
Abstract
Objective
Pregnant women and unborn babies are at increased risk of complications from influenza, including pneumonia, yet in the UK, uptake of flu vaccination amongst this population remains <50%. Pregnant women hold beliefs about risks of flu and efficacy of vaccination that consistently predict them to decline vaccination. This study aimed to develop a theory and evidence-based intervention addressing these beliefs to promote flu vaccine uptake.
Methods
The intervention was developed by behavioural scientists, pregnant women, midwives, clinicians and Public Health professionals, informed by Intervention Mapping. Six predefined steps were performed in line with Intervention Mapping.
Results
The intervention is an animation addressing beliefs about risks of flu and efficacy of vaccination. Preliminary testing using qualitative methodology indicates the information within the animation is appropriate, and the animation is acceptable to pregnant women.
Conclusions
This is the first known intervention for pregnant women, aiming to increase flu vaccination through addressing risk and efficacy appraisals. It has been implemented within seasonal flu vaccination campaigns during 2018/19 and 2019/20 within one geographically and ethnically diverse area of the UK.
Keywords
Introduction
Due to physiological and immunological changes associated with pregnancy, pregnant women are at increased risk of serious illness, hospitalisation and mortality because of associated complications. 1 Maternal flu also has serious implications on the health of the unborn baby, increasing the likelihood of stillbirth, neonatal death, premature birth and below average birth weight. 2 Since 2010, pregnant women in England, and in the whole of the UK have been classed as an at-risk population by the Joint Committee on Vaccination and Immunisation (JCVI) 3 and are routinely offered annual, free flu vaccinations. Flu vaccinations have been proven to be safe at any stage of pregnancy 4 and generally have a good record of effectiveness. 5 Despite this, uptake of the seasonal flu vaccination amongst pregnant women has consistently fallen short of the 75% target since it was set, with only 45.2% of pregnant women receiving the flu vaccination during the most recent 2018-19 flu season in England. 6 Socio-demographic factors may impact the uptake of flu vaccination.
Previous literature has shown that pregnant women who are of non-white ethnicity, at or below the poverty line, and with a lower educational level were less likely to receive the flu vaccination.7–9 Other barriers to vaccination amongst pregnant women include fears around the safety of the flu vaccination, including perceived risks to themselves or their unborn baby,2,7 a lack of recommendation from a GP or midwife,2,9,10 and differing organisational strategies and interventions offered by healthcare providers.11,12
Risk appraisals are defined as ‘people’s beliefs about a potential harm’. 13 Health Psychology theories (such as the Health Belief Model, 14 Protection Motivation Theory, 15 and the Extended Parallel Processing Model 16 ) propose that protective behaviours can be increased through increasing individuals’ beliefs about the risk of harm. Recent meta-analytic evidence indicates that increasing risk appraisal may be a potentially effective way to increase vaccination uptake albeit with small effects.17–19 Efficacy appraisals are perceptions made by an individual, consisting of response efficacy; the ‘ability of the recommended behaviour in reducing the threat’, and self-efficacy; ‘beliefs about one’s ability to perform the risk-reducing behaviour’. 13 Health Psychology theories suggest that under circumstances where the target populations’ efficacy appraisals for the recommended behaviour are either low or unknown, efforts should be made to increase these in conjunction with risk appraisals to avoid occurrence of a counterproductive effect on the health behaviour.15,16 This counterproductive effect is theorised to occur when people’s beliefs about the risk of harm are heightened but they feel either unable to perform the required behaviour to remove that threat or that the recommended action is ineffective.
Technology use and accessibility is advancing rapidly, with 87% of all adults using the internet daily or almost daily during 2019, and with almost two thirds of households in the UK having access to mobile broadband. 20 These statistics reflect growing acceptability and familiarity with the internet, indicating that digital interventions are likely to be an engaging and wide-reaching mode of delivery for health interventions. Advantages of digital interventions include the flexibility of delivery (both in terms of location and time) and anonymity. 21 Furthermore, digital interventions have been found to be effective in reaching people who are less inclined to access face-to-face interventions, and when the content is of a sensitive or personal nature. 22
In addition to evidence indicating that digital interventions are likely to have good reach, recent research has also demonstrated their efficacy in increasing the uptake of a range of health promoting behaviours including smoking cessation amongst pregnant women, self-management of asthma symptoms and physical activity and diet in cancer patients.23–25 Interventions using digital methods of delivery expand the possibilities of communicating risk information, and have the advantage of easy distribution and wide reach due to the pervasive nature of internet use.
Previous research shows that risk messages that are visual and engaging are more effective in changing appraisals of risk. 26 In addition to this, risk information that is provided purely statistically, is not reliably understood. 27 The use of an animation or video providing narrative and engaging material, rather than listing facts and statistics alone, is likely to be an effective approach to motivate a change in behaviour. Interventions that use vivid images and scenario based information, have been shown to be more effective at increasing appraisals of risk, and the subsequent adoption of preventative behaviour.28,29 Furthermore, visual content may elicit feelings such as worry about the potential dangers flu can cause. In line with the Risk as Feelings theory, engaging with a visual intervention may trigger anticipatory emotions which motivate the individual to carry out the protective behaviour, 30 which in this case may encourage the individual to make the decision to have the vaccination. Such interventions can include visual and engaging elements, and have the potential to trigger anticipatory feelings of worry, making a visual intervention a reasonable format for an intervention to target flu vaccination uptake amongst pregnant women.
In 2014, Coventry University was approached by Warwickshire County Council (WCC) and Coventry City Council (CCC) public health departments and commissioned to develop an animation for pregnant women on flu and the flu vaccination. The aim specifically was to develop an intervention (in the form of an animation) that could be used as one part of a wider annual flu vaccination campaign to increase flu vaccination uptake locally amongst this at-risk population. Uptake across Coventry and Warwickshire is similar to national uptake, with 48.4% of pregnant women receiving the flu vaccination during 2018/19 in Coventry and Warwickshire. 31 Involving the target audience in the design and development of an intervention (also known as co-design), has been shown to result in improvements in the relevance and appropriateness of the finished intervention. 32 This article describes the development of the animation; the first known intervention aiming to increase the uptake of the flu vaccination amongst pregnant women by targeting risk and efficacy appraisals.
Method
Overview
The current intervention (referred to from this point onwards as ‘the animation’) was designed using the Intervention Mapping framework. 33 Intervention Mapping is an approach to the development of theory- and evidence-based health behaviour change interventions, with an emphasis on the benefit of community participation, and involves six iterative steps and takes an ecological approach to develop multi-level interventions. 34 Intervention Mapping fits in to the Medical Research Council (MRC) guidelines for developing complex interventions. 35 Table 1 shows the steps involved in Intervention Mapping.
Steps of Intervention Mapping (Bartholomew 2016).

Multiple methods are applied across a series of steps based on Intervention Mapping. These methods, described below, include primary research, secondary research and consultation, and were applied and revisited throughout the development of the intervention.
Step 1: Needs assessment
The research team consisted of two behavioural scientists with experience in intervention development and health research. The research team were responsible for developing the content of the animation, and making design and content decisions throughout.
Health psychology theories,14–16 and meta-analyses that examined the influence that risk and efficacy appraisals have on behaviour17–19 were used to inform the selection of behavioural determinants to target, that would work to increase risk appraisals. Recent evidence shows that current interventions are not effective in increasing vaccination intention or behaviour. It was noted that many of these interventions did not target an increase in efficacy appraisals, which may have led to interventions having a counterproductive effect on behaviour. 36
Review of existing literature revealed that little was currently known about how pregnant women perceive the risk of flu and the benefit of the flu vaccination. Qualitative work, consisting of interviews with 24 pregnant women, recruited from hospital antenatal clinics and social media sites was conducted to fill a gap in the current research by providing insight into the beliefs (categorised using the Illness Risk Representation (IRR) Framework37,38 to establish what beliefs are underlying estimates of likelihood and severity of flu. 39
Step 2: Defining the intervention objectives
The intervention goal was discussed by the steering group and agreed upon. The steering group consisted of the research team, plus an additional health psychologist, a Midwife and Research Fellow and a Consultant in Public Health from the local authority. The research team discussed the intervention goal, and what was required by individuals to achieve this goal, and subsequently identified the performance objective. The performance objectives were discussed and confirmed with the steering group.
Developing the matrix of change objectives
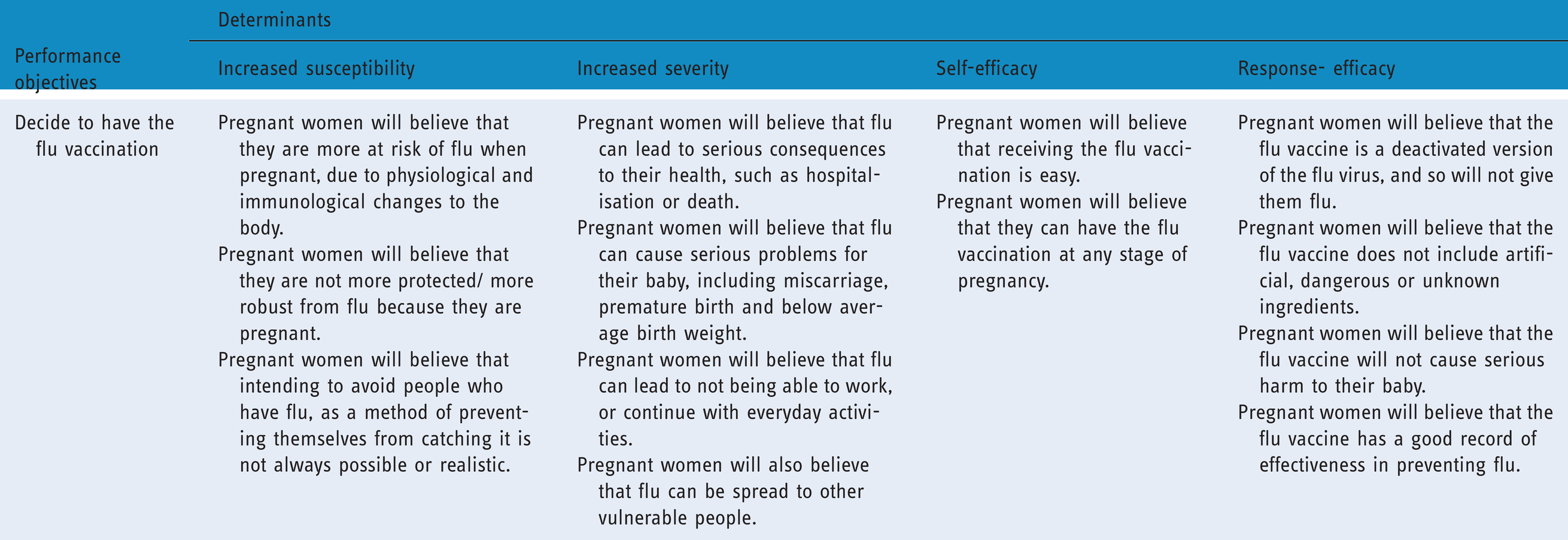
A matrix of change objectives (see Table 2) containing the beliefs that need to change, related to each determinant (risk and efficacy appraisal) in order to change the performance objective was developed by the research team.
Matrix of change objectives.
Step 3: Designing the intervention
During initial planning, WCC and CCC conveyed their requirements. They specified that they would like the amination to include clear ‘plain English’ information on the risk of flu during pregnancy, and how the flu virus causes flu. They also required that factual information about flu was provided that was consistent with their existing public health campaigns. In parallel with capturing the requirements of the commissioners, the team set about identifying active intervention content capable of achieving changes in risk and efficacy appraisals.
Selection of behaviour change techniques
The Behaviour Change Taxonomy 40 was consulted by the research team to identify suitable Behaviour Change Techniques (BCTs) to change the selected determinants of vaccination (risk and efficacy appraisal). This process was further informed by the results of a recent consensus exercise conducted by experts in the field, 41 in which the level of agreement for the links between BCTs and mechanisms of action was established. In this exercise, consensus was considered to have been reached if 80% or more agreement in the exercise was achieved. This allowed the research team to identify and select BCTs (where there was =>80% agreement that the technique could change risk and/or efficacy) for inclusion in the animation, which helped to shape the content of the animation (by ensuring that each BCT was addressed by elements of the animation). The research team checked throughout the development process to ensure that the BCTs chosen were still present in the animation.
Consultation with experts
A workshop with experts was run to generate ideas for the practical applications (components of the animation that convey the messages) that will target the change objectives. Experts were presented with information about the need for the animation, and preliminary plans for it, and were asked to provide feedback and thoughts on the proposed content and structure. Experts attending the workshop were those working in pregnancy related public health research, and in the design and implementation of Public Health interventions. Attendees of the workshop included two behavioural scientists, a midwife, a Health Protection Officer, and four representatives from Public Health England and Coventry and Warwickshire Clinical Commissioning Group. A workshop was also held with pregnant women (recruited to participate in patient and public involvement (PPI) activities from hospital antenatal clinics) to discuss the suitability of the proposed practical applications. Both experts (Clinicians, Public Health Professionals and Midwives) and pregnant women were also consulted repeatedly at various points throughout the design and development of the animation process.
Step 4: Producing the intervention
Development of content
The agreed practical applications resulted in six components of the animation being specified. The development of each component and content for each was informed by extensive consultation with pregnant women, midwives, clinicians and Public Health professionals.
A design company was commissioned to create the animation following open tender and interview process. The successful design company worked closely with the research team to develop the look and content of the animation. In total, 14 pregnant women, ten midwives, four clinicians and four public health professionals commented on and provided input at various stages of the development of the animation. Consultation was sought a number of times with these groups about the content, the visual representation of the flu virus and the characters, the wording of the script and the structure and ordering of the animation. Some of the changes that were made to the animation, as a result of the consultation included changes to the colouring of the characters and the background, changes to the voices used for some of the characters and changes to the ordering of the components in the animation. All feedback from consultation was discussed by the research team, and any decisions were made after consultation with the wider steering group.
Acceptability study
Qualitative interviews with twelve pregnant (or recently pregnant) women (recruited from earlier qualitative work, and via social media) were conducted to find out the acceptability of the animation prior to making final changes. Institutional ethical approval was received for this study. Participants all provided consent prior to interviews. A total of twelve pregnant or recently pregnant participants were interviewed, either face to face or using remote video calling. Participants were asked to watch the animation (either on researchers’ laptop in face-to-face interviews, or by being sent the animation by email immediately before the interview). Thoughts on the content, length and information within the animation were gathered and responses were analysed using content analysis.
Results
Step 1: Needs assessment
Overview
The priority population for the animation was determined as all pregnant women, shown in the Logic model of the problem (Figure 1).

Logic model of the problem.
It was intended from the outset was that the animation would form part of a wider flu campaign delivered by Warwickshire County Council (WCC) and Coventry City Council (CCC).
Evidence review
Table 2 shows the determinants that were identified as the basis for the animation, informed by health psychology theories15,16 and a review of existing literature. A review of the evidence included meta-analyses17–19 that found that increasing risk appraisals (specifically estimates of vaccination severity and likelihood) are potentially effective in increasing vaccination uptake (although with small effects).
Qualitative work, consisting of interviews with 24 pregnant women, (each lasting between 20 and 60 minutes) aiming to further understand the beliefs pregnant women hold about flu and the flu vaccination provided information about what determinants would be targeted by the animation. Thematic analysis was conducted on interviews, using the Illness Risk Representation framework37,38 to categorise beliefs that pregnant women hold about flu and the flu vaccination, it was established that these women felt that being pregnant did not increase their vulnerability to flu and were largely unaware of the consequences it could cause for themselves and their unborn baby. They also often believed that the vaccination could cause ill-health, and that it was a live vaccine. 39 This informed determinants that the animation will target in an attempt to change risk and efficacy appraisals, and subsequently increase the uptake of flu vaccination in this population.
Step 2: Defining the intervention objectives
Establishing intervention goal and programme objectives
The intervention goal was agreed as ‘all pregnant women to have the flu vaccination each flu season.’ The performance objective was confirmed as ‘pregnant women decide to have the flu vaccination’.
Developing the matrix of change objectives
Table 2 contains the matrix of change objectives agreed upon for the animation.
Step 3: Designing the intervention
Selecting behaviour change techniques
Table 3 contains the BCTs that were selected for inclusion in the animation.
Change objectives, behaviour change techniques and practical applications included in the design of the intervention.

Consultation workshops
Feedback from the workshop conducted with experts, and from the workshop with pregnant women to generate ideas about the design of the animation, resulted in a set of ideas about the practical applications that would form the content of the animation, and informed the script and storyboard for the animation.
Step 4: Producing the intervention
Overview
Ideas generated by the workshops led to the identification of six components of the animation. Ideas and content evolved through an iterative process involved considerable input from pregnant women, midwives, clinicians and public health professionals (as described in the Method section). The components of the animation were as follows: 1. Inform pregnant women about how flu can be transmitted; 2. Inform pregnant women about why they are more at risk from flu whilst pregnant; 3. Inform pregnant women about the consequences to themselves and their baby should they get flu; 4. Inform pregnant women what is in the vaccination; 5. Demonstrate to pregnant women how the vaccination is administered; and 6. Demonstrate to pregnant women how the vaccine works to protect them from flu.
Details of finished animation
The basis of the finished animation was the behavioural determinants, and the beliefs that underlie these determinants. The finished animation is approximately four and a half minutes long, and is in full colour. It portrays the physiological changes that take place during pregnancy and explains why this makes pregnant women more susceptible to flu. The animation provides an explanation of what the consequences of flu are to pregnant women, and their unborn babies. It continues by showing the journey of a pregnant women deciding not to have the flu vaccination, how she becomes infected with flu, and the personal consequences this has for her. The animation then shows what alternatively happens to her if she has the flu vaccination, showing in detail the ingredients of the vaccination, how the vaccine works, and how it protects her and her unborn baby. Screenshots from the finished animation can be seen in Figures 2 to 5, and the full animation can be seen here. https://media.coventry.ac.uk/View.aspx?id=15358~5j~BZGUS3vBws&code=Jn~sxNNicdbThnroI6OLadcRTbhRElXcOWhpBILTobWqlKNn3plS2W6umoxWaqsfEiotCOexK&ax=7D~LNpaexM2ChCzTL.

Depiction of how the heart and lungs change and move as a result of the development of the baby as pregnancy develops.

The midwife visits the pregnant woman and asks if she has had the flu vaccination and provides her with an information leaflet to read about the vaccination.

The pregnant woman visits the practice nurse and asks some questions about the flu vaccination before deciding to have it. The practice nurse then administers the flu vaccine.

Depiction of the unborn baby in utero, with the illustration of the protection provided by the flu vaccination.
Acceptability study
Findings from the qualitative acceptability study (consisting of interviews with twelve pregnant or recently pregnant women) were analysed using content analysis, and showed that participants felt that the animation was acceptable and provided relevant information about flu and the flu vaccination at an appropriate level to increase pregnant women’s knowledge and understanding of the risks of flu and the flu vaccination. Participants also felt that the animation was likely to increase pregnant women’s intentions to take up the offer of the flu vaccination. 39 There were minor changes identified as a result of the acceptability testing, such as changes to colouring of background and characters within the animation, and ordering of the animation, which resulted in a final round of amendments and minor changes being made.
Step 5: Implementation of the intervention
It was planned from the outset that the animation would be embedded as one part of the wider WCC and CCC 2018/19 and 2019/20 seasonal flu campaigns. The animation was hosted on the WCC and CCC websites and was used actively as part of their social media campaigns.
Discussion
Summary of the animation design process
This paper describes the development of a theory and evidence-based intervention to increase the uptake of flu vaccination amongst pregnant women. The intervention was shaped by considerable consultation with pregnant women, midwives, Public Health professionals and clinicians. The intervention design process resulted in the production of an animation conveying facts about flu and the vaccination, and detailing the potential risks of flu during pregnancy. Risk appraisals were targeted for change by informing pregnant women: that they are more at risk from flu due to physiological and immunological changes to the body, how flu is spread, that flu can lead to serious consequences to the health of pregnant women and their unborn baby, the consequences of getting flu on ability to work and carry out daily activities, and the potential risk of spreading flu to vulnerable people (such as young children). Efficacy appraisals were targeted for change by informing pregnant women: that having the flu vaccination is easy and is available at any stage of pregnancy, that the vaccination is a deactivated version of the flu virus and will not give them flu, the ingredients in the flu vaccination, and that the flu vaccination is a safe and largely effective way of preventing flu during pregnancy.
The final version reflected comments and feedback from pregnant women, midwives, clinicians and public health professionals, following extensive consultation, and this led to great improvements upon earlier drafts. The suggestion made by pregnant women and midwives, to reorder the scenarios to show in full the impact of choosing not to get vaccinated, before moving onto to the impact of having the vaccination, makes the final animation clearer and easier to follow. Inclusion of a resource for more information at the end of the animation was suggested, which increases the usefulness and professionalism of the animation. Minor changes to language used to convey facts about the safety, recommendation and administration of the vaccination, made the animation more in-line with existing Public Health messages and campaigns, and more in line with current midwifery practice. The process of making repeated versions was time consuming, and increased the financial cost of the completed animation, but was valuable to the overall usefulness and appropriateness of the animation.
Strengths of the animation and the study
Previous research suggests that digital interventions, such as websites, text messages videos and computer games, are effective in changing health behaviour.23–25 The animation has the potential to have good reach due to the rapid increase in the use of internet and mobile devices. 20 This means that the animation can be accessed easily, and by a large proportion of the target population. Furthermore, the use of evidence and recommendations in development increase the potential usefulness of the animation, in increasing vaccination behaviour amongst pregnant women.
The current animation will have no implementation costs and is easily embedded into the wider Public Health flu campaigns. Despite being developed with the intention to include the animation in campaigns across Coventry and Warwickshire, it is in fact suitable for all pregnant women in the UK (subtitles can be enabled to overcome language barriers), as the content and information is not specific to the geographic area, and therefore could be shared on a wider scale.
The animation has the potential to be useful as a resource for midwives too. Future plans for the animation include using it as an online resource to allow midwives to disseminate appropriate information about flu to pregnant women. Furthermore, if successful in increasing the flu vaccination rates, it has the potential to reduce the financial burden that flu in pregnancy has on the NHS, by way of less pregnant women hospitalised due to serious complications, and less premature births or neonatal care needed as a result of maternal flu during pregnancy.
As the animation was subjected to thorough consultation, and was designed in collaboration with various stakeholders, it is a reflection of what pregnant women want, and what midwives are happy to signpost these women to.
A benefit of the process, is the consultation and collaboration with important stakeholders. Many advantages of working co-creatively with the target audience have been documented. In particular, collaborating with people who will potentially use the product increases the range of perspectives included, can lead to unique and innovative ideas, and can better match the end product with the need of the audience. 32 Pregnant women, midwives, public health professionals and clinicians were consulted at each stage of the process. This approach to the intervention design helped to increase the acceptability and appropriateness of the animation for the target audience. Without the consultation and the collaboration, the animation would differ to the final product.
A strength of the intervention development process lies with the chosen methodology. Intervention Mapping 33 is a robust process, using clearly defined steps, resulting in an intervention that is theory- and evidence-based, whilst grounded in the needs of the target population. Using Intervention Mapping allows for transparent reporting of the process, including what was involved at each step, making it replicable if required.
Weaknesses of the animation and the study
One weakness is the fact that other potentially important determinants of behaviour (beyond risk and efficacy appraisal) are not addressed by this intervention. The animation was only designed to change appraisals of risk, with no attempts made to change environmental factors, for example, GP surgeries vaccination strategies, accessible clinic times, 11 or influence from healthcare professionals. 42 This places the focus of the intervention firmly on changing risk and efficacy appraisals but as a consequence limits its potential efficacy. However, this decision was also made in light of discussions around vaccination behaviour being a relatively simple health behaviour that individuals are only required to perform once. Accordingly, unlike for other behaviours such as physical activity, or smoking cessation that require high levels of sustained self-regulation, motivation was expected to have a more direct relationship with action. Flu vaccination behaviour itself is relatively simple to execute (i.e. the process of being vaccinated requires little effort on the behalf of the recipient, and only one dose is required rather than repeated effort), and approaches of some GP surgeries (such as vaccinating opportunistically) make access to the vaccination easy and convenient 11 ). Furthermore, meta-analysis evidence suggests a relationship between intention and behaviour, showing that a medium-to-large increase in intention, leads to a small-to-medium increase in behaviour. 43 This suggests that intention to vaccinate is a suitable outcome to address.
Ultimately this animation is designed to sit within wider Public Health Campaigns in addition to being used on its own. It is acknowledged that this animation may be successful in changing flu related risk, but it may be that changing risk alone, may not be sufficient to change behaviour. The aim of this animation was therefore to target an increase in intention to vaccinate, with the acknowledgement that when placed within a larger campaign, other elements (such as information around the safety of the vaccination, or measures to increase healthcare provider recommendation) may compliment the animation and help motivate a change in behaviour. A wider campaign would be well placed to target a number of factors, including environmental factors that influence the decision to vaccinate amongst pregnant women.
A challenge lies with the length of the animation. Initial plans were for the animation to be between two and three minutes, but this was not possible. Due to the amount of information covered, the completed animation was longer than anticipated, lasting four and a half minutes. Work has been conducted into optimum lengths of videos, which suggests that audience’s engagement peaks at 70% when the length is up to two minutes in length, after which it drops. However, for videos lasting four to five minutes such as the current animation, engagement is still approximately 65%, reflecting little drop-off compared to videos lasting two or three minutes. 44
One important consideration throughout the animation development process was the presence of different priorities for researchers and the Public Health departments of WCC and CCC. There was a need to balance the needs and aims of the public health professionals, who wanted the animation to compliment other elements of their seasonal flu campaign, whilst ensuring the integrity of the intervention and the theoretical influence were maintained and not diluted.
Differing priorities of the parties involved led to some time delays. There were project-related time constraints, and in order for the animation to be included in the 2018/19 Public Health flu campaign, it needed to be completed by a specified date. The design company however, had no academic or campaign considerations, and as a commercial company had other work ongoing. This meant that the design company needed encouragement to complete as quickly as possible.
Implications for practice and research
The animation has potential usefulness to the NHS. It could be a way for midwives to disseminate information about flu and the flu vaccination to pregnant women, without impacting on consultation time, as it could be a resource that is given to pregnant women to look at outside of an appointment. It also has potential usefulness for midwife practice. Furthermore, used within a primary care setting such as a general practice as part of routine flu vaccination communication could further increase the access to the information within the animation. As the animation was based on findings of qualitative work with pregnant women, 39 the information contained within the animation is likely to be consistent with questions or concerns that pregnant women may have about flu and the vaccination.
Further research surrounding the implementation of the animation into routine care is needed to establish the effectiveness of the animation (related to Step 6 of Intervention Mapping). The study authors are planning a future experimental study to test the effectiveness of the animation. As well as ascertaining the effectiveness of the intervention, this will provide valuable evidence, lacking in the risk literature, about the relationship between risk and health behaviour. Despite decades of research into risk appraisals, little is known about their influence on changing health behaviours, as much research to date consists of correlational analysis, highlighting the need for more experimental evidence. 45
Conclusions
This article describes the development of an animation that aims to increase the uptake of flu vaccination amongst pregnant women. It is the first known intervention to use an animation to target an increase in flu vaccination uptake amongst pregnant women, using risk and efficacy theory. Previous literature proposes that risk and efficacy appraisals can change behaviour, providing an evidence base for the animation. The animation targets both risk and efficacy appraisals, which builds on previous interventions which often only target risk appraisals. The Intervention Mapping approach 33 provided a systematic basis for the design and the development of a theory-based intervention, heavily influenced by consultation and collaboration with pregnant women, midwives, clinicians and Public Health professionals. This collaboration increases the likelihood that the animation is appropriate for pregnant women and strengthens the potential usefulness of it.
Footnotes
Acknowledgements
The authors would like to thank Warwickshire County Council and Coventry City Council for funding the costs of producing the animation, and all the pregnant women, midwives, clinicians and Public Health Professionals in taking the time to provide feedback and advice on the intervention materials.
Contributorship
JP led the research, supported by KN, EB and NI. EB. All authors contributed to the writing and revising of the manuscript.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was completed as part of a PhD studentship at Coventry University dated September 2015–September 2018. The animation design costs were funded by Warwickshire County Council and Coventry City Council Public Health Departments. Funding for publication of this paper was provided by the Open Access Fund at the University of Warwick.
Guarantor
JEP.
Peer review
This manuscript was reviewed by reviewers who have chosen to remain anonymous.