
Abstract
Automated external defibrillators are pervasive computing devices designed for the treatment and management of acute sudden cardiac arrest. This study aims to explain users’ actual use behavior in teams formed by different professions taken after a short time span of interaction with automated external defibrillator. Before the intervention, all the participants were certified with the American Heart Association Basic Life Support for healthcare providers. A statistically significant difference was revealed in mean individual automated external defibrillator technical skills between uniprofessional and interprofessional groups. The technical automated external defibrillator team scores were greater for groups with interprofessional than for those with uniprofessional education. The nontechnical automated external defibrillator skills of interprofessional and uniprofessional teams revealed differences in advantage of interprofessional teams. Students positively accept automated external defibrillators if well-defined and validated training opportunities to use them expertly are available. Uniprofessional teams were successfully supported by their members and, thereby, used automated external defibrillator effectively. Furthermore, the interprofessional approach resulted in as much effective teamwork as the uniprofessional approach.
Keywords
Introduction
In order to reduce costs and increase safety, quality, and sustainability, healthcare authorities continuously integrate new healthcare technologies into existing systems. The application of pervasive computing technologies to healthcare ensures its availability to all irrespective of place and time. 1 Sometimes, these efforts result in problems in the dissemination and acceptance of technologies, especially where healthcare workers are unable to use the products, devices, or guidelines as designed by the manufacturers. 2 Currently, healthcare providers face different issues when using the numerous new technologies available on the market. Therefore, organizations are currently acting to incorporate these technologies into the daily routines of users, provide necessary support and facilitation for integration, and create necessary time and training opportunities.
Healthcare can be defined as a collaborative patient-centered practice. In order to play an active role in ensuring patient care and making associated decisions, healthcare providers must communicate with each other and organize themselves; they must respect each other’s contributions, as well.3,4 The existing literature strongly suggests that interprofessional learning associated with interprofessional work is effective.5,6 Interprofessional education (IPE) is an effective teaching method that develops effective collaboration among healthcare practitioners. 5 It proposes to educate healthcare providers from different professions together in a supportive environment so that they gain necessary skills to practice together throughout their careers. As concepts like patient safety and rights became prominent, 7 it became difficult to perform learning activities in real environments. Current approaches to the professional competence development of students emphasize controlled experiences of rare and risky situations, learning from mistakes, reflection, and multiple sets of feedback. Using simulation techniques, it is possible to build lifelike, supervised, and safe environments that allow learners to develop significant learning experiences and educators to evaluate the quality and competency of learning outcomes.8,9
Sudden cardiac arrest (SCA) is a worldwide public health problem that may result in death in the absence of timely and correct intervention. For the survival of SCA cases, early defibrillation and effective chest compression are critical. 10 Research shows that unless caregivers are ready, willing, and motivated, they will not start an initial intervention for a patient having a cardiac arrest. 11 Although the individual resuscitation attempts of healthcare providers are vital for the patient, multiple providers working in concert, sharing tasks and acting simultaneously, are much more useful. Automated external defibrillators (AEDs) sense cardiac arrests, give feedback, and provide cardiopulmonary resuscitation (CPR) instructions to the rescuer. The use of AEDs by basic life support (BLS) providers improves the quality of CPR.
The International Liaison Committee on Resuscitation (ILCOR) offers AEDs for SCA treatment and management. 10 This has resulted in the adoption and dissemination of innovative medical technologies in CPR practices. The American Heart Association (AHA) BLS training is a certification program that recognizes the use of AEDs as a basic skill and focuses on the importance of teamwork. Although ILCOR recommends the use of AEDs, they are not widely used in all CPR training programs to date. The use of this new technology in an interprofessional healthcare setting is inevitable; however, studies focusing on the adaptation and integration of this globally used technology are not sufficient. Moreover, direct performance measurements are limited in the social influence studies investigating health professional’s behaviors and intentions; they are mostly based on self-reported data. Current studies reveal that team characteristics and team-directed strategies influence technology acceptance via perceived support from peers or coworkers. This study discusses how social interaction influences a healthcare professional’s decision to use an AED in an emergency.
Background
BLS with AED
BLS is the principal practice followed in treating SCA cases. The adult BLS chain of survival includes early diagnosis of SCA; early access to emergency response systems; early, high-quality CPR; and, if necessary, early defibrillation. An AED is a pervasive computing device 12 designed for the treatment and management of acute SCA. An AED guides its user through the stages of administering CPR, monitors the patient’s heart rate, and diagnoses the condition and administers a shock automatically, if necessary. 13 The AED training device is preferred by educators because it provides monitoring and evaluation of the task and the entire learning process. 14
Technology acceptance and implementation
Introducing users to a new medical technology does not automatically lead to the realization of expected benefits. The main problem with the introduction of innovations is that caregivers do not automatically use them as intended by the developers. 15 Even though many innovations have the potential to improve the quality of healthcare significantly, their implementation can be delayed due to the resistance offered by some caregivers. In order to predict the determinants of caregivers’ adoption and use of new technologies, technology acceptance models (TAMs) were developed. The main assumption of TAMs is that behavioral intention is a valid predictor of actual use. There are four prominent models (TAM1, TAM2, TAM3, and Unified Theory of Acceptance and Use of Technology (UTAUT)) and two frameworks (theoretical and implementation) related to TAMs.
Often, TAM1 is used to explain the acceptance and use of computerized technologies. 16 It has two external variables that determine the attitude toward technology usage (A): the users’ confidence that technology will improve their performance is “the perceived usefulness (U),” and their confidence that using the technology in daily work will demand extra effort is “the ease of use (E).” TAM2 preserves the basic structure of TAM1; however, the attitude toward using the technology is extracted from the model, and predictors of “perceived usefulness” and “intention to use” are detailed under social influence. 17 TAM3 is the advanced version of TAM2. 18 Similar to TAM2, perceived usefulness is the strongest predictor of behavioral intention. Image perception using innovation will enhance users’ status in the social system, and experience is an important moderating variable in the contexts of information technology (IT) adoption. UTAUT formulates the core determinants of performance and effort expectancy, social influence, and facilitating behavioral conditions to use IT. 19
Venkatesh and Bala 18 developed a theoretical framework presenting the determinants of TAM belief structures using the variables produced by all the TAM studies (Figure 1). In this framework, the core model of TAM2 is used; furthermore, in this model, the perceived ease of use directly influences perceived usefulness. Individual differences, system characteristics, and social influence direct and shape the perception of IT. Facilitating conditions represent the organizational support that facilitates the use of an IT. Fleuren et al. 20 developed an implementation framework that explained the relationship and interaction among an innovation’s determinants, strategy, and process.
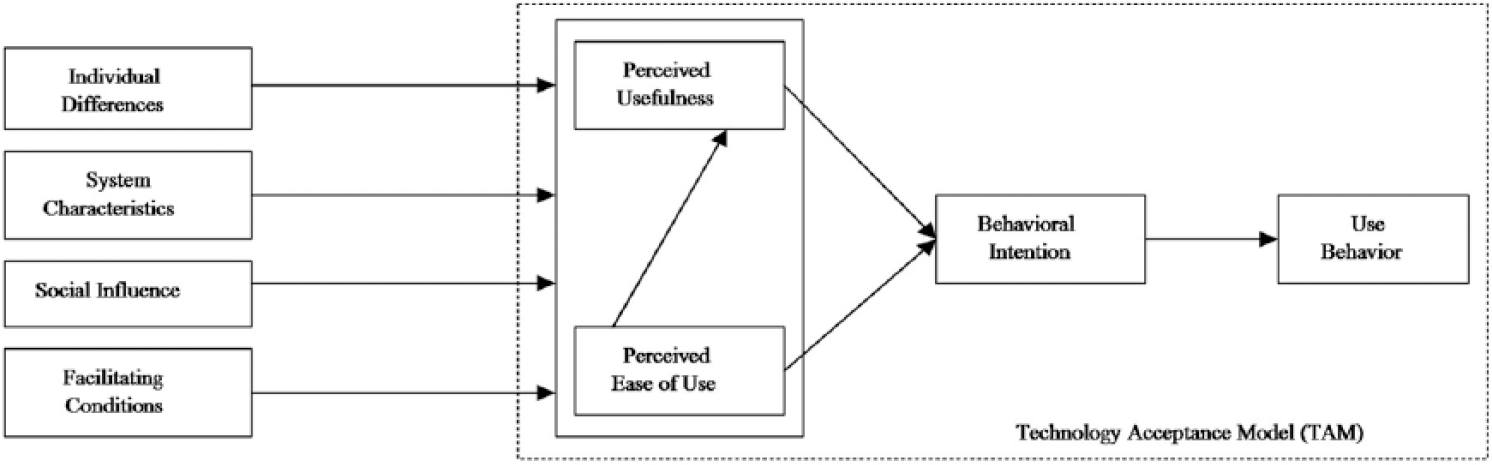
TAM Theoretical framework. 18
The successful introduction of a new technology makes it easier for a user to use and accept it. Effective implementation processes can enhance the adoption and use of IT by employees. 21 This study aims to explain the actual usage behavior of users in teams comprising different professions, which is determined after a short time span of interaction with an AED. Therefore, this study includes both the TAM theoretical 18 and implementation 20 frameworks (Figure 2).
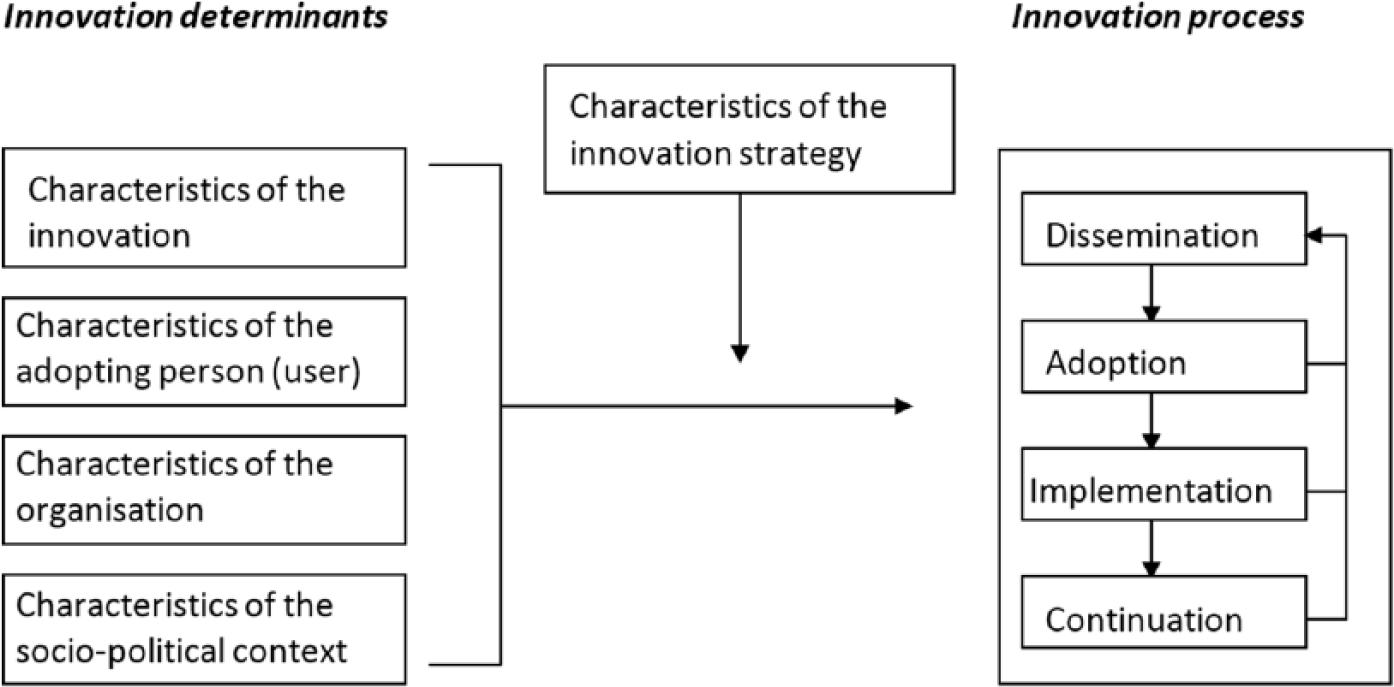
Framework represents the innovation process and related categories of determinants. 20
Methods
The study was designed to investigate how uniprofessional and IPE methods influence the adoption and use of AEDs by students (Figure 3). Recent studies emphasize that innovation processes, strategy, and determinants influence technology acceptance.2,19,20 Therefore, we followed the TAM theoretical framework and developed certification and matching processes to bring the determinants and variables under control, consolidate differences, and ensure that members are equally distributed among the groups.
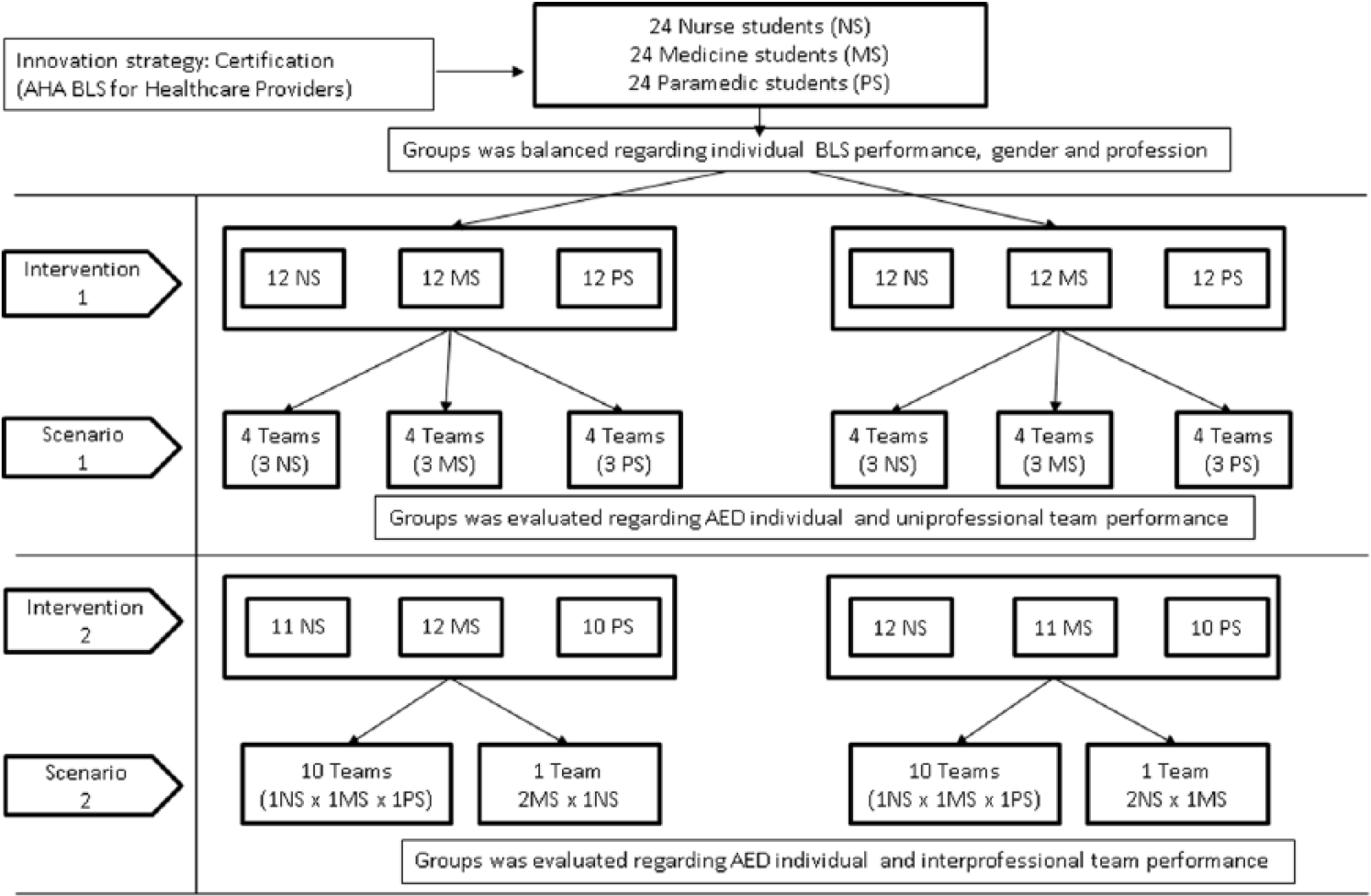
Flowchart for overall research design.
The learning domain BLS and subdomain AED skills existed in the professional competency definitions of all participants. The differences in expertise and experience among the subjects were equalized using the AHA BLS certification. In order to build balanced, distributed groups, individual differences, gender, profession, and knowledge were considered. The purpose of building balanced groups was to equalize the parameters as dynamic influences—except the sociopolitical context and social influence—for both groups and explain the differences using the method. Table 1 shows the innovation determinants, processes, and strategy that are in line with the implementation framework of this study. Students were assigned to the groups based on their CPR knowledge, and individual BLS with AED performance scores were used at the end of the certification stage.
The determinants, process, and strategy of innovation.
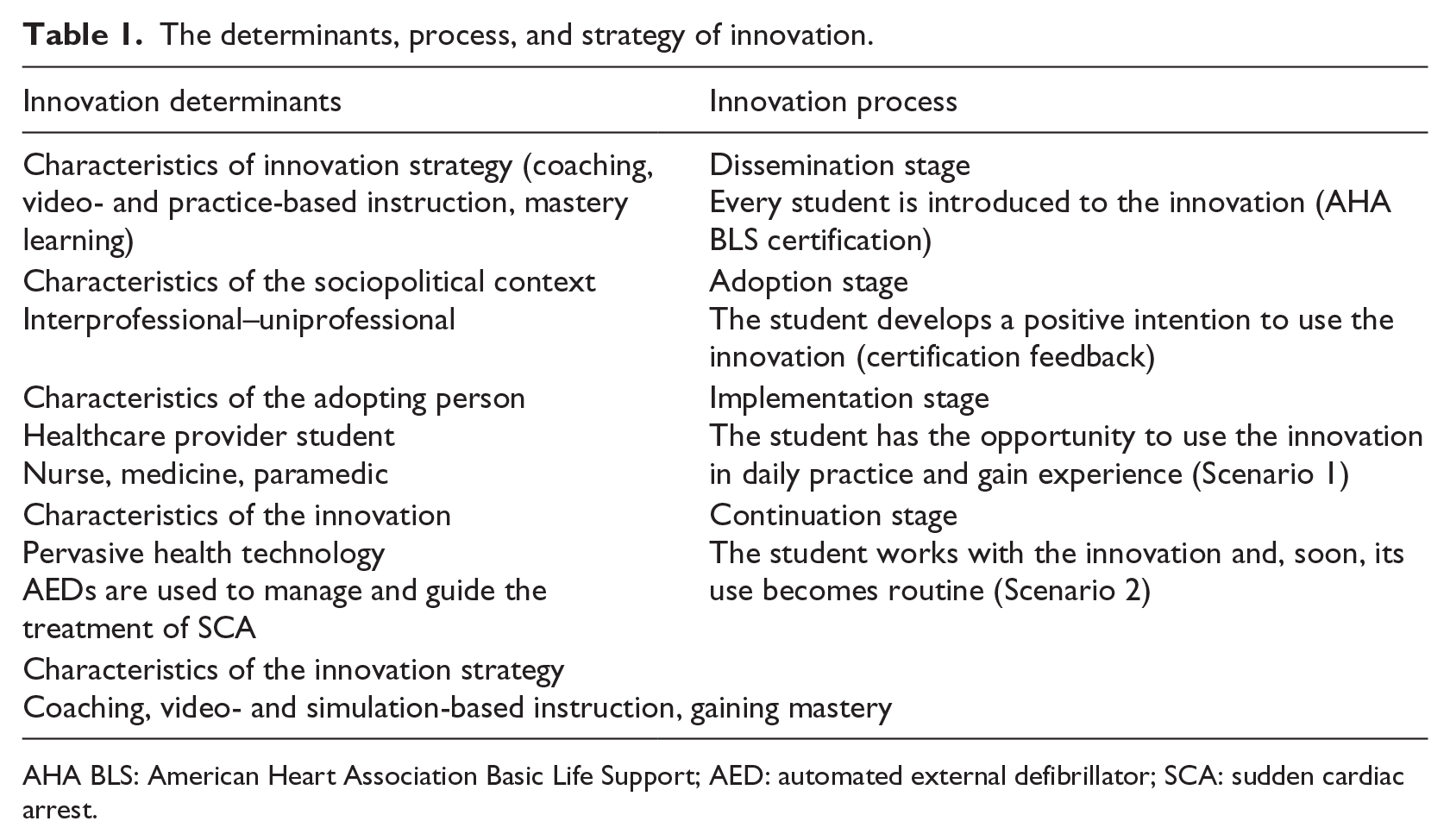
AHA BLS: American Heart Association Basic Life Support; AED: automated external defibrillator; SCA: sudden cardiac arrest.
Participants
In this study, 72 fourth-year medicine, third-year nursing, and second-year first and emergency aid program students from Hacettepe University participated during the 2013–2014 academic year. A free AHA BLS certification was offered to these students. A conformity consent, dated 24 July 2013 was granted by the Non-interventional Clinical Trials Ethics Council of Hacettepe University. Among the participants, male students comprised the minority, and 21 of the nursing, 70 of the medicine, and 14 of the paramedic students were female.
Assessment instruments and devices
Quantitative data were derived from video analyses of CPR performances to examine the changes in individual and team-level technical AED skills, and qualitative data were collected to define the effects of the collaborative practices on nontechnical AED skills.
Technical AED skills form for individual and team evaluation
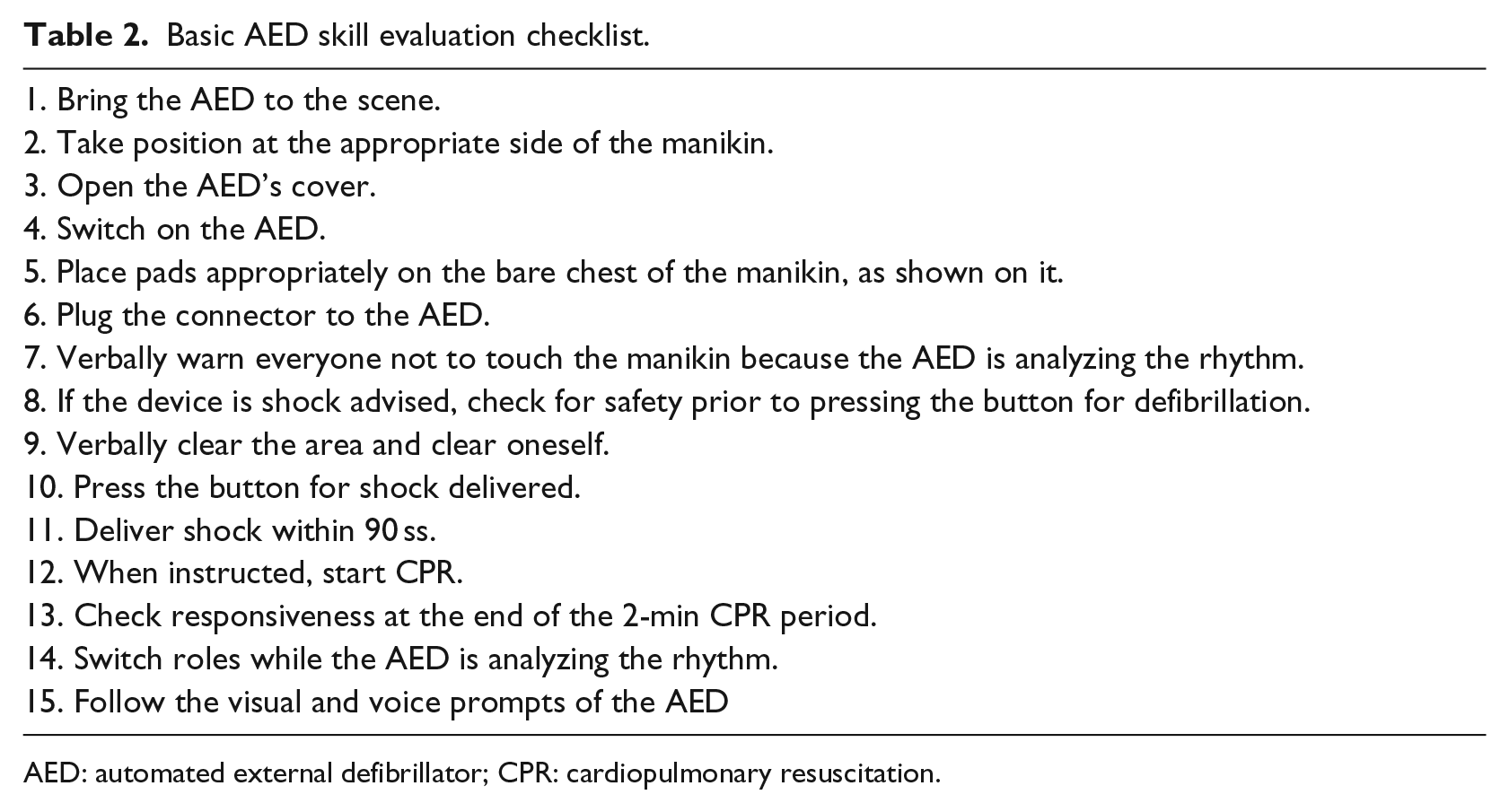
In this study, a technical AED skill evaluation form preserving the basic structure of the AHA BLS with AED skill testing sheet was developed. An evaluation set examining the participants’ general ability to follow AED instructions and manage situations was used to assess their technical AED skills at the endof each scenario. Recorded videos were used for detailed evaluation. Using the technicalAED skill evaluation checklist, a team could score a maximum of 42 points and individualsup to 45 points (Table 2).
Basic AED skill evaluation checklist.
AED: automated external defibrillator; CPR: cardiopulmonary resuscitation.
Nontechnical AED skills form for individual and team evaluation
In this study, a thematic observation form preserving the basic categories of the Team Emergency Assessment Measure (TEAM) 22 was developed for the evaluation of nontechnical AED skills. An evaluation set examining the participants’ abilities such as effective communication, adaptability to changing situations, situation awareness, and supportive behavior was used to assess their technical AED skills at the end of each scenario. We used the Resusci Anne manikin with SkillReporter, manufactured by Laerdal, and Life-Point AED training defibrillator, manufactured by METsis Medikal.
BLS team performance scenarios 1 and 2
In the first performance scenario, a BLS team comprising three students from the same professional group performed BLS for 10 min on the patient in need of support. The second scenario mainly differed from the first one in that the team comprised students from different professional groups.
In this study, each professional group was represented by 24 students. In both scenarios 1 and 2, practice rescue teams comprised three students. The participants formed uniprofessional and interprofessional teams for scenarios 1 and 2, respectively (Figure 4).

Interprofessional BLS team performing CPR with AED.
There were differences in the BLS education programs of the students involved in the study. In order to evaluate the effects of educational intervention impartially, study groups were shaped according to similar BLS competency and professional maturity. Therefore, a 1-day AHA BLS provider training was planned and delivered to enable the students to master BLS skills. Experiment and control groups were built according to the initial CPR knowledge and individual BLS performance assessments and evaluations of students. After each learning intervention, the evaluation of students took place in different scenarios. The study groups were evaluated in terms of individual and team technical and nontechnical AED performances.
Results
BLS with AED performance for the first scenario
The technical AED skills of teams
The median AED performance scores of the experimental and control groups were 38 and 39, respectively. There was no significant statistical effect of the differences in method on the AED performances of the teams comprising participants of the same profession (Mann–Whitney U = 46.500, p = 0.352).
Individual technical AED skills within teams
A two-way analysis of variance (ANOVA) was conducted to examine the effects of profession and method on individual AED performance. The technical AED score averages of the experimental and control groups were
BLS with AED performance for the second scenario
The technical AED skills of teams
The Mann–Whitney test indicated that the technical AED scores were greater for groups with interprofessional (median = 36) than uniprofessional (median = 31) education (U = 12.000, p = 0.001, r = 0.68).
Individual technical AED skills within teams
A two-way ANOVA was conducted to examine the effects of profession and method on individual AED performance. The technical AED score averages of the experimental and control groups were
Evaluation of nontechnical AED skills
The nontechnical AED skills of participants were evaluated using the thematic observation form derived from TEAM. 21 Students did not hesitate to use the AED; furthermore, they did not face any difficulty in demonstrating AED competence in an environment in which their team members were present. It is thought that IPE overcomes the professional differences of team members, which is believed to cause underperformance in teams. With the IPE group, problems recognized by team members are corrected either by the members themselves or through feedback. Team members share respiratory and heartbeat recovery information, and the performer rotates according to the analysis warning of the AED. The situational awareness of interprofessional teams was higher compared to the control group.
Within teams, the team members had to be appropriately assigned specific duties and tasks. This requirement was covered by the IPE teams. They properly assessed airway, breathing,and compression (ABC) when a shock was not recommended. IPE teams shared moresupportive and task-related (touch or not) feedbacks. They gave appropriate warnings to the interprofessional group and voiced feedbacks loudly with much more self-confidence. Furthermore, IPE teams took turns working and relaxing.
Discussion
Uniprofessional design
The differences in individual AED performances of students explained by profession were not significant. Similarly, educational methods did not cause any differences in individual and team AED performance scores. Considering the students’ expertise in using AEDs, pre-BLS certification can be stated as the appropriate strategy for introducing AEDs.2,20
Interprofessional design
The individual AED performance differences of students explained by profession were not significant; however, differences in educational methods resulted in differences in individual and team AED performance scores. The findings of the study indicate that collaborative learning has a positive effect on the IPE group. In this group, the IPE method improved the individual and team AED performance scores of team members, even when they were from different professions. This result is consistent with the findings of Mäkinen et al. They observed that nurses hesitated to use AEDs in emergency situations, even though the previous training and the availability of equipment. 23 In our study, nurses gained confidence to start CPR after the IPE intervention, which made the difference on it. Wilkes et al. 24 stated that specific organizational, cultural, and teamwork factors significantly affected the use of new health technology. They defined the key operational and cultural barriers as lack of trust, poorly defined leadership, and lack of communication policies. Lapkin et al. 25 measured subjective norms of students, which explained how healthcare provider perceived the opinions of other health professionals, patients, and family member in relation to medication safety and collaborative practice. Their results showed that health professional students appeared to place less value on the contribution and perceptions of others regarding medication safety. Their suggestions for the solution were education on role reversal, team-building activities, and feedback mechanisms to share concerns.
According to the research conducted in this field, the sociopolitical context is an important determinant of innovation acceptance and its influence either suppresses or enhances technology usage behaviors.2,19,20 According to Pynoo et al., 21 physicians perceive that their social environment encourages the use of technology; in contrast, Liu et al. 26 report that social influence is not important for therapists’ acceptance of new technologies for rehabilitation if their usage is not mandatory. Furthermore, Casey and Wilson-Evered 27 suggest that trust may mediate the effects of technology acceptance constructs.
Conclusion
Although BLS performed by lone rescuers is effective in the treatment of SCA, patient outputs are much more positive when BLS is carried out by a team. 11 Social influence within the team affects practitioners’ decision regarding the use of AEDs and individual and team AED performances.
It is observed that teams comprising individuals from the same profession tend to communicate positively, give feedback, and behave supportively. The supportive activities performed by team members may help a practitioner in effectively using a new technology. Furthermore, IPE approaches help to remove professional barriers and the perception of competition.
In this study, all participants displayed mastery of AED techniques. It is thought that audio and visual guidance reduces the cognitive load of students in complicated situations. Hence, audio and visual performance support systems can be used in learning environments to strengthen the students’ ability to make sense of their learning and connect with their professional performances.
Individual difference variables such as personality and demographics can influence an individual’s perception of the usefulness of a technology. 19 In this study, female students constitute the majority of participants. Although the groups’ gender distribution was balanced, one should consider this limitation when evaluating the findings.
This study has a pre-implementation value for the acceptance of AED technology in Turkey because the use of AEDs was recognized officially and added as an option to the valid national first aid course in 2016. This study is expected to contribute to the reduction of initial resistance of workers and students to newly introduced technology and help them perceive realistically the features of the technology and understand how the technology can support them in their daily work.
Footnotes
Author's Note
The data in this study were collected as part of a larger dissertation study. 28
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.