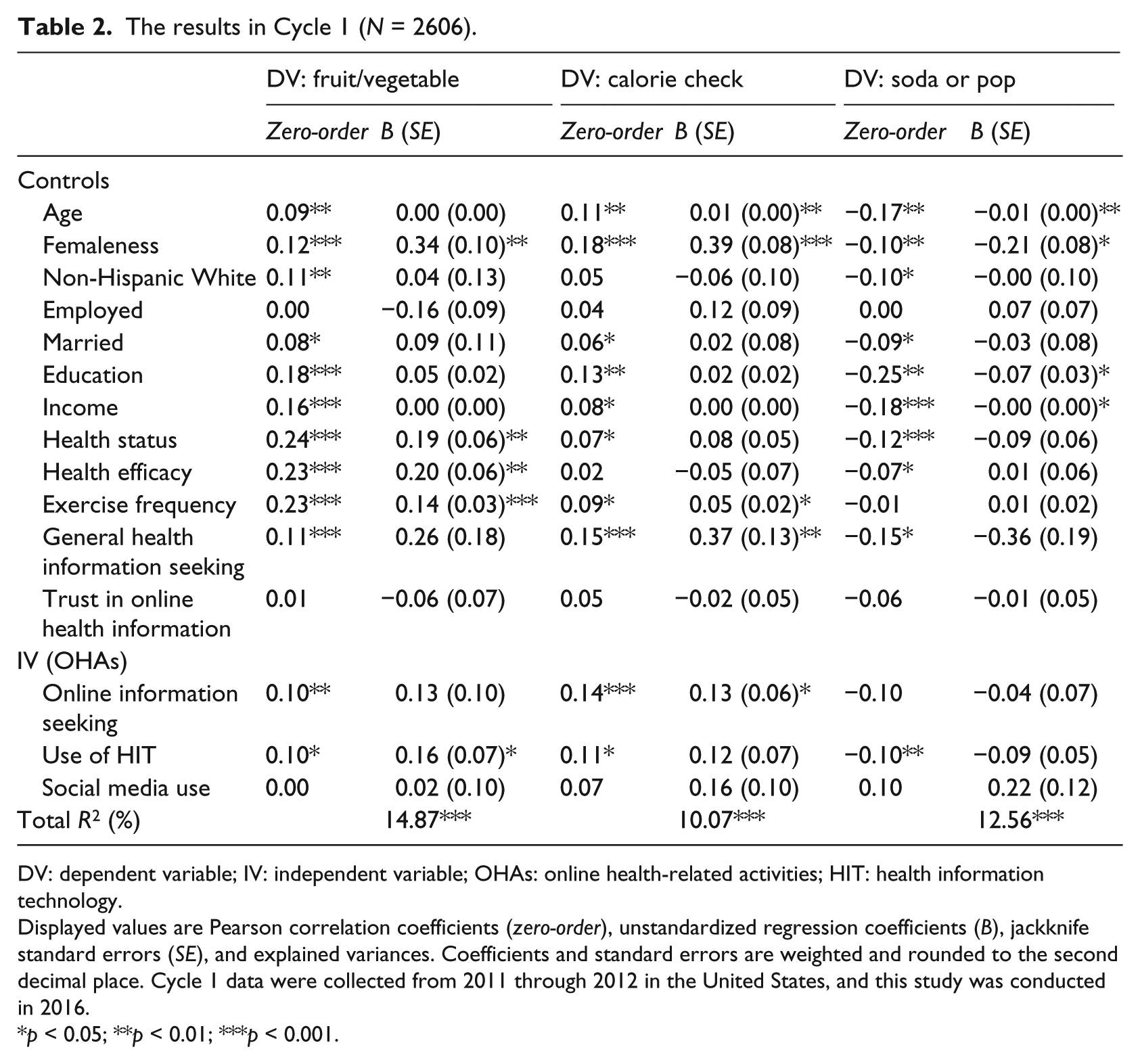
DV: dependent variable; IV: independent variable; OHAs: online health-related activities; HIT: health information technology.
Displayed values are Pearson correlation coefficients (zero-order), unstandardized regression coefficients (B), jackknife standard errors (SE), and explained variances. Coefficients and standard errors are weighted and rounded to the second decimal place. Cycle 1 data were collected from 2011 through 2012 in the United States, and this study was conducted in 2016.
p < 0.05; **p < 0.01; ***p < 0.001.
Cycle 3
The results of preliminary analysis were the same as in Cycle 1. Non-users showed a lower mean level of fruit/vegetable intake (t (3081) = −5.10, p < .001) and calorie checking (t (3119) = −8.10, p < .001) and a higher mean level of soda intake (t (3125) = 5.05, p < .001) than Internet users. Then, with only Internet users, the main analysis was conducted to see any further difference.
The fruit/vegetable consumption model was significant and explained 13.39 percent of the variance in the DV. Online health information seeking was positively related to the DV, along with female gender, education, and exercise frequency. Calorie checking (R2 = 10.03%) was predicted by the use of HIT. In addition, those with female gender, higher income and education, and higher frequency of exercise were more likely to check calories on a menu. In the soda consumption model (R2 = 16.28%), younger people, less educated people, and males were more likely to drink soda or pop. As in Cycle 1, social media use was not associated with any of the DV. For unstandardized coefficients and jackknife standard errors, see Table 3.
The results in Cycle 3 (N = 2284).
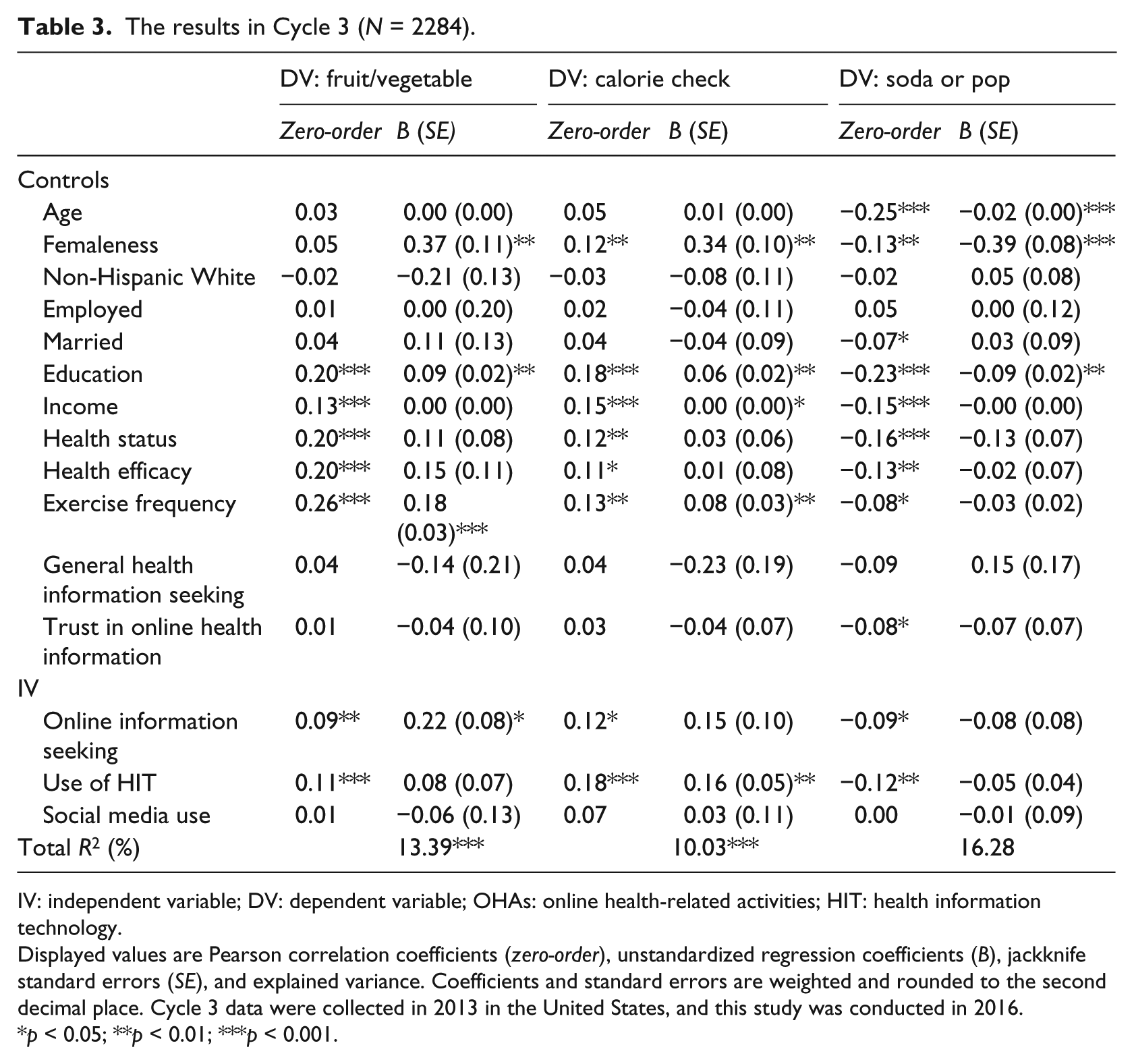
IV: independent variable; DV: dependent variable; OHAs: online health-related activities; HIT: health information technology.
Displayed values are Pearson correlation coefficients (zero-order), unstandardized regression coefficients (B), jackknife standard errors (SE), and explained variance. Coefficients and standard errors are weighted and rounded to the second decimal place. Cycle 3 data were collected in 2013 in the United States, and this study was conducted in 2016.
p < 0.05; **p < 0.01; ***p < 0.001.
Discussion
This study examined associations between various OHAs and preventive dietary behavior based on uses and gratifications theory. Online health information seeking and the engagement in HIT were positively associated with two of the three preventive dietary behaviors, but social media use was not associated with any of the behavior. The implications of the findings are discussed below.
Online health information seeking and HIT engagement
This study demonstrated that seeking online health information and the use of HIT online have the potential to increase healthy dietary behaviors. The results indicated that the two activities differ conceptually but have a similar beneficial impact on health. Through information seeking for oneself and someone else, individuals will acquire new information or reconfirm their existing knowledge about health. Using HIT—tracking personal medical information or contacting providers online—individuals have the opportunity to understand their own health status better and learn what types of preventive measures would benefit them. The difference between the two types of activity is that online health information seeking does not require help from healthcare professionals, but the use of HIT entails provider involvement. Tracking personal health records or e-communication with doctors means a past or future medical appointment. Thus, through online health information seeking, individuals acquire information in which they have a personal interest, but the information is more general rather than tailored for them. Using HIT, individuals can acquire more specific and tailored health information with the help of healthcare professionals. However, despite the difference, the effects of each activity are similar. In this study, when one was a significant predictor, the other was not. In Cycle 1, a positive association existed between information seeking and fruit/vegetable consumption and between HIT use and calorie checking. In Cycle 3, the results were the opposite. Thus, rather than having differential effects, both activities have similar beneficial effects on health outcomes. Supporting this assumption, after the main analyses, the associations between the average of four items (two items about information seeking and two items about HIT) and the three DVs were tested. The average of four items was a significant predictor of both fruit and vegetable intake and calorie checking in both cycles. Therefore, although the types of information that each activity provides are somewhat distinct, the mechanism through which the acquired information influences health may be similar. As Ramírez et al. 22 suggested, by providing new information, these activities may influence health motivation to perform preventive behaviors, instruct practical ways to perform the behaviors, and psychologically encourage such behaviors.
Social media use for health
However, findings regarding social media use were different from those regarding other OHAs. This study did not find any effect of social media. The use of social media was not even correlated with dietary behaviors in the bivariate analysis. Although consistent with previous studies that reported no association of social media with health beliefs,9,10,30 the results raised a question about the use of social media for health. Individuals can acquire new information through social media postings and share opinions and experiences with other users, but such activities might function differently from other OHAs. This study suggests five possible reasons. First, health information from social media mostly comes from peers 2 and thus sometimes it can be incorrect or outdated. 9 In such case, health information acquisition would not lead to a positive outcome. Second, the outcome of social media use may depend on one’s online social capital. For example, Yoo and Jeong 31 demonstrated that social media use has positive psycho-social effects only when the user has high online social capital. Likewise, the type of information that one can get from social media can vary depending on the number of online friends or the identity of online friends. Third, based on uses and gratification theory, those who use social media for health have goals other than information acquisition. For example, participation in an online support group might be more appropriate for obtaining emotional support rather than practical information.
Fourth, people who rely on social media for health may differ from those who depend on other OHAs. To demonstrate this, a further analysis was performed after the main study. Three OHAs were regressed on the covariates used in the study. In both cycles, consistently, education and general health information seeking were positively associated with online information seeking and the use of HIT. However, social media use for health was predicted only by younger age and female gender, and it was even negatively related to income. In previous studies, gender and age were consistent predictors of social media use for health,5,32 but other factors showed an inconsistent or no relationship.6,32 It seems that online information seeking and HIT engagement are more consistently associated with higher SES, which can partly explain why such behaviors differ from social media use. Fifth, the percentage of people using social media for health is still lower than for the other two activities. In Cycle 1, 80.5 percent of respondents did not use social media for health but only 15.1 percent did not seek health information and 71.5 percent did not engage in HIT. Similarly, in Cycle 3, 74.1 percent were not users of social media for health, but only 13.6 percent were non-seekers of health information and 59.3 percent did not engage in HIT (weighted percentage). As Prestin et al. 1 suggested, in the health context, social media use is still not very usual, and this may be related to its less clear effect on health outcomes. However, a meta-analysis showed that health intervention using social media is effective for behavior change. 33 Carefully conducted social media interventions are necessary, but the point of this study is that mere exposure to health information from social media might not be helpful.
Implications for the digital divide
This study confirmed that how we use the Internet matters for health and extended the scope of the digital divide. Although the racial and socioeconomic disparities in computer and Internet access have been closing, the gap in the quality of access and how to use the Internet still can make a difference in health outcomes. 34 Previous studies have shown that differences in SES can influence the engagement in OHAs. Higher SES is linked to HIT engagement, such as the use of an online patient portal among diabetes patients 35 or online personal health records 36 as well as health information seeking. 5 Rains 37 showed that broadband users are more likely to engage in diverse OHAs, meaning that the quality of access brings about differences in how we use the Internet. Adding to previous findings, this study showed that the type of OHA can make a further difference even among Internet users, when all SES and health-related factors are controlled for. The findings imply that the digital divide and health disparities are still ongoing issues. Communication technology is changing at higher speeds than ever before. New technology will appear and will require better equipment or higher subscription costs, 38 and it will make possible new OHAs that lead to a healthy life, but are available only to some people.
Limitations and suggestions for future studies
This study has several limitations. First, the data were cross-sectional and the causality of the suggested relationships cannot be established. It is possible that those who engage in healthy behaviors are more interested in OHAs. However, the effect of information seeking on dietary behaviors has been demonstrated in a longitudinal study. 21 Thus, the effect of health information on dietary behaviors exists, and this study showed one possible association focusing on OHAs. Second, to measure OHAs and dietary behaviors, this study used items provided by HINTS. For other types of OHAs and healthy behaviors, the suggested relationships might not be significant. For example, no OHAs predicted the intake of sugar-sweetened beverages in this study. The intake might be associated with other types of OHAs. Third, the intake of sugar-sweetened beverages was operationalized as the amount in Cycle 1, but as the frequency in Cycle 3. Those two different measures were standardized in the analysis. Future research should use more diverse and reliable measures for OHAs and healthy behaviors and test their relationships.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.