
Abstract
The Ambient Assisted Living Joint Programme, instituted in 2008 by the European Union, aimed to create better living conditions for older adults through the funding of information and communications technology projects. This review aimed to uncover what can be learned from the Ambient Assisted Living Joint Programme by determining (1) the target populations served, (2) technology-based interventions used and (3) effects on health and well-being outcomes. Information from the Ambient Assisted Living catalogue, project websites and deliverables and from papers in PubMed and EMBASE was reviewed. Overall, 152 projects from the first six rounds of funding were identified. Sensors, computers, phones, tablets and televisions were used for various purposes, that is, monitoring, feedback, coaching, reminders and communication. In total, 12 projects reported evaluating health and well-being outcomes; however, these evaluations demonstrated poor methodological quality. Only three projects reported exact values. For all other projects, published evidence on the effect of these projects on health and well-being outcomes was not available.
Keywords
Introduction
The European Union (EU) has predicted that more than 20 percent of Europeans will be aged 65 years or older by 2025, 1 and the increase in the ageing population is expected to have far-reaching consequences in all European member states. 2 Promotion of healthy ageing has been identified as a key objective by the EU. 3 While healthy ageing remains inadequately defined, 4 it has been considered a means for optimizing opportunities for physical, social and mental health and enabling individuals to take an active part in society without discrimination and enjoy independence and a good quality of life. Additionally, promoting healthy ageing means taking a holistic approach that takes into consideration the multifaceted aspects of life. 5
While the majority of older adults have been found to report good health, 6 the prevalence of chronic conditions and disability nonetheless increases with age.7,8 Indeed, older adults more often experience frailty, functional dependency, loneliness and isolation, cognitive impairment, falls, dizziness, syncope and urinary incontinence.9,10 Adequate management of these common conditions necessitates detection, prevention and early intervention.
The main challenge associated with promoting healthy ageing is supporting quality of care in the context of restricted budgets and limited informal and professional care availability. Here, the use of technology, and specifically information and communications technology (ICT), could offer solutions. ICT points to the integration of telecommunication solutions (e.g. telephone lines and wireless signals), computers and middleware, storage and audio-visual systems to enable users to access, store, transmit and manipulate information. 11 Given the constraints of and high demands on professional healthcare, ICT can increase the efficiency of or offer alternatives to professional care. However, ICT has not yet been frequently used in gerontology and geriatrics.
The use of technology in relation to ageing has recently proliferated following the establishment of the AAL JP by the EU. The AAL JP was initiated in 2008 with the objective of creating better living conditions for older adults and strengthening industrial opportunities in Europe by funding ICT projects. 12 Ambient and Assisted Living (AAL) may refer to heterogeneous applications of technologies, products and services ranging from simple devices (e.g. medication dispensers and sensors) to networked homes and complex interactive systems. 13 AAL provides a digital environment that supports autonomous living at home, self-confidence, mobility, health, functional capability and healthy lifestyles and prevents social isolation, enhances security, supports caregivers and increases the efficiency and productivity of resources. A Cochrane review published in 2008 identified a significant volume of the literature on the use of smart technologies within the healthcare setting but did not identify any studies that evaluated the effect of these technologies on person-centred health and well-being outcomes, measures of health or social care requirements or professional performance. 14
Because the Cochrane review did not identify any studies assessing effectiveness outcomes in the published literature, we screened the projects funded by the AAL JP under the purview of the EU beginning in 2008. We aimed to uncover (1) the target populations of current AAL initiatives, (2) the type and commercial availability of the developed technology-based interventions and (3) the effects that have been demonstrated on health and well-being outcomes. The overall aim of this article was therefore to provide a person-centred health and well-being perspective on AAL.
Methods
The catalogue of AAL projects was reviewed, 15 which includes the abstracts of all AAL projects funded within the first six calls of the EU programme, including their contact, consortium and funding details and project websites. Two more recent calls have been issued (in 2014 and 2015); however, projects funded through these calls were excluded, as most of the information for these projects is not yet publicly available. All project abstracts and the websites of all projects were reviewed. If a project website was not available, the project page on the AAL website was reviewed (http://www.aal-europe.eu/our-projects/). All public webpages, reports and papers related to one or more of the AAL JP programmes were reviewed. In addition, the website, http://deliverables.aal-europe.eu/, which contains links to the published deliverables of the AAL JP projects was reviewed, and all available deliverables were scanned for relevant content. The names and acronyms of the AAL projects were entered into PubMed and EMBASE to retrieve published papers. Similarly, Google was searched for commercially available products originating directly from AAL JP projects. Lastly, two public intellectual property rights (IPR) databases (i.e. Espacenet Patent Search and the United States Patent and Trademark Office (USPTO) Patent Full-Text and Image Database) were searched using project acronyms and company and company representative names. Project coordinators were contacted when clarification was needed.
For each project, a standardized summary was drafted containing the following information: contact details, aim of the project, target population, sampling strategy, project methodology, technologies used for intervention purposes, results related to the effect of the intervention on health and well-being outcomes and project outputs (commercial products, intellectual property). Project data were analysed thematically to summarize their aims and the target populations and uses of ICT within the AAL JP. Projects were first screened to determine whether they reported health and well-being outcomes. Next, both reviewers (B.V.G. and T.v.A.) reached consensus on which outcomes reflected health and well-being, and data were collected on the study methodology (i.e. sampling strategy, sample size, methodology (qualitative or quantitative evaluation)) and characteristics of the study design (i.e. group allocation, follow-up periods and measurement of outcomes). In all cases, the health and well-being outcomes of these projects were summarized by a second reviewer. As all studies on health and well-being outcomes used comparative quantitative approaches, nine criteria (i.e. randomized allocation, allocation concealment, groups similar at baseline, eligibility criteria specified, outcome assessors blinded, care provider blinded, subjects blinded, variability of primary outcomes and intention-to-treat analysis) were assessed to determine their methodological quality. 16
All searches, data abstraction, data appraisal and analyses were performed by one reviewer, with discussion with another reviewer in cases of doubt or unclear reporting of results. Additionally, the main findings, their interpretation and conclusions were reviewed and discussed by both authors.
Results
Projects within the Ambient and Assisted Living Joint Programme
In total, the AAL JP fostered 152 projects funded through six calls for innovative projects in support of healthy ageing. 15 The six calls have focused on (1) prevention and management of chronic conditions in older adults, (2) advancement of social interaction in older adults, (3) advancement of independence and participation in the ‘self-serve-society’ in older adults, (4) advancement of mobility in older adults, (5) solutions for (self-) management of daily life activities in the home in older adults and (6) solutions for supporting the occupational life of older adults. The development of ICT-based services for and solutions to age-associated problems was a central component of every project.
Target populations
Overall, community-dwelling older adults were the end-users of interest. Many studies included relatively younger patients; 11 projects sampled data from individuals aged 50 years or younger, 55 projects included individuals younger than 65 years old and 70 projects included individuals younger than 70 years old. In 23 projects, the oldest participants were aged 70 years or older; 13 projects included individuals aged 80 years or older and only 2 projects included adults over the age of 90 years. Seven projects reported the mean age of their participants, and the mean ages of participants in these studies were 61, 62, 65, 74, 71, 51 and 82 years. Many projects also included (informal) caregivers as either primary or secondary users. General populations of older adults living at home were targeted in 68 projects, and (informal) caregivers were included by 19 projects. Only one project focused on nursing home residents. Other projects focused on specific populations of individuals living at home (see Table 1). These projects targeted working older adults or retired individuals from a labour perspective (n = 15), individuals with specific geriatric problems or conditions (n = 40) and individuals with chronic health problems (n = 8). Finally, one project aimed to support producers of AAL technology.
Target populations.
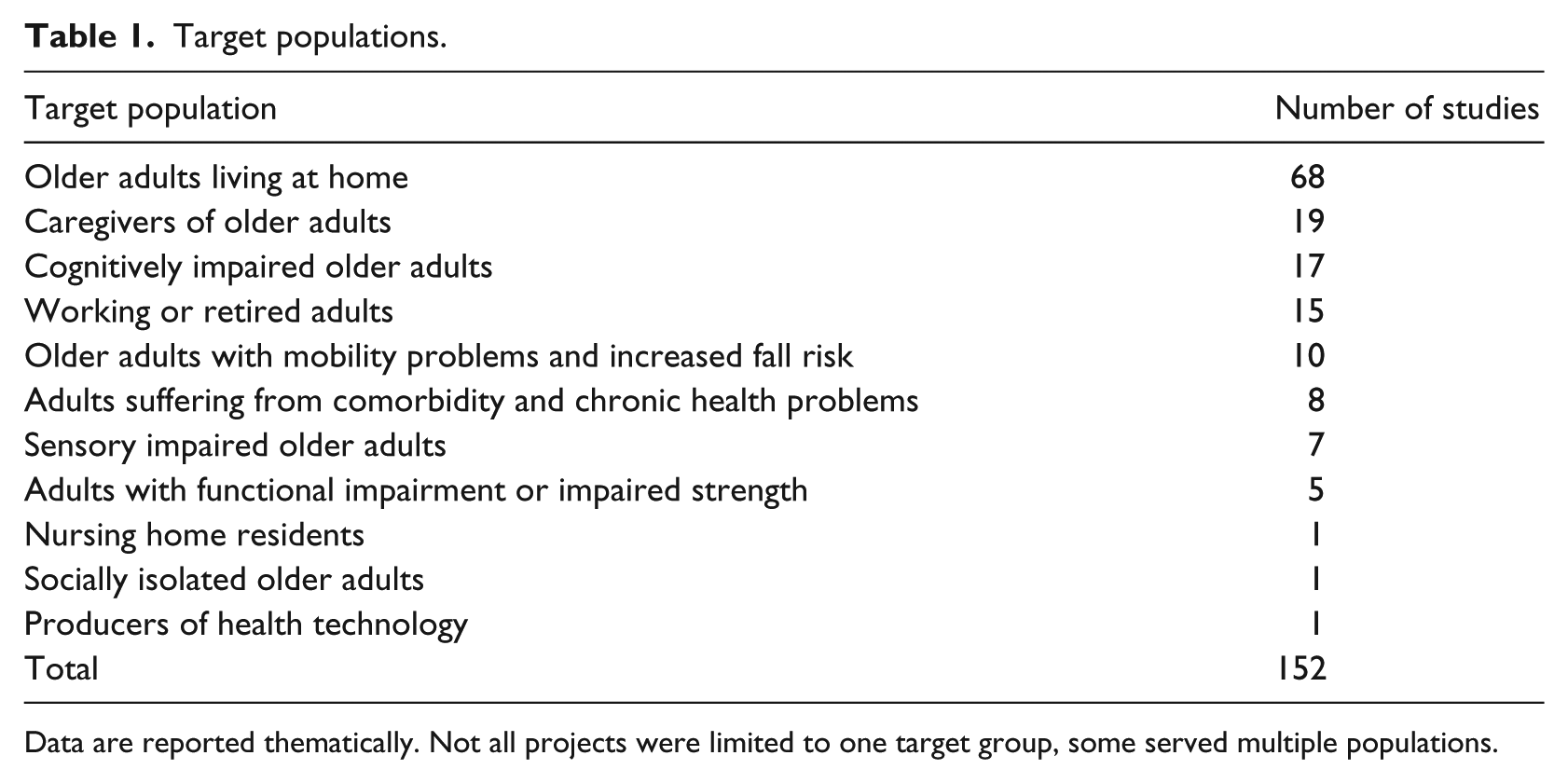
Data are reported thematically. Not all projects were limited to one target group, some served multiple populations.
Technologies and purposes
As a result of the six AAL JP calls, various technologies were utilized for different purposes (Table 2). Sensors were frequently used, often in combination with other technologies and with various purposes. Sensor technology was always used for the purposes of monitoring and measurement and most often used for the measurement of vital signs or other physical parameters (n = 26), measurement of activity level (n = 15) and detecting emergency situations (n = 12). Sensor technology was used less frequently for monitoring medication intake (n = 3), locating and/or tracking individuals (n = 5) and detecting care needs (n = 3). Personal computers (PCs), phones, tablets and televisions often facilitated various intervention components. These technological devices were most often used to facilitate communication and interaction (n = 56) through video, audio, text, social media and networks, interactive games, virtual worlds and forums to support social inclusion, connectedness and telemonitoring. These telecommunication means were also employed for coaching or education purposes (n = 32); giving feedback on activity (n = 11); sending reminders for activities of daily living, medication intake or exercise (n = 23); monitoring or assessing older adults and supporting them during emergency situations or with care needs (n = 30) and service provision such as information related to news, social events, activities, trip planning, shopping assistance or health planning (n = 27). Finally, these technologies were also used for outdoor orientation, navigation and mobility (n = 24) and exercise (n = 2). Other ICT applications that were used to a lesser extent were smart kitchens (n = 1), electric power wheelchairs (n = 1), e-stockings (n = 1), assistive exoskeletons (n = 1), AXO-suits (n = 1), ambient lighting (n = 1), all terrain walker frames (n = 1), intelligent loudspeakers (n = 1), white canes (n = 1), hearing implants (n = 1), wall displays (n = 1) and smart gloves (n = 1). Some differences were noted with respect to the main purpose of these ICT solutions, for example, phones were more frequently used for outdoor orientation and navigation (n = 24) and monitoring the status and activities of relatives (n = 11). A PC, however, was more frequently used for coaching and education purposes than were other technologies (n = 19).
Technology-based interventions.
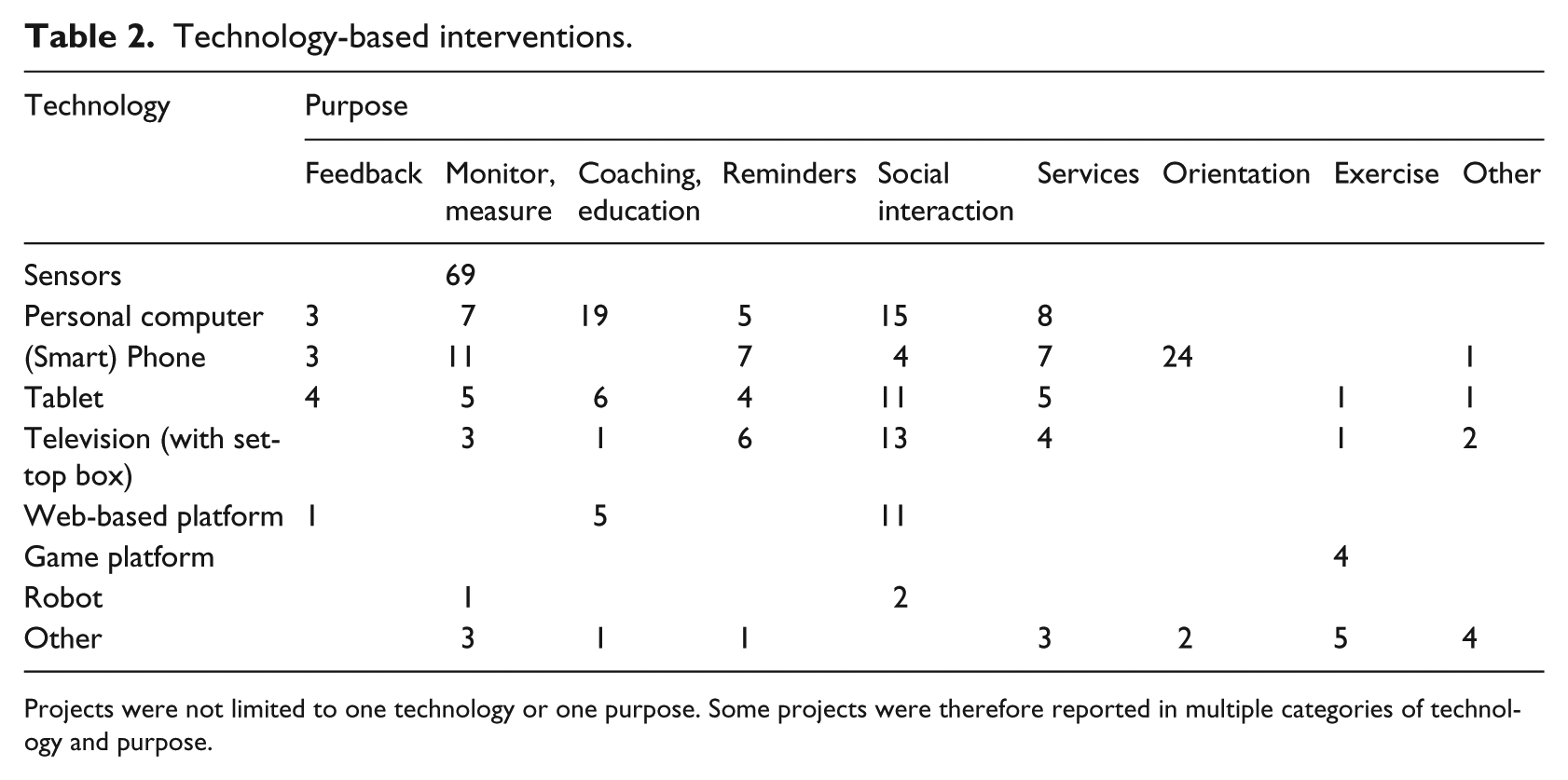
Projects were not limited to one technology or one purpose. Some projects were therefore reported in multiple categories of technology and purpose.
Project outputs: commercial products and intellectual property
A total of 62 projects reported developing a business model and marketing strategy. Of these projects, four (the RGS, M3W: the RGS, M3M, T-Break Osteolink and Dalia projects) made their product available to the public, and three (the Inclusion Society, I’CityForAll and T&Tnet projects) publicly reported registration of an IPR.
The RGS project developed a virtual reality–based system for stroke rehabilitation and, based on this project, founded a spin-off company named Eodyne. Eodyne offers a rehabilitation gaming system that can be used at home or in the clinic for recovery of motor and cognitive function after brain damage. 17 The Maintaining and Measuring Mental Wellness (M3W) project developed an online tool with computer games to measure mental changes and support mental wellness in an online community. 18 An account can be created on the M3W project website for free. The T-Break Osteolink project developed an online osteoporosis community to address the educational and support needs of osteoporosis patients in Europe and Australia. An account can be created on the T-Break Osteolink project website for free. 19 The Dalia project developed a personal virtual assistant for communicating with family and friends, maintaining a calendar and diary writing, emergency calls and falls detection, medication reminders and health state tracking. 20 The Virtask company has made this virtual care assistant, called ‘Anne’, available as a commercial product. 21
The Inclusion Society project developed a service system platform that connected users with friends, family and healthcare providers to support self-management of health and well-being, and, based on this project, developed a spin-off company named ‘WellTogether’ who would own the IPR (but no further information is available). 22 The I’CityForAll project developed audio systems to improve community mobility in hearing impaired adults and filed a patent for these systems. 23 The T&Tnet project developed a personalized context-based multimodal journey planning app and reported sharing the intellectual property rights within its published strategies. 24
Evaluation methodology and outcomes
A user-centred design was utilized by all the AAL JP projects. Generally, the performance of an end-user requirement analysis provided support for the development of ICT-based services. These services were then validated during lab-tests or field-tests, employing survey analyses of usability and acceptability. Specific sampling strategies were generally not reported, but a small sample of volunteers usually piloted the ICT within the projects.
A total of 12 projects reported aiming to evaluate the effects of AAL solutions on health and well-being outcomes. All of these projects used quantitative comparative designs, and qualitative evaluations of health and well-being outcomes were not described. By 1 June 2016, six of these projects had not yet reported results (four of the six projects were ongoing during the first half of 2016, while the other two projects were completed on 1 March 2011 and 1 March 2013).
Six projects (Agnes, Aladdin, RGS, Rosetta, Confidence and GAMEUP) reported results for the health and well-being outcomes assessed using a comparative design. Three projects used randomized controlled trials (RCTs); two projects used non-RCTs and one project used a single group pre-post comparison. These six projects included modest numbers of subjects (between 30 and 60) in their evaluations; however, their methodological quality was questionable (Table 3). Study reports often provided unclear descriptions of several aspects of the studies including blinding of outcome assessors, baseline equivalence of study groups and eligibility criteria for participants. Information on the specific outcomes of these projects is provided in Table 4.
Methodological quality.
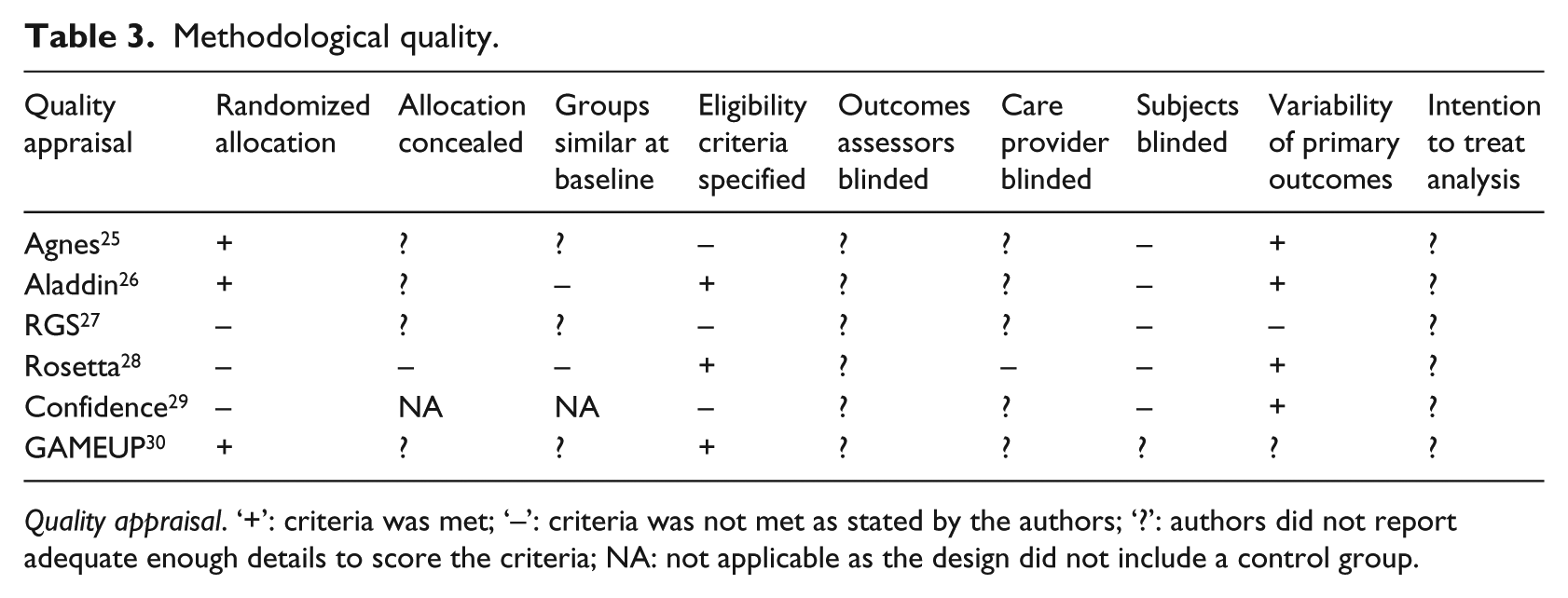
Quality appraisal. ‘+’: criteria was met; ‘–’: criteria was not met as stated by the authors; ‘?’: authors did not report adequate enough details to score the criteria; NA: not applicable as the design did not include a control group.
Effectiveness of AAL solutions on health and well-being outcomes.
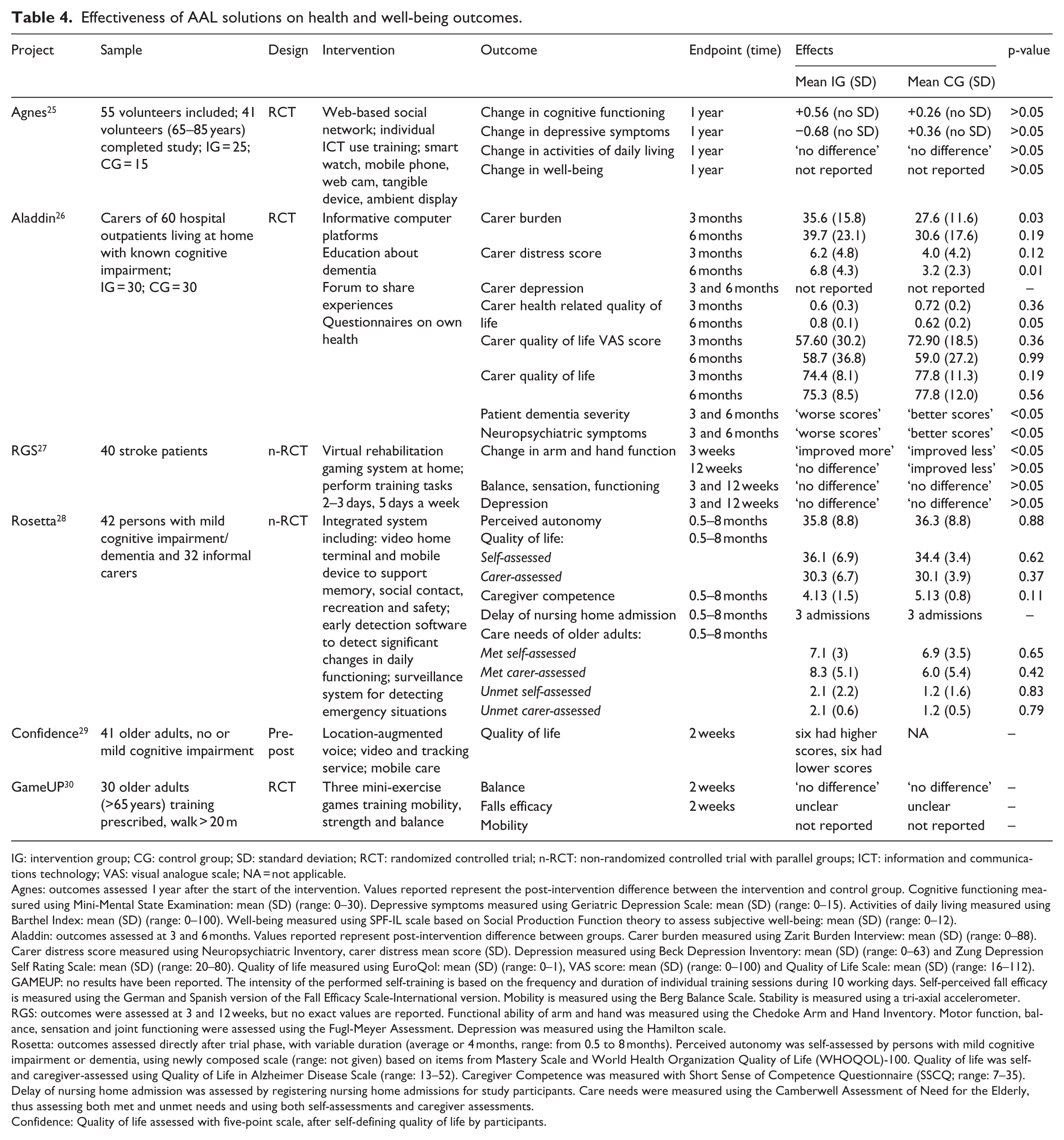
IG: intervention group; CG: control group; SD: standard deviation; RCT: randomized controlled trial; n-RCT: non-randomized controlled trial with parallel groups; ICT: information and communications technology; VAS: visual analogue scale; NA = not applicable.
Agnes: outcomes assessed 1 year after the start of the intervention. Values reported represent the post-intervention difference between the intervention and control group. Cognitive functioning measured using Mini-Mental State Examination: mean (SD) (range: 0–30). Depressive symptoms measured using Geriatric Depression Scale: mean (SD) (range: 0–15). Activities of daily living measured using Barthel Index: mean (SD) (range: 0–100). Well-being measured using SPF-IL scale based on Social Production Function theory to assess subjective well-being: mean (SD) (range: 0–12).
Aladdin: outcomes assessed at 3 and 6 months. Values reported represent post-intervention difference between groups. Carer burden measured using Zarit Burden Interview: mean (SD) (range: 0–88). Carer distress score measured using Neuropsychiatric Inventory, carer distress mean score (SD). Depression measured using Beck Depression Inventory: mean (SD) (range: 0–63) and Zung Depression Self Rating Scale: mean (SD) (range: 20–80). Quality of life measured using EuroQol: mean (SD) (range: 0–1), VAS score: mean (SD) (range: 0–100) and Quality of Life Scale: mean (SD) (range: 16–112).
GAMEUP: no results have been reported. The intensity of the performed self-training is based on the frequency and duration of individual training sessions during 10 working days. Self-perceived fall efficacy is measured using the German and Spanish version of the Fall Efficacy Scale-International version. Mobility is measured using the Berg Balance Scale. Stability is measured using a tri-axial accelerometer.
RGS: outcomes were assessed at 3 and 12 weeks, but no exact values are reported. Functional ability of arm and hand was measured using the Chedoke Arm and Hand Inventory. Motor function, balance, sensation and joint functioning were assessed using the Fugl-Meyer Assessment. Depression was measured using the Hamilton scale.
Rosetta: outcomes assessed directly after trial phase, with variable duration (average or 4 months, range: from 0.5 to 8 months). Perceived autonomy was self-assessed by persons with mild cognitive impairment or dementia, using newly composed scale (range: not given) based on items from Mastery Scale and World Health Organization Quality of Life (WHOQOL)-100. Quality of life was self- and caregiver-assessed using Quality of Life in Alzheimer Disease Scale (range: 13–52). Caregiver Competence was measured with Short Sense of Competence Questionnaire (SSCQ; range: 7–35). Delay of nursing home admission was assessed by registering nursing home admissions for study participants. Care needs were measured using the Camberwell Assessment of Need for the Elderly, thus assessing both met and unmet needs and using both self-assessments and caregiver assessments.
Confidence: Quality of life assessed with five-point scale, after self-defining quality of life by participants.
Agnes included 55 older adult volunteers in an RCT and evaluated improvements in cognition and well-being using validated screening instruments at 1-year follow-up. 25 The intervention used in-home sensing technology to collect information on the emotional status, living situation and activity of older adults and facilitate social inclusion with their family and friends. For this project, a web-based social network was developed using input gathered from a smart watch, mobile phone, web cam, tangible device and ambient display. One year after the start of the intervention, no effect was observed on cognition, mood, functional performance or overall well-being when comparing the post-test scores between the intervention and control groups. Only the ‘affection’ well-being subscale demonstrated significant improvement.
Aladdin included 60 participants with known (mild to moderate) cognitive impairments and their caregivers in a multicentre RCT. The project aimed to reduce caregiver burden and distress and improve caregivers’ quality of life with assessment at 3 and 6 months using validated screening instruments. 26 Sensors monitored the daily activities of the older adults and assessed psychiatric and behavioural symptoms. PCs were used to administer questionnaires, to provide support, information and education and to share experiences. Health-related quality of life of informal caregivers improved significantly more in the intervention group as compared to the control group over a 6-month period, but other assessments of quality of life showed no differences between the intervention and control groups. The distress score in caregivers at 3 months’ follow-up was higher in the intervention than control group, but this difference could be related to the higher distress scores identified at baseline. Among participants with mild to moderate cognitive impairment, individuals in the intervention group suffered from more severe dementia and neuropsychiatric symptoms at 3 and 6 months than did individuals in the control group; however, the differences identified at follow-up between the two groups resembled baseline differences.
RGS reported conducting a non-RCT including 40 stroke patients to evaluate the effects of virtual rehabilitation gaming at home. 27 Stroke patients in both groups were asked to perform a 20-min training task two to three times a day, 5 days a week. The intervention group played the RGS project’s virtual games, whereas the control group was asked to stack and unstack plastic cups. The study report provided p-values for statistical tests only, which indicated no differences in any outcomes at 12 months. At 3 months’ follow-up, the study results indicated ‘more improvement’ in arm and hand function in the intervention group but no differences in other study outcomes.
Rosetta evaluated an integrated ICT system for older adults with mild cognitive impairment or dementia. 28 The system included a video home terminal, mobile device to support memory, social contact and recreation and software to detect changes in daily patterns or emergency situations. The non-RCT performed to evaluate the effects of this intervention included 42 older adults and 32 informal caregivers. The study evaluated perceived autonomy, care needs, quality of life and time to nursing home admission in older adults and competence in caregivers but did not detect any differences between study groups.
Confidence included 41 older adults with or without mild cognitive impairment in a single group pre-post study. 29 The Confidence project set out to provide a mobility safeguarding service for older adults that included a location-augmented voice and video-channel, tracking service and mobile care service. The quality of life in older adults was assessed at baseline and after 2 weeks of using the mobility service. Statistical testing results were not provided, but the study report indicated a lack of pre-post differences in quality of life; out of the 12 participants with a changed quality of life, 6 reported improvement and 6 reported deterioration.
GAMEUP utilized an RCT including 30 individuals older than 65 years of age and able to walk independently for over 20 m to determine post-intervention effects on balance, mobility and perceived falls efficacy. 30 Participants used a Kinect®-based system to play three mini-exercise games, and improvements in the aforementioned outcomes were evaluated. The available study report did not provide exact numbers or estimates but reported no differences in balance between the intervention and control groups and provided an unclear description of the effect of the intervention on falls efficacy. Outcomes for mobility were not reported.
Discussion
The AAL JP was instituted to foster ‘the emergence of innovative ICT-based products, services and systems for ageing well at home, in the community, and at work’. 12 With the original programme running from 2008 to 2013 and covering a budget of 600 million Euros, the AAL JP resulted in a total of 152 projects aimed to support healthy ageing.15,31
The ICT solutions funded by the AAL JP were selected for their potential to support independent living among older adults by facilitating health monitoring, coaching and education, feedback, reminders, activity and social interaction through the use of technology. While many projects aimed to develop a marketable product, only two projects met this objective (a spin-off company was established in both cases). Indeed, other reviewers have also concluded that few devices and standards were tested and applied beyond the pilot study level. 32 The observed lack of, or delay in, offering marketable products as a result of these projects is in accordance with the results of a recent systematic review on the development of robots for supporting independent living. 33 The review identified 107 robot development projects, of which only six were commercially available. The authors concluded that there is a large discrepancy between what robots were claimed to be capable of doing and what was demonstrated in publications, suggesting that it will be a long time before a robot will really be able to enhance independent living in older adults.
The AAL JP was created with the aim of ‘increasing the quality of life, autonomy, participation in social life, skills and employability of older adults, and reducing the costs of health and social care’. 12 However, only 12 (out of 152) projects reported aiming to evaluate the effect of these AAL solutions on health and well-being outcomes. Of these studies, only six reported the results of these evaluations and only three reported exact comparative values. The overall quality of these studies was very low (both in design and sampling methods), and sample sizes were small, thus limiting their internal, external and statistical conclusion validity.
While innovative ideas are proposed, their values must be ultimately demonstrated by improving outcomes relevant to older adults and using prospective controlled studies. Others have suggested that health technology assessment should focus on process measures rather than outcomes. 34 We believe that both are needed, as changes in processes can affect outcomes, but complex interactions with context determinants can result in non-linear relationships.35,36 It would be incorrect to assume that changes in processes will automatically affect the desired outcomes. First, the theoretical assumptions underpinning the changes in the process might not be valid (i.e. theory failure). Second, a novelty effect may initially produce change, but this change may not be maintained over time (i.e. implementation failure). As a result, the value and impact of AAL technology can only be considered in relation to the longitudinal outcomes associated with its use in answer to the following question: Does the technology produce the hypothesized change and lead to the desired effect, and is this effect sustained over time?
While we highlighted the importance of outcome assessment, other key dimensions of quality should be considered in evaluations. Solutions should (1) be tailored to individual needs, (2) recognize a natural decline in health and progressing disability, (3) be continuously co-created and (4) be embedded in social networks based on service integration and (5) learn and improve. 37 valuation of AAL solutions can, therefore, not be restricted to quantitative outcome evaluations but should also incorporate in-depth qualitative evaluations that address the following question: How did a unique individual experience the value of AAL solutions in relation to their personal life values, needs, challenges and context? However, no such evaluations were identified in the AAL JP projects.
Based on the results of this study, we recommend AAL projects to consider the following. First, ICT should be considered as a facilitator of health and well-being interventions but not their main driver. 38 Theory- and evidence-based behavioural strategies should inform the use of technology for health and well-being purposes. Second, ICT should not be considered a standalone solution. While self-management aims to increase individuals’ involvement and control over their own lives, professional involvement is still needed for teaching new skills, instilling confidence, providing self-management tools and assessing problems and accomplishments.39,40 Third, ICT solutions should be designed to fit into everyday life to be used to their full effect, 14 and should, therefore, require minimal effort and be relevant, as indicated by the perception of the user. Indeed, the solution should fit a personal need. 37 Furthermore, ICT solutions should be designed to support long-term usefulness and fidelity to their designed use, as abandonment of the solution is a major threat to its effectiveness. Fourth, designing ICT solutions to fit current care, health and well-being initiatives, services, processes and structures could help facilitate their uptake. Primary care professionals, for example, have a central role in supporting self-management in individuals39,40 and have been considered key to the success of telehealth. 41 Fifth, AAL projects should demonstrate their effectiveness in order to facilitate implementation within the healthcare setting and convince healthcare professionals to use the designed solutions. 42 Sixth, ICT solutions should be designed to accommodate what matters most to individuals with assisted living needs (i.e. social connectedness, mobility and autonomy). 43 Overall, AAL solutions should be considered a complex intervention for which the UK Medical Research Council framework for the development and evaluation of complex interventions could be used. 35
Considering the perspectives of the AAL JP and other published studies, the value of ICT for healthy ageing and independent living in general and AAL specifically remains to be determined. However, three studies funded by the AAL JP are ongoing and may still prove their effectiveness towards promoting healthy ageing and independent living. Protection of intellectual property may also explain why information regarding the effectiveness of these interventions was unavailable, as companies may not want to publish key information regarding their studies and results; however, it should be noted that very few studies set out to study effectiveness. Furthermore, the search strategy employed in our review was limited to projects funded by the AAL JP in the EU, and although our results are in line with other reviews and a database search of abstracts in PubMed and EMBASE, other AAL solutions may exist that have proven to be effective in the improvement of health and well-being outcomes. This review only considered outputs related to population health and well-being. However, while an evaluation of the user-centred design process leading to project outputs might also prove to be a useful exercise, such an assessment was outside the scope of this study.
Finally, the results of this review could be considered very disappointing. So far, an investment of 600 million Euros in 152 projects has led to two marketable products and no evidence indicating superior health and well-being outcomes in older adults. However, it should be noted that the vast majority of these projects ran for 3–4 years and were initiated with the development of new or partly new ICT solutions. The AAL JP probably encouraged its project consortia to promise marketable solutions and demonstrate benefits, but it could be questioned if these objectives were realistic. In this light, the AAL programme’s goals could be revisited with the objective of increasing realism and specifying priorities. A more realistic end goal might either be proof of concept or starting from proof of concept and aiming for impact evaluation. Nonetheless, the EU should be clear on what is expected from project outputs.
Conclusion
A discrepancy between project aims and outputs was identified, as the majority of projects focused on product development but have not yet demonstrated a significant impact on healthy ageing and independent living in terms of the products available on the market or beneficial outcomes in older adults. This discrepancy reflects a lack of clear objectives provided by the AAL JP and a lack of standards for developing, evaluating and implementing health technology in general. When developing technology, products should be co-created and driven by end-users instead of technology-driven, which appears to be the current standard. A particular concern is the maintenance of technology use over time and how the technology fits the dynamic needs of an older adult progressing through the course of life. When evaluating technology, several perspectives should be considered including both quantitative effects and qualitative user information, and long-term use should be monitored. Ultimately, the value of the AAL JP, in specific, and health technology, in general, will be determined by the benefits associated with older adults’ health technology use in everyday life. However, this information is not yet available.
Footnotes
Author contribution
Both authors conceived the study, designed the search methodology and performed the literature search and analysed the data. Both authors drafted and revised the paper. The second author supervised this research.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.