
Abstract
This mixed methods study evaluated student and provider attitudes and expectations about offering students online access to their student health services visit notes (open notes). Six (N=6) health care providers from four public universities in northeastern Massachusetts participated. Qualitative interviews were completed by students (N=14) from one University in fall of 2013 and an online survey was completed at two universities in Spring of 2014. Attitudes and expectations were explored using qualitative data and descriptive statistics were used to analyze survey questions. Students’ interviews revealed that they desire control over their health and open notes would give them insight and involvement in their health care. Survey data supported these themes. In contrast, providers worried about how it could impact provider-patient relationships. Open notes has the potential to promote students’ understanding and responsibility for their healthcare, which could assist students in their transition from pediatric to adult health care.
Keywords
The Health Information and Technology for Economic and Clinical Health Act of 2009 (HITECH Act) encourages healthcare providers to give patients the copies of their health information. 1 Although patients have long had the right to view their health records, these records are somewhat difficult to access, often involving onerous permissions and copy charges and extensive delays. As a result, their usefulness to patients is limited and health records are not typically considered a tool to assist patients in managing their health. However, with the advent of electronic health records (EHRs), some healthcare systems have begun allowing patients to access sections of their health records through patient Internet portals.1,2 Through these portals, patients are typically given access to their laboratory results, and medication and problem lists. However, few systems provide patients access to providers’ office visit notes. Opening the visit notes to patients can have important benefits to patients, including better understanding of their healthcare, tracking health over time, and better planning for healthcare visits.1,2 This transparency offers the potential to enhance the quality of care by allowing patients to better understand their diagnoses and treatment plans or by detecting errors in their records.2,3 Recently, Delbanco and colleagues2-4 were the first to study the impact of providing adult primary care patients with online access to their EHRs, including visit notes, through a patient Internet portal (aka “The OpenNotes Study”). The majority of patients reported that access to their visit notes was beneficial while doctors reported little to no negative effects. 4 Allowing patients to read their healthcare visit notes is an evolving trend, and it may become a standard moving forward.
While more health centers, including mental health, are moving toward the OpenNotes model,2-5 many college health centers have not yet considered this important step. College is an ideal time to prepare young adults to become effective communicators with their healthcare providers and become effective managers of their own health and health care. Providing opportunities for students to understand how to best access and utilize their medical record, including visit notes, may assist youth in the transition from pediatric to adult care. Gaining this independence will be critically important to learn essential life skills as they become independent, and later, as their parents age and need more assistance and advocacy from them.
To our knowledge, no studies have examined students’ and their providers’ attitudes and opinions about offering open notes in university health centers. Given the emerging use of open notes in adult ambulatory care, understanding how it could impact college health is warranted. Additionally, college students today have “grown up” with technology and can offer unique insights into how electronic medical records, portal systems as well as other computerized devices, could improve their healthcare experience. The purpose of this study was to evaluate student and provider attitudes and expectations about offering open notes in college health.
Methods
Procedures and study design
A mixed-methods descriptive study was completed to explore attitudes and opinions about student-accessible health records including access to providers’ visit notes (i.e. “open notes”). The study was conducted in two phases: the qualitative (Phase I) and quantitative phases (Phase II). Phase I took place in Fall 2013 and used in-depth interviews with providers and students to obtain data about their expectations and attitudes toward open notes. Providers (n = 6) from four public universities in Eastern Massachusetts completed a semi-structured interview either in-person or over the telephone. Students (n = 14) from one university were interviewed in-person. All Phase I participants received a gift card, US$20 for providers and US$25 for students. Phase II took place in Spring 2014 and used a survey to explore attitudes about open notes. Prior research on open notes 3 and information from Phase I were used to inform the survey questions. Respondents were entered into a random drawing for a gift card (one valued at US$200, two at US$100, and three at US$50). All study procedures were approved by the institutional review boards of the University of XXa (XXXa) and the University of XXXb (XXXb).
Participants
Phase I: qualitative interviews
Provider participants were recruited from the student health service centers (SHS) at four public universities in Eastern Massachusetts. An e-mail was sent to clinic directors at these institutions to inform them of the study and invite them and their providers to participate in the interviews either in-person or by phone. Snowball recruitment methods were used to recruit additional providers.
Student participants were recruited from only one of the four public universities. Flyers were posted on campus, and a mass e-mail announcement was sent to students with a valid university e-mail address. Students were asked to contact the study office by phone or e-mail if interested in participating. Students were eligible if they were at least 18 years of age, had completed at least one primary care visit to the student health center in the past year, and were currently enrolled full-time at the university.
Phase II: student survey
Student participants were recruited from two of the four public universities. Originally, the study was to take place only at an urban commuter school, XXXa. To gain the perspectives of students at a residential campus, however, an additional public university with campus housing was invited to participate. Students at XXXa were recruited using the same methods as in Phase I, with the addition of an information table set up in the university student center. Students at XXXb were recruited via postings on the university’s website and announcements in the daily university e-mails. All interested students were asked to contact the study office (via e-mail or phone) to receive a unique web address to the online survey. Students were eligible if they were at least 18 years of age and currently enrolled in one of the two universities. Surveys were administered using a secure, web-based application, Research Electronic Data Capture (REDCap). 6
Data collection
In-depth interviews
One of the study investigators (J.W.) conducted interviews with the students, and two trained research assistants interviewed the providers. A semi-structured interview guide was used (see Appendix 1). The interviews were designed to elicit attitudes and expectations about open notes.
Student survey
The online survey was designed to take about 15 min to complete. Questions about age, college enrollment, and healthcare utilization were assessed. Only respondents defined as “users,” those who reported at least two healthcare visits to any healthcare provider at any health center or at least one visit to SHS (excluding immunization visits) in the previous 12 months, answered questions to assess attitudes and expectations about open notes (see Appendix 1). All others, defined as “non-users,” were not asked about open notes.
The survey included questions from the original OpenNotes survey.3,7 The questionnaire was used to measure how reading visit notes might affect the respondent. Students were asked whether they disagreed or agreed with each of 16 statements. The stem for each item was, “If I could read my doctor’s visit notes on a secure website,” for example, “I would understand more about my health and medical conditions”—A 5-point Likert response from disagree to agree plus the option of “I don’t know.” This scale was originally developed using qualitative methods to generate item content, face validity evaluation, and cognitive testing of the final survey to ensure that patients understood the meaning and intent of each question. The development of the OpenNotes survey is described elsewhere.3,7 The introduction to the scale was modified slightly to define doctor as either doctor or nurse practitioner (NP).
Data analysis
Qualitative data analysis
Qualitative analyses, including manual data reduction, data display, and data interpretation, were conducted using methods described by Farzanfar. 8 Recordings of five of the six provider interviews were transcribed by a research team member. Recording was unavailable for one interview, and analyses were conducted using interviewer notes. One team member acted as lead coder for the provider interviews and the student interviews. These coders read the transcripts, highlighted and took notes about emerging themes, created a code book, and extracted text that represented themes and categories. Another team member was trained by the lead coders to use the code book to extract text from the transcripts that represented the themes and categories. The codes and text fragments were entered into Excel for review and analysis by an investigator, who conferred with the coders about the results until an agreement was reached.
Quantitative data analysis
Descriptive statistical analysis was used for the survey responses including means, modes, and standard deviations for continuous variables, and frequency percentages for categorical variables. Sample proportions were calculated for students who agreed with statements about potential risks and benefits of open notes. 7 The categories of “agree” and “somewhat agree” were combined, as were the “disagree” and “somewhat disagree” categories; “don’t know” responses were retained as a separate category and were included in denominators for that questionnaire. 7 All analyses were performed in SPSS Statistics for Windows (version 22.0; Armonk, NY, 2011).
Results
Qualitative results
Six female providers, who were NPs, participated in the in-depth interviews as the primary providers of college healthcare and represented four public universities. We had no inclusion criteria other than that participants needed to be direct care providers to college students and tend to be of this demographic. In other words, males and physicians were not excluded. In total, 14 full-time students, 4 men and 10 women from one of the public universities, participated in the interviews. Their ages ranged from 20 to 25 years (mean, 22.5 years), and 3 of the 14 were graduate students. The median number of visits to any provider in the last year was 3, with a range of one to five times.
There were three major themes that emerged from the analysis of the provider surveys: (1) communication with students takes time and consideration, (2) a “one woman show” from educator to navigator to provider, and (3) uncertainty about student access to health records. These themes and their subthemes are described below. The overarching theme, however, was that providers seek to develop and preserve relationships with student patients via good communication. Most of what providers do and how they currently approach care with their patients (e.g. using phone rather than e-mail, communicating treatment plans verbally, and teaching patients about navigating the healthcare system) are done with the intention of developing or preserving a good patient–provider relationship. Their concerns about open notes (e.g. misunderstandings and offending patients) are things that could negatively impact the patient–provider relationship. Establishing and maintaining a good rapport with patients are important, and the introduction of new technology or procedures that could jeopardize those relationships is not something providers desire.
Theme 1: communication with students takes time and consideration
A subtheme was that providers use verbal instead of written communication. The providers discuss the treatment plan verbally. While most providers mentioned that there are written patient education materials, it appears that these are not used often: I have various teaching sheets in my office that I will hand to the student just to reinforce what we talked about, more from an educational standpoint, but no specific written discharge instructions, unless I write them down myself, which I do on occasion. I can’t say 100% of the time.
Additionally, the providers value their interactions with the students and are satisfied with their patient communication. The providers seem to act in ways to protect the patient–provider relationship; for example, most of them take very short notes (e.g. key words) on the EHR or on paper during the visit, then complete the visit notes after the visit, so as to not detract from their time with the patient.
Theme 2: a “one woman show” from educator to navigator to provider
The first subtheme was that providers see their role as being different from other health centers or practices. NPs at student health centers take on many roles. Their approach to care might be different, given all the hats that they wear. NPs do everything at the health center and differentiate it from other types of clinic offices: … other places have a lot more, um, people doing other things for you. So, you know, like when I go to my primary, … so there is a lot of sort of other stuff that we do. We are sort of like a one man show in a way.
The second subtheme was that providers see themselves as teachers and navigators. The data suggest that providers view themselves as teacher, navigator, and protector of the student. They do things in the visit to help the student navigate the system. They encourage students to obtain their health records upon graduation, teach them about insurance, and they strive to maintain the privacy and security of the student’s data.
The providers see it as a part of their job to teach students about the healthcare system: So one of the big roles I see fulfilling with this student population is really educating them about the healthcare system, how to use it, how to use it appropriately.
Providers also talked about student patients being a part of the team (“patients really should be partners”) and expressed that they would like to see the students become more engaged (“… it would engage students more in their healthcare process … a positive thing to engage them in their own health care”). There was no discussion, however, about how the providers used this approach (i.e. they did not talk about how they used it during the interview).
Theme 3: uncertainty about student access to health records
Providers expressed worry about providing quality care in a limited amount of time. There was uncertainty about open notes. Two subthemes, advantages and disadvantages, illustrate this wavering. For example, a few providers expressed concerns that open notes could generate more questions. Also, a secure messaging function in the portal could allow the student to type questions, which could allow more time to discuss the main reason for the visit but could also generate more follow-up questions later.
The advantage of open notes would be improved patient–provider communication. It was unanimous that the providers thought access to the notes is a “great thing.” There was, however, less clarity on what the specific advantages might be. As a whole, the advantages were about better patient–provider communication: I think it, you know, if you really look at it from just a fundamental … improvement, I think it, it can’t be a bad thing. I think for some of our patients to have access to their records and understand … and take some responsibility and … ownership, I think it is a great thing.
There was a general consensus that English language learner (ELL) students would benefit from being able to read a note or e-mail: It is going to make it easier to communicate with them in e-mail because they can read English better than they can hear or understand or speak it.
The disadvantages of open notes might be the misunderstandings and their negative consequences to providers and patients. Although advantages were discussed, providers had a more unified voice about concerns. Providers were concerned that patients may not understand the medical terminology in their notes. They believed that students will not understand the terms, will have questions, or may become overly concerned. They also wanted to know how students will get those questions answered: I also would be interested in knowing if they had specific questions about something that was in the note, how would they go about getting those questions answered?
Students’ misunderstandings might have a negative impact on the clinician’s relationship with the student. All providers voiced concerns about possibly offending the patient because of the medical terminology in the note. They mentioned terms (e.g. obese) that could be offensive to some patients given the cultural meanings or render some patients distraught when seeing terms with emotional connections (e.g. abortion, sexual assault, and risky behaviors). The providers were worried about patients not returning to see them or not opening up: I’d have to be extra careful about, I mean the majority of patients, I don’t think I document anything that would offend them. But … there are instances where you recommend something and the patient doesn’t want to go with that treatment plan, or you spent maybe an extra-long amount of time discussing something you thought should have been quick. You … have got to admit that kind of expense, like 50% of the visit prepping this or patient declined this. I think that is enough that certain people could get offended by and could cause problems between the provider and the patient.
The providers were concerned about how this would impact not only patients but themselves as well. All providers mentioned time as a concern, mostly the time spent answering questions that open notes could generate after a visit. For example, Right now, to me, it is accountability that I would have to see if I spent all day trying to reply to people, then I would be concerned.
Results from the student interviews
The overarching theme from the student interviews was students’ desire for control over their health, which influences how they manage their health and the healthcare system. This desire for control is illustrated in the two major themes: (1) Gathering information: Web or Family first, provider last and (2) Access provides insight and involvement. Their desire for control is indicated by their positive views on having access to their doctors’ notes (e.g. having access to them could help them be more active and informed participants), but that desire for control may also drive, at least in part, their tendency to use the Web and family members first before they see a healthcare provider.
Theme 1: gathering information: web and family first, provider last
Students indicated strongly that they rely on sources other than the provider to manage their own healthcare decisions and information. They use websites as their go-to source of information before and after an appointment. They access the Web for information to help them decide whether they should make an appointment, to help them prepare for the visit, and to improve their understanding of their health: When they give you the diagnosis, you can also go online and check. If you don’t understand what he is saying, you can say hold on, I need to check this.
Students seek out information from websites or family members, particularly their mothers, to determine what to do about a health issue. They used their sources (Web or family) first, and then go to the provider if necessary: First source is definitely mother, then I look online, then I usually talk to a doctor.
The students also talked about self-diagnosis prior to seeking medical help, suggesting a reluctance to make appointments and a tendency to attempt to treat health problems by themselves unless absolutely necessary. This approach suggests that students have a general concern about their health and a desire to do something for it: Whenever I have a problem I usually call, um, for, if I don’t think it is that serious. Sometimes I will go online and try and self-diagnose, and then if I just don’t know …, if I see symptoms that are extreme diseases like cancer, or whatever, I definitely will call and make an appointment.
Theme 2: access provides insight and involvement
The students indicated that being able to view their health records would help them track their health over time and be in control of their health. The students talked about how seeing their medical record could help them analyze and evaluate their health because they would be able to see patterns. These patterns or data could help them make decisions based on what worked in the past: Because she [healthcare provider] might not verbalize everything she is writing down, so I can see all the records and feel like I have more control.
The students also indicated that viewing the notes would offer them insight into their provider’s recommendation and give them better understanding and would then allow them to be more involved in the treatment plan (e.g. being able to correct communication errors): … There have been times when I think they have misheard me and wrote something different than what I said down in the notes that I would see and correct at the moment, um, but I don’t know if that is true all of the time. They might be with their back turned and they miss what I say. Um, sometimes I think it helps just to see it, and then I can think, ‘Oh, they recommended because they heard this, but I have this instead,’ so maybe the recommendation would be different if we could all sit down and look at it to make sure it is accurate.
While students liked the idea of having access to their providers’ notes, they were concerned about control over their medical record. The theme that no data are secure arose. Students talked about “hackers and hacking” in general and how that could mean that their medical data are at risk: … just because of the risk of that being on the Internet or online access, that kind of thing. Um, it’s dangerous … and for certain things to get out that way. Um, so yeah, if you understand the risk of your personal information being put on the Internet that way, then sure; you should be able to have access to it.
Phase II: survey results
There were 194 students who contacted the study office and were subsequently sent a link to the online survey. Of those, 95 percent (n = 184) were at least 18 years old and completed the consent. The final sample consisted of 178 students who completed or partially completed the survey from both universities. Demographics are displayed in Table 1. The percent of students in the survey study was less White (43% vs 56% and 64%) and more female (68% vs 59% and 37%) than the distribution at the two universities.
Descriptive statistics of the students in the survey study.
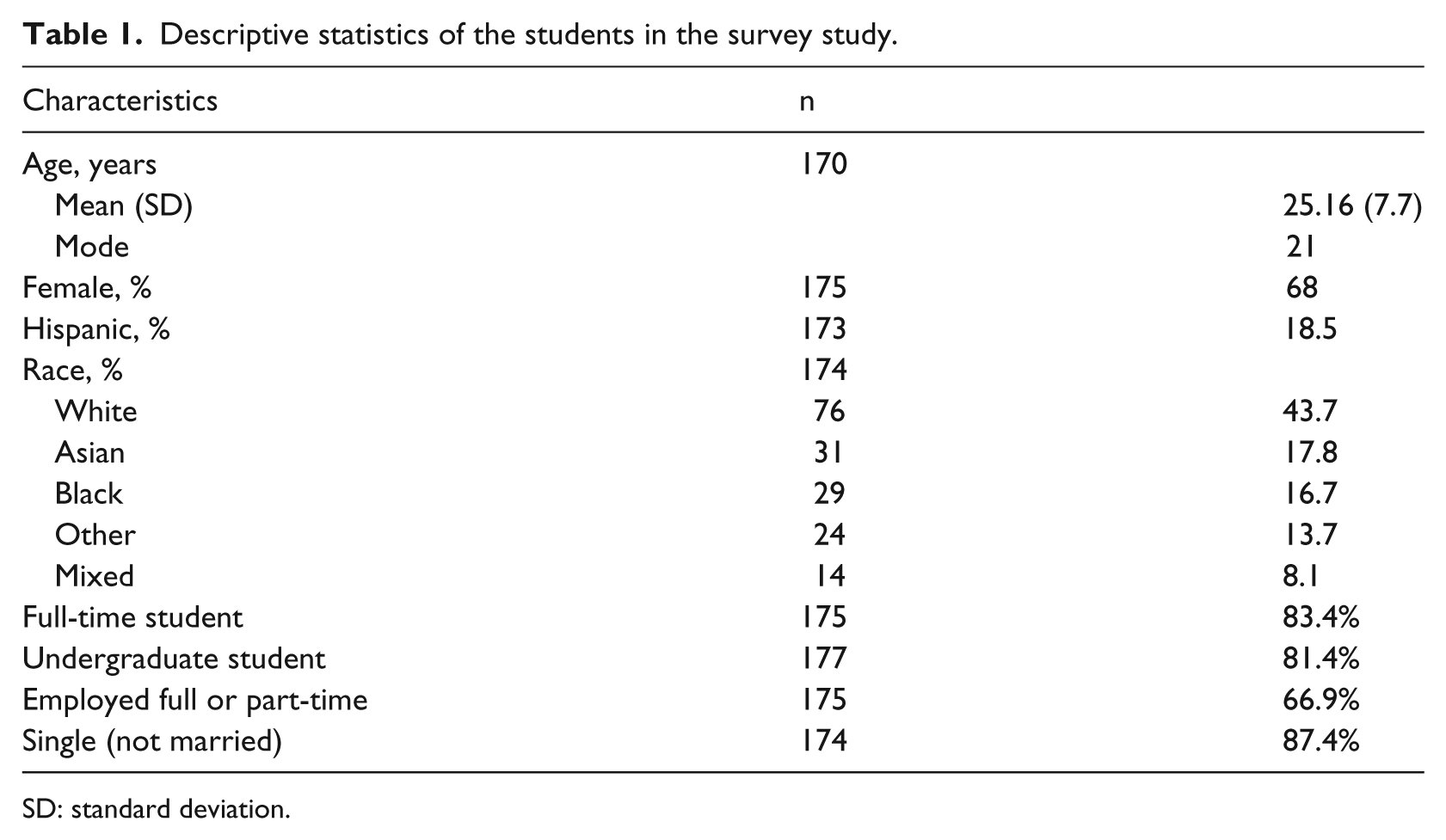
SD: standard deviation.
The majority of the sample, about 80 percent (n = 141), reported having a primary care provider (a PCP, “doctor or nurse practitioner who takes care of your general health”). Of those 141 students who reported having a PCP, 94.3 percent considered their main provider to be outside of SHS. Of the 178 respondents, 92 percent reported a visit to any provider within the last 12 months, and 41 percent (n = 73) reported at least one visit to SHS in the last 12 months. The majority of those who visited SHS reported more than one visit (51%). Of the 178 students, 89 percent reported owning a smart phone, and about 40 percent reported accessing the Internet at least once a week to obtain health information for themselves or someone else.
Student attitudes and beliefs. Table 2 displays the perceived benefits and risks of open notes for those students considered “users” of healthcare. The vast majority of respondents (93%) reported that gaining access to their health records would help them understand more about their health and medical conditions, and they would better remember the plan of their care. Similarly, 89 percent reported that they would feel more in control of their healthcare.
Proportion of students defined as users of healthcare who agreed or somewhat agreed with statements about the potential benefits of open visit notes for patients.
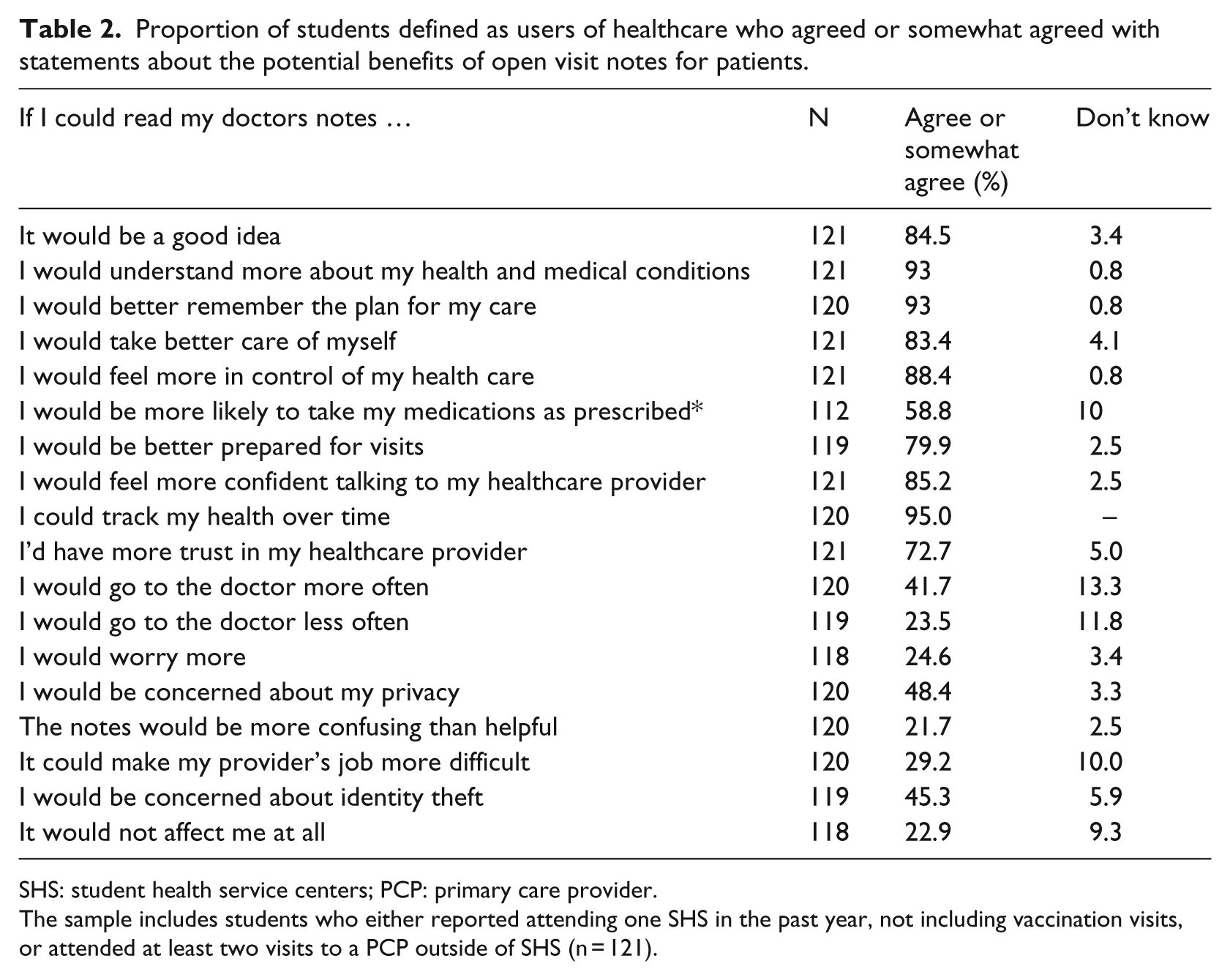
SHS: student health service centers; PCP: primary care provider.
The sample includes students who either reported attending one SHS in the past year, not including vaccination visits, or attended at least two visits to a PCP outside of SHS (n = 121).
Fewer students agreed with statements about risks of open notes. Less than one quarter of participants reported that open notes would make them worry more (23%), and only 21 percent said open notes would make them go to the doctor more frequently. The biggest concerns were identity theft (47%) and privacy (49%).
Comment
The findings of this mixed-methods study suggest that the attitudes about the concept of open notes in college health are generally positive with some uncertainties. Provider and student interviews resulted in contrasting sets of attitudes about access to the visit notes. While provider interviews indicated that open notes would improve communication, stronger themes emerged about the potentially negative impact open notes might have on the patient–provider relationship and the probability that students might not understand the medical terminology used in the notes. In contrast, students had confidence that websites help them understand the medical terminology used by providers. Student interviews and surveys indicated more positive attitudes about open notes. They believed that open notes would allow them to access information that could help them understand and track their health and be more involved in their care. Their main concerns were about privacy and security of their online medical data.
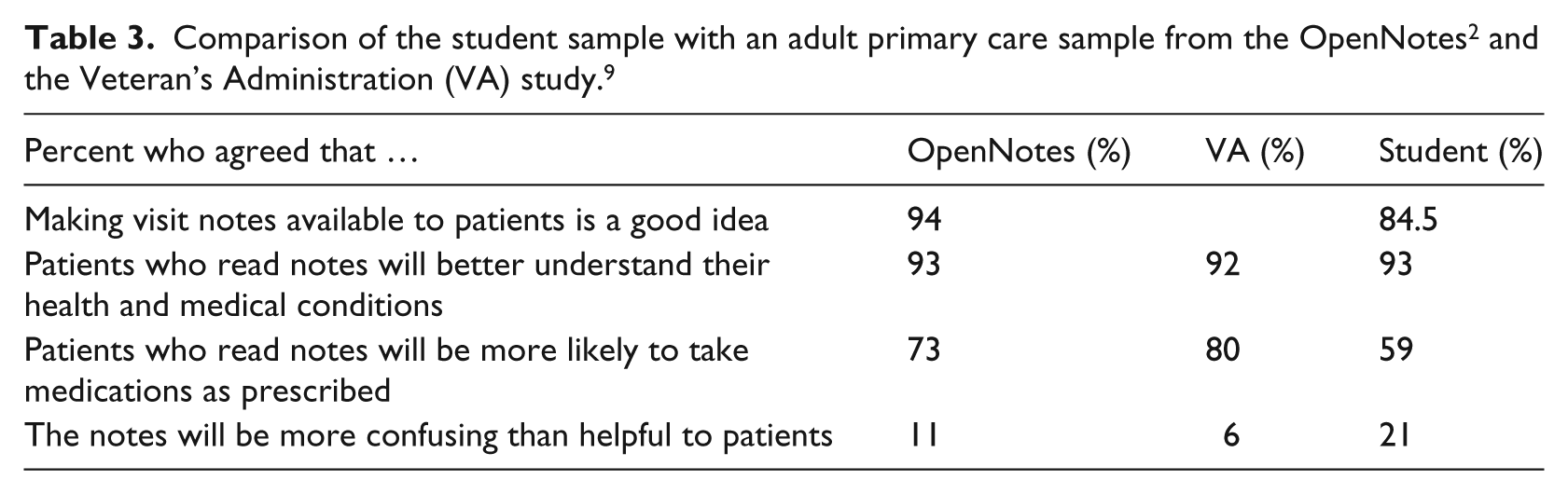
Students in this study overwhelmingly reported that having access to visit notes was a good idea and believed the notes would help them remember their plan of care. These results are consistent with earlier studies in adult primary care.2-4 Table 3 displays a comparison of this study’s findings to the OpenNotes 2 and a more recent study at the Veteran’s Administration (VA). 9 All of these studies used the same OpenNotes survey. 2 However, the VA study included nearly 7000 respondents who had already viewed at least one open visit note (“early adopters”) through the VA patient portal, MyHealthyVet, 9 which is in contrast to the OpenNotes and the present study where the respondents did not have access to open notes. Three out of four early adopters reported they were very satisfied with open notes (rating 8 out of 10 on a 10-point satisfaction scale). Although the VA patients had actually viewed open notes, their attitudes were similar to those reported by patients in the initial OpenNotes Survey, that is, patients’ attitudes prior to having access to open notes 7 and the students. The largest difference appears to be with whether open notes would be more confusing than helpful to patients. Although the percentages were low, 21 percent of students thought the notes would be more confusing than helpful compared to 11 and 6 percent of the OpenNotes and VA patients, respectively.7,9 Another difference was the lower percent of students who agreed (59%) that they would be more likely to take medications as prescribed if they read the notes compared to the other open notes studies, 73 and 80 percent, respectively. This question may not be as relevant to students who most likely to take fewer medications than VA and primary care patients. Overall, these comparisons suggest that although demographically different, students perceive open notes in similar ways. It will be important to examine whether students report fewer worries or less confusion once they have access to their visit notes.
Similar to our study, others have reported patient concerns about privacy and security related to having access to their medical records online.4,7,11 In the original OpenNotes survey, 34–38 percent of patients responded that they had privacy concerns in anticipation about open notes. 7 In a later report, once patients had seen at least one note, 26–36 percent of patients reported privacy concerns, reflecting no material change in this area of concern. 4 In this study, about half of the students reported concerns about privacy in regard to the possibility of accessible medical records. Students have grown up in the age of great transparency through the Internet; in some ways, their attitudes may be more relevant given the frequent media reports of massive security breaches. Such concerns, however, may not have any effect on whether students decide to view their notes through the patient Internet portals. Indeed, a study of privacy concerns among OpenNotes patients came to a similar conclusion, 9 reporting that patients felt that the benefits outweighed the risks of having accessible visit notes.
Although students’ attitudes toward open notes were generally positive, a small percentage of students agreed that it might lead to worry or confusion, or that it would create more work for their providers. This concern was echoed in the themes that emerged from the provider interviews. Providers were more specific in voicing their concerns about open notes and were more ambivalent about the benefits. They used general statements about the benefits like “transparency is a good thing,” or said that patients taking “responsibility” and “ownership” was a “great thing.” In contrast, they described more specific situations where they could foresee open notes either causing more work for them or affecting the patient–provider relationship in a negative way. Providers expressed greater concerns regarding patient access to notes than did patients.
Providers viewed their student populations as fairly healthy, in general, with issues mostly related to risky behaviors or sexually transmitted infections (STIs). Statistics from the American College Health Association (ACHA) suggest that the greatest health concerns are alcohol, tobacco and other drugs, sexual health and mental health, along with weight, nutrition and exercise, and personal safety and violence. 10 Providers in this study echoed these health issues as priority among their patients. At this time, it is unknown how open notes will influence the quality of care or patient engagement among the college population. Furthermore, given that college students may have fewer chronic care needs than the general population, their encounters with the healthcare system tend to be more acute or episodic in nature. These acute healthcare issues can provide opportunities for students to learn about the healthcare system and how to utilize resources, including how to go about filling prescriptions and completing insurance procedures. The findings from our provider interviews suggest that student health providers differentiate their role from the typical primary care clinician in the community. They see themselves as teachers and navigators, primarily educating students about various aspects of their health and healthcare.
An open notes system could include an option to allow family members or other healthcare providers to view a note. As students transition from childhood dependency to independency, they may be more likely to consult other people about their health issues. Students could benefit from such an option in the electronic record system by having the ability to share their records while conferring with trusted adults about their healthcare. Of the students in this study who thought they might share their records with others, many chose a parent or healthcare provider as the person with whom they would share the information. An area of great interest in adolescent and young adult healthcare research is the transition from pediatric care to adult care. The students’ opinions seemed to express that access to open notes would help them be in control of their health. The strong themes that emerged from the interviews suggest that providers value teaching and guiding the students and they strive to help them learn to be independent adults who are able to manage their own health. The providers also value communication with their student patients to the extent that they do not want to jeopardize the patient–provider relationship.
Another potential benefit of open notes for the student population is that it may help in managing students’ back and forth lifestyle in regard to their healthcare. Students tend to rely on student health services during the academic year and then return to their PCPs at home during school breaks and in the summer. An open notes system would help improve communication and facilitate care from provider to provider if students could print notes from the portal website and bring them to their healthcare provider at home. This benefit, however, was not identified by the providers we interviewed. Their current approach with students appears to be more education-focused, guiding students through acute episodes rather than encouraging students to take more active roles in managing their own care. This incremental approach described by providers is understandable because students need knowledge and experience first before being able to take control over their healthcare. In addition, development-wise, they may need to gradually transition into assuming responsibility for their own healthcare; thus, their years in higher education is an optimal time to do so. The question remains, however, how to best accomplish this with busy student and provider schedules. Open notes may be a viable facilitator to assist students in assuming more responsibility with their healthcare and may increase engagement in the future; however, the true impact of open notes in student health is yet to be determined.
Limitations
This study was conducted in a very diverse student population at four public universities in the Eastern Massachusetts and, because of the variety of recruitment methods used, we cannot conclude that the participants were representative of the broader student populations on these campuses. Nonetheless, the diversity of the student respondents reflects the diversity of the participating campuses. Similarly, only a small group of providers were interviewed for this study and they were relatively homogeneous which may be secondary to a high number of female NPs practicing in college health. It may be that their views do not represent the majority of student health service providers limiting transferability. Although our findings cannot be generalized to the campus populations or other college populations, this is the first study to explore student and provider attitudes toward open visit notes. It is important to begin to understand expectations and the potential impact of open visit notes, which are likely to become available through most university health services in coming years with the expansion of secure patient Internet portals.
Conclusion
This study was one of the first conducted to determine the attitudes and expectations of college students and college health providers regarding patient access to medical records, provider visit notes, in particular. The findings suggest that the attitudes and beliefs of the college population are not different than other general adult patient populations with vastly different demographic characteristics, including veterans and adults in primary care who already have accessible records. Students want to be able to view their records, and they indicate that it would help them take control of their own healthcare and help them understand it better. While the actual benefits and risks of open notes in the college health population remain unclear, the potential risks appear to be modest and do not outweigh the potential benefits. Implementing open notes may potentially help young adults effectively manage their own healthcare, an important step in the transition from pediatric to young adult care.
Footnotes
Appendix 1
Appendix 2
Funding
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.