
Abstract
The psychosocial effects of web-based information have yet to be tested for patients joining a fast-track total hip arthroplasty programme. This study compared and evaluated the psychosocial impact of standard total hip arthroplasty programme, with and without supplementation with a web-based information platform (E-total hip arthroplasty programme). Totally, 299 patients were enrolled in an un-controlled, before-and-after study, 117 in the S-total hip arthroplasty programme group and 182 in the E-total hip arthroplasty programme group. Psychosocial outcomes before and during admission and then 3 months post-surgery were evaluated, with analyses conducted between and within groups. All outcomes improved significantly from pre-admission to 3 months post-surgery, with no between-group differences. In all, 112 of the 182 E-total hip arthroplasty programme patients accessed the learning platform. A subgroup analysis showed no significant differences between users and non-users, either at baseline or in terms of outcome. This study found no positive psychosocial effect between groups, but a significant effect within groups.
Introduction
Web-based health informatics using animated information has the potential to reduce the complexity of preoperative information, thereby improving the mental health of patients undergoing surgery. However, this expectation has yet to be tested for patients accessing a fast-track total hip arthroplasty (THA) programme, which presupposes comprehensive educational and mental resources.1,2 The most common indication for THA surgery is arthrosis, with complaints of hip pain and reduced functional ability. 3 Demand for THA procedures is expected to increase in the future as a function of greater physical activity, together with an expectation among elderly patients of an improved quality of life. 4
In 2001, Wilmore and Kehlet 5 were the first surgeons to describe the concept of fast-track treatment. Later, they described fast-track regimes as a treatment which ‘focuses on enhancing recovery and reducing morbidity by implementing evidence in the fields of anaesthesia, analgesia, reduction of surgical stress, fluid management, minimal invasive surgery, nutrition, and ambulation’.6,7 Thus, fast-track treatment focuses on optimising the preoperative education of patients, attenuating their surgical stress response, optimising pain relief, enforcing mobilisation, nutritional support and the provision of up-to-date postoperative nursing care and rehabilitation.8,9 In this way, a fast-track programme aims to optimise recovery, reduce hospital stays and diminish postoperative morbidity.7,10 Patients are encouraged to take an active part in their treatment and rehabilitation and to use the fast-track total hip arthroplasty programme (THAP) as an accelerated intervention that commences during the preoperative period (with an information meeting scheduled prior to admission) and continues through hospitalisation until the day of discharge. 11
Emotional health among patients going through orthopaedic surgery has an influence on physical recovery post-surgery. 11 Preoperative anxiety is a well-known and recognised mental state which influences cognitive ability.12,13 Reducing anxiety may therefore help to improve learning ability, 14 and improving informational level and mode may reduce anxiety.14,15 Thus, learning capacity and mental health are mutually reinforcing, a consideration which should be ‘factored-in’ to current practice in health education.
In line with this, a review on computerised cognitive behavioural therapy (CCBT) has documented success by providing patients with non-catastrophic images of anxiety-triggering processes. 16 Using this technique, animated health information seems to confer some benefit in terms of preoperative anxiety. 17 The visual approach optimises the acquisition of knowledge by reducing data complexity,18–21 as well as minimising cultural and personal differences. Animation using advertising techniques such as light, colour, size and music also confers beneficial effects in terms of attentiveness to the displayed material and knowledge retention.18,20,21
Thus, web-based and animated information may help to bridge unmet needs in health literacy,22,23 given that both media types improve learning irrespective of health literacy.20,24 Furthermore, strengthening health literacy correlates positively with improved learning ability and a high level of self-efficacy in accomplishing postoperative tasks.25,26
The beneficial impact of pre-surgery animated health information and Internet-based education on patients’ health, especially mental health as well as learning ability, has yet to be evaluated for patients undergoing a resource-intensive fast-track THAP. Furthermore, the identification of clinically relevant predictors of patient anxiety in relation to THAP can facilitate the provision of individualised support to the most susceptible patients. Very few studies have identified such characteristics with a view to their possible influence on fast-track pre- and postoperative processes. 22
Objectives
Our objectives were twofold
First, to compare and evaluate the impact of a standard THAP (S-THAP) with an S-THAP extended with a web-based information platform (WIP) (E-THAP) with regard to chance in anxiety (primary outcome), depression, health condition and self-efficacy from pre-surgery to 3 months post-surgery.
Second, to determine whether anxiety pre-surgery is a predictor to both anxiety during hospital stay and anxiety, depression, health condition and self-efficacy 3 months post-surgery.
Methods
Design and setting
Our study incorporated an un-controlled before-and-after design and was hosted from September 2012 to October 2014 at an elective surgical centre in a Danish hospital, which performs approximately 700 THA procedures annually. A fast-track THAP, in accordance with the fast-track criteria described by Kehlet and colleagues,5,7 is practised at this centre.
THAPs
For S-THAP, the expectation is that patients are discharged the day after surgery, which leaves relatively little time in which to prepare them for surgery, discharge and post-surgical rehabilitation. In general, the time frame from setting the date of surgery in the outpatient clinic, to the day of surgery, was approximately 2–3 weeks. Patients were informed about their surgery at the outpatient clinic by a surgeon, and then by a specialist nurse. The nurse also provided a 36-page pamphlet to patients who were advised to read it thoroughly before attending the information group meeting, 1–2 weeks prior to surgery. Patients as well as relatives were invited to this 2-h meeting, which included oral and written information, together with a power-point presentation of the THA procedure and postoperative recovery. A clear division of pre- and post-surgery tasks between patients, their relatives and healthcare professionals was emphasised as a prerequisite for achieving a successful surgical outcome. 27 Throughout the programme, starting from the day of their outpatient clinic appointment, and ending 3 weeks after hospital discharge, patients were encouraged to contact their coordinator (a specially trained nurse or physiotherapist) for continuity of care should they have any health-related concerns. The day after discharge, the coordinator phoned patients in order to evaluate their health status. During the third post-surgery week, patients met with a physiotherapist in an outpatient clinic for a final follow-up on functional performance and general health status.
The E-THAP protocol encouraged patients to access a WIP that incorporates an animated video. The platform was available to patients as soon as they had consented to surgery and participation in the study, which was prior to the information group meeting. Each patient received a login and password, and the research nurse subsequently provided hands-on instructions in how to use the WIP. The login was used to verify patient accessed to the WIP.
The visual approach was designed to reduce the complexity of the information and bridge challenges in health literacy. 28 In line with Internet provision of CCBT, 16 our approach was also designed to reduce the risk of developing catastrophic thoughts and misconceptions in relation to surgery. Our animation comprised a 12-min, two-dimensional (2D) video, comprising 10 sequences to explain the THA procedure, from initial symptoms to post-surgical rehabilitation at home. The animation video showed a patient avatar as a middle-aged woman undergoing the THA procedure, with a male voice-over explaining the procedures (Figures 1 and 2).

The avatar model (Silkeborg Regional Hospital, Denmark, 2013. 356 × 200 mm (72 × 72 DPI)).

Pre-surgical interaction. Interaction between avatar patient and health providers during anaesthesia (the animation anaesthesia study, Silkeborg Regional Hospital, Denmark, 2013. 356 × 200 mm (72 × 72 DPI)).
The animation displayed on the platform was divided into chapters mirroring the chronology of the THA. The intention was to offer the patient the advantage of knowledge acquisition in familiar surroundings (at home), 29 at a speed dictated by the patient. 30 Research has shown that paced and repeated information appears to improve learning ability both pre- and post-surgically. 20 Furthermore, the platform held written and audio information, in parallel with animation. Animated instructions for physical exercises, bio-feed-back in relation to pain and pain management and contact information for healthcare professionals in the hospital were provided. Patients could access the platform for up to 3 months after their hospital discharge.
Patient enrolment
The patients receiving standard care, S-THAP (control group), were enrolled consecutively from September 2012 to March 2013. Subsequently, S-THAP was substituted by E-THAP (the intervention group), with patients consecutively recruited to this group from August 2013 to October 2014. The sample size calculation was based on a between-group difference in Hospital Anxiety and Depression Scale (HADS)–Anxiety change (primary outcome) from pre-surgical to 3 months post-surgical of 1.5, defined as the minimal clinical relevant difference according to Puhan et al. 31 With an expected standard deviation (SD) of 3.44, 32 a significance level of 0.05 and a power of 0.80, the required sample size was estimated to be 83 patients for each group.
Due to a possible low response rate in some outcome variables, and to accomplish our secondary aim of performing a predictor analysis, we included a total of 299 subjects in the study. The inclusion criterion was a patient undergoing a primary THA surgical procedure; exclusion criteria included cognitive deficiencies and the inability to speak or understand Danish.
Instruments
The HADS 33 is a validated 14-item psychological screening scale that measures symptoms of anxiety and depression (7 items each) with a score range of 0–21. The recommended cut-off in defining symptoms of anxiety or depression is >7. 33
The Visual Analogue Scale-Anxiety (VAS-A) 34 measures self-perceived anxiety from 0 mm (not anxious), to 100 mm (most anxious). 34 VAS-A is validated 35 with a recommended cut-off at >30 mm.
EuroQoL-5 Dimension Questionnaire (EQ-5D)-3L, including EQ-VAS,36,37 is a 9-item validated instrument that measures health conditions according to the following subscales: mobility, three items; self-care, three items; usual activities, three items; pain/discomfort, three items; and anxiety/depression, three items.36,37 These subscales are divided into three levels of perceived problem: level 1, no problem; level 2, some problems and level 3, extreme problems. A time trade off (TTO) was used to estimate the EQ-5D index.36,37 EQ-VAS measures self-perceived health condition from 0 mm (worst) to 100 mm (best).
The General Self-efficacy Scale (GSES) 38 is a 10-item validated scale to assess optimistic self-belief in coping with a variety of difficult demands in life 38 and is scored between 1 and 4 points, without a cut-off.
Data collection
Data collection pre-surgery and 3 months post-surgery was with a composite questionnaire comprising all instruments (see Figure 3). In addition, VAS-A was measured before admission (prior to the information meeting), just before surgery (at the ward) and again before discharge.
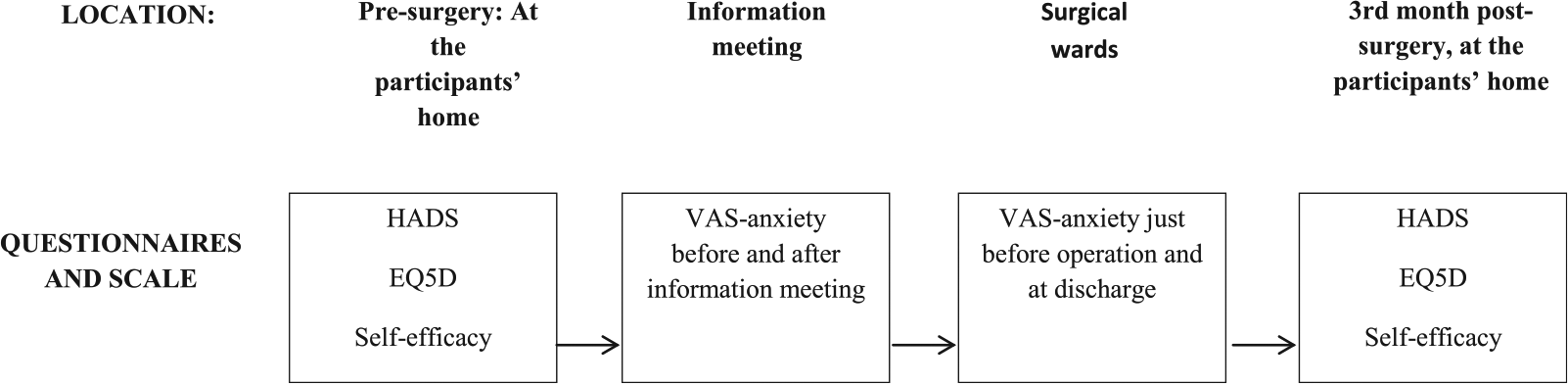
Flowchart of the chronology and location of the data collection process.
Ethical considerations
The Danish Data Protection Agency 39 provided permission to conduct this study (J. No. 2007-58-0010). Given the absence of any biologic tests, no contribution was required from the Scientific Committee for the County of Central Jutland, or the Biomedical Research Ethics Committee. In line with the Helsinki Declaration, 40 patients were informed about the study both verbally and in writing, and all participants gave their written consent to participate.
Statistical analyses and outcomes
Data were double-entered in EpiData 3.1 (Epidata Association, Odense, Denmark), with statistical analyses performed using the STATA 13 software package (StataCorp, College Station, TX, USA). Normally distributed data were described by means and SD, non-normally distributed data, by medians and interquartile range (IQR), with categorical variables described by numbers and proportions. Between-group and within-group differences were tested with an unpaired t test, and a paired t test, or the equivalent non-parametric Wilcoxon rank-sum test. Categorical variables were compared between groups using the chi2 test or Fisher’s exact test for less than five subjects in a category. The primary analysis was a between-group comparison regarding change in HADS score from pre-surgery to 3 months post-surgery. Secondary analyses were (1) a between-group comparison of scores for the remaining outcome variables and (2) a predictive analysis performed for pre-surgical values of VAS-A >30 mm, as the predictive variable (defined as a score >30 mm at a pre-surgery ambulatory visit or information meeting), with scores for outcome variables for VAS-A just before surgery, at hospital discharge and 3 months post-surgery. Due to a substantial proportion of patients not using the platform in the E-THAP group, a subgroup analysis was performed to compare users (those who accessed) versus non-users (those who did not access) of the platform. A log related to each patient’s study number on the platform allowed us to the identify users versus non-users.
Results
A total of 299 patients were included: 117 in the S-THAP group and 182 in the E-THAP group (see Figure 4).
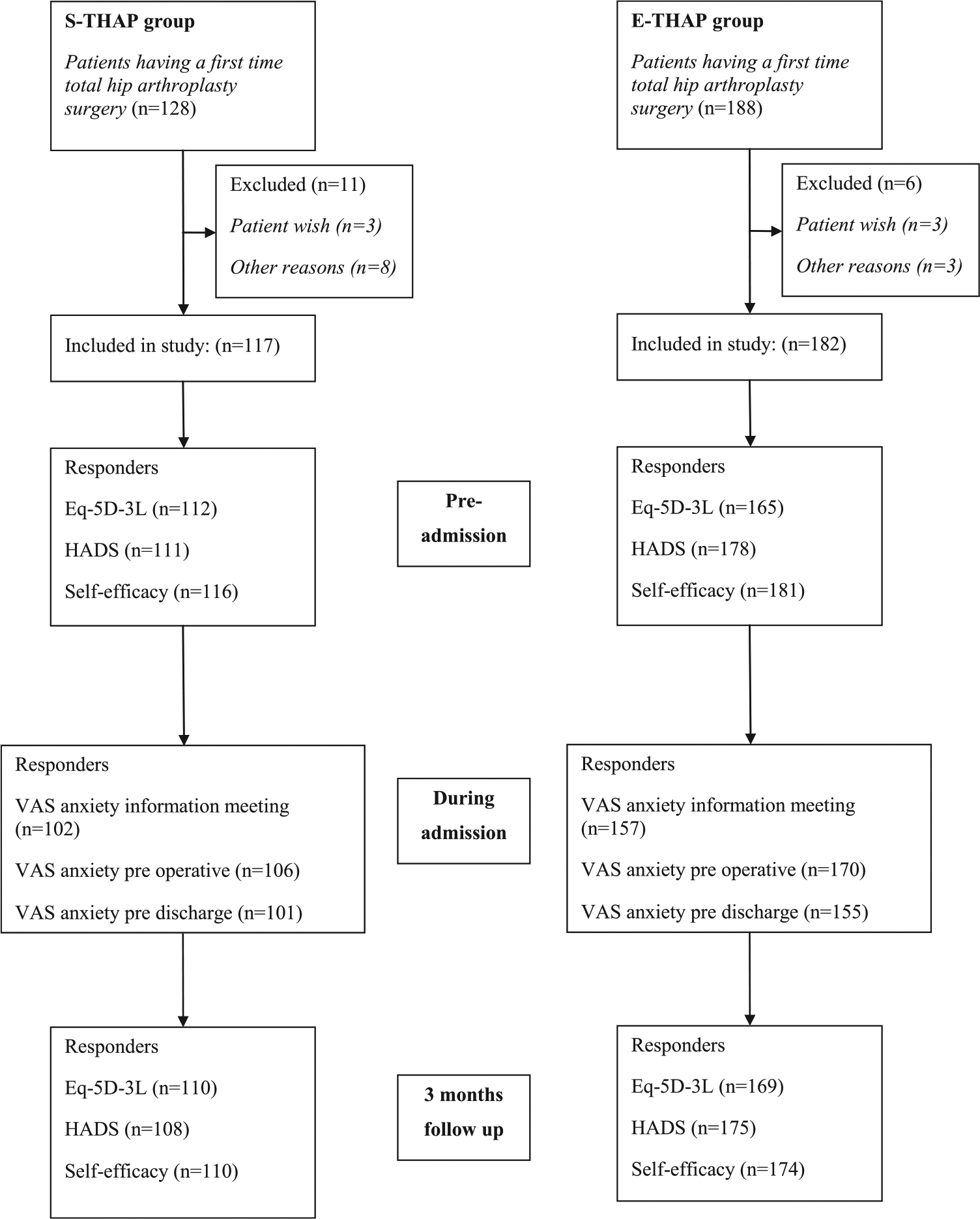
Inclusion and exclusion criteria for participants, with the distribution of responders.
No significant differences on baseline characteristics were found between the groups (see Table 1).
Baseline characteristics for patients with and without access to the web-based information platform.
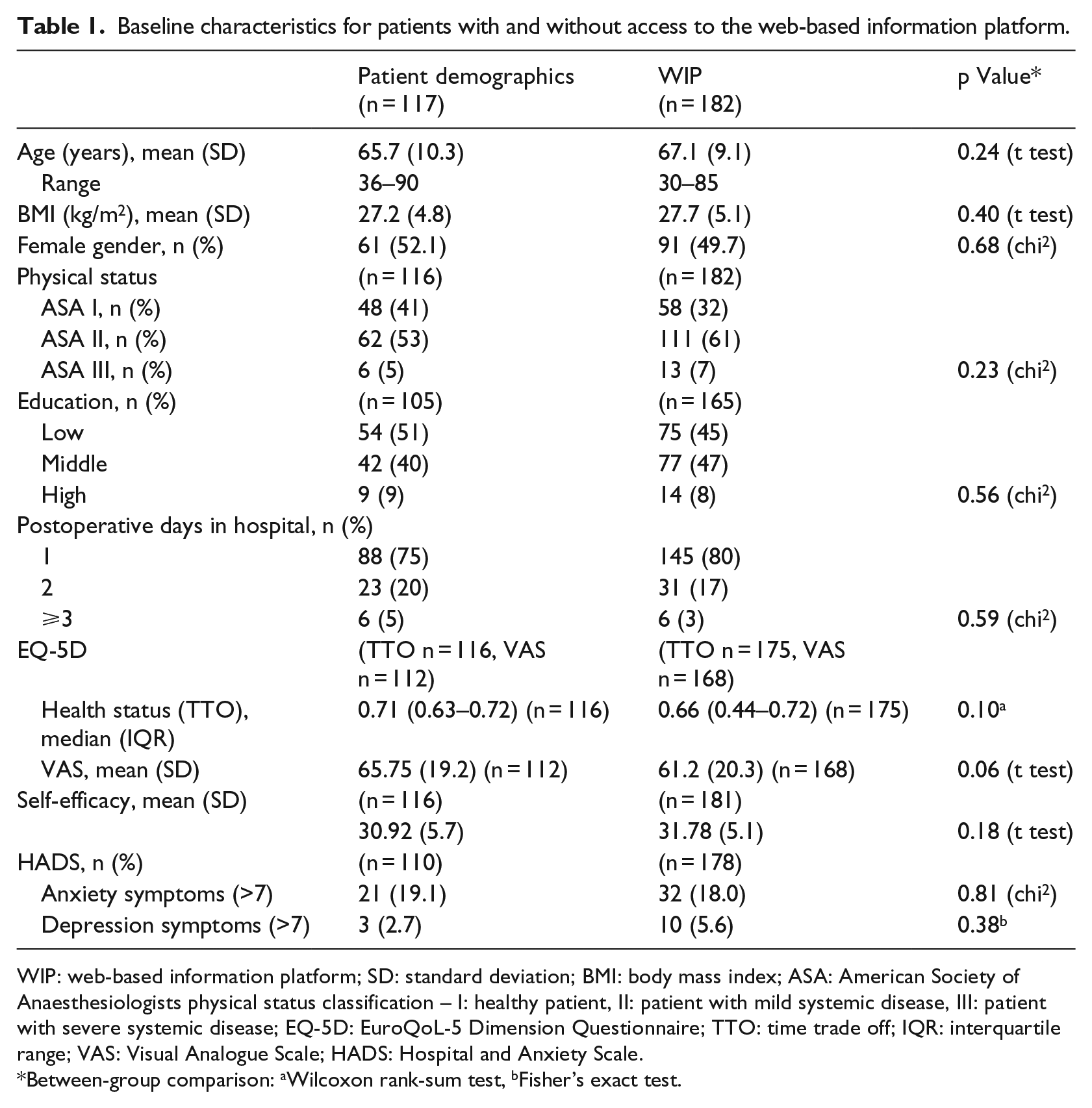
WIP: web-based information platform; SD: standard deviation; BMI: body mass index; ASA: American Society of Anaesthesiologists physical status classification – I: healthy patient, II: patient with mild systemic disease, III: patient with severe systemic disease; EQ-5D: EuroQoL-5 Dimension Questionnaire; TTO: time trade off; IQR: interquartile range; VAS: Visual Analogue Scale; HADS: Hospital and Anxiety Scale.
Between-group comparison: aWilcoxon rank-sum test, bFisher’s exact test.
The effect of supplementing standard information with web-based assistance
On the primary outcome of HADS, there was no significant improvement for the E-THAP versus the S-THAP group (p = 0.06). However, all outcomes improved significantly from pre-admission to 3 months post-surgery within groups, but with no between-group differences as illustrated in Table 2.
Changes from baseline to 3 months postoperative, values are mean (95% CI).
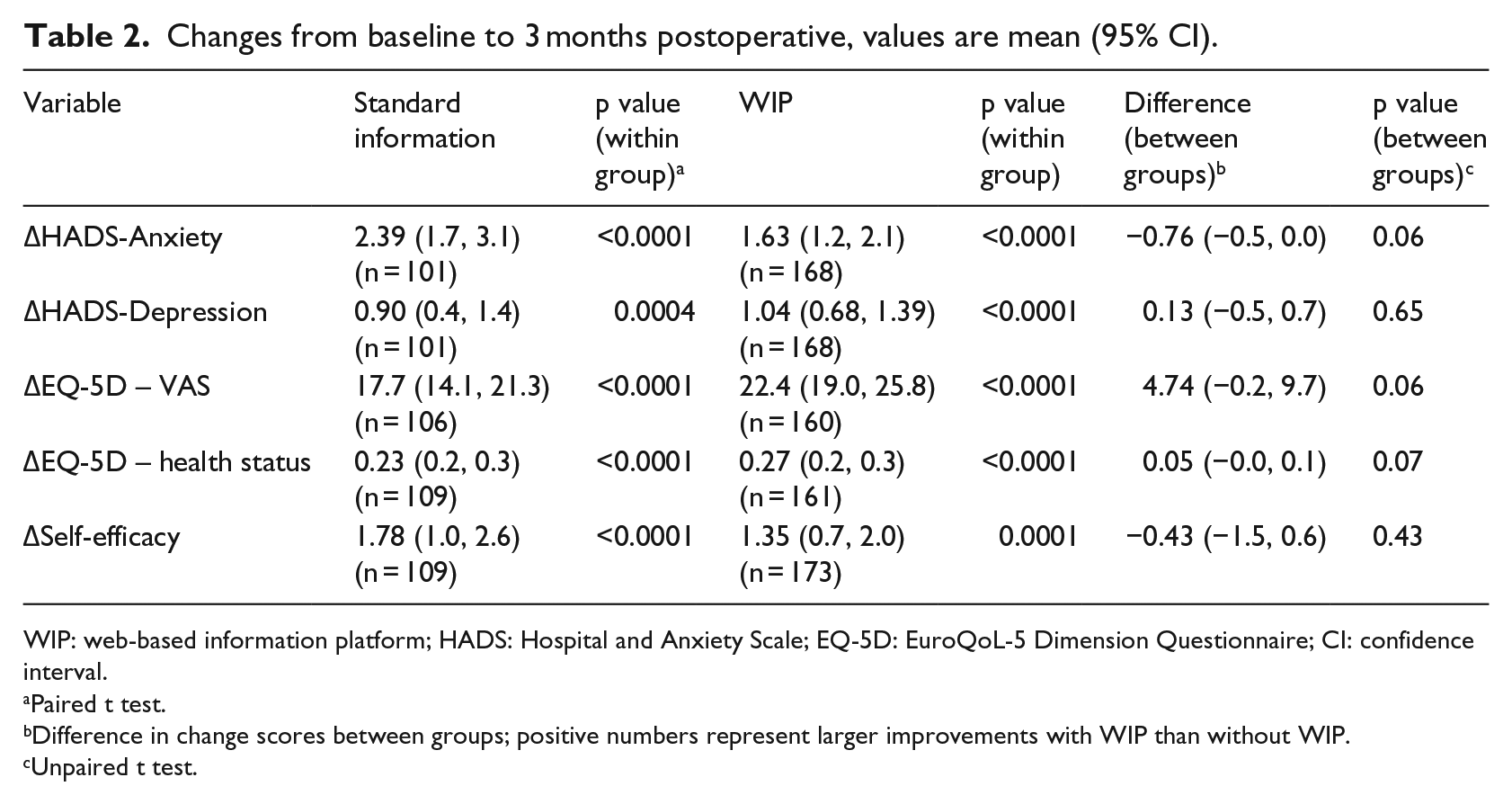
WIP: web-based information platform; HADS: Hospital and Anxiety Scale; EQ-5D: EuroQoL-5 Dimension Questionnaire; CI: confidence interval.
Paired t test.
Difference in change scores between groups; positive numbers represent larger improvements with WIP than without WIP.
Unpaired t test.
Predictor of psychosocial outcomes within groups
As demonstrated in Tables 3 and 4, pre-surgery anxiety >30 mm VAS was associated with a significantly higher level of anxiety just before surgery for both groups (p < 0.0001) and at discharge for the S-THAP group (p = 0.04). Patients with pre-surgery anxiety (>30 mm VAS) demonstrated significantly lower self-efficacy after 3 months compared to those with lower pre-surgery anxiety (⩽30 mm); this finding applied to both groups (p = 0.05), with only small differences in median values for S-THAP (Table 3) versus E-THAP (Table 4).
VAS anxiety as a predictor for psychosocial outcomes in the group with standard information (phase 1) (n = 111, due to six missings on the predictor variable).
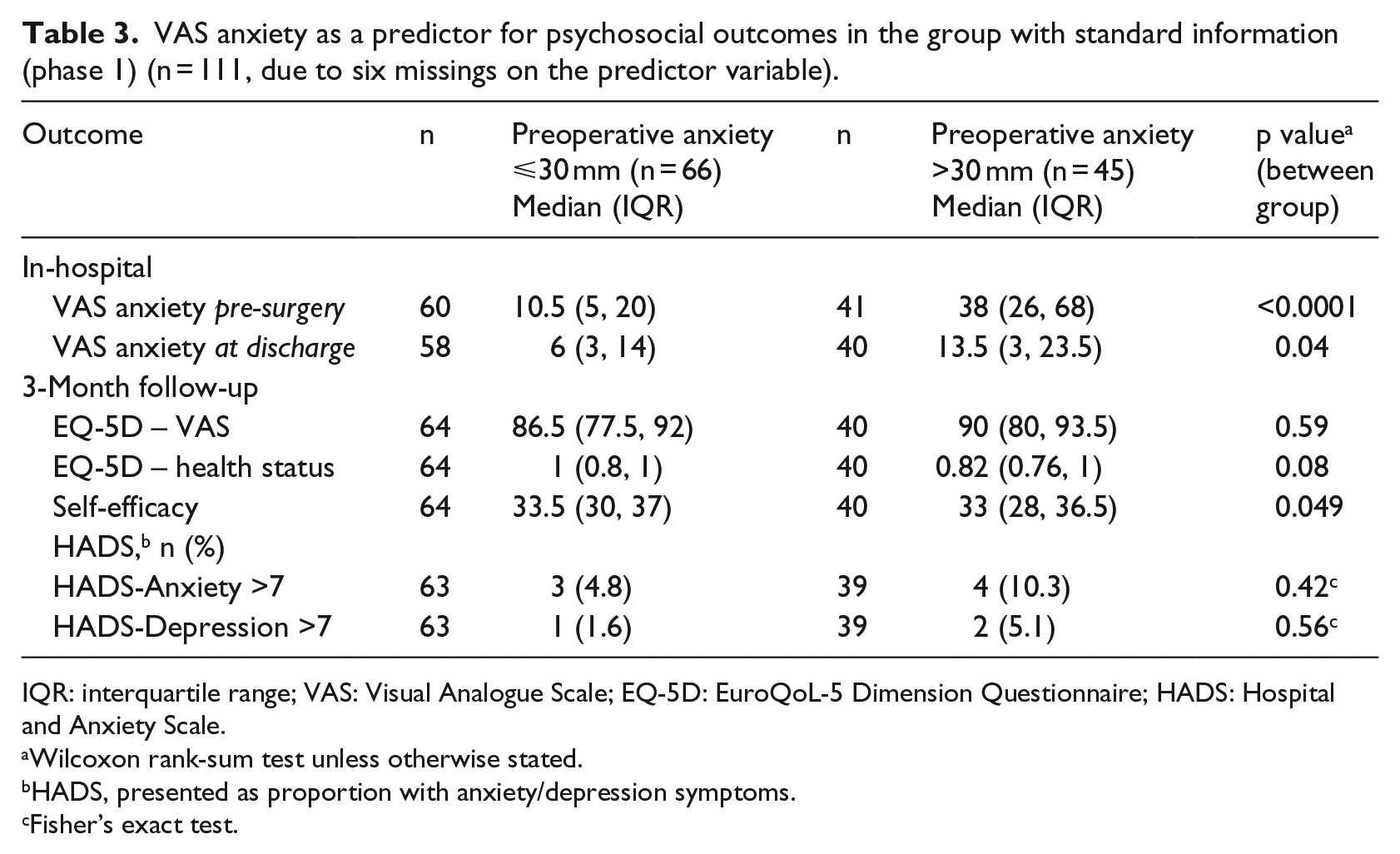
IQR: interquartile range; VAS: Visual Analogue Scale; EQ-5D: EuroQoL-5 Dimension Questionnaire; HADS: Hospital and Anxiety Scale.
Wilcoxon rank-sum test unless otherwise stated.
HADS, presented as proportion with anxiety/depression symptoms.
Fisher’s exact test.
VAS anxiety as a predictor for psychosocial outcomes in the group with WIP (phase 3) (n = 173 due to 10 missings in the predictor variable).
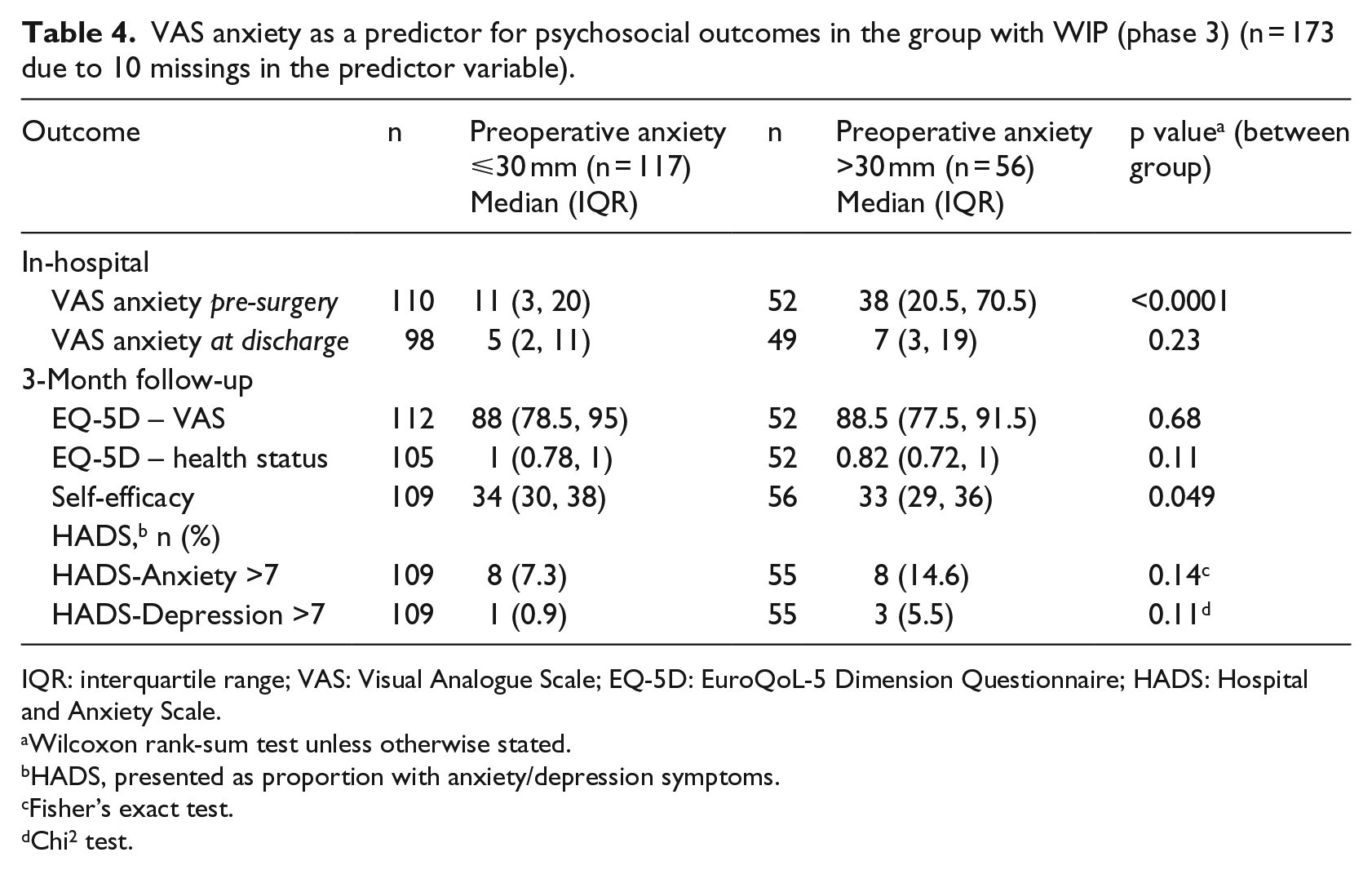
IQR: interquartile range; VAS: Visual Analogue Scale; EQ-5D: EuroQoL-5 Dimension Questionnaire; HADS: Hospital and Anxiety Scale.
Wilcoxon rank-sum test unless otherwise stated.
HADS, presented as proportion with anxiety/depression symptoms.
Fisher’s exact test.
Chi2 test.
As illustrated in Figure 5, a chronologic plot of the anxiety level ‘profile’ between groups was comparable.
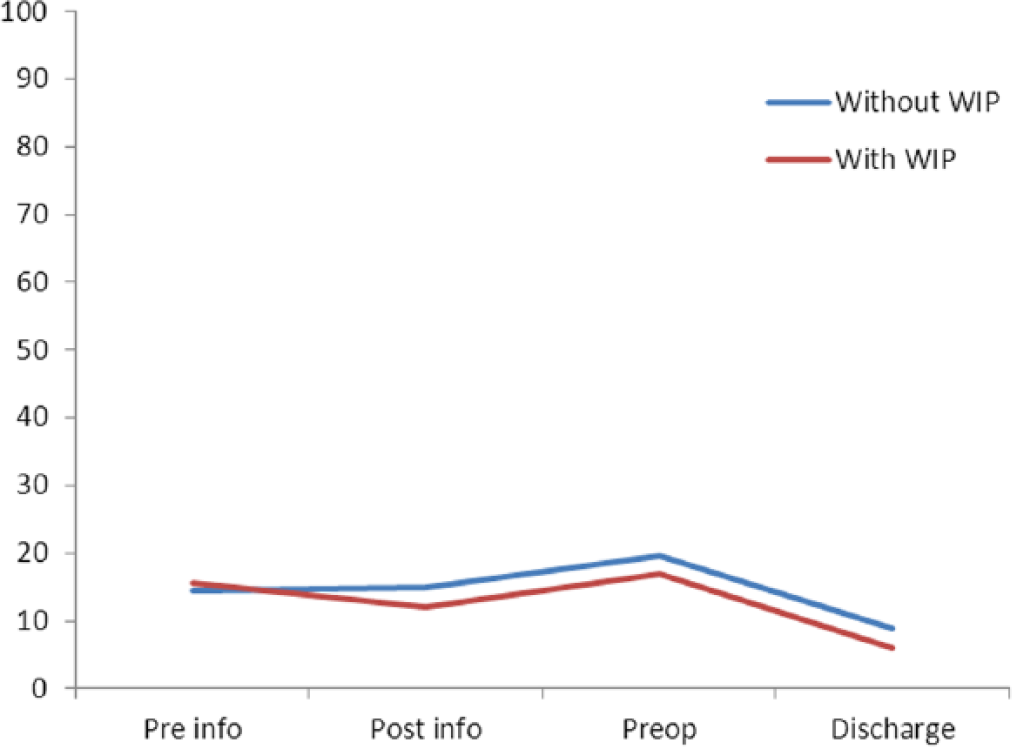
VAS anxiety median scores before and during hospital admission for groups with and without access to the WIP.
When comparing the means for all four measurements of VAS anxiety between groups, there were no significant differences between the overall VAS anxiety level for S-THAP versus E-THAP (p = 0.10) (Figure 5).
Subgroup analysis in the E-THAP group for users and non-users of the WIP
In all, 112 of 182 participants in the E-THAP group accessed the platform. As illustrated in Table 5, a subgroup analysis showed that there were neither significant differences between users and non-users at baseline nor changes in outcome.
Patients in the group with access to WIP, grouped according to its usage.
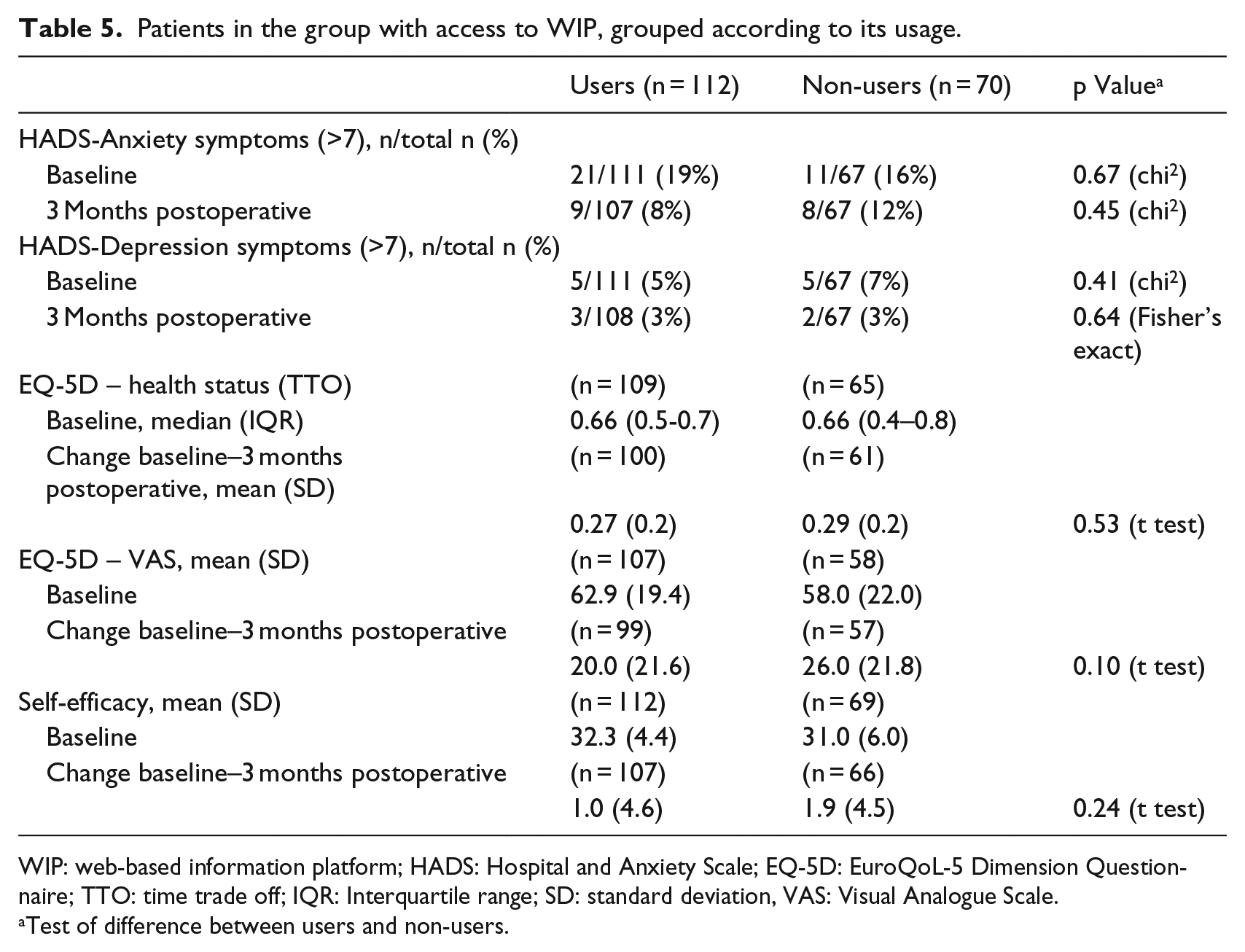
WIP: web-based information platform; HADS: Hospital and Anxiety Scale; EQ-5D: EuroQoL-5 Dimension Questionnaire; TTO: time trade off; IQR: Interquartile range; SD: standard deviation, VAS: Visual Analogue Scale.
Test of difference between users and non-users.
Discussion
This un-controlled, before-and-after study showed no significant psychosocial effects for patients joining E-THAP compared to S-THAP. Any difference between groups in favour of S-THAP was beneath the 1.5 point threshold suggested to indicate minimal clinical relevance. Extensive written preoperative information as used in both S-THAP and E-THAP is a well-known intervention with which to address preoperative anxiety 14 and may explain the lack of any additional benefit when using WIP.
Regarding the didactic elements of the ‘animated information video’, contradictory effects on surgery-related anxiety have previously been reported. Kakinuma et al. 24 reported no beneficial effect on pre-surgery anxiety following the provision of animated information. In contrast, a positive effect was identified by Tou et al. 17 Neither study dealt with orthopaedic fast-track surgical programmes, with measurement times also varying between studies. Interestingly, a beneficial effect conferred by the animated video on learning ability was found. 24 When considering the correlate of mental health and learning capacity, improved learning abilities may, at length, help to diminish anxiety. Patient preferences in terms of self-identification with the avatar used in the animation video may also explain the missing psychosocial effect. Based on the learning theory by Bandura, 41 identification with an avatar may have a beneficial effect on learning ability through the theory of vicarious reinforcement. 41 We conducted an ethnographic study on a subset of the total S-THAP group. 42 Fifteen of the most anxious patients (VAS anxiety >30 mm) were included after 3 months of follow-up. Individual preferences were found for two different narrative models, one speaking from the patient’s perspective and the other with a more formal instructor perspective (i.e. a healthcare professional), as used in E-THAP. The most anxious patients preferred the narration to reflect the patient’s perspective, which contradicts the approach taken in the WIP. Different types of avatar may have also impacted patient cognition, due to their anxiety level. This suggests that individual-specific targeting is appropriate for the didactic components of the WIP, such that these can be aligned with preoperative levels of anxiety.
As all outcomes improved significantly from pre-admission to 3 months after surgery, with no between-group differences, both programmes had positive psychosocial effects. The finding of post-surgical improvement of health status among THA patients is in line with previous findings, 38 and may be related to the surgery in itself, 43 and the extensive preoperative information given. 26 Irrespective of the mode of information delivery, the fast-track concept, with clear expectations of operative course, rehabilitation and patient agency, contributes to the success of THA.
Having preoperative anxiety >30 mm VAS was associated with significantly higher anxiety levels during admission in both groups, significantly lower self-efficacy in postoperative tasks after 3 months for both groups and a significantly higher anxiety level at discharge in the S-THAP group. Previous studies have shown that anxiety measured in the anxiety/depression dimension of EQ-5D is a strong predictor of pain and satisfaction after total hip replacement surgery. 44 Additionally, anxiety is a predictor for pain, opioid consumption and level of function pre- and post-surgery. 14 , 44 Identifying those patients who are most preoperatively anxious is therefore of clinical relevance in a resource-demanding fast-track setting, for which success is contingent on a sufficient level of mental and educational patient resources. The validity and reliability of using the VAS anxiety score to determine pre-surgery anxiety, and as a predictor for a patient’s mental state while participating in a fast-track programme, must be further studied.
A subgroup analysis showed no significant differences between users and non-users at baseline and in terms of outcome. However, a trend was evident with respect to a larger positive change in HADS-anxiety for users compared to non-users. Conversely, non-users seemed to have slightly larger improvements for the remaining outcomes, suggesting no overall positive effect from use of the WIP. Providing a pamphlet with extensive information for both groups may have had the effect of influencing some participants not to access the WIP. However, different perceptions of usefulness (i.e. utilitarian motivation) may have influenced the choice of whether to access the WIP, as reported for users and non-users of a mobile application. 45 More information on individual preferences are needed 45 before any firm conclusions can be drawn; these may contribute to our ability to predict how and why groups chose to engage with different modes of health informatics.
Despite no psychosocial effect of the intervention, animated information is still used in the department as former THA patients with a VAS-A >30 mm find the information trustworthy and the displayed THAP recognisable. 42 The department is continuing to study the effects of WIP for patients undergoing THAP and other surgical treatments.
Study limitations
Compared to a randomised controlled design, this un-controlled design may have compromised data quality given its suboptimal ability to measure the effect of a given intervention. However, the choice of this study design was predicated by economic and logistic considerations, as a randomised study would have required a greater staff allocation, with duplicated in-parallel information meetings, and separate wards.
The un-controlled design also introduces a risk of bias due to the unequal distribution of confounding factors between groups. However, these quality flaws may be compensated for by the consecutive recruitment as well as baseline characteristics, which indicated equal distributions, at least among the measured variables, and support the validity of our finding of no significant effects of the E-THAP programme on psychosocial outcomes. The size of the study, which complied with a sample size calculation, also strengthens its validity. However, missing data, as indicated in Figure 4, is a weakness.
In this study, multiple comparisons were made which increases the risk of type I errors. Consequently, the significant differences that we found should be interpreted with caution and in relation to the clinical relevance of the findings. All questionnaires used in the study are validated and commonly used in studies for patients undergoing THA. 32 ,44,46
Conclusion
This study documented improved psychosocial effects for fast-track THAP, with no additional effect of web-based and animated information. Anxiety was a possible predictor of a higher anxiety level during hospitalisation and lower self-efficacy post-surgery. Using VAS-A to identify the most nervous patients must now be tested in a further validation study. Likewise, an evaluation of the psychosocial effect of E-THAP should be conducted in a randomised controlled trial, taking individual coping preferences as well as avatar preferences into account. Identifying utilitarian motivational factors may be necessary to improve our understanding of the psychosocial benefits of E-THAP and allow us to target fast-track THAPs that incorporate psychosocial challenges.
Footnotes
Declaration of conflicting interests
The author(s) declared the following potential conflicts of interest with respect to the research, authorship, and/or publication of this article: Co-author Martin Vesterby is a co-founder and partner of Visikon Inc. that produced the animation video used in the study.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.