
Abstract
Objective
To provide high-quality elderly care, digital health technologies (DHTs) can potentially assist in reaching the full capacity of comprehensive geriatric assessments (CGAs) to improve communication and data transfer on patients’ medical and treatment plan information and health decision-making. This systematic review aimed to describe the evidence on the feasibility and usability, efficacy and effectiveness, and implementation outcomes of DHTs developed to facilitate the administration of CGAs for long-term care settings or community care and to describe their technical features and components.
Methods
A search strategy was conducted in three databases, targeting studies evaluating the DHTs facilitating the administration of CGAs used in long-term care settings or community care. Studies in English and Spanish published up to 5 April 2023 were considered.
Results
Four DHTs supporting the administration of the CGAs were identified. Limited information was found on the technical features and required hardware. Some of the barriers identified regarding usability can be overcome with novel technologies; however, training of health professionals on the assessments and staff knowledge regarding the purpose of the data collected are not technology related and need to be addressed.
Conclusions
Barriers regarding usability were related to experienced difficulties navigating the software, unstable network connectivity, and length of the assessment. Feasibility obstacles were associated with the lack of training to use the DHT, availability and accessibility to hardware (e.g. laptops), and lack of insight into the clinical benefits of collected data. Further research must focus on these areas to improve the implementation and usefulness of these DHTs.
Keywords
Introduction
Ageing is associated with comorbidity, polypharmacy, and declining physical and cognitive functioning, causing frail elderly people to receive multiple treatments and interventions from healthcare providers with different specialisms working in different sectors (e.g. community care, acute care, and long-term care). Declining health and the risk of developing functional and cognitive impairment have implications on the quality of life and capacity for independence and autonomy of the older adult population.1,2 This complex interplay between factors related to clients, care professionals, and care sectors yields comprehensive information on elderly persons’ health status, highlighting the need for a high degree of coordination and accurate communication between healthcare providers and clinical interventions to provide quality older-adult-integrated care. 3 This could improve the early identification of individuals at risk of (further) decline, facilitating adequate and timely treatment, care plans, and clinical decision-making.4,5
To tackle the aforementioned complexities, comprehensive geriatric assessments (CGAs) have become an important assessment tool in elderly care, as they capture multiple domains and focus on the variety of complex problems experienced by frail older people.1,4,6,7 CGAs are considered multidimensional assessments that support multidisciplinary care teams in clinical decision-making and personalized care planning to address the needs of older people and their families and carers, emphasizing functional status and quality of life.2,4,8,9
A wide range of benefits of the utilization of CGAs in elderly care has been documented, such as reductions in hospitalizations, admissions to long-term care facilities (LTCF), functional decline, and mortality4,8,10; prevention of negative health outcomes, such as shortened survival times and care dependency 2 ; or supporting improvements in care planning and quality of care. 1 However, as a result of the higher percentage of transitions between care settings in older populations, associated with the complexities of an ageing population and the shift from institutional care to home care (HC) delivery,3,11,12 accurate communication of medical information and treatment plans have become fundamental to provide quality elderly care. 3 For this reason, to reach the full potential of CGAs, their implementation should be supported by electronic data systems that provide relevant output and enable information sharing within multidisciplinary teams of care professionals and multiple care settings in a timely manner, thereby optimizing the coordination of care and avoiding potential discrepancies in terms of the completeness and reliability of data collection.13–15
Digital health refers to the general use of a variety of information and communication technologies (ICTs), big data, genomics, and artificial intelligence (AI) to address health needs and to improve the health, well-being, and care of people.16–19 Digital health technologies (DHTs) are intended to enhance people's health and well-being and to improve health and social care systems.20,21 The variety of digital tools includes, amongst others, the adoption and use of computer platforms, software, mobile apps (mHealth), wearable devices, electronic health records, telemedicine or telehealth, robotics, and monitoring and sensor devices.19,20,22 The employment of DHTs can potentially assist in reaching the full capacity of CGAs and overcome the constraints of data transfer between settings and stakeholders.14,15 Involving DHTs in healthcare systems has been shown to improve the availability, quality, and use of data for healthcare decision-making and offer opportunities for the sustainability of healthcare systems by providing better insight into the quality and efficiency of care delivery.16,23 However, concerns have been raised regarding the overwhelming diversity of available digital health tools and the limited evidence on their impact on health systems and a person's well-being. 16
A previous scoping review identified a lack of publications on web-based applications for frailty assessments in older adults and limited data regarding their time efficiency, security, algorithm efficiency, environmental requirements, and browser requirements. 24 Also, the lack of comprehensive instructions, training materials, and materials to support the interpretation of the results was also highlighted. 24 Nonetheless, the web-based assessment tools showed several advantages such as their convenience and ease of completing the assessments, the implementation of highly friendly user interfaces by most tools identified, and the high cost efficiency of most of the applications. 24
Despite this initial attempt to identify the challenges and opportunities of web-based applications for the assessment of older adults, the scoping review excluded the diversity of digital tools comprised under the term DHTs. Additionally, it focused exclusively on frailty, excluding other potential DHTs covering a wider range of functional domains such as those provided by CGAs, where frailty scales are also embedded. 24 For this reason, we aimed to describe the evidence on DHTs that have been developed to facilitate the administration of CGAs and describe their technical features and components and address the feasibility and usability, efficacy and effectiveness, and implementation outcomes of the DHTs.
Methods
Eligibility criteria
Studies considered eligible for inclusion in this review focused on the feasibility, usability, efficacy, effectiveness, or implementation of DHTs supporting CGAs for long-term care settings or community care. Searches were conducted up to 5 April 2023 in the following databases: PubMed, CINAHL, and Web of Science. Only studies in English and Spanish were considered eligible. See Table 1 for inclusion and exclusion criteria.
Inclusion/exclusion criteria for the search strategy.

CGA: comprehensive geriatric assessment; DHT: digital health technology.
Search strategy
A list of free text keywords and Medical Subject Headings (MeSH) was developed by two authors (MMU and HGvdR) for PubMed. Subsequently, the list was translated to the correspondent-controlled vocabulary headings and appropriate syntax of the other databases. The following search strategy was used:
CGA. ‘geriatric assessment’ (MeSH Major Topic) OR ‘geriatric assessment/methods’ (MeSH Major Topic) OR ‘geriatric assessment’ OR ‘geriatric evaluation’ OR ‘geriatric instrument’ OR GA OR ‘comprehensive geriatric assessment’ OR CGA OR ‘multidimensional geriatric assessment’ AND
Setting. ‘residential facilities’ (MeSH Major Topic) OR ‘Community Health Centers’ (MeSH Major Topic) OR ‘Community health services’ (MeSH Major Topic) OR ‘long-term care’ (MeSH Major Topic) OR ‘elderly care’ OR ‘residential facilit*’ OR ‘long-term care facilit*’ OR ‘LTCF’ OR ‘geriatric care’ OR ‘aged care’ OR ‘home care’ OR ‘primary care’ OR ‘senior center*’ OR ‘residential care’ OR ‘community care’ AND
DHT. ‘internet’ (MeSH Major Topic) OR ‘telemedicine’ (MeSH Major Topic) OR ‘software’ (MeSH Major Topic) OR ‘digital*’ OR ‘internet’ OR ‘electronic*’ OR ‘computer*’ OR ‘automat*’ OR ‘software’ OR ‘web’ OR ‘web-based’ OR ‘mHealth’ OR ‘telehealth’ OR ‘mobile’ OR ‘eHealth’ OR ‘online’ OR ‘app*’
Selection procedure
After duplicate removal, the remaining publications were divided amongst three pairs of authors (six reviewers in total), who screened the titles independently according to the inclusion and exclusion criteria. Within each pair, the screening was compared, deviations were discussed, and agreement was sought. The abstracts of potentially eligible publications were screened by two authors independently (MMU and AM), leading to the final full-text review stage. As the last step, the same authors checked the full texts for eligibility (see Figure 1). In case of discrepancies, a third author (HGvdR) made the final decision to include or exclude the study.

PRISMA flow diagram.
The data extracted from the studies were performed by one author (MMU). The following data were extracted from the final selection: (a) author and year of publication; (b) name of the DHT, (c) name of the CGA; (d) technical features; (e) stage of maturity; (f) aim of the study; (g) study design; (h) country; (i) care setting; (j) description of the study sample (size, female percentage, mean age, and standard deviation); (k) outcomes; and (l) main findings.
State of evaluation (outcome variables)
The state of evaluation aims to determine whether the DHT under evaluation is functioning, is effective or is ready for scale-up, 17 in other words, if the DHT is feasible, usable, and effective or if it can be implemented on larger scales. According to the WHO, 17 the definitions of these outcomes are as follows: (1) the feasibility assesses whether the DHT works as intended in a given context; (2) the usability assesses if the DHT can be used as intended by the users; (3) the efficacy assesses if the DHT can achieve the intended results in a controlled research setting; (4) the effectiveness assesses whether the DHT can achieve the intended results in an uncontrolled (non-research) setting; and (5) the implementation assesses the uptake, integration, and sustainability of the DHT for a specific context (includes policies and practices).
Stage of maturity
The maturity life cycle of DHTs ranges from a concept to a fully developed and functioning platform that is ready for upscaling, providing insight regarding if the DHT has been developed and evaluated for the first time or if it is mature to undergo scale-up. 17 In brief, the different stages of maturity as described by WHO 17 are as follows:
Pre-prototype. This includes hypothesis building, needs/context assessment, and testing of usability/feasibility and technical stability.
Prototype. The user-focused designs are created and tested, as well as the functionality, technical stability, and usability. Improvements are examined.
Pilot. This examines the digital intervention in controlled research settings to assess if it produces the expected effect.
Demonstration. The evaluation is done under some restricted population/region conditions but does not take place in controlled settings.
Scaled-up. At this step, the intervention is ready to be implemented widely across multiple settings or at the population level.
Integration and sustainability. This is the final stage where the intervention is already being used in a broader system, and other supporting features to enhance the impact of the intervention at a large scale are assessed (such as policies, financing, human resources, interoperability, etc.).
Risk of bias (quality assessment)
The quality of the studies was evaluated by two raters through the ‘mERA Methodological Criteria’. 17 This tool contains two sections: (a) essential items that must be evaluated for all studies, independent of study type (23 items), and (b) items specifically for qualitative (3 items) or quantitative (3 items) research. In the case of mixed method studies, items from both categories (quantitative and qualitative) were used.
For this study, each item was rated according to the degree to which the study met the criteria (0 = no, 1 = partial, and 2 = fully). When an item was not applicable to a particular study, the item was not considered in the calculation of the summary score. The summary score was calculated for each study by summing the total score obtained from the relevant items and dividing it by the total possible score. According to this scoring system, results are between 0 and 1: if closer to 0, the methodology is considered poor, and scores closer to 1 indicate a stronger methodology.
Results
After duplication removal, the titles and abstracts of 2723 records were screened, of which 2696 records were excluded. The remaining 27 studies were analysed through a final full-text review. After the final screening, five papers were included for analysis (see Figure 1, PRISMA flowchart, and Supplementary Material, PRISMA Checklist).
The feasibility and usability of the MDS-HC© Electronic web-based interface and the interRAI electronic assessment tools were assessed by one study each.25,26 Kim et al. 27 studied the effectiveness of the System for Person-centered Elder Care (SPEC). Vanneste et al.28,29 focused on studying the implementation of the BelRAI (Table 2).
Characteristics and data extracted from the studies.
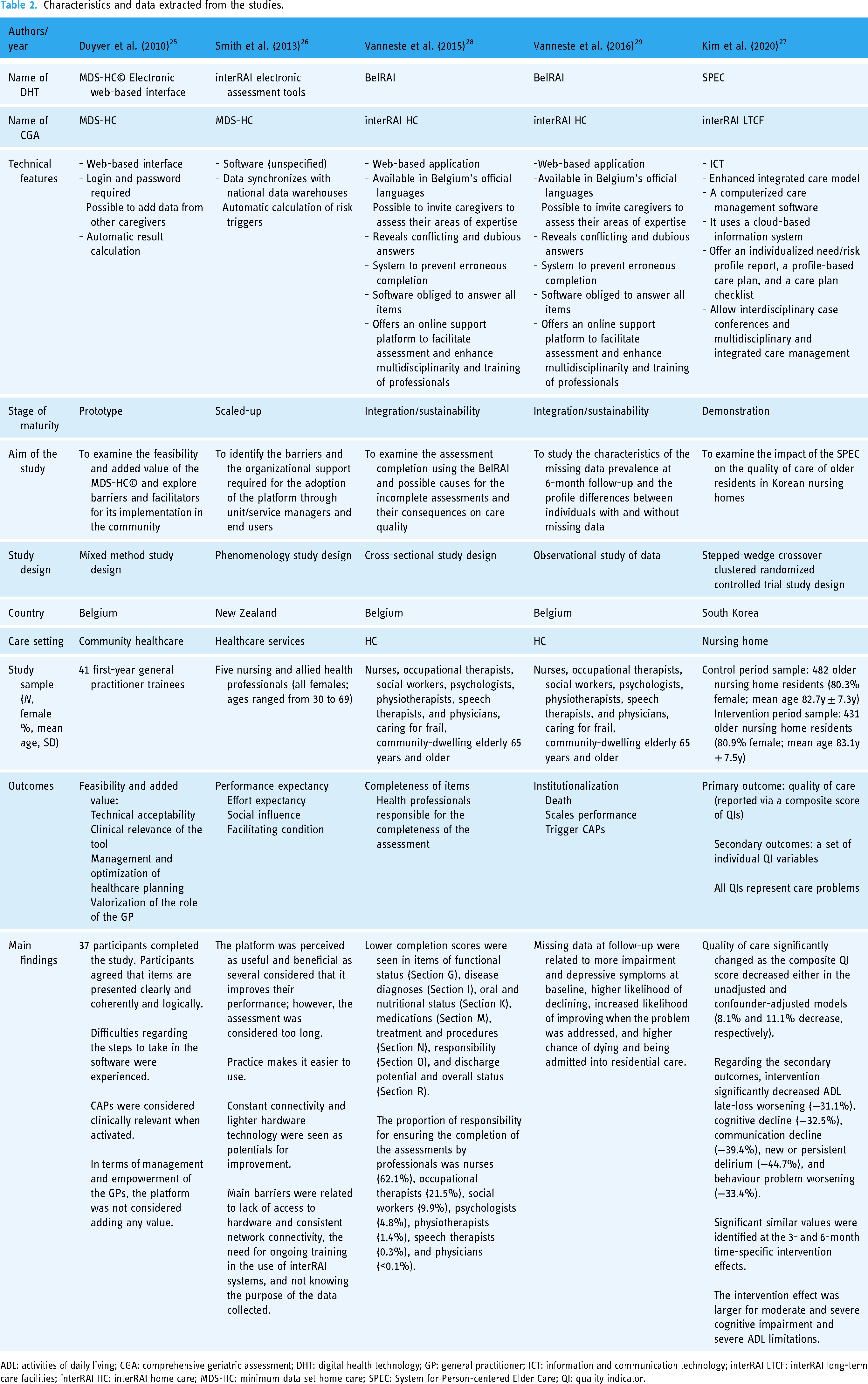
ADL: activities of daily living; CGA: comprehensive geriatric assessment; DHT: digital health technology; GP: general practitioner; ICT: information and communication technology; interRAI LTCF: interRAI long-term care facilities; interRAI HC: interRAI home care; MDS-HC: minimum data set home care; SPEC: System for Person-centered Elder Care; QI: quality indicator.
Study outcomes (feasibility, usability, efficacy and effectiveness, and implementation)
Five studies on four different DHTs developed to support the implementation of CGAs for long-term care settings or community care were identified: (a) MDS-HC© Electronic web-based interface, 25 (b) interRAI electronic assessment tools, 26 (c) SPEC, 27 and (d) BelRAI.28,29 The SPEC was studied in LTCF and the four other DHTs in community care. The DHTs support three CGAs, the minimum data set home care (MDS-HC), the interRAI long-term care facilities (interRAI LTCF), and the interRAI home care (interRAI HC) (Table 3). Two platforms were studied in Belgium (the MDS-HC© and the BelRAI), one in New Zealand (the interRAI electronic assessment tools), and one in South Korea (SPEC) (see Table 2).
CGAs supported by the DHTs identified.

CGA, comprehensive geriatric assessment; DHT: digital health technology; interRAI LTCF: interRAI long-term care facilities; interRAI HC: interRAI home care; MDS-HC: minimum data set home care; SPEC: System for Person-centered Elder Care.
The MDS-HC© and the interRAI electronic assessment tools were at the feasibility and usability stage of evaluation and were in the prototype and scaled-up state of maturity, respectively. The other two platforms, SPEC and BelRAI, have been studied in uncontrolled settings. The SPEC was investigated at the stage of maturity of demonstration and the effectiveness state of evaluation. The BelRAI was in the integration/sustainability stage of maturity and at the implementation state of evaluation.
Regarding how feasible and useful professionals perceived the DHTs, Duyver et al. 25 and Smith et al. 26 found mixed results. Regarding usability, nurses and other healthcare professionals found the interRAI electronic assessment tool software useful and beneficial, as it improved their performance. The DHT helped them gain a broader perspective of the individual's situation and needs and supported them in gathering the relevant information for professionals to provide good care. However, the assessment was considered too long and tiresome. 26 The MDS-HC© was tested amongst general practitioners, who did not report added value regarding their management and empowerment, but they considered activated triggers that warn of clinical risks in clients in the MDS-HC© (clinical assessment protocols (CAPs)) as clinically relevant. 25
Reported facilitators for implementing a DHT were familiarity with the DHT and ease of use 26 and clear and coherent presentation of the items. 25 Usability barriers were related to experienced difficulties navigating the software, 25 unstable network connectivity, and length of the assessment. 26 Feasibility obstacles were associated with the lack of training to use the DHT, availability and accessibility to hardware (e.g. laptops), and lack of insight into the clinical benefits of collected data. 26
The effectiveness of a DHT was only studied for the SPEC by Kim et al. 27 The use of SPEC was shown to have a significant positive impact on the quality of care in nursing homes. This was measured via a composite score of quality indicators, showing reductions in care problems of 8.1% and 11.1% for an unadjusted model and a confounder-adjusted model, respectively. 27 Decreases were also observed in secondary health and functional outcomes, such as ADL late-loss worsening, cognitive decline, communication decline, new or persistent delirium, and worsening of behavioural problems. 27
In terms of implementation, the BelRAI was the only DHT that was studied. Analyses showed that seven out of the 18 domains reported lower completion rates 28 (see Table 2 for the specific domains). The authors attributed this amongst others to the incapability of the assessors due to insufficient training, insufficient information required by other caregivers, and lack of time to complete the assessment during the first house visit. Missing data at follow-up assessments were related to worse health status at baseline, higher risks of decline, admission to LTCF, and mortality. 29 The authors point out that missing data could be an indicator of poor quality of care. The responsibility for data collection was not adequately distributed amongst health professionals involved in the care of a client and relied mainly on nurses. 28
Technical features and components of the DHTs
The MDS-HC© and BelRAI were web-based interface applications, while the interRAI electronic assessment tools and SPEC were software. The used hardware for the interRAI electronic assessment tools was laptops. For the other DHTs, information about required hardware was not reported. Only for the SPEC, it was mentioned to be computerized. Multiple access for data collection, allowing access to multiple health professionals and caregivers to single assessments for data entry, was reported for the MDS-HC© and the BelRAI. The SPEC was reported to allow multidisciplinary and integrated care management; however, multiple access for data collection was not reported. No information regarding user access was obtained for the interRAI electronic assessment tools. The data of the interRAI electronic assessment tools were stored in national data warehouses, and the SPEC was reported to use cloud-based data storage. For the MDS-HC© and BelRAI, no information on data storage was reported. All DHTs enabled the calculation of composite outcomes and scales, reflecting clinical outcomes and risks of decline.
Other technical characteristics were described for the BelRAI, such as revealing conflicting and dubious answers, preventing erroneous completion, and the obligation to answer all items, and it has an online support platform for assessors. In the case of the SPEC, it offers an individualized needs/risk profile report, a profile-based care plan, and a care plan checklist.
Quality of the studies
An initial interrater agreement of 86.2% was reached by two reviewers for the quality appraisal of included studies. The total quality score for the studies ranged between 0.62 and 1.00 (Table 4). The main weaknesses in the quality of identified studies were found in the participant eligibility and sampling, which was only mentioned in Kim et al. 27 ; participant recruitment, reported in Kim et al. 27 and Smith et al. 26 ; and enrolment, described in Duyver et al. 25 and Kim et al. 27 See Table 4 for a detailed overview of the quality appraisal.
Results of quality assessment.

Discussion
To provide high-quality elderly care, accurate communication of the patients’ medical and treatment plan information has been identified as fundamental.3,30 For this reason, we aimed to describe the evidence on the feasibility and usability, efficacy and effectiveness, and implementation outcomes of DHTs developed to facilitate the administration of CGAs for long-term care settings or community care and to describe their technical features and components.
Little information regarding technical features and hardware characteristics that could provide insight into the functioning of the platforms was reported. Only Smith et al. 26 reported using laptops; however, the used software was not specified. In terms of the description of the platform, more features were identified for the BelRAI and the SPEC as compared to the other two DHTs.
Three of the four platforms were studied in community care settings, supporting two CGAs, the MDS-HC and the interRAI HC. Only the SPEC was studied for LTCF and supports the interRAI LTCF. These results raise a concern in terms of how many CGAs are being supported by DHTs, as in this study, only the interRAI family of CGAs was identified, even when a previous systematic review reported a total of three CGAs for long-term care and seven for community care. 31 According to Molinari-Ulate et al., 31 the interRAI family of instruments is the most studied CGA in the scientific literature in both settings, which could explain why there is evidence of the DHTs supporting them. Nonetheless, we cannot conclude if the lack of scientific literature reporting on DHTs supporting the remaining CGAs is because they are not being supported by DHTs or because of a lack of studies and evidence on their feasibility and usability, efficacy and effectiveness, and implementation. The limited research publications in this area have been also highlighted in a previous scoping review studying the web-based applications for the assessment of frailty in older adults. 24
A lack of studies in this regard could lead to poorly designed systems jeopardizing patients’ safety and contributing to psychological stress for users, including burnout and low morale.30,32,33 Two of the studies included in this review identified outcomes associated with this problem. Vanneste et al. 28 identified that several sections were less completed than others, which might lead to concerns regarding decision-making, quality of care, interventions, and care planning, as they are supported by the assessments’ results. Also, Vanneste et al. 29 considered that missing data could be related to lower quality of care, as they identified that the group with missing data at follow-up had worse health status at baseline, were more functionally impaired, showed more depressive symptoms, had a higher risk of health problems (such as cardiorespiratory conditions, undernutrition, dehydration, etc.), and reported an increased risk of mortality and institutionalization when missing data were found in the 6-month follow-up. Additionally, the identified high responsibility of nurses for the completion of assessments 28 associated with the perception of lengthy and time-consuming assessments25,26 could lead to overloading the workload of healthcare professionals and contradicts one of the basic premises of a CGA, the multidisciplinary cooperation to achieve high-quality care.
The results gathered from the studies of feasibility and usability reported some important barriers that could affect the implementation of these DHTs in care practice. Regarding usability, the following barriers were reported: (a) difficulties navigating the software, (b) length of the assessments, and (c) inconsistent network connectivity. In terms of feasibility, (d) availability and accessibility to appropriate hardware, (e) the need for ongoing training to perform the assessment correctly, and (f) the lack of staff knowledge regarding the information collected and its purpose were identified as potential obstacles. Some of these barriers might be overcome nowadays as the DHTs could include novel technologies that have evolved since their publication; for example, there are multiple and novel wearable and lighter devices that can be carried around instead of laptops; network connectivity is constantly evolving in terms of coverage, speed, and consistency; novel software and apps might be able to perform offline assessments; technology can support multiple access for data entry and break down long assessment instruments facilitating a more efficient and multidisciplinary administration; and guidelines and recommendations on the assessment and development of DHTs have been developed.16,34,35 Nonetheless, there are some barriers that are associated with the training of the healthcare workforce, such as the training of health professionals on assessments and staff knowledge regarding the purpose of the data collected. These barriers were also highlighted by Chang et al. 24 who described a lack of comprehensive instructions, training materials, and materials to support the interpretation of the results in web-based applications used for the assessment of frailty in older populations. As these obstacles are not technology related, they need to be addressed by the healthcare systems and policymakers.
Some of these barriers can be tackled by considering the major priorities for strengthening DHTs identified by Sheikh et al. 30 For example, the lack of staff understanding of the information collected and its purpose could be approached by building capacity for managing and analysing data through investing in data science, quality improvement, and health informatics training for the workforce and by incorporating new professionals such as data scientists and clinical informaticists that jointly work with healthcare professionals and patients. 30 Also, engaging the healthcare task force and patients in DHTs’ design and development, research, and implementation process will inform developers on design and evaluation issues, which could translate into early amendments, reducing costs before releasing the system.30,36 This also could lead to more engaging and user-friendly systems 37 that could be more aligned with the needs of the different stakeholders and the context of their healthcare systems.
Identified features that reinforced the usability, effectiveness, and implementation of DHTs supporting the application of CGAs were as follows: (a) utilization of a safe data storage warehouse, such as clouds; (b) inclusion of automatic alerts, notifications, or a continuous check for item completion in the DHTs; (c) access allowance for multiple healthcare professionals on individual assessments in the DHT, avoiding to rely on one professional to complete the CGA but using the expertise of each team member; (d) provisioning of individualized profile reports of needs and risks and personalized care plans; and (e) automatic calculation of the composite outcomes and scales. Assuring the security and privacy of the data and improving the exchange of information between healthcare organizations have been also identified as major priorities for enhancing the implementation of DHTs in healthcare systems. 30
By embedding novel technologies into DHTs supporting the administration of CGAs, such as AI and robotics, the accuracy and efficacy of these identified features could be increased, for example, by including a graphical representation of the person's health profile and status or by providing real-time people's information and feedback from large databases that can facilitate the development of machine learning algorithms. 38 Through this learning health system, clinically relevant information regarding the progression or deterioration of the person can be obtained and could improve timely decision-making and quality and personalization of care.30,38,39
Limitations and future research
The results presented in this review describe the state of the art of the DHTs supporting the administration of CGAs for long-term care settings or community care. The oldest study was published in 2010, and technology has evolved since then. Some of the limitations reported in this review might have been solved; however, information on potential updates and increased maturity of these DHTs not published in selected databases were not taken into account in this review.
We identified limited information regarding technical features and hardware characteristics needed for the proper functioning of the DHTs. The reported characteristics are based on the information available in the articles. Descriptions are often incomplete, missing relevant information that can lead to better insight regarding factors contributing to the usability, feasibility, and effectiveness of the DHTs in care practice, such as devices needed for the administration of the assessments, which functions the platform performs (e.g. automatic calculation of outcomes, alerts, notifications, and notes), or the possibility to involve different disciplines in the assessment. Similarly, there is a lack of studies targeting the implementation of these DHTs on a large scale. Further investigation is required to dig into the technological features of these DHTs and how to fit them into general information systems of health or social care. The relevance of using these tools for improving the quality of care makes it necessary to prove their usability, implementation, and usefulness in clinical settings, which will become relevant for clinical decisions and policymakers.
The scope of this review did not cover any costing implementation analysis of the DHTs. None of the studies included were reviewing this area; however, we consider it very important for future studies to include cost-effectiveness as a relevant outcome as it could improve health and policy decision-making regarding the available platforms. Similarly, due to the limited information and the number of studies identified, it is very difficult to provide a comparison between the DHTs reported. Only one platform was developed for long-term care and the other three for community care, and the description in terms of technological features, hardware characteristics, and other relevant data to provide a helpful comparison is very limited. Additionally, the healthcare systems where the DHTs have been studied might differ substantially as the studies were performed in three different countries on three different continents (Belgium, New Zealand, and South Korea). For this reason, this review provides recommendations and describes different barriers identified from the DHTs included in an attempt to offer some guidelines for future developers and policymakers.
Only studies in English and Spanish were considered, omitting other possible DHTs developed that have been reported in different languages. Also, our definition of a CGA excludes those DHTs that support multidimensional assessments that consist of a collection of single-domain measures, tests, or assessments. For example, digitized frailty assessments or indices were not addressed and not included in the search terms, as we considered that they do not cover the whole spectrum of domains included in the CGAs. Insights on these DHTs that might contribute to improvements of DHTs for CGAs are lacking in this study.
To the best of our knowledge, there are other commercial platforms available. However, studies on usability, feasibility, efficacy, effectiveness, or implementation were not identified. One of the authors contacted several companies that developed and deployed these platforms to inquire about performed studies on these topics. According to the responses received, no studies have been performed on these DHTs.
Even though DHTs are considered essential in collecting, processing, and reporting outcomes relevant to daily care practice, we only identified studies of DHTs supporting the interRAI suite of instruments from all the CGAs identified in Molinari-Ulate et al. 31 For further development of DHTs for this goal and to support optimal utilization of valuable CGAs to improve the quality of care, more insight is required into how care professionals use DHTs and their outputs efficiently, in such a way that it supports daily care practice.
Considering the barriers and limitations reported in this review, there is still a lot of room for improvement regarding the development and implementation of DHTs supporting the application of CGAs in LTCF or community care. Further research should focus on solving the barriers reported in this review, study the functionality of the platforms in up-to-date devices (such as tablets, mobiles, smartwatches, etc.), and focus on the integration of data from CGAs with monitoring data acquired via novel technologies such as wearable technology devices and AI within the DHT.
Conclusions
Data on DHTs supporting the application of CGAs in LTCF or community care are limited, with only five studies and only the interRAI family of CGAs being supported. These studies reported on barriers regarding usability, mainly concerning inconsistency in network connectivity; technical issues leading to inappropriate, inconsistent, and missing data; duration of the assessment; feasibility obstacles such as the availability and accessibility to appropriate devices; and lack of training and knowledge regarding the information collected and its purpose.
Regarding effectiveness, the results of one study reported a significant impact on the quality of care in long-term care settings and a decrease in ADL late-loss worsening, cognitive decline, communication decline, new or persistent delirium, and worsening of behavioural problems. In terms of implementation, the incompleteness of some sections was attributed to insufficient training, insufficient information required by other caregivers, and lack of time to complete the assessment. Responsibility for data collection was identified as not adequately distributed amongst health professionals, relying mainly on nurses.
Recommendations that might enhance the usability, effectiveness, and implementation of these platforms are accessibility to the individual's assessment by multiple healthcare professionals and allowance to break down the sections according to the professional expertise to share the assessments’ responsibility; the use of safe data storage, such as clouds; automatization of a real-time calculation of the scales and outcomes with a graphical representation of the person's profile and health status; automatic alerts, notifications, and continuous monitoring for item completion; and provisioning of personalized care plans according to the data collected.
Limited information reporting on the technical features, required hardware, and lack of implementation studies of DHTs limits the conclusions of this review. Further research must focus on these areas to improve the implementation and usefulness of these DHTs to support the application of CGAs in the healthcare system.
Supplemental Material
sj-docx-1-dhj-10.1177_20552076231191008 - Supplemental material for Digital health technologies supporting the application of comprehensive geriatric assessments in long-term care settings or community care: A systematic review
Supplemental material, sj-docx-1-dhj-10.1177_20552076231191008 for Digital health technologies supporting the application of comprehensive geriatric assessments in long-term care settings or community care: A systematic review by Mauricio Molinari-Ulate, Aysan Mahmoudi, Esther Parra-Vidales, Juan-Luis Muñoz-Sánchez, Manuel A Franco-Martín and Henriëtte G van der Roest in DIGITAL HEALTH
Footnotes
Contributorship
MMU, HGvdR, and MAF-M conceptualized and designed the review. MMU, AM, EP-V, J-LM-S, MAF-M, and HGvdR screened the titles of the records resulting from the search. MMU and AM screened the abstracts and full text of the records that remained after title screening. MMU and AM evaluated the records for risk of bias. MMU extracted the data from the included studies, and it was verified by HGvdR. MMU, HGvdR, and MAF-M drafted and critically revised the manuscript. HGvdR and MAF-M provided overall study supervision. All authors authorized the final version of the manuscript that was submitted. All authors read and approved the final manuscript.
Declaration of Conflicting Interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: MAF-M and HGvdR are fellows of the interRAI Network.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project is part of the Marie Skłodowska Curie Actions Innovative Training Network H2020-MSCA-ITN (grant agreement number 813196).
Guarantor
MMU
Supplemental material
Supplementary material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.