
Abstract
Objectives
Efficient and accurate communication between healthcare professionals (HCPs) serves as the backbone to safe and efficient care delivery. Traditional pager-based interpersonal communication may contribute to inefficient communication practices and lapses in medical care.
Methods
This study aimed to examine the impact of Medic Bleep, a National Health Service (NHS) information governance-compliant instant messaging application, in an NHS Hospital Trust. We examined Medic Bleep’s impact on participant time and workflow using time–motion methodology. Cohorts of doctors and nurses using both Medic Bleep and the traditional pager were compared. Secondary endpoints of our study were to assess whether efficient communications could lead to better resource utilisation, patient safety as well as better quality of work life for the end user.
Results
Assimilation of Medic Bleep corresponded to a reduction in mean task-duration that was statistically significant (p < 0.05) for To Take Out (TTO) and Patient Review categories. Nurses saved an average of 21 minutes per shift (p < 0.05), whereas doctors saved an average of 48 minutes (p < 0.05) per shift. Qualitative analysis suggested that HCPs benefited from better work prioritisation, collaboration and reduced medical errors enabled by an auditable communication workflow.
Conclusion
Medic Bleep reduced time spent on the tasks requiring interpersonal communication. Efficiencies were seen in Discharge Patient Flow, Patient Review and TTO categories. This improved HCP availability and response times to the benefit of patients. End users revealed that Medic Bleep had a positive effect on quality of work life.
Background
Information communication technology (ICT) has revolutionised the landscape of medicine as never before. Efficacious communication between caregivers is a key objective in the pursuit of safe and efficient care delivery. This study explores how traditional pager-based interpersonal communication may contribute to inefficient communication practices and lapses in care. 1
Technology is transforming our ability to predict, diagnose and treat diseases. Researchers have identified that 92.6% of doctors possess a smartphone, and of that 80% are willing to use their device within the workplace in a bring-your-own-device (BYOD) manner.2,3 Although this allows access to a vast amount of extra medical resources, very few efficient technologies are being used to serve a hospital’s information technology (IT) requirements. Therefore, the use of safe and reliable interpersonal communication will play a vital role in improving the use of IT in the workplace in the future.
Historically ubiquitous, if not synonymous with the image of the doctor, the humble pager is no longer seen as an effective solution to handle communications between healthcare professionals (HCPs). This outdated mode of communication suffers from a number of issues not limited to long waiting times for an answer, process bottlenecks at the ward phone, lengthy time to complete or return to tasks as well as an inability to identify the location or identity of the caller and relative urgency of the required task. 4
Consequently, with these constraints in mind, compounded by staff and bed pressures, we are at risk of lapsing in the care that we can deliver to our patients. There are many research papers that have outlined the use of mobile telecommunication devices and their importance in hospital workflows.5,6 Many dimensions are considered, including decision-making capability, interoperability with existing digital architecture, interoperability with electronic health records (EHRs) and online reference access. 3 Nevertheless, few studies quantify the time wasted due to communication inefficiencies and how this can affect an HCP’s ability to deliver optimal care.
To address these shortcomings in healthcare communication, Medic Bleep, an app-based instant messaging system was devised and designed by Medic Creations. Medic Bleep operates across mobile phones, tablets and computers to facilitate instant, information governance-compliant communication with features tailored for HCPs to deliver enhanced patient care. The full description of Medic Bleep along with relevant FAQs can be viewed at www.medicbleep.com.
Objectives
Our study aimed to:
Examine the impact of Medic Bleep on HCPs’ time and workflow. Evaluate staff satisfaction on using their own smartphone in a BYOD capacity, ascertain whether they would welcome the adoption of Medic Bleep into their clinical workflow and determine whether Medic Bleep could increase their quality of work life.
Materials and methods
In May 2017, West Suffolk NHS Foundation Trust commissioned Medic Bleep to conduct a pilot study to evaluate the ability to replace the non-cardiac pager with Medic Bleep. The study was designed to evaluate both quantitative and qualitative endpoints in a representative clinical environment. The pilot programme commenced on June 5th 2017, where a doctor and a nurse were followed using the time–motion study (TMS) methodology for two days each, prior to the pilot of Medic Bleep, as well as during the pilot, amounting to eight days in total.
This pilot programme aimed to explore the efficiency of Medic Bleep compared with the traditional pager device in three varied clinical wards and their respective multidisciplinary team in West Suffolk NHS Trust. We aimed to capture the typical stream of interpersonal communication in an NHS hospital and quantify differences in task duration using an instant messaging mobile device. Comparators included the ease and mean duration of task, efficiency of information transfer, end-user perception and how all these factors affected care quality and delivery.
Prior to the live adoption of Medic Bleep in selected wards, several pre-pilot protocols were implemented to ensure user buy-in, optimal functionality of the smartphone application as well as staff training. Care was taken to consider all aspects of introducing a new method of communication into a clinical environment maintaining a focus on patients as well as the end user.
Post-pilot questionnaires were administered to relevant staff in September 2017 to evaluate smartphone application usage, experience of Medic Bleep and end-user satisfaction
Participant selection
During the pilot, three distinct clinical areas were selected: the trauma and orthopaedics ward (F3), the maternity ward (F11) and the maternity day assessment unit (including community midwives). Each clinical area had a two-week period to engage with Medic Bleep; regular team debrief meetings were set up to ensure successful adoption. The rationale for selection of these diverse wards was that their distinct hierarchies would enable us to analyse the different communication networks and workflows that reflect a typical hospital.
Study design
We used a TMS design to evaluate our primary objective. Participants were allocated via a random number generator to use the conventional pager or Medic Bleep for communication. Continuous time–motion observations were performed with HCPs at all three wards both before and after Medic Bleep implementation. Observers included both independent recruits from West Suffolk Hospital and also from Medic Bleep. They followed pilot participants throughout their shifts and timed specific activities that required interpersonal communication. Each HCP was followed across a two-week period and timed to elicit task durations for each task that demanded communication with other HCPs. Tasks were further categorised by HCPs, allowing for fair assessment and analysis.
Quantitative analysis
Following the recording of each communication event during the two-week period on each respective ward, data were extracted and then categorised into the initiator and receiver of each message, the aim of each communication event, response times, and the duration of each entire communication event. Data were analysed using the R Project for Statistical Computing, and statistical significance was taken at the 95% confidence interval (CI). Kernel density plots were used to visualise the differences in observed task-duration; Welch’s t-test was used to determine whether the apparent differences in distribution were likely to have occurred due to random chance or were due to a real difference in the mean task-duration.
Qualitative analysis
To assess the current state of interpersonal communication, 24 interviews were conducted across the nominated wards and the IT team. We sought to identify communication workflows considering each step in a communication pathway and how it might affect care delivery. A visual process-map illustrating bottlenecks in communication as well as potential areas where Medic Bleep could provide considerable benefit. We also created a visual process-map.
An 11-item questionnaire (Figure A1, Appendix) based on market research conducted on various focus-group users of Medic Bleep, and incorporating commonly seen user issues from literature regarding mobile phone communication application use. The questionnaire was developed dynamically using the authors’ own experiences but also drawing on similar questionnaires developed at other NHS Hospital Trusts, to ensure that questions would be comprehensive and representative.
Results
Throughout the pilot, over 2600 minutes (43 hours) of task duration were analysed, amounting to over 90 points of interaction between the multidisciplinary team. Whilst using the traditional pager, 86 points of interaction yielded over 3800 minutes of clinical communication over two days of recording. A visual interpretation of the tasks recorded can be seen in Figure 1. Figure 2 shows the task duration for both Senior House Officer and Nurse categories with sufficient data for further analysis.

Task duration for SHO and Nurse categories.

Task duration for SHO and Nurse categories (with sufficient data for analysis).
Quantitative task mean duration analysis
In order to quantify the efficiency of communication modality, we observed the mean task-duration when using Medic Bleep versus the traditional pager for communication. To determine whether these observations could be explained by random chance, or were statistically significant, we conducted a Welch two sample t-test on each of the distributions. For both doctors and nurses, we observed that the reduction in task mean duration was statistically significant (p < 0.05) in both To Take Out (TTO) and Patient Review categories. Due to a relatively small sample size, we also considered the 75% CI (at its conservative, lowest value), as results were often skewed by outliers.
Nurse task mean duration
The kernel density plot (Figure 3) results visually demonstrate the distribution of task duration when using the traditional pager and Medic Bleep. Nurses saved on average 10 minutes per TTO (Range: 6 to 22 minutes) and 11 minutes (Range: 3 to 38 minutes) per Patient Review and Escalation of Care, which amounted to a daily saving of 21 minutes per nurse (95% CI) to up to 56 minutes (75% CI). However, we found that time saved during the Drug Round was not statistically significant.

Kernel density plot of Nurse task duration.
Doctor task mean duration
The kernel density plot (Figure 4) results visually demonstrate the distribution of task duration when using the traditional pager and Medic Bleep. Doctors saved on average 10 minutes (Range: 6 to 29 minutes) per Patient Review, and Escalation of Care amounting to a saving of 48 minutes per shift at the 95% CI to up to 80 minutes at the 75% CI.
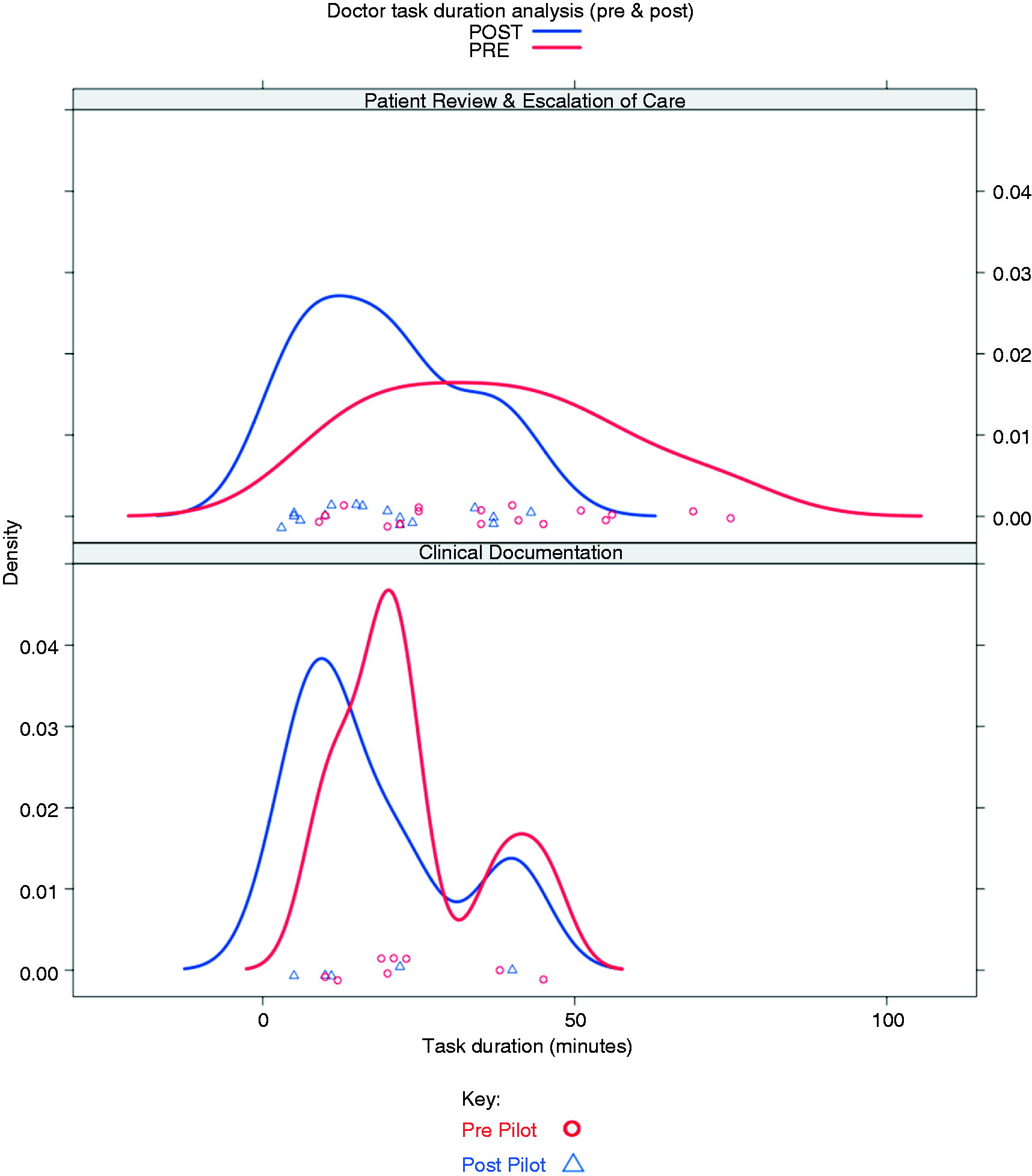
Kernel density plot of SHO task duration.
Midwifery and pharmacy
When we analysed the data aggregated from the communication events by midwives and the pharmacy, we found that there were insufficient data collected to be statistically significant.
Discussion
This study used both qualitative and quantitative methods to compare the use of Medic Bleep against the traditional pager in three clinical areas at West Suffolk NHS Trust. Due to the paucity of research examining task duration as a result of interpersonal communication, we felt that this topic deserved focus and analysis. It is widely understood that poor communication between HCPs can lead to a variety of negative outcomes including poor resource utilisation, increased patient length of stay (LOS), medical errors and poor quality of work life.1,4,7,8 In this study, we have demonstrated that many of the negative outcomes described above can be overcome using Medic Bleep.
Benefits from quality of information transfer
Timely, accurate and efficient information transfer between HCPs promote patient safety and prevents negatively impacting the continuity of care. 5 A systematic review by Prgomet et al. examines the benefits of smartphones in clinical sites with clear implications for optimised information transfer. These include better staff and resource allocation, reduced adverse medical events and earlier notification and treatment of patients. 5
Current use of the pager only alerts the recipient with a mere notification of a message. Therefore, there is no initiator identity, location, content or, often, indication of level of urgency. Regardless of the actual clinical event in question, the recipient will be interrupted from their current task to determine the urgency of the message. Chisholm et al. showed that, on average, a physician was interrupted during their primary task over 30 times in a 3-hour period. 9 Other Studies looking into physician interruptions cite an average interruption occurring every 12.6 minutes. 9 Although avoidable adverse events have not been included in these studies, other industries have widely documented primary task interruption as a direct cause of error. Reviews into the aviation industry have implicated nearly 50% of errors to primary task interruption. 10 Here we can anticipate a clear propensity for individuals to inadvertently contribute to error, harm or adverse events when constantly interrupted.
Although it can be argued that interruptions are ubiquitous in modern medicine – patients, tasks and emergencies are continuously added to a doctor’s list – and that interruptions are integral to ensuring that those with the greatest clinical need are prioritised, interventions must be made to reduce the length of avoidable interruptions and in turn, reduce potential harm.
Failures in information transfer are common in the surgical field, however researchers suggest that it is endemic throughout the continuum of care. 11 Key points of communication breakdown throughout the surgical workflow have been indicated: incomplete handover, primitive forms of information transfer, and a lack of standardised protocols have been identified as the most prevalent causes.11,12 Although a direct quantitative measure cannot be derived, there is broad consensus from participants that these failures contribute to harm.11,12 Especially affected by optimised communication was the TTO process; here failure to provide accurate and timely information can ordinarily contribute to wasted resources and an increased patient LOS. 1 These results are promising and indicate that improved communication workflows may contribute to a reduced LOS; however, further research must be conducted with much larger sample sizes to produce a quantitative and definitive conclusion.
Users of Medic Bleep reported that the application facilitated more efficient task completion on the assessed parameters. Qualitative analysis revealed that Medic Bleep reduced primary task interruption, improved quality of information transfer and allowed users to prioritise tasks. But perhaps the most significant benefit was a reduced interruption-duration at the bedside, which may enhance the doctor–patient relationships.
Benefits from reduced mean duration of task
Perhaps the most striking finding was that there was a statistical difference in the average time taken to complete a task across doctors and nurses. This finding is concurrent with Joseph et al. His team noted that 98% of individuals surveyed demonstrated that there were ‘improvements in speed and quality of communication amongst team members’ when using smartphone devices. 13 Authors have also suggested that electronic modes of communication may be advantageous during handover. 14 Specifically, the robust transfer of information using a watertight electronic system is key to reducing workload and optimisation of physician workflow and, therefore, a better utilisation of resources and man-power. 14 Raptis et al. suggest that over two-thirds of junior doctor task time is devoted to small tasks and interventions. 14 Optimisation of these tasks electronically has the potential to reduce overall task time, allowing physicians to increase task efficiency and improve availability and response times to the benefit of patients. 14
Delays in task completion can hinder care and eventually risk the development of adverse events. Much of these delays occur when an HCP needs interpersonal guidance from another HCP. Wu et al. demonstrate that smartphone use for interpersonal communication leads to improved efficiency and strong user preference. 15 Strikingly, the time required to contact a physician improved by over 60% compared with the traditional pager on an internal medicine ward. 15 Similarly, our results indicate that the use of an instant messaging application could facilitate similar improvements in task completion and efficiencies in task duration. By reducing task duration, HCPs can save time during interpersonal communication that may result in faster patient processing or a reduced patient LOS.
End-user perception
Following the pilot, HCPs were invited to complete a questionnaire on various aspect of Medic Bleep. Qualitative analysis indicated that the use of Medic Bleep may offer a better quality of work life. The vast majority of participants cited reasons including more patients seen, more time for patient care, less distraction in workflow and easier communication. Moreover, participants were extremely likely to recommend Medic Bleep to a friend, with an average score of 8.7 (on a Likert scale of 1 being unlikely and 10 being extremely likely).
Current communication modalities are on the whole begrudged by HCPs with common reasons including ‘waiting for the phone’ (after being bleeped with the traditional pager) and being constantly interrupted by non-urgent messages. Users were grateful for Medic Bleep’s ability to triage tasks and reduce bottlenecks in their workflow. Nevertheless, further research must be completed to identify the full consequences of inefficient communication and particularly its effects on quality of work life especially in highly charged environments like a hospital.
Limitations
Although the total number of study participants was 181, we feel that our results offer an indication of how an application-based instant messaging device could result in task-duration efficiencies in an NHS hospital. Despite this, we require larger sample sizes and a study of longer duration to ensure the findings are representative. In further studies we will endeavour to observe a greater range of members of the multidisciplinary healthcare team to evaluate Medic Bleep as a comprehensive communication tool.
Furthermore, a different individual doctor was followed on each day (and at different times), these both amount to participant and temporal variance.
Despite our low sample size, care was taken to include a wide variety of HCPs. The pilot was undertaken in several representative wards and Medic Bleep demonstrated improvements in each.
Conclusion
From our pilot study, we have demonstrated that Medic Bleep reduced time spent on tasks that required interpersonal communication. Efficiencies were seen in Discharge Patient Flow, Patient Review and TTO categories. These efficiencies potentially improved HCP availability and response times to the benefit of patients.
End users revealed that Medic Bleep had a positive effect on quality of work life. The use of Medic Bleep and its assimilation into clinical workflow demonstrated the staff’s appetite to replace the traditional pager. With high levels of smartphone ownership and usage of medical applications amongst HCPs, transition to a mobile application-based interpersonal communication may be more straightforward. Nevertheless, further study must be conducted on a larger study sample with greater clinical variability to further support the benefits of using Medic Bleep as a tool to improve interpersonal communication.
Abbreviations
HCP – healthcare professionals
MB – Medic Bleep
TTO – To Take Out (describes the process of writing up and processing medications before a patient is discharged)
ICT – information communication technology
BYOD – bring your own device
EHR – electronic health records
NHS – National Health Service
TMS – time–motion study
LOS – length of stay (describes the duration of time a patient spends in hospital)
Footnotes
Acknowledgements
This research would not have been possible without the hard work and diligence of West Suffolk Hospital NHS Foundation Trust. In particular we would like to thank our colleagues Dr Nick Jenkins, Mr Dermot O'Riodan and Rowan Procter whose insight and expertise were integral to the success of this study.
Conflict of interest
Rahul Menon is an intern at Medic Creations.
Funding
This work has not received any funding.
Guarantor
Rahul Menon.
Ethical approval
Not applicable.
Contributorship
Rahul Menon and Christopher Rivett researched the literature and conceived the study. Both authors contributed to the manuscript equally, reviewed and edited the manuscript and approved the final version of the manuscript.
Peer review
This manuscript was reviewed by two individuals who have chosen to remain anonymous.