
Abstract
The aim of the review was to describe consumer-led health-related online sources and their impact on consumers. The review was carried out as an integrative literature review. Quantisation and qualitative content analysis were used as the analysis method. The most common method used by the included studies was qualitative content analysis. This review identified the consumer-led health-related online sources used between 2009 and 2016 as health-related online communities, health-related social networking sites and health-related rating websites. These sources had an impact on peer support; empowerment; health literacy; physical, mental and emotional wellbeing; illness management; and relationships between healthcare organisations and consumers. The knowledge of the existence of the health-related online sources provides healthcare organisations with an opportunity to listen to their consumers’ ‘voice’. The sources make healthcare consumers more competent actors in relation to healthcare, and the knowledge of them is a valuable resource for healthcare organisations. Additionally, these health-related online sources might create an opportunity to reduce the need for drifting among the healthcare services. Healthcare policymakers and organisations could benefit from having a strategy of increasing their health-related online sources.
Introduction
The Internet has become the major resource of information relating to health,1,2 and its use by healthcare consumers is expected to increase. 3 The Internet, with its ubiquitous nature and potential anonymity, 4 has fascinated millions of healthcare consumers who access it every day to find health-related information.5,6 The channels that the healthcare consumers use, either for obtaining or sharing health-related information, are, in this review, called health-related online sources. In this review, the sources are assumed to be consumer-led, which here means that they are not offered by healthcare organisations. For the Internet user searching for health-related information, this review uses the term consumer, which has replaced the term patient. 7 Health policymakers have begun to recognise the potential of the Internet as a source of consumers’ experiences, 4 and, in the United Kingdom’s National Health Service (NHS) Future Forum Report on Information, 8 have actually talked about ‘a new culture of transparency and public voice being fuelled by the digital revolution’.
Studies have revealed the need for combining healthcare and the Internet in order to produce better services.9–11 Previous studies have addressed this idea from four key viewpoints. The first observed health-related online sources through the lenses of marketing and was, therefore, interested in how the marketing of health services can benefit from online sources and consumers’ experiences.12,13 The second viewpoint was related to health science, which, in most cases, focused on how successful interventions, tools and guidelines using the Internet11,14 were. The third viewpoint covered misleading and unverifiable information.15,16 The fourth viewpoint was technological, which primarily examined the development of health-related online sources for the purposes of healthcare. 17 Despite the increased research interest in the use of the Internet in the healthcare context, research into health-related online sources seems to be limited: quite little is known about their impact.4,6
The aim of this study is to describe the consumer-led health-related online sources and their impact on consumers. The research questions are as follows:
How have health-related online sources been studied in the past?
What kind of consumer-led health-related online sources have been accessed between 2009 and 2013?
What kinds of impact of health-related online sources have been explored by previous studies?
The use of health-related online sources, drifting among them and the implications
Internet usage differs between countries and across continents. For example, mainstream culture might create certain attitudes towards Internet use, thereby reducing it among a certain part of the population. Also, access to the Internet varies and is most often bound to the development of the country. 18 Users of the Internet, compared to non-users, tend to be more educated and have better earnings; their mean age is 45.8 years.19–21 Several studies have reported health-related Internet usage to be more common among women.19,20 The Norwegian study carried out by Wangberg et al. 3 found no significant differences between genders’ health-related Internet use. This review uses characteristics of Internet users that could be applied to the Scandinavian population, where Internet use is very high. The Scandinavian countries all have similar health-related Internet usage. According to Norwegian, Swedish and Finnish studies, nearly 70 per cent of Scandinavian people have used the Internet to find illness, nutrient or other health-related information,3,22,23). Using the Internet for these purposes is, in this review, understood to mean using health-related online sources; the channels offering such information are referred to as health-related online sources. When healthcare consumers offer these sources, these sources are, in this review, understood to be consumer-led.
The relationship between healthcare consumers and the Internet is to be expected, since learning more about a disease and interacting with others in a similar situation are the major coping strategies used by the consumer. 9 Ye 24 found that people without a family history of cancer were half as likely to participate in online health activities. Healthcare consumers as users of the Internet play different roles: patients, caregivers and family members coping with the illnesses of others in the household. 1 It has been claimed that online consumers do not want to be treated as stereotypical patients with a specific condition. 25 Thus, one of the main ways in which healthcare consumers are asserting their individuality is through the Internet and online sources. The Internet offers a way to question healthcare providers and professionals; 26 search for information relating to second opinions, complementary or alternative medicines; and learn about specific diagnoses. 20 The Internet increases the consumers’ ability to influence their healthcare. 9 The information taken from the Internet seems to be highly appreciated,20,27 since as much as 60 per cent of consumers looking for information on the Internet considered the information found to be as good as, or better than, the information received from a doctor. 20
Healthcare consumers’ feedback is posted on the Internet for the whole world to see, 28 and thus, it offers scientists, society and end-users the chance to learn what their consumers have to say. In addition, in most Scandinavian countries, healthcare is in crisis caused by an ageing population and failing economies. 29 The Internet has been seen as society’s chance to secure good patient-centred care, since the major benefit of the Internet is its ubiquitous nature. Thus, it can be easily applied in healthcare environments to solve modern challenges. 28 Ultimately, the evaluation and usage of health-related online sources is a job for end-users, for whom these online sources can provide an opportunity to produce services that are of high quality, driven by experience-based knowledge, to increase the safety of consumers and to help healthcare administrations to find innovative ways 30 of using such health-related online sources for development.
Methods and materials
The review was carried out as an integrative literature review with a qualitative content analysis being used as an analysis method. The integrative review method was chosen for this review since it is especially useful and applicable in areas where there is only a little pre-existing knowledge and where the issues are complex and require more detailed exploration. Literature searches were conducted in accordance with guidelines relating to literature reviews. 31
The data were collected using well-known healthcare and administration databases: CINAHL, Business Source Complete (EBSCO), ABI/INFORM complete and PsycINFO (Table 1). To make sure that information retrieval was relevant, a librarian was consulted to determine the appropriate search strategy for this area of research. The information retrieval was carried out by using relevant words for the phenomenon, including their combinations and synonyms, and by finally undertaking test searches in the selected databases. The search for some terms was limited to the title of the article in order to deal with the volume of results. The inclusion and exclusion criteria for the studies were determined at the beginning of the process.
Search strategy.
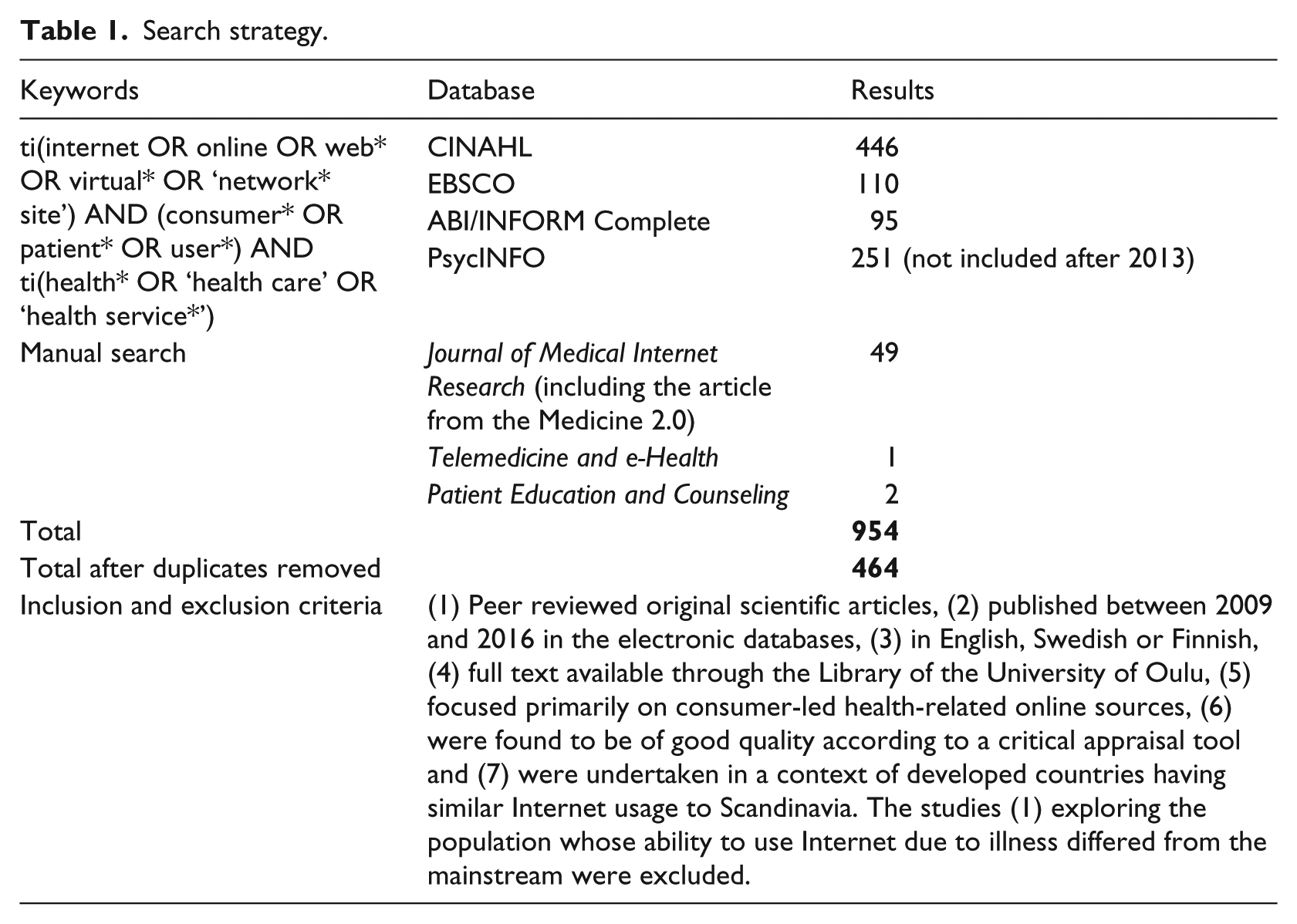
In this review, a manual search was carried out using the journals that appeared to include good and relevant studies after the database search. The journals scrutinised were: The Journal of Medical Internet Research, Telemedicine and e-Health, and Patient Education and Counseling. While researching The Journal of Medical Internet Research using its official webpages, one good article was found from a journal called Medicine 2.0, and it was included. The previous year range of 2009–2016 was also valid for this search. In total, the number of articles found was 954, which reduced to 464 after duplicates were removed using Refworks.
Following the information retrieval, the studies’ titles and abstracts were screened by the primary author. If no abstract existed, or a decision on inclusion could not be made from the abstract alone, the whole text was analysed. In the second screening, the studies’ complete texts were screened and, prior to inclusion, their quality was appraised by two independent researchers using their own criteria for quantitative, qualitative and mixed-methods studies. Suitable critical appraisal tools were found from the list by the Sansom Institute 32 and modified forms of the following tools were applied: McMaster Critical Review Form (for quantitative studies), Critical Appraisal Skills Programme (CASP) screening tool for qualitative studies and Evaluation Tool for Mixed-Methods Studies. Since there is no specific threshold to determine whether a study is of sufficient quality, 33 the studies were included if they met a minimum of 50 per cent of the addressed criteria or were otherwise felt to be of sufficient quality. If there were any disagreements over the quality, they were resolved through discussions and further reading of the full text until a consensus was reached.
Finally, 26 studies were chosen. The studies were analysed by using qualitative content analysis in which the aim is to understand the contents of the text and search for the essential themes in the studies. 34 In addition, quantisation was used while addressing the first research question. After reading and understanding the content of the studies, the following topics were produced for addressing the second research question: health-related online communities, health-related rating webpages and health-related social networking sites (Table 2). The following impacts were found that addressed the third research question: peer support, empowerment, health literacy, physical, mental and emotional wellbeing, illness management and relationships between healthcare organisations and consumers.
Studies exploring health-related online sources and their impacts.
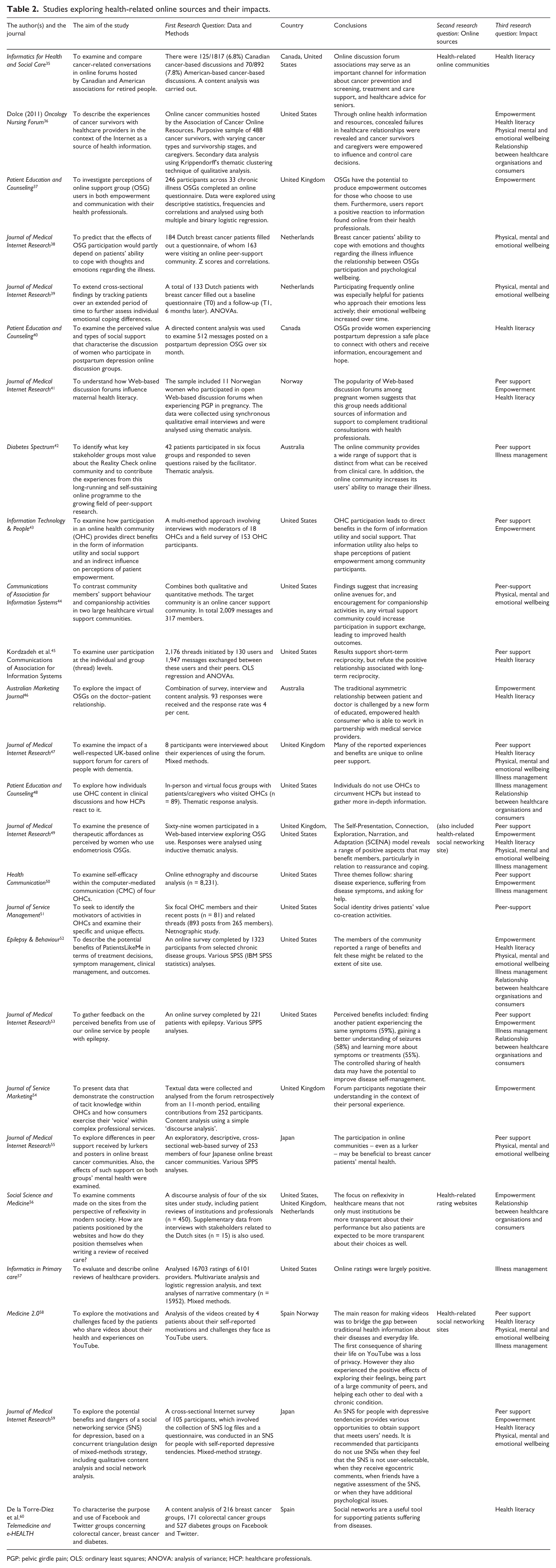
PGP: pelvic girdle pain; OLS: ordinary least squares; ANOVA: analysis of variance; HCP: healthcare professionals.
The research methods used and the branches of sciences covered in studies exploring health-related online sources and their impact on consumers
Of the 26 studies selected for this review (Table 2), 13 were carried out using qualitative methods, seven using quantitative methods and six using a mixture of both. The sources of the information were most often healthcare consumers but caregivers were also included in a few studies. By caregiver, studies meant either healthcare professionals or relatives of a patient suffering from a specific illness. Research data were most often collected either through observation or using surveys but a few studies used interviews, and one study was carried out as secondary analysis. The most popular method was observation, which was most often used in the context of health-related online sources. Some studies used more than one data collection method with online surveys often being used. The studies were carried out in the following countries: United States, United Kingdom, Netherlands, Canada, Norway, Japan, Australia and Spain. Some of the studies covered more than one country, but the most commonly researched countries were United States, United Kingdom and Netherlands. Also, the Spanish study and the other Spanish–Norwegian study examined English-speaking sources.
Most of the data were processed using different types of analytical methods, which produced descriptive information. The qualitative studies were most often analysed using content analysis, but also discourse analysis, text analysis, thematic analysis, social network analysis and video analysis were carried out. The quantitative methods used in analysing data were statistical analysis methods, of which the most popular were Chi-Square, Kruskal–Wallis, Student’s T-test, correlations, logistic regression and ANOVAs.
The health-related online sources were explored from the viewpoint of health science, medicine, psychology, economics and informatics. One of the studies clearly combined two branches of science, while several other studies were less clear on their combinations of scientific fields. The combination of sciences used most often was nursing or medicine combined with informatics.
Consumer-led health-related online sources
Online communities (Figure 1) consist of large, geographically dispersed groups of healthcare consumers who may or may not know each other, but share a common interest. 43 Some of the online communities were distinctive groups only representing one illness, but some of them, such as PatientsLikeMe, included several different forums for several different illnesses.
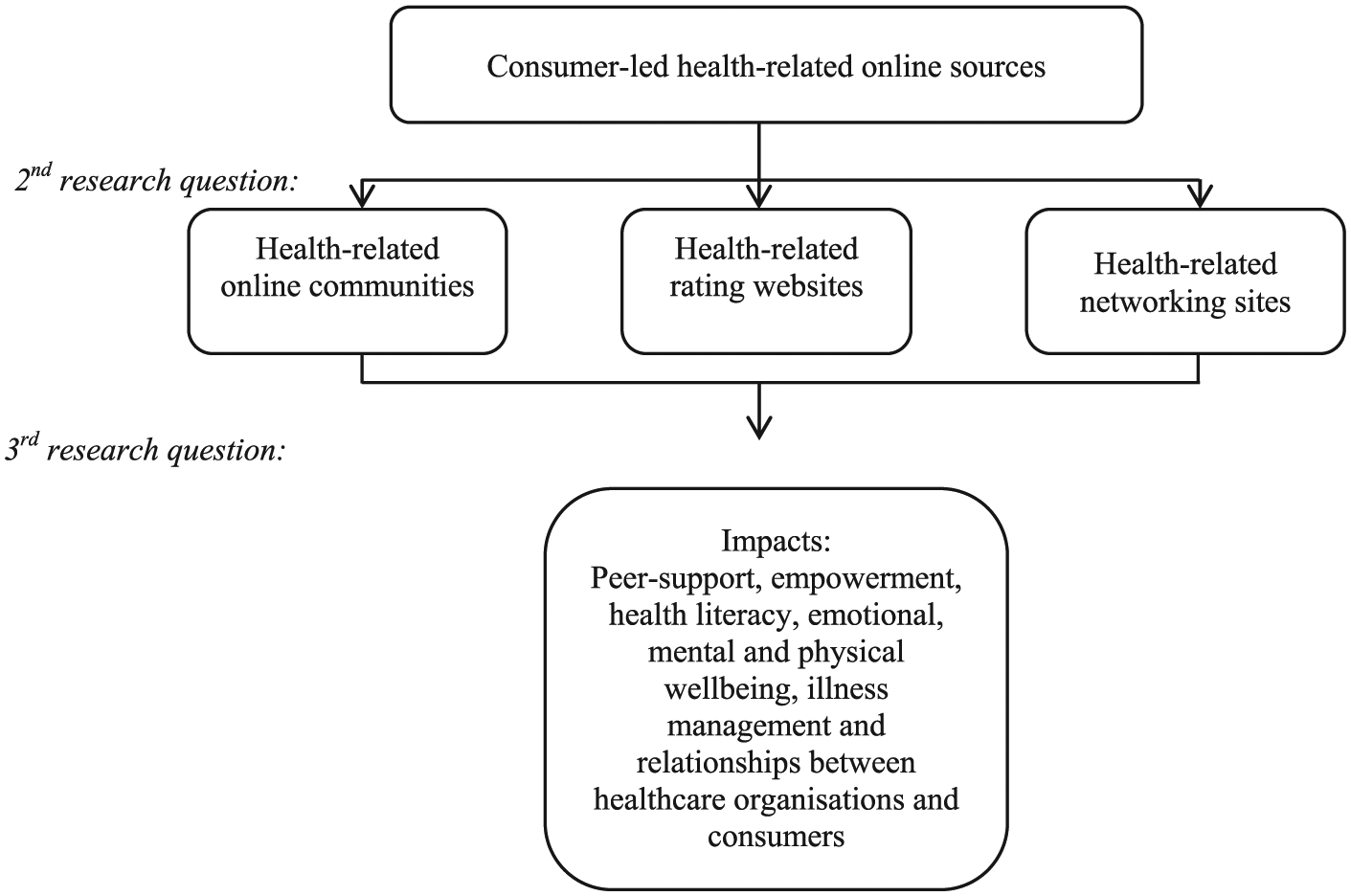
A synthesis figure for research questions 2 and 3.
Health-related online communities were usually used and developed by people with similar health experiences.40,42,43,55 Their purpose was usually to increase knowledge among the healthcare consumers with particular illnesses. 52 The users of the online communities adopted different kinds of roles among the groups: they were either active posters or lurkers 55 and, in some cases, users of the groups became experts (Dolce, 2009). Health-related online communities may contain social networking and rating possibilities. 46
Social networking sites are Internet-based Web 2.0 applications that allow online social networks to be created where individuals are able to share interests and activities. 59 The included studies referenced three different social network sites that included content related to health: Facebook,49,60 Twitter 60 and YouTube. 58 One of the studies did not specify the services used, but did reference MySpace. Health-related social networking sites gave similar types of support as health-related online communities58,60 but they also included several disjunctive features. Social networking sites are different from the other online communities, since they allow the users to be made visible to their social networks. 60 Shoebotham and Coulson 49 noted that compared to health-related online communities, consumers expressed more concerns over privacy when using social networking sites. Social networking sites do not allow anonymous profiles unlike health-related online communities. While communities are most often targeted at healthcare consumers with specific illnesses, health-related social networking sites also involve the mainstream population for purposes such as raising illness awareness, 58 fundraising, advancing disease prevention or fighting against the diseases. 60
Healthcare rating websites offer a consumer the chance to rate their medical providers. 57 They presented a different kind of viewpoint in comparison to the health-related online communities and social networking sites. On the rating websites, healthcare consumers did not share information about their illness but they evaluated the functionality of the healthcare organisations or physicians.56,57 On these sites, healthcare consumers reported their experiences of institutions, professionals, medication or treatments and could be asked to rate different aspects of the care, such as communication, hygiene or accessibility. 56
The impact of the health-related online sources
All three of the consumer-led health-related online sources mentioned earlier aspire to increase the level of health-related information.53,56,58 Some of them evaluate illness-related information, while others may evaluate the information related to healthcare providers or professionals. They all have an impact on the person with the specific illness as well as society and healthcare in general, but they have different types of users and different ways of disseminating information.57,60 The primary impacts seen in studies exploring health-related online sources are peer support; empowerment; health literacy; physical, mental and emotional wellbeing; illness management; and relationship between healthcare organisations and consumers.
In most of the cases, health-related online sources enabled peer support. Seeking a connection with others with the same medical condition is one coping strategy, with the resulting process being termed ‘peer support’. 42 Healthcare consumers were able to find another person with similar symptoms through online sources. This made it possible to make new friends and share experiences, thus helping consumers to understand what it was like to have specific treatments for their condition.49–51,53,59 Sharing stories related to their illnesses made some consumers realise that other users of the online sources were in a worse situation than they were, which made some of them feel positive about their own situation. 47 In some cases, online sources were not merely used for the purpose of peer support but also for deeper companionship. 44 Sometimes consumers took on the role of helper or adviser to others since they felt they had a lot of experience to share.41,46,49 Several studies showed that health-related online sources created a strong feeling of belonging even becoming family-like, which again had positive impacts on emotional and physical wellbeing.49,51 Zhao et al. 51 noted that when consumers strongly identify with their health-related online source, they are more willing to co-create value with peers through sharing. Although peer support was most often seen as a positive impactor, Shoebotham and Coulson 49 noted that a small part of the consumers found arguments and preoccupation had negative impacts.
Empowerment is still poorly defined within literature, 61 but according to some views, an empowered healthcare consumer has been seen as a part of a more productive relationship with their healthcare professional. 62 According to this review, empowerment included different kinds of features, which were usually combined with the fact that the consumer is better informed about the disease.37,46,50,54 Being better informed enabled, for example, better knowledge of treatments, and the health-related online sources better prepared a consumer for consultations since they knew what questions to ask and felt more informed about the symptoms.37,49,52 In addition, empowered consumers were able to question, persuade and even coerce healthcare professionals.41,63 Furthermore, they even took on roles similar to those of health educators and government agencies responsible for public health. 56
According to Gómez-Zúñiga et al., 58 health-related online sources were created because of a lack of information and, thus, one of their goals was to increase health literacy. Health literacy embodies the cognitive and social skills that determine the motivation and ability of individuals to gain access to, understand and use information in ways that advance and maintain good health. 35 According to Kordzadeh et al., 45 the primary goal of healthcare consumers is to seek health-related information, rather than socialising with peers. It was shown that health-related online sources made it possible to learn more about diagnoses, illnesses and treatments.48,52,59 Healthcare consumers learned about the latest treatments and were able to access the best available research through health-related online sources (Dolce, 2009). Many healthcare consumers commented that they were able to find information that had not been provided by medical professionals.41,49 Some of the healthcare consumers turned to online sources since they did not know where else they could get information. 47 These sources also developed the expertise of consumers, since, in some cases, users of the health-related online sources took the role of mentors or ‘patient experts’.40,46,58 The consumers said that even the healthcare professionals reported the growing level of expertise among consumers and noted that they were reaching higher levels of expertise than the professionals themselves (Dolce, 2009). Health-related online sources were also a way of sharing health literacy among other people.46,58,60
Health-related online sources had an impact on physical, mental and emotional wellbeing (e.g. Dolce, 2009).44,48,52 Studies showed that being a member of a health-related online source may cause a reduction in behaviour that is harmful to their illness.52,59 For example, membership of a particular health-related online support group decreased HIV patients’ risky behaviour and helped them decide to start taking antiretroviral drugs. 52 Online sources might also reduce the feeling of loneliness, help accept the condition and, through narration, impact positively on mental wellbeing.47,49 According to Setoyama et al., 55 who researched active posters and lurkers in Japanese online groups, a poster who received emotional support in online communities felt less anxious. Lurkers also experienced positive effects on their mental health. Also Batenburg and Das 39 noted that participating frequently online was especially helpful for healthcare consumers who approach their emotions less actively. In addition, the relationship between online sources and wellbeing might be influenced by individual differences in coping styles. 38 In one case, health-related online support groups were even seen as ‘life-saving’ during cancer survival (Dolce, 2009). Takahashi et al. 59 noticed that negative and egocentric comments were seen mostly as a psychological issue that might be bad for emotional or physical wellbeing.49,58,59 Finally, Gómez-Zúñiga et al. 58 reported that those persons sharing health-related information on YouTube noted that loss of their privacy was a negative impact on their wellbeing, while the people behind the health-related online sources became targets of unwanted marketing.
Most of the consumers using health-related online sources agreed that the sites improved their ability to manage their own or their relative’s illness, that is, cope with problems in their lives.47,48,52,58 Consumers also reported that meeting other consumers made them feel less self-conscious about their condition, that the online source made them feel more in control of their condition and, finally, that the online source enhanced their quality of life.49,53 Health-related online sources enabled more effective illness-related decision-making, since the majority of healthcare consumers found that online information had a significant influence on their decision-making. 57 In some cases, patients managed their illness themselves having self-diagnosed it (Dolce, 2009) or asking for help with the medicines from other healthcare consumers instead of healthcare professionals. 50
In some studies, health-related online sources seemed to have an impact on the relationship between a healthcare organisation and its consumers (e.g. Dolce, 2009).46,56 Health-related online sources have been seen as a consumer’s opportunity to make healthcare organisation or public health more transparent. One of the main purposes of rating websites is to increase the transparency of a healthcare organisation’s policies and practices, making it respond to publicly broadcast concerns and complaints. 56 Dissatisfaction with healthcare providers may be one reason to start using health-related online sources. 48 Also, stories about diagnostic failures are shared on health-related online sources (Dolce, 2009) and, in some cases, discussions on those sites has brought about a change of doctor,52,53 or a demand to see another specialist. 53 Although some healthcare consumers are unhappy with their healthcare professional, many studies found that health-related online sources may also provide a better relationship between caregivers and healthcare consumers.53,56 According to Wicks et al., 53 healthcare consumers reported receiving better care from healthcare professional after starting to use health-related online sources. On the other hand, Rupert et al. 48 found cases where healthcare providers reacted negatively when the consumer mentioned online source usage. Finally, using the sources has a developmental impact on healthcare since it may make healthcare consumers more capable of evaluating the medical expertise and professional capabilities of a healthcare professional and, additionally, it may improve the quality of the care they receive. 56
Discussion and conclusion
The aim of this research was to describe consumer-led health-related online sources and their impact on consumers. The number of scientific articles over the last 5 years describing research into health-related online sources has been rapidly increasing. At the same time, the impacts of online health sources on their users have also been explored, but there is a need to explore this area more effectively and deeper.
The main research approach used in the articles explored was qualitative. The predominant use of qualitative research could be because the phenomenon of health-related online sources is relatively new and qualitative research is flexible, capable of adjusting to new information. 64 In addition, there may only be a little quantitative data from the field, since there may be a lack of suitable standard measures and interpreting the data using those measures might be challenging. Identifying the data collection method was found to be complicated for some studies, as they did not strictly obey the basic rules of any of the data collection methods because the data were derived from the Internet. It should be noted that, as a research environment, the Internet can be considered a new type.
When undertaking Internet research, the use of complementary data analysing methods might be useful. Since it has been argued that online sources are a way for a consumer to voice their opinions, 54 using analysis methods such as discourse or text analysis might offer significant results. Using these methods might be especially useful for research into rating websites or communities, which possibly include a great deal of data encapsulated in colourful speech, complex writing styles and interwoven contexts. Also, newer methods such as networking analysis and video analysis should be used more. One observation was that researching the combination of the Internet and healthcare is multidisciplinary. It may even be that a new branch of science, which combines informatics and healthcare, is about to be born.
As Setoyama et al. 55 and this review noted, research involving non-English speaking countries is limited. In this review, most of the studies explored countries where English was the primary language. The studies from English-speaking countries were most likely found because of the English language inclusion criteria. On the other hand, it should be noted that English-speaking sources may also include consumers from non-English speaking countries. 52
In this review, three different kinds of health-related online sources were investigated as determined by the content analysis: health-related online communities, health-related rating websites and health-related social networking sites. These types of online sources were identified in research by Ziebland and Wyke, 4 who categorised some of the well-known health-related online sources. In addition, they found general health information sites and blogs, which were not found in this review. The lack of health information sites might be explained by the year range used by this study since, as a phenomenon, these kinds of sites are not new and are thus already a lot researched. While searching data, some articles described traditional health information sites, but they were not included since they did not include information of these sites’ impacts. Thus, it can be asked, are the impacts of health information sites investigated enough? Usually, they were only explored from the viewpoint of secure and trustworthy information content. The lack of blogs and healthcare applications was surprising. There are plenty of blogs related to health 4 but the information retrieval did not include any articles that had researched just blogs and their impacts. Are blogs actually investigated or are they such a new phenomenon that they are still not found in searches? Unlike this review, Ziebland and Wyke 4 categorised PatientsLikeMe as a consumer review/reputation site, whereas this review saw it used more as a illness-related community, unlike the rating websites which included little or no illness information. It should also be noted that there are many different names for the different sources so, for example, online communities may also be called forums or groups. Therefore, there needs to be standard terms applied to health-related online sources.
The primary impacts found in the studies exploring consumer-led health-related online sources, as noted in this review, are empowerment; health literacy; physical, mental and emotional wellbeing; relationship between healthcare organisations and consumers; illness management; and peer support. The studies carried out by Ziebland and Wyke 4 and Barak et al. 65 supported the impacts found. As Ziebland and Wyke 4 found, so this study also found both negative and positive impacts. The negative impacts were that consumers felt that health-related online sources may create psychological issues through negative and egocentric comments and, in addition, they inflicted a loss of privacy. It is important to note that losing privacy occurs only in those cases where the consumer agrees to publish information under his or her own name. Usually, privacy site will offer the chance for a consumer to remain anonymous.4,47
Healthcare organisations need to also take information related to negative impacts into account when developing services related to online sources. However, negative impacts have been little researched in comparison to positive ones, 66 possibly because previous studies only focused on positive impacts. However, the absence of evidence for negative impacts does not mean they do not exist. Thus, exploring the negative impacts is also important, especially in cases where they might cause great harm or risks to the health of the healthcare consumer or to others. 66 Also, those impacts seen in a positive light might have a hidden dark side. Healthcare professionals are concerned that health-related online sources might become too trusted. 5 They believe that Internet information can often lead to consumers’ becoming confused, distressed or misinformed and result in harmful self-diagnosis or self-treatment. 67 Is it safe for non-healthcare educated consumers, who have comprehensive access to all health literature provided on the Internet, to start diagnosing themselves or others? 68 Earlier studies have a disagreement over whether the healthcare consumers inform the healthcare professionals about the information picked from the Internet. The studies in this review showed that the use of online sources improved the relationship between the consumer and the healthcare professional.46,52,56 However, some studies found that consumers preferred to hide Internet-based information from their healthcare professionals.5,20
In contrast to this review, Bartlett and Coulson 37 saw empowerment as a hyponym, causing further impacts such as health literacy and peer support. This review did not find that, but it is notable that empowerment was the most common emergent impact in the included studies46,49,50 and it was often used in a context which implied that other things were caused by it. Thus, it can be questioned whether the empowerment is, as Bartlett and Coulson 37 predicted, a major impact of health-related online sources that enables the other impacts or, as Bartlett and Coulson 37 called, ‘empowerment outcomes’. On the other hand, Johnston et al., 43 whose main interest was empowerment as well, considered empowerment as a consequence of social support (cf. peer support). What is the relationship between impacts? Are some of them major impacts causing minor impacts?
Given that health-related online sources, in most cases, made healthcare consumers more competent actors and more aware of health issues, these sources may reduce consumers’ drifting among the healthcare services. If almost 70 per cent of Scandinavians use the Internet to improve or maintain their health3,22,23), should also healthcare professionals, administrators and policymakers take advantage of this development? Healthcare consumers share their experience-based knowledge across the sources, in the process becoming experts or consultants whose knowledge might even be better than that of the healthcare professionals (Dolce, 2009). At present, the information exchange occurs between healthcare consumers and consumer-led health-related online sources. The recommendation based on the results of this review is that healthcare organisations should become a part of this behaviour by providing health-related online sources as a part of their corporate strategy. By doing this, healthcare organisations can become a part of this bidirectional information exchange, in which an organisation provides care for its consumers through trustworthy and safe information. According to Vennik et al., 69 some healthcare consumers felt that the risk of getting untrustworthy information from the Internet could be reduced by getting the healthcare provider to participate in the conversation. In return, the organisation would receive valuable experience-based information from the consumers and possibly save resources. This is similar to the strategy of the site PatientsLikeMe – which is not only used inter alia for patient communication but also for providing data about the real-world nature of disease to help researchers, pharmaceutical companies, regulators, providers and non-profit organisations develop more effective products and care. 70 Finally, the Internet, with its health-related online sources and ubiquitous nature, could offer a cost-effective base for low-threshold services by providing anonymity and 24 h-a-day access.
As a whole, the use of online sources satisfied healthcare consumers’ needs for a sense of community and emotional support,49,51 as well as in terms of peer support.47,50 Healthcare organisations could use this information when developing services in times of scarcer resources towards providing more effective healthcare services. Studies show that this is also what patients would like. This kind of development work is even more justified when the information available via online sources is of low quality, 16 in the situation when consumers primarily search for deeper information via online resources. 48 This kind of development would challenge the traditional way of working in healthcare 41 and shift the usual relationship between patient and professionals into more of a partnership. 46 So the big question is, are healthcare organisations and professionals ready for this size of change in their activities?
Our conclusions are as follows:
The predominant use of qualitative methods might be explained as the phenomenon of online sources is a relatively new one and the need for greater information is required. Also, research into consumer-led health-related online sources is largely limited to the English-speaking population. It could be essential to develop standard measurements when obtaining quantitative data from online sources. These measures could be developed in a way that takes account of the differences (e.g. culture, age or illness) between consumers.
The knowledge of the existence of the sources provides healthcare organisations with an opportunity to listen to their consumers’ ‘voice’. More research from the field of consumer-led health-related online sources is required, with it being important to define them and actively note new ones.
Healthcare consumers, as the users of consumer-led health-related online sources, are more competent and connected actors in regards to healthcare, even becoming experts who are capable of managing their illness. Their knowledge is a valuable resource for healthcare providers and policymakers that could be used more to develop better care.
Consumer-led health-related online sources have several positive impacts that might reduce the need for drifting among healthcare services and might save healthcare organisations’ resources, should such companies incorporate these sites into their own corporate strategy. By doing this, an organisation could create a bidirectional channel with healthcare consumers, along which the healthcare organisation itself could transfer care and trustworthy information to its consumers. In return, consumers would offer their experience-based knowledge to the organisation. The Internet might be useful in producing low-threshold services. The Internet could provide the solution to many of the current problems with healthcare.
For future studies, the following subjects would be of interest to research: more detailed information about health-related online sources and their positive and negative impacts, the organisational viewpoint of online sources, and the use of health-related online sources among the non-English speaking population. In the future, research should analyse data collected from the Internet more effectively.
Limitations
An integrative literature review has the following limitations. As is the case with most literature reviews, there remains the possibility that some relevant articles may have been overlooked, particularly if studies did not mention specific online sources. Additionally, choosing the correct search terms for the retrieval of information may have been unsuccessful and using electronic databases may have introduced errors because of differences between different databases. Only peer-reviewed studies were included and thus relevant studies classified as grey literature might have been excluded. Finally, the researcher’s lack of fluency in certain languages may have resulted in the exclusion of potential studies (n = 32). Undertaking a literature review does not raise any ethical questions, since it analyses previously completed research and no participants in that research are ever contacted. 71
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.