
Abstract
Continued development of mobile technology now allows access to information at the point-of-care. This study was conducted to evaluate the use of one such tool on a mobile device, from the carer perspective. Caregivers across 12 aged-care facilities were supplied mobile devices to access a Picture Care Plan (PCP), a specific tool designed around the role of the personal carer. An anonymous questionnaire was subsequently completed by 85 carers with questions relating to participants’ experience. Perceived helpfulness of the PCP at the point-of-care was high (87%). A significant number of participants believed the use of the PCP increased resident safety and quality of care (76%). Practical components related to the carrying of the device, network speed and the requirement to maintain communication with senior members of staff to ascertain updates were also expressed by participants. Findings suggest that staff are receptive to adoption of mobile devices to access care directives at the point-of-care and that the technology is useful.
Introduction
Continued development of mobile technology has seen the integration of mobile devices, software and operating systems into the healthcare sector. Access to information at the point-of-care to increase accuracy and efficiency has been a primary driving factor.1,2 Particularly for the aged-care sector, the pressure to increase efficiency and quality of care in the face of limited resources has led to increased focus on mobile technologies to provide a cost-effective method of providing greater information access regarding resident care needs. 3 Increasing integration and acceptance of mobile device–accessed documentation systems in aged care has the potential to dramatically increase access to resident care directives for not only nurses and allied health professionals but also for personal carers completing routine care tailored to the individual.
Continued development and successful integration of such software and technology is especially poignant considering that current evidence suggests that accessibility of appropriate resident information is still lacking in the aged-care sector. One study reported that only 38.5 per cent of participating staff across four Australian residential aged-care homes (RACH; including managers, registered nurses (RNs), enrolled nurses (ENs) and personal carers (PCs)) always had access to resident information at point-of-care. 4 There is significant potential for mobile devices to dramatically increase this figure. However, several barriers to successful integration exist, including reluctance of staff to use mobile devices at point-of-care due to fear of being alienated from residents, fear of a foreign tool or due to inadequate fit of the operating system to meet work requirements and individual preferences. 1 Adoption of mobile technology across the aged-care sector is variable. 3
In addition to variability in integration of mobile technology and health management software, work intensity for RACH nurses is increasing. Trends indicate that supply projections will not keep pace with predicted demand for future resident placements. Australian data reveal that aged-care nurses are increasingly required to supervise more residents as well as more staff, raising concerns over the continued quality of care provision. 5 The changing landscape of the RACH workforce in Australia has seen increases in PC numbers, with PCs (also termed as assistants in nursing (AINs)) constituting 68 per cent of the RACH workforce in 2012, while RNs and ENs constituted only 15 and 12 per cent, respectively. 6 Specific to addressing concerns over the continued quality and continuity of care is the use of handheld mobile devices to access resident data at point-of-care.
Currently, research has primarily focused on the use of mobile devices by RNs or other medical practitioners; however, day-to-day care of residents in RACHs is primarily provided by PCs. These carers are actively involved in the daily lives of residents with approximately 45 per cent of their time, not including indirect care and preparation, spent directly interacting with residents, completing tasks, such as personal hygiene, toileting, mobility, medication, nutrition, assessment and oral communication. 7 PCs engage with residents, spending an estimated 2 h per shift in oral communication with residents, often concurrently with care activities. 7 Although care has traditionally been seen as task oriented, 8 there has been a greater emphasis on a person-centred approach in recent years. PCs are therefore integral to the personal well-being of residents and are significant to the functioning of aged-care homes. Research must focus not only on health management systems as experienced by RN, ENs and other health practitioners but also on the experience of PCs involved in providing direct care for the resident. The potential of health management systems designed around the role of the PC and integrated into care are yet to be thoroughly explored.
Methods
Sites
A total of 12 RACH, located in Queensland, Australia, operated by the same not-for-profit organisation participated in the study. The large long-standing RACH provider had implemented a new documentation system, yet to be appraised from the PC/AIN perspective.
Documentation system
Leecare Solutions, Leecare Platinum 5.0 Care, Lifestyle, and Management software had been initiated at each of the sites over a 2-year period. Go live dates ranged from 2 December 2013 to 15 June 2015 earning the participating RACH provider the 2015 Best Implementation of the year ITAC (Information Technology in Aged Care) award for organisations with a budget of over $30 million per year. The Leecare software utilised was developed specially to meet the needs of the Aged an Community Care industry, with access to resident information at point-of-care of particular focus, ‘… specifically engineered for advanced touch screen interface devices such as Apple and Android tablets, this solution provides users with an application that is completely device and location independent’. 9 The primary aim of the software was to provide efficient access for healthcare professionals, PCs and other relevant aged-care workers to accurate resident information within a simple and easy-to-use interface. The software allows users to navigate within the programme within two clicks or two touches, in the case of mobile devices, and was designed to be adaptable to specific organisational needs. The Leecare software implemented at the participating sites continues to undergo development alongside the organization’s own clinical support team in consultation with facility managers and aged-care employees.
Included in the programme is the application, a Picture Care Plan (PCP), developed specifically to aid carers to complete daily-care activities required by the individual resident. The tool aims to provide clear summarised information, accompanied by relevant illustrations, to be accessed immediately prior to providing care or at the bedside. Sections are broken into safety, movement in bed, transfers, mobility, hygiene, toileting, meals/drinks, skin care, oral/dental, communication and pain management, as well as a brief life history. Text is limited to provide only care directives. Pictures typically represent aids/tools necessary for the care of the resident and are included as appropriate in each section. Examples of typical images include the following: support, transfer and mobility aids, hygiene, skin care and incontinence products, hearing aids/glasses, chairs, beds and commodes, which are to be used for that individual resident. PCP is accessed on Samsung Galaxy Tab 3 7.0″ provided by the organisation for PCs/AINs to utilise as part of their normal work practices. Tablet dimensions are as follows: 188 × 111.1 × 9.9 mm3 and weight: 306 g. For example screenshots of the PCP displayed on the device, please refer Figures 1 to 4. Please note these examples are for a fictional resident.
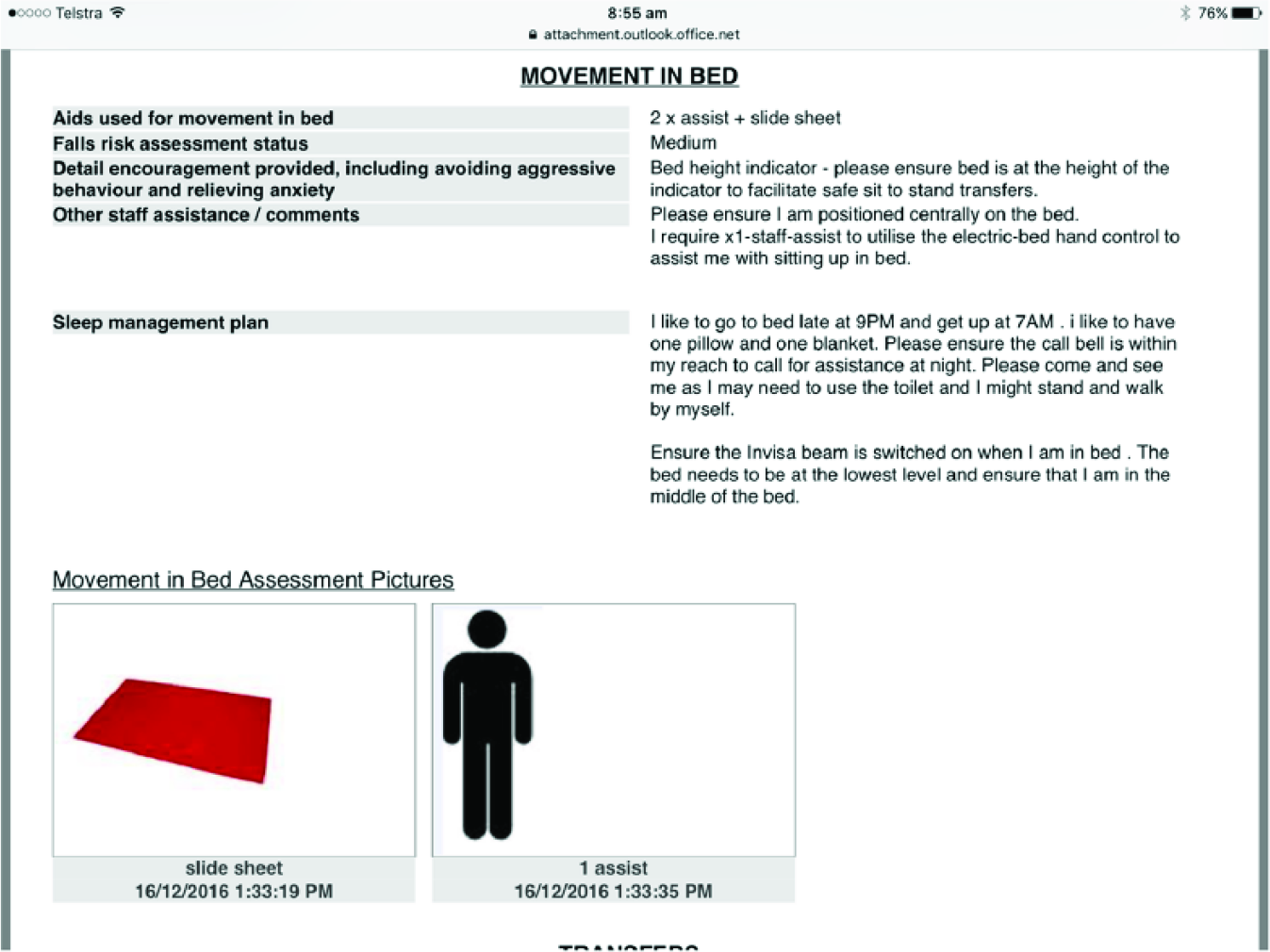
PCP screenshot: movement in Bed.
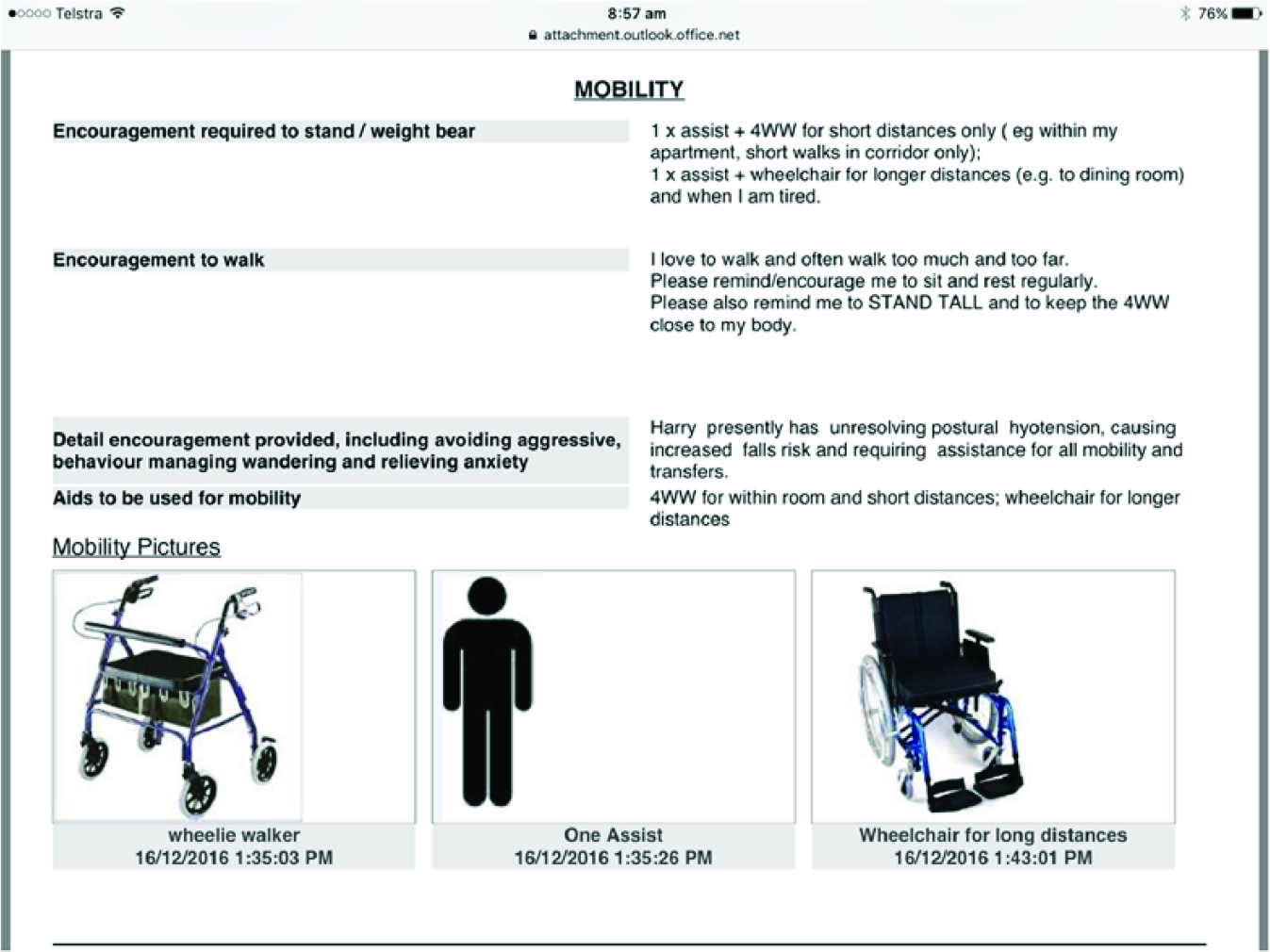
PCP screenshot: mobility.
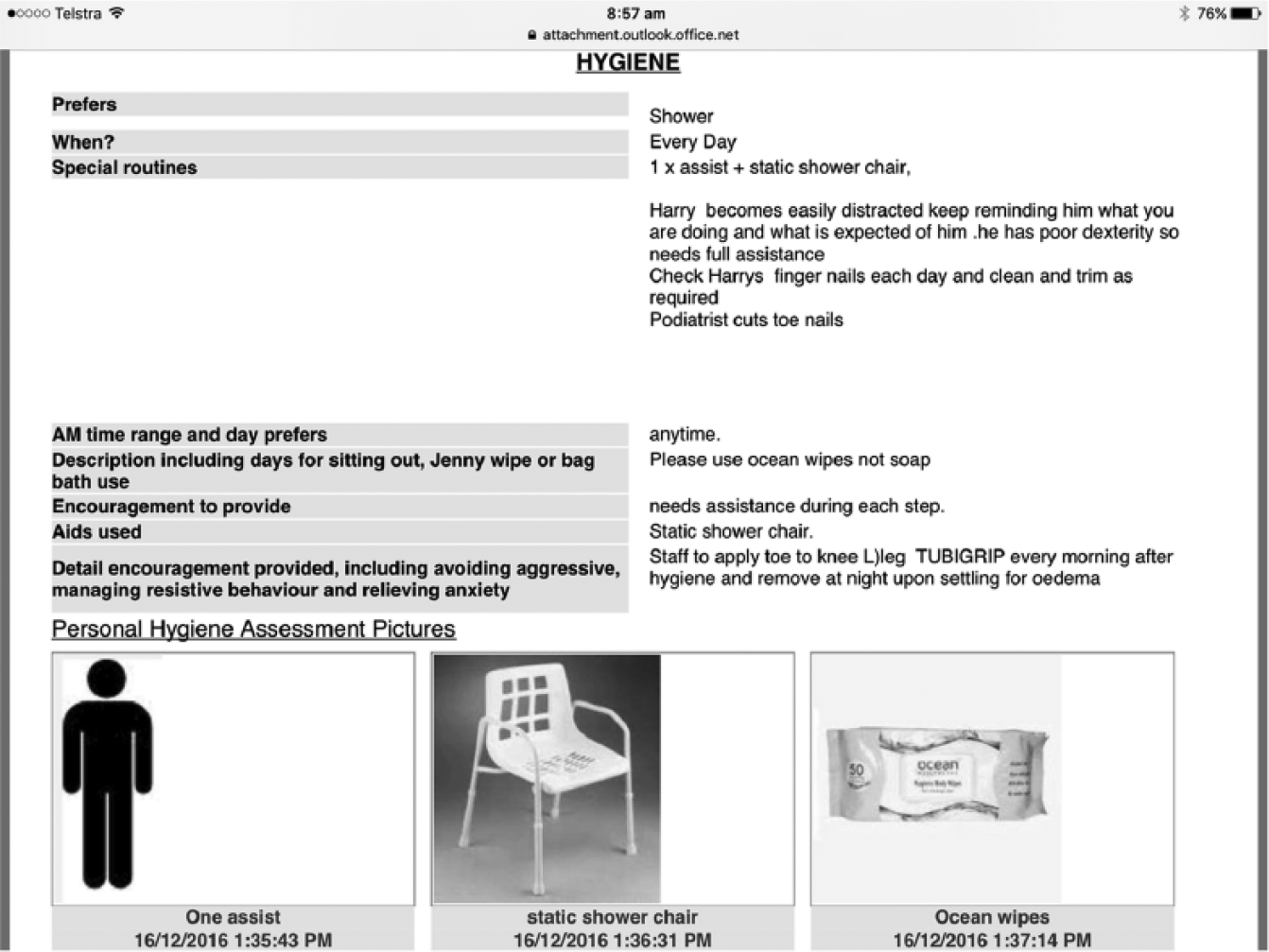
PCP screenshot: hygiene.
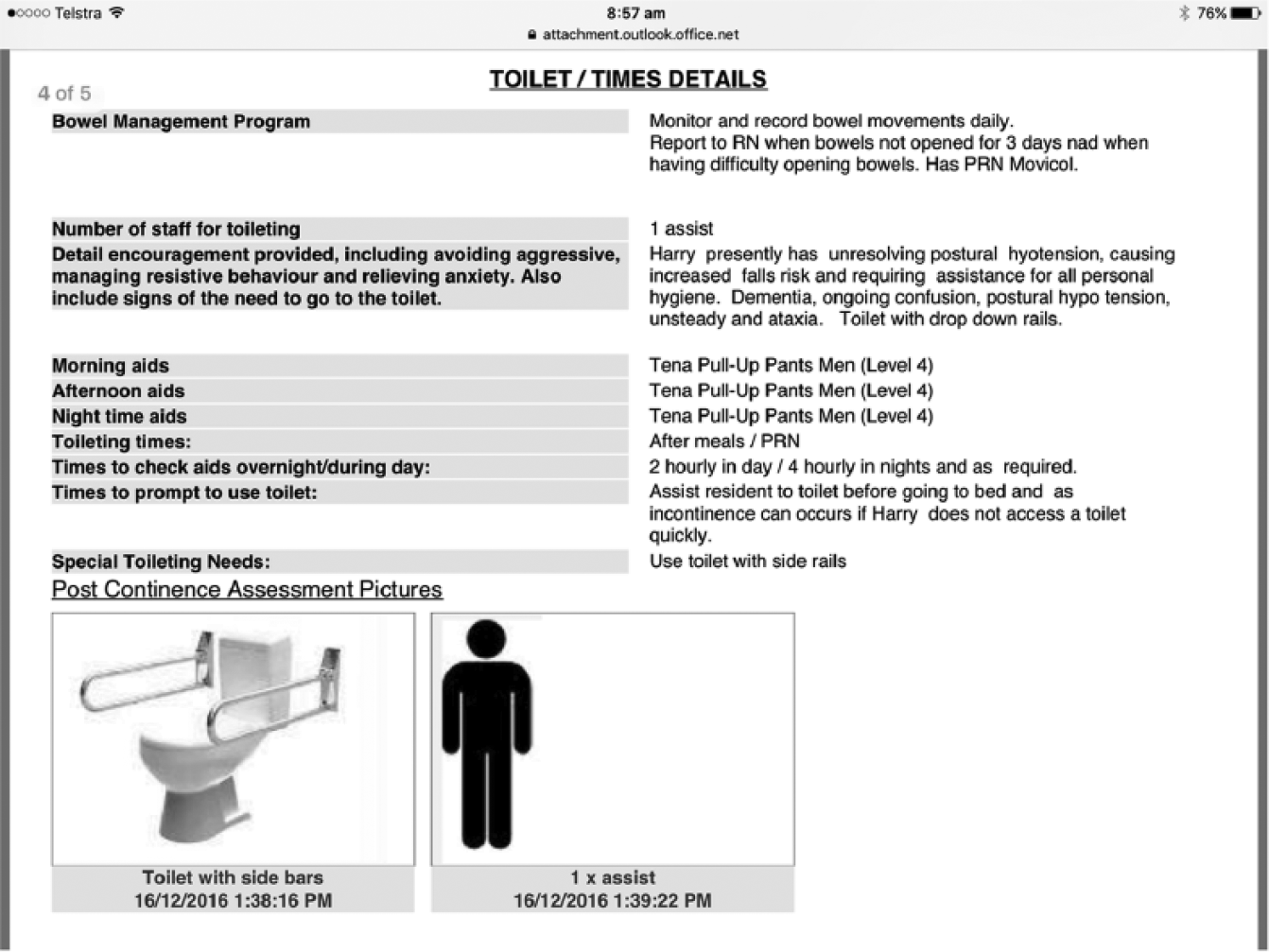
PCP screenshot: toiletting.
Participants and process
A total of 85 PCs/AINs were recruited across the 12 sites constituting an overall participation rate of 14.4 per cent (n = 589). Study design targeted specifically day-shift workers, bringing the participation rate of relevant workers to 24.1 per cent (n = 353). Research indicates that response rate for aged-care workers in Australia is approximately 39.8–44 per cent completing similar studies;10,11 however, research has also shown that AINs are less likely to respond to surveys than RNs or ENs in aged care. 4 Very few studies have targeted or included PCs. Participation was anonymous. As part of the rollout of Leecare across the homes, all PCs/AINs received 3 h in-house training on the use of Leecare as relevant to their role. These employees then received 1 week of onsite support during rollout of the software. Staff who started after the rollout received the same training and were then supported by colleagues on site. PCs/AINs were expected to carry the dedicated mobile devices (tablets) supplied by each site for the purposes of carrying out work-related duties. Specifically, PCs/AINs were expected to carry and use the mobile device to access the PCP application located in Leecare Platinum v5.0, which displayed concise, summarised data specific to the care of each resident.
Questionnaire
The questionnaire developed for this study was based specifically on the needs of the organisation. Questions were designed and selected based on pre-existing research,12,13 current knowledge of organisational structure and software implementation of participatory sites. The questionnaire included demographic characteristics and questions relating to participants’ own experience of mobile device use, specifically including the use of the PCP, that had been recently implemented across all homes (Supplementary Material 1). Questions relating to the current use of mobile devices and the PCP as part of normal working practices consisted of a five-point Likert response, ranging from never to always and were developed to measure usefulness, time-saving ability, training, ease of use and information content of both the mobile device and PCP, at a level appropriate for the English literacy of PCs. These factors have been shown to be useful when assessing feedback from nurses and nursing students. 10 Three questions relating to participant’s own reflections on the use of a PCP to increase resident safety, quality of care and staff confidence were included with a five-point Likert response, ranging from strongly disagree to strongly agree, adapted from Johansson et al.12,13 Qualitative questions were also included to provide an opportunity for the staff participants to provide rich insightful data to compliment the quantitative feedback addressing their suggestions for possible improvements and limitations of mobile device use and the associated tool. Nearly, one-third of PCs/AINs came from non-English speaking backgrounds, according to human resources. Challenges around English language literacy were limited by keeping the wording of the survey questions to an appropriate level and by conducting the surveys using an interview style: reading the questions aloud for participants, while providing a written copy for them to read through, and transcribing their responses verbatim.
Data analysis
Descriptive statistics (frequencies and mode) were applied and data analysis was conducted using SPSS v 22. Examples of quotations received in response to qualitative questions were used to complement and highlight the results and are presented in text.
Ethics
Ethical approval was received by the UnitingCare Queensland Human Research Ethics Committee in conjunction with approval from the organisation’s own Research Awareness Group.
Results
As seen in Table 1, participants (n = 85) typically consisted of female PCs/AINs aged between 25 and 64 years, with a peak in workplace constituents between 35 and 54 years (55%). Of the participant cohort, 89 per cent held a certificate III in Aged Care or higher in line with current industry practice 6 and 86 per cent reported home use of mobile technology. (Note: Graduates at the Certificate III level have theoretical and practical knowledge and skills for work and/or further learning, which is roughly equivalent to a National Vocational Qualification-Level 2 (NVQ 2)/General National Vocational Qualification (GNVQ) Intermediate in the United Kingdom. 14 )
Demographics.
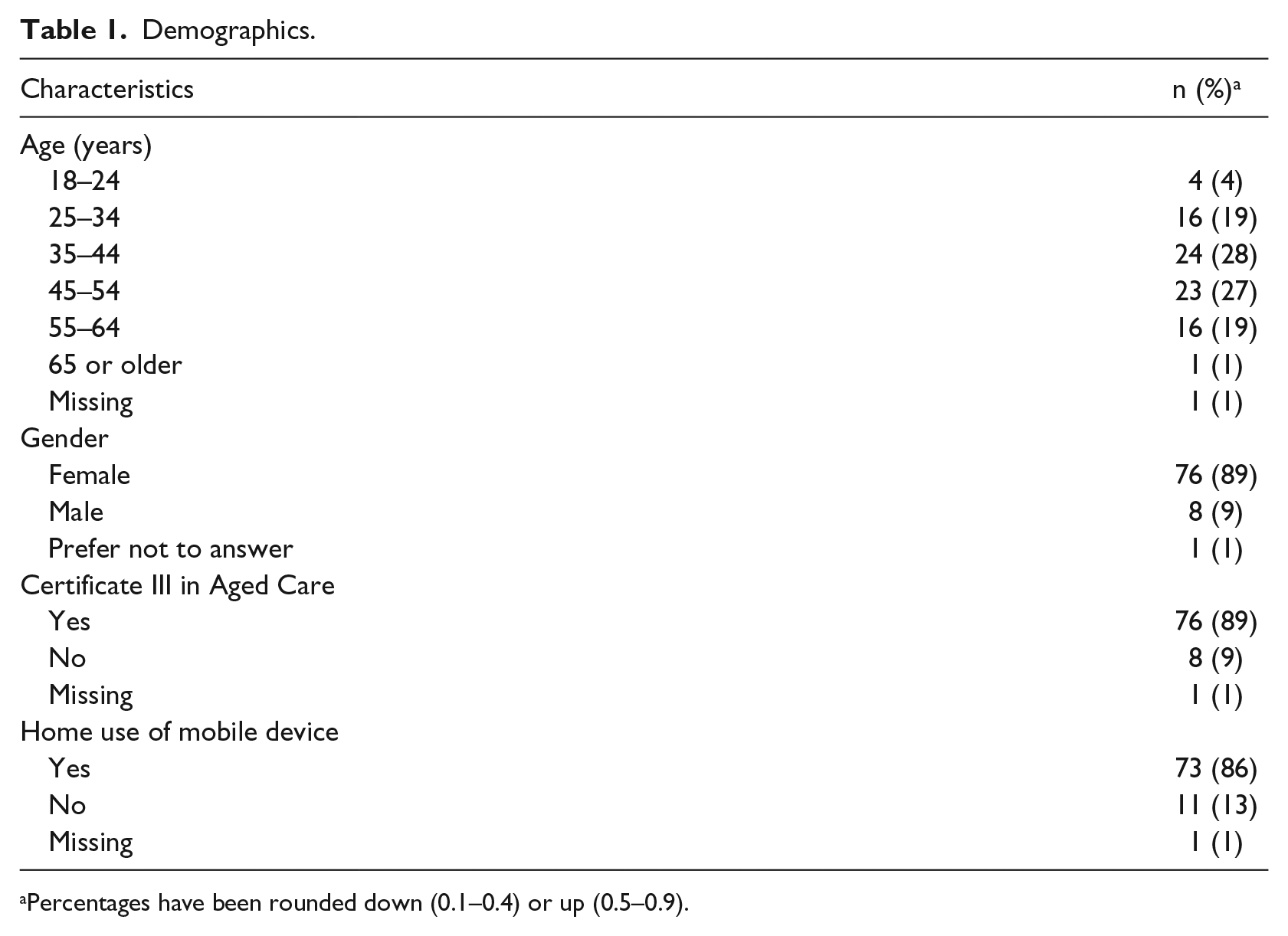
Percentages have been rounded down (0.1–0.4) or up (0.5–0.9).
Results from the questionnaire revealed that 60 per cent of participants reported consistent use of the mobile device when providing care, with a further 15 per cent reporting they sometimes used the device (Table 2). In all, 75 per cent of participants reported that the device was helpful most of the time. Similarly, 73 per cent found it time-saving and 81 per cent found it easy to use. Illustrations were reported to be particularly helpful (85%). Satisfaction with training was high. However, there was no consistency in responses in terms of accessing resident information by other means, for example, desktop computers.
Mobile device and PCP use among PCs/AINs (n = 85).
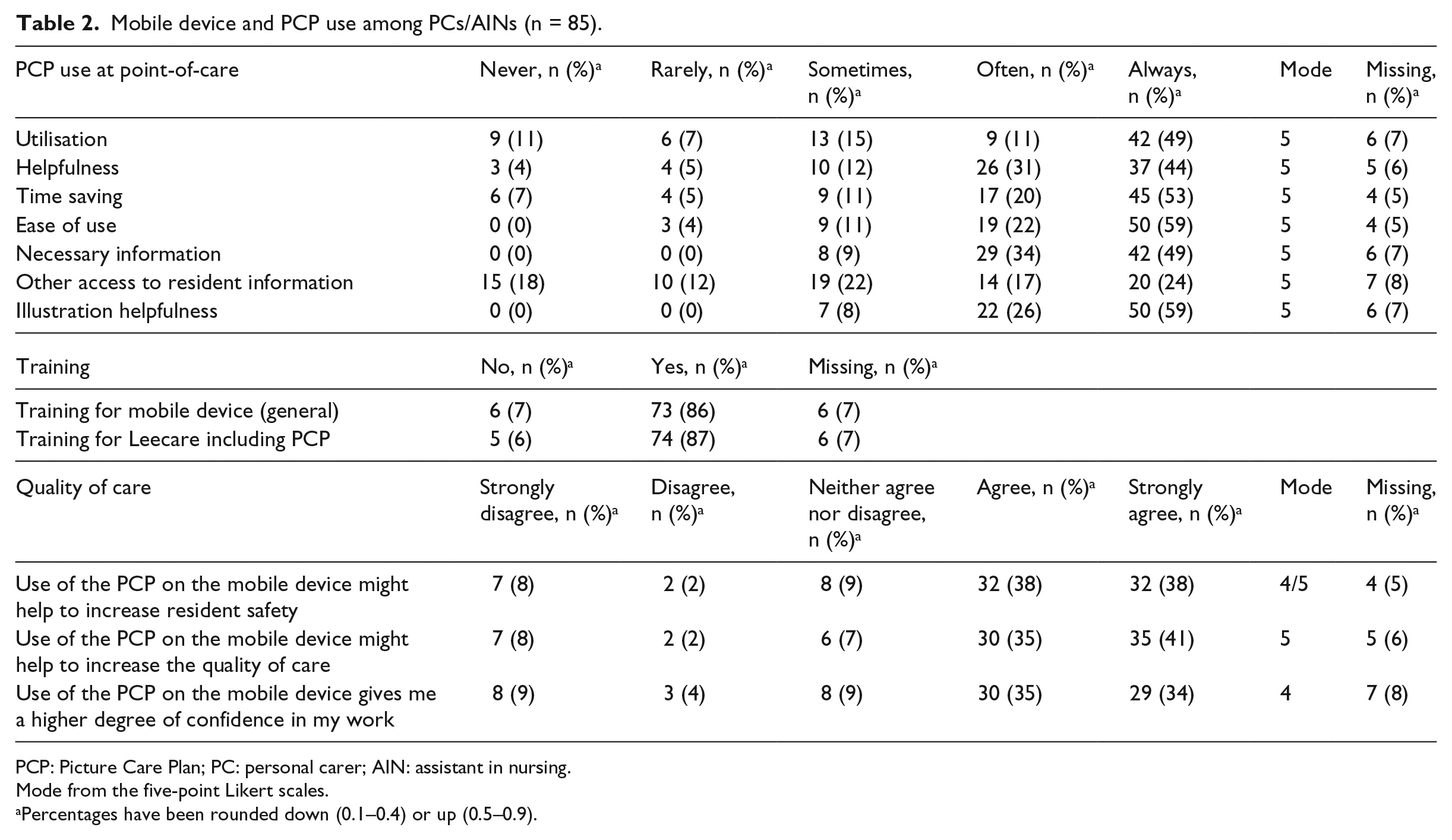
PCP: Picture Care Plan; PC: personal carer; AIN: assistant in nursing.
Mode from the five-point Likert scales.
Percentages have been rounded down (0.1–0.4) or up (0.5–0.9).
Qualitative findings
Comments and questions throughout the survey revealed common themes among respondents with regard to the limitations of utilising the mobile device during care. The number one concern of staff was the weight of the device, with some staff reporting that the tablet was heavy and cumbersome pulling down on their utility belt/shoulder bag. This practical component deterred some staff from using the device while carrying out care duties, ‘to carry the tablet and the phone together when we are providing care for the residents is a bit uncomfortable, the bags provided to us cannot fit both devices’. The tablet weighs 306 g. Some staff also highlighted the need to log into the device due to inactivity several times during a shift as time-consuming and suggested logging in and out only once per shift as a time-saving measure. The current system requires staff to re-enter their password after 20 min of inactivity. This is a security setting to ensure that if a device is accidently left on resident, data are protected. Some staff reported that device and wifi speed as issue and citing time constraints as a deterring factor when utilising the device. Limitations of the device and system expressed by staff predominately surrounded, heaviness, log in times and speed.
In addition to these comments, staff also made suggestions for future improvements. These included the following: wall mounting the devices in the hallways to allow quick access as staff pass to negate having to carry the device and to ensure battery life, more pictures to be included, and having the option to call up only specific items in the PCP, that are needed in that instance. Other useful device applications, such as alerts to be included for 2-h repositioning and for two-person assists were also suggested. Suggestions provided insight into what PCs/AINs believed would be useful in their current work format.
When asked how they, the PCs/AINs, determined that the PCP was updated, the need to confer with the RN or clinical nurse consultant (CNC) at the start of each shift was expressed. PCs/AINs were not able to update changes directly into the PCP, having to verbally report any changes or observations to senior staff members for documentation. The carers cannot update a care plan as this requires a review by RNs and allied health professionals. A care plan guides and provides specific detail of the care that specific resident needs. To determine whether there were any changes to resident care needs confirmation of any changes at handover was necessitated due to the lag time in updating the PCP. One PC/AIN highlighted the importance of communication between staff members of differing positions: Better communication between RN’s/CN’s and PC’s in regards to changes and updates in the PCP. Perhaps more comprehensive and frequent staff messages regarding the change/editing of the PCP. It is difficult for the PC to just ‘know’ what residents have had changes to their PCP, so in this regards I feel like it is extremely important for the lines of communication to be open between all staff when dealing with this.
Despite ongoing technological developments and solutions, communication between staff members at all levels of an aged-care home remains significant to the functionality of the team.
Discussion
Utilisation of PCP at the point-of-care was reported by the staff participants to be easy to use and helpful with most participants employing the technology at least some of the time. Previous findings had indicated that caregivers in long-term care facilities were highly receptive to the use of mobile devices to access residents’ information.15,16 Information from this study further supports that aged-care workers are open and receptive to the integration of new technologies and systems to provide a convenient manner to access resident information. Relevant illustrations accompanying care directives were perceived to be helpful. As one-third of all aged-care staff are from culturally and linguistically diverse backgrounds, with PCs comprising 74.4 per cent of this demographic, 6 pictures may aid in comprehension. Moreover, a significant number of participants believed that the use of the PCP increased resident safety and quality of care, in addition to increasing confidence in their work.
The demographics of the study cohort revealed that 86 per cent of PCs/AINs currently used mobile device technology outside of work, which reflects current trends. 17 Older members of the workforce also readily accepted and used mobile devices in and out of work. In all, 40 per cent of the participating PCs/AINs were aged 45 years or older, reflective of the Australian RACH workforce. 6 This is significant as user age and background knowledge impact user behaviour of electronic devices, with background knowledge shown to influence trial-and-error behaviour and frustration levels. 18 Findings from this study may suggest that home use of similar devices, training and clinical support may positively influence mobile device adoption while undertaking care duties. Computer skills, perceived usefulness and perceived ease of use, all positively influence behavioural intention to use IT applications in long-term care. 16 In total, 86–87 per cent of this study’s participants believed that they received adequate training on the mobile device and PCP, respectively, and perceived usefulness and ease of use were high.
However, barriers to successful integration and consistent utilisation were evident. Personal factors, physical design, software inefficiencies, security and speed of wireless transmission and fear of breaking the device have previously been identified as possible barriers to mobile device adoption in healthcare. 19 In this study, physical design was reported to be particularly problematic. The weight and current method of transporting the device in the custom belt holder or shoulder bag of the Samsung Galaxy Tab 3 7.0″ (306 g) was reported to be cumbersome, echoing a finding from a previous study into the integration of mobile devices in an Australian aged-care facility. 3 The study reported that handheld devices were problematic when carers required the use of both hands to perform manual tasks in the care of their residents. 3 Other factors including device speed and personal preferences for desktop computers and desire to maintain engagement with the resident were also expressed.
Individual characteristics influence perceived fit and ultimate utilisation of the device. 1 Organisational environment may help to reduce the impact of these barriers through physical modifications, adaptations to the software interface and content, and through continued support and encouragement of PCs/AINs utilising the PCP on the mobile device. It has been recommended by Aged and Community Services Australia (ACSA) that industry and government support the implementation and uptake of technological initiatives through support of change management strategies and training. 20 Fostering of positive attitudes towards such technology change and resilience among staff may help to increase uptake of new technological solutions in the workplace.
Communication between staff was also highlighted as an important component of receiving up-to-date information. Data from this study suggest that point-of-care access to information does not impact the need to seek out information by other means. The PCP did not replace the need for carers to confer with senior staff members, in relation to resident changes occurring immediately prior. Practices surrounding communication and care plan updates can be streamlined. Notifications of upcoming reviews would allow PCs/AINs to know which residents were likely to have changes to their PCP and therefore to know to check the PCP prior for changes. Implementation of a communication book detailing observations made by PCs/AINs during their shift, along with current verbal reporting, may also assist communication and help to initiate resident care plan reviews as necessary. A collaborative approach to reviews between not only qualified nurses and allied health professionals but also carers with knowledge of the resident at the coalface may be of benefit not only to residents but also to workplace cohesion. PCs/AINs may contribute further value to the workplace.
Limitations
Limitations included staff participation rates and the absence of an appropriate validated tool. Although participation was open to all PCs/AINs, staff participation rates are typically low, approximately 25 per cent based on previous research at the participating sites. In this study, 20 per cent of PCs participated. Factors affecting participation were availability of staff, with care activities taking priority, and shift work. Nightshift and weekend shift workers were under-represented. Generalisability may also be limited, without the use of a validated instrument. There was no appropriate tool to determine the useability of software tools for carers in aged care. The survey had to be based on practical components of the integration of the PCP, as well as audience readability, influenced by participants’ education level and English literacy. Practical limitations highlighted may provide some insight into the challenges of successfully implementing research in a mostly under-represented group in the healthcare literature.
Future directions
Following consultation with PCs/AINs, revision of the current PCP has and is being undertaken. Senior management in conjunction with clinical support provided by internal business and support services are conducting a review of the efficacy and user-friendliness of the current system with changes to be made based on PCs/AINs preferences, scope of practice and organisational policy. Trialling of some aspects of Leecare as an app on the devices is also being conducted at present with the intention to also add the PCP to the app to increase functionality of the tablet and increase the speed of accessing the information. Future integration of a resident preference-based care planning tool within the application may also fall within scope of the PC duties. The use of mobile technology to help elicit resident preferences by nurses and encourage shared decision-making has previously been shown to improve patient-centred care for elderly patients. 21 Ongoing evolution of the software in line with staff requirements is to be continued to improve utilisation and maintain best practice.
More broadly, ongoing critical evaluation of new mobile devices and tailored software products are required. With the continual emergence of new software packages and technological devices’ usability and effectiveness need to be critically reviewed. As much as technological advancements may seem to enhance accuracy and efficiency, the system still relies upon communication between different members of a team. Up-to-date recording of residents’ care needs relies upon a sufficient system for assessment of the resident, communication and appropriate documentation. As it is outside scope for PCs/AINs to update a residents’ care plan independently, a system needs to be in place to ensure efficient communication and reporting of any changes in the residents’ needs are yet to be addressed.
Conclusion
Continued integration of mobile devices and health management systems into aged-care homes has the potential to increase accuracy and efficiency. Provision of technological solutions designed around the role of the PC is particularly important given that PCs constitute the greatest proportion of aged-care staff and their direct role with the resident. Currently, there is little research into adoption and usefulness of point-of-care information systems around PCs in an aged-care setting. This study aimed to evaluate, from the carer perspective, a mobile tool to assist in the daily-care activities of residents to provide a basis for future developmental changes. Findings suggest that staff are receptive to adoption of mobile devices to access care directives at point-of-care and that the technology is useful. However, barriers pertaining to physical characteristics of the device, speed and staff communication were noted. Evolution of the PCP will continue alongside critical evaluation to provide a successful means of delivering resident information in a manner that supports PCs/AINs to fulfil their role as PC.
Footnotes
Acknowledgements
The authors would like to acknowledge the residential aged-care managers: Arline Burnell, Denice Beauchamp, Fran Larky, Janet Morganti, Jean Moss, Marcelle Maxwell, Silvia Holl, Melissa Peterson, Vicki lea, Wendy Crack and Yvonne Horvath and their staff who participated. The authors would also like to acknowledge Business Support Services for their technical guidance and Silvana Camilleri for providing her knowledge of PC/AIN education and training.
Author contribution
R.E.B. conceived and contributed to study design, data collection, analysis and interpretation, drafting of article and final approval of the version submitted. A.G. contributed to conception of study design, revision of article and final approval of the version submitted. S.M. provided necessary background information for the design of the study and interpretation, and contributed to revision of article and final approval of the version submitted. J.A.W. contributed to conception and design of study, aided in data interpretation, revision of article and final approval of the version submitted.
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: The authors were employed by the not-for-profit group, Wesley Mission Brisbane, which operates the residential aged-care facilities used as participating sites. The primary researcher was independent of the aged-care division, with no restrictions on publication.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.