
Abstract
The main objective of this study was to preliminary explore the effects of DARWeb on different outcomes. A Quasi-experimental, one-group, pretest–posttest design was used. Parents and children were asked to complete questionnaires and questions (separately) about quality of life, abdominal pain severity, and satisfaction. Semi-structured interviews with families were also performed. This study focuses on 17 families. Results showed that parent’s ratings of children’s abdominal pain severity were significantly lower after finishing the intervention and at the 3-month follow-up, and quality of life scores had increased significantly after 3 months. From children’s ratings, mean abdominal pain severity scores were significantly lower after the intervention compared to the preintervention assessment. Both parents and children were quite satisfied with the intervention. In qualitative interviews, families suggested that DARWeb helped them to give less importance to pain and to learn coping strategies. In conclusion, this study showed the potential usefulness of DARWeb for children with functional abdominal pain and for their parents.
Keywords
Introduction
The development of Internet-based interventions for the management of chronic or recurrent pediatric pain has increased in recent years.1,2 The results are promising and show great potential in this field, mainly because access to face-to-face psychosocial interventions, the gold standard for children with pain,3,4 is quite difficult. This difficulty exists because few multidisciplinary pain services are available, 5 and there are few professionals with adequate training in pain assessment and management.6,7
Specifically, trials using Internet-based interventions for children/adolescents with headache,8,9 juvenile idiopathic arthritis, 10 and mixed pain problems (including children with functional abdominal pain (FAP))11–14 have been conducted. These are remote interventions based on the cognitive behavioral model (CBT), and they include therapist support/supervision (reviewing assigned tasks, commenting on doubts, and giving advice) using e-mail, 8 messages sent to families through the program website,9,12,13 e-mail and phone,11,14 or phone. 10 Some of them include separate content for parents,9–14 whereas others focus their interventions only on children/adolescents. 8 In general terms, and summarizing the available evidence, these interventions have been found to be effective in reducing pain frequency,8,9,11 pain duration, 8 pain intensity,9–12,14 activity limitations/pain interference,9–12,14 depressive and pain-related anxiety symptoms,9,13 maladaptive parents’ behaviors,9,13,14 parents’ perceived impact (i.e. the impact of caring for a child with pain on the parent’s functioning), 13 parents’ miscarried helping (i.e. efforts made by parents to assist the child with pain that result in resistance), 13 and pain catastrophizing. 8 Also, they have been shown to increase sleep quality.13,14
To contribute to this field, we have created DARWeb: an Internet-based intervention for children with FAP and their parents. Our aim is to provide a condition-specific Internet-based intervention for children with FAP. Although it is one of the most frequent pain complaints in children and adolescents, 15 causing a high degree of suffering for both children and their families,16,17 there is no condition-specific Internet-based intervention available for this type of pain. In fact, although four previous Internet-based interventions included children with FAP and their parents in their trials, their programs were targeted at mixed pain samples.11–14 However, many studies exist that have tested face-to-face interventions specifically designed for children with FAP.18–22 These condition-specific interventions allow addressing factors that can be relevant to one pain problem but not to others. Targeted content can help participants to better identify with said content, as they may find it more relevant and meaningful.23,24 By way of example, in our intervention we used vignettes to guide the content for the children. They portrayed different day-to-day situations in the life of Alex (a child with FAP); although they may not be relevant to other types of problems, they were all typically related to this pain problem. Moreover, worked into our written materials were small pieces of personalized information garnered from participants’ input. For example, we included the names they gave in the materials or information they provided about the difficulties they faced in the text.
It is also important to note that all the available studies testing Internet-based interventions (in the pediatric pain field) included therapists who periodically contacted users to follow their progress. In our intervention, we only contacted the families to send them reminders in order to foster their participation. However, this contact was minimal, and we did not talk with families about their progress or the content they were working on (as previous research did). We did this to reduce the long-term cost of the intervention and, thus, increase its sustainability.
Another aim of our intervention was to achieve the involvement parents at the same level of dedication as that given by the children. To our knowledge, of the above-mentioned Internet-based interventions, only the one by Palermo et al. 12 required similar dedication from both children and parents. We consider it important to involve parents to the same extent as children because their lives are also affected by the situation and they can have an effect on children’s pain. 25 Parents need to work to understand the main characteristics of abdominal pain (including triggers), effective ways to manage abdominal pain, communication skills and how to show their children positive reinforcement when they cope effectively. These topics were addressed in our content for the parents and require time for them to be internalized. For this reason, we divided them into seven units (as in the case of the intervention for the children).
Finally, it is also worth noting that we wanted to add to the available knowledge by introducing qualitative data to improve knowledge about what families learned through our program and the perceived effects. Qualitative information can be useful in the context of chronic pain in order to better understand and complement quantitative information. Some studies dealing with the acceptability and feasibility of interventions for children with pain are starting to include a qualitative approach. 26 However, most of the available studies focusing on the effects of interventions on the pain experiences of children limit their assessment to quantitative data.
Overall, the objective of this study is to perform a preliminary exploration of the effects of DARWeb on different outcomes (i.e. abdominal pain severity, disability, and quality of life), from the point of view of the different actors involved (parents and children). In addition, we wanted to qualitatively study the impressions of the participating families about the effects of our program. Taking into account this objective, and with the aim of qualitatively interviewing participating families, we have chosen a one-group, pretest–posttest design.
Method
A mixed-methods concurrent study design was employed. We combined qualitative and quantitative data with equal status to obtain complementary information from both strategies (QUAN + QUAL). 27 A combination of the results from the two types of data and their relation with previous literature is made in the “Discussion” section later on.
We used a quasi-experimental, one-group, pretest–posttest design to evaluate the effects of DARWeb on different outcome variables assessed through questionnaires. Participants were also asked to rate their satisfaction, and they were interviewed to obtain qualitative data about their views regarding the effects of DARWeb on their situation.
Procedure
Families were recruited through a number of collaborating healthcare professionals in Spain and advertisements on various different websites. For dissemination among healthcare professionals, we used three strategies: (1) the holding of conferences and presentations at different healthcare services (e.g. conferences in seminars organized by specific healthcare centers) and congresses for pediatricians; (2) informative e-mails sent to affiliates of different associations through their mailing lists; and (3) the setting up of personal meetings with various key pediatricians in our environment. In relation to advertisements on various different websites, these include our online campus, and the different websites (or blogs) of health centers or professionals that decided to include the information after hearing about our project. Finally, to all the contacts interested in the project, we send a bimonthly newsletter reporting our progress and highlighting any news.
When a family was referred to us, we contacted them by phone to give them a brief presentation of the study; if they were interested, we arranged a meeting with them (by videoconference or face to face; whichever the families preferred). In this meeting, a more detailed explanation about the program and associated assessments was provided to the families, and they were verbally asked (both parents and children) for their willingness to participate. If they accepted, the parents were asked to sign an informed consent for their participation and their child’s participation. Participating parents and children were each asked separately to answer an online survey (pre-treatment online survey-T0) to gather socio-demographic information and information related to the study outcomes (please, see measures section). Those who completed this survey were given access to the intervention. Two weeks after finalizing DARWeb, the parents and children were asked to complete the same online survey (post-treatment online survey-T1) separately. Families were also interviewed (face to face or by videoconference) using in-depth semi-structured interviews (children and parents were interviewed together) after they had completed the post-treatment online survey. Two research team members conducted the interviews with each family together. These interviews lasted approximately 30 min and were audio recorded. A follow-up assessment was performed 3 months after completing DARWeb (T2). Participants were asked to complete the same questionnaires as in T1. The study was approved by the Ethics Committee of our University.
DARWeb intervention
DARWeb is a self-directed intervention, and families were only contacted if they had not logged on to the system for about 10 days. The intervention includes parallel but separate content for parents and children, distributed in seven units for each. Our intervention is rooted in the cognitive-behavioral model of pain and, for this reason, we teach families coping strategies to reduce pain impact and disability (i.e. relaxation, changing maladaptive thoughts, pain distraction, and assertive communication). However, we also place a special emphasis on transmitting the idea that pain is not everything in life and that the most important thing is living the life they want despite having pain.
Units are scheduled weekly, and each unit takes about 30 min to be completed (participants were encouraged to complete each unit on one or two different days). They had to complete one unit before they were allowed to start the next one. Parents and children were told to complete their units separately, although we encouraged parents to supervise their child’s progress and motivate him or her to follow it. Units were composed of text, graphics and multimedia, and each of them was divided into five sections: objectives, introduction, training, exercises and summary. The objectives section presents the main aims for the unit. Moreover, parents receive a brief explanation of the topic their child is going to work on during the week and a PDF file with the corresponding content of the children’s unit. The introduction section provides a theoretical basis for the topic addressed, whereas the training section provides specific instructions about how to apply the skills taught in the unit. In the exercises section, some small tasks are proposed to further consolidate the skills taught. Finally, the summary section includes a short summary of the content of the unit, and the system automatically sends an e-mail to the participants with a PDF file containing the content.
DARWeb was implemented using the Intelligent Research and Intervention Software (IRIS) platform. 28 Some more details about our intervention can be found in our previous report. 29 Content was interactive and personalized (e.g. with the name provided by the participant). Figure 1 shows a screenshot of the vignettes used to guide the intervention for children; the screenshot in Figure 2 provides a sample of typical content.
Screenshoot of teh vignettes used to guide the intervention for children.
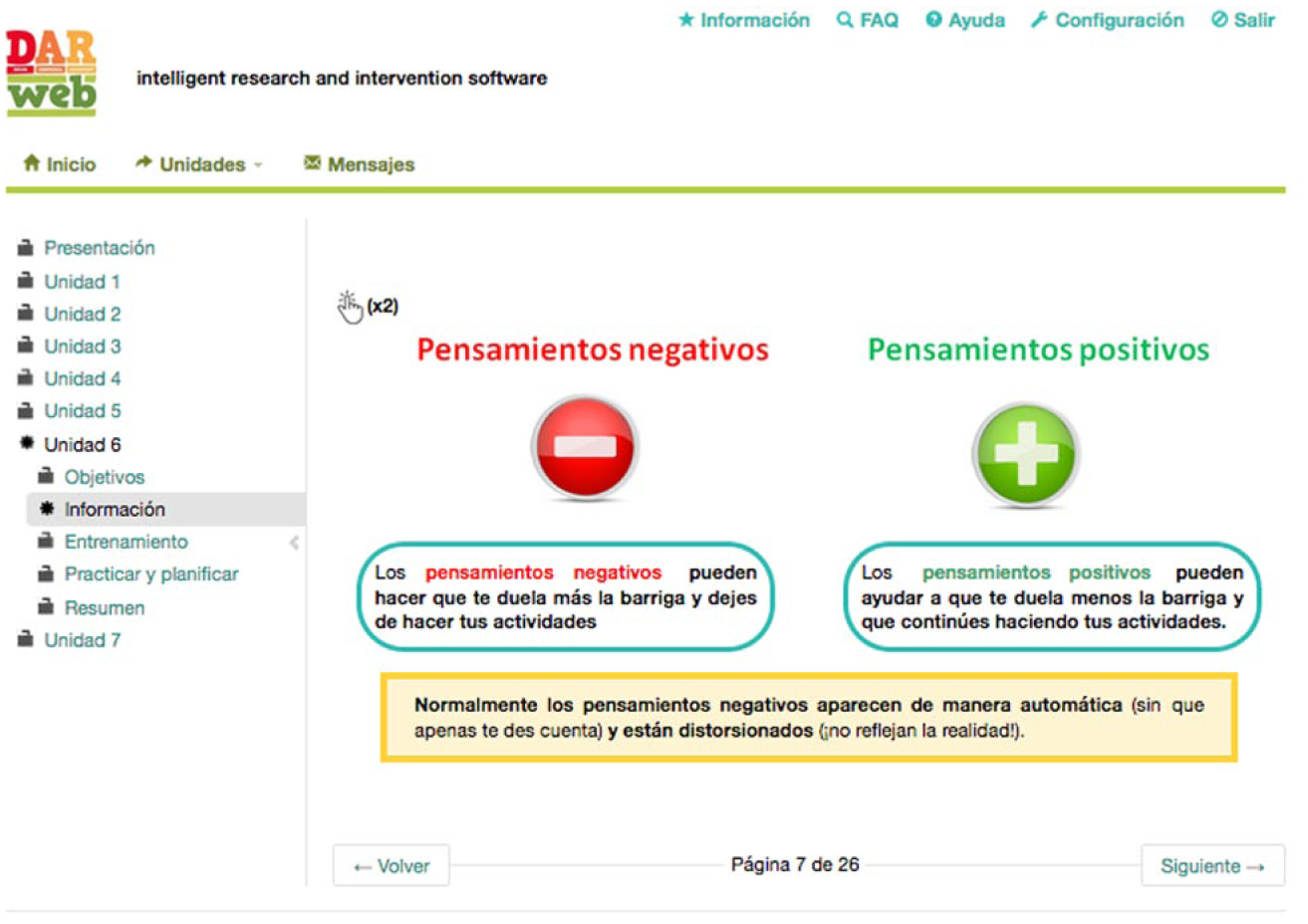
Screenshoot whowing how content is displayed typically to users in our intervention (including interactive elements).
Participants
Following the inclusion criteria, children with FAP from 9 to 15 years old and their parents were invited to take part in this study. The inclusion criteria were the classic ones proposed by Apley and Naish, 30 that is, children (and their families) were invited to participate if they had had a minimum of three episodes of abdominal pain that interfered with their daily activities during the past 3 months. These criteria were used instead of those proposed by the most recent ROME criteria (http://www.romecriteria.org), which require the presence of abdominal pain at least once a week. This decision was taken because Apley criteria give us the opportunity to include children with less frequent abdominal pain problems who would otherwise be excluded.
Children with an organic cause for their abdominal pain or with a severe mental illness were excluded. These criteria were assessed by the pediatrician who referred them or confirmed by the participants during the initial interview with the research team. Moreover, children or parents who were unable to understand the Spanish or Catalan language were excluded.
A total of 37 families who fulfilled the criteria were included in the study and completed the T0 assessment. Of them, 22 (59.46%) completed the whole program, and 17 had complete data after the intervention (post-intervention assessment) and are the focus of this study (see Figure 3, which provides a flow chart of participating families). Of the 15 families who did not complete the program, 13 families completed some of the DARWeb units, and 2 families did not complete any of them (neither the children nor the parents entered DARWeb). Of the 13 families who completed some units, the children completed a median of three units, and the parents completed a median of 2. A more extensive analysis of non-completers was performed in our previous study. 29 Finally, reasons mentioned for not being willing to follow the program included (information was not available on four families, and each family could report more than one reason) the following: (1) not having enough time to follow DARWeb (n = 6), (2) feeling that there was too much material to read (n = 3), (3) feeling it was tiresome to complete DARWeb (n = 3), (4) not having a severe enough problem (n = 2) and (5) having another problem that needed more attention than FAP (n = 1). Non-completers were not asked to respond to the questionnaires again since our objective was to explore the perceived effects in families completing the whole program, and because it was difficult to ask them to make the effort required to complete the questionnaires again once the families had left the intervention. In any case, there were no significant differences in the pre-intervention assessment (T0) in any of the measures of interest described in the next section when we compare participants who completed DARWeb (22 families) and those who did not (15 families).
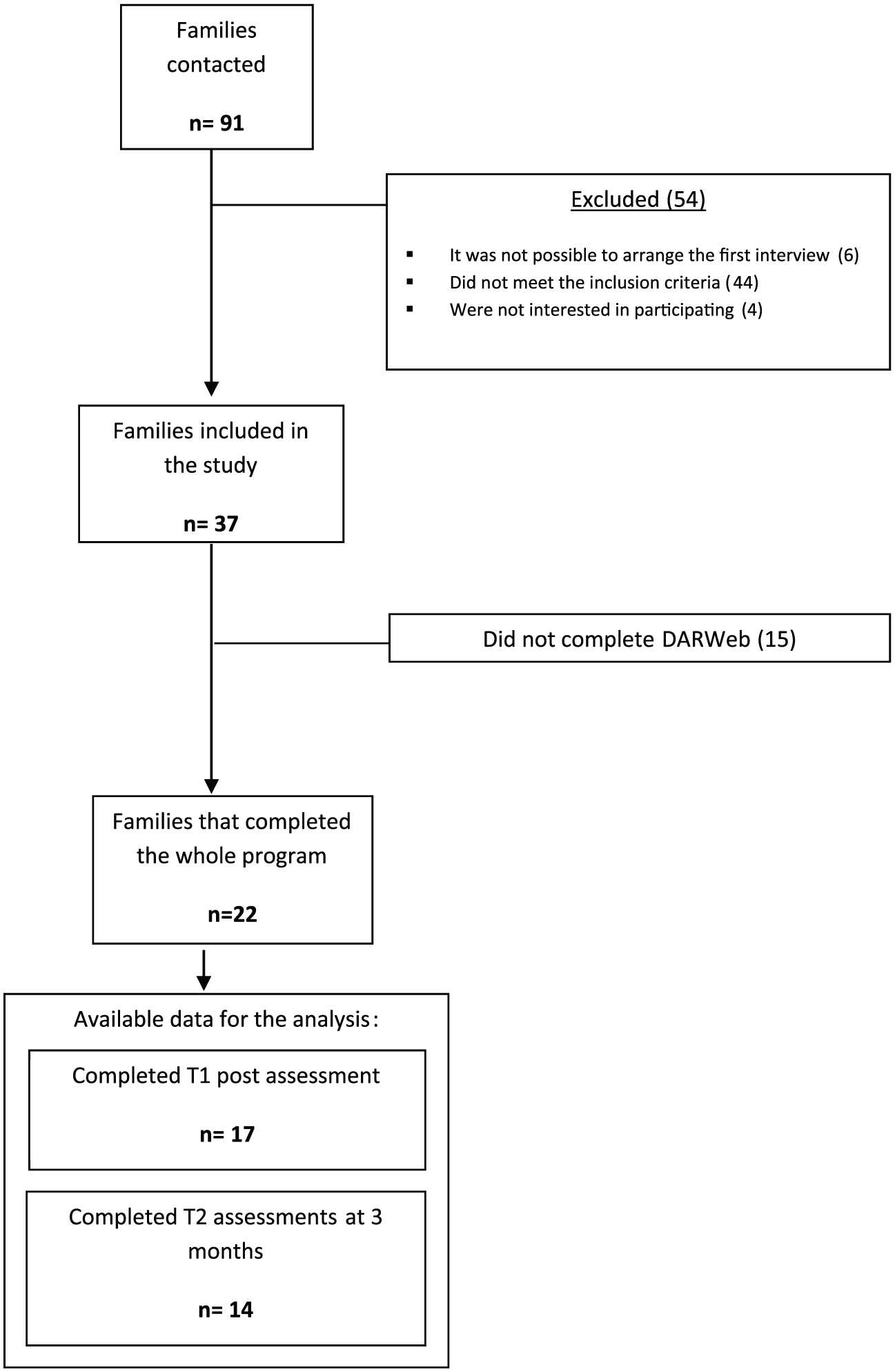
Flow chart of participating families.
Measures
Below we present the different variables assessed at the different assessment points: pre-intervention (T0: online questionnaires were sent 1 week before access to the intervention), post-intervention (T1: online questionnaires were sent 2 weeks after finishing all units), and 3 months after post-intervention (T2: online questionnaires were sent 3 months after finishing the intervention). As shown in Figure 3, 5 families out of the 22 who finished DARWeb did not complete T1 questionnaires, and 3 of the remaining 17 for analysis at T1 did not complete T2 questionnaires.
Below, we also describe the characteristics of the semi-structured interview conducted with all the families after finishing the program.
Quantitative evaluation (assessed at T0, T1 and T2)
All the instruments in this section were administered to both parents (in relation to their children’s situation) and their children.
Quality of life
Quality of life was assessed with a short version of the Pediatric Quality of Life Inventory (PedsQL), a frequently used and recommended questionnaire, 31 which was validated in the Catalan population. 32 This version is composed of 12 items designed to assess the children’s (or parents’) perception of their quality of life. Participants are asked to what extent each item has been a problem in the past month. Items are scored on a 5-point Likert-type scale, from 0 (never a problem) to 4 (almost always a problem). Items are reverse-scored and linearly transformed to a 0–100 scale (0 = 100, 1 = 75, 2 = 50, 3 = 25, 4 = 0), and a total score can be computed by averaging all the items.
Pain severity, frequency and intensity
The Abdominal Pain Index (API) 33 was used. This is a short instrument, frequently used in the abdominal pain literature,34,35 composed of five items that assess abdominal pain frequency, duration, and intensity. We used the Spanish version developed following a back-translation procedure approved by Dr Walker. 36 With the API, the frequency of pain, in terms of days, is rated from 0 (not at all) to 5 (every day), and in terms of times per day, from 0 (none) to 5 (persistent). Duration of pain episodes is measured from 0 (no pain) to 8 (most of the day). Finally, typical and highest abdominal pain intensity are measured on a 0 (no pain) to 10 (the most possible pain) numerical rating scale. From the API, a global rating of abdominal pain severity was computed, following a new scoring procedure that has shown adequate psychometric properties, 34 and resulting in an overall pain severity score from 0 to 4.
Overall ratings of improvement and satisfaction with treatment
At the end of the program (at T1), both parents and children were asked to rate the following (using an 11-point numerical scale): to what extent they thought DARWeb had helped them to improve the way they cope with pain, to what extent they felt that DARWeb had improved their overall situation and how satisfied they were overall with DARWeb. Similar questions have been created and included in previous studies,11,14 and the assessment of global improvement has been recommended by the Pediatric Initiative on Methods, Measurement, and Pain Assessment in Clinical Trials. 31
Qualitative evaluation
We conducted semi-structured in-depth interviews with the whole family (parents and child at the same time) to better understand the quantitative ratings they provided. As each family was interviewed together by two researchers, we analyzed the results obtained considering each family as a group. We planned to carry out interviews by two interviewers as we felt it was easier to follow families’ explanations and not miss important messages they may be sending. One of the interviewers assumed a more active role introducing the topics, while the other acted in a supporting role annotating and introducing emerging themes when needed. To avoid any possible negative influence of this interview format, the first moments of the interview were spent creating a positive climate and explaining the rationale for the interview and its procedure. We based our methodology on the book by Mack et al., 37 among other resources, in which carrying out interviews by two interviewers is considered as an option when deemed necessary.
During the interviews, we introduced two topics in broad terms: (1) impressions about the program and online interventions and (2) perceived effects of DARWeb on their pain situation and learned skills.
The analysis related to families’ qualitative views about the program was the focus of a previous paper testing the feasibility of the intervention. 29 Therefore, here, we focus on analyzing the content of the interview in relation to the effects of DARWeb on their pain. This was also analyzed in our previous paper, 29 but the sample was smaller and here we want to integrate these results with the quantitative ones in the “Discussion” section in order to gain an overall impression about the effects of DARWeb on participating families. Thus, regarding this topic, we wanted to know whether, and in what way, DARWeb had changed their ideas and perceptions about their pain situation. Moreover, we were interested in discovering which of the skills that they had learned were most useful to them and most frequently used after they had finished the program.
Data analyses
Descriptive statistics are presented for the quantitative data described in the “Measures” section. Paired t-tests were used to evaluate the effects of DARWeb on the quantitative variables, comparing T0 with T1, T1 with T2 and T2 with T0. Effect sizes were also computed using Cohen’s d statistic, corrected for dependence between means using Morris and DeShon’s 38 equation. T-tests were used instead of analyses of variance (ANOVAs) because the sample was reduced at the 3-month follow-up (17 families at T1 and 14 at T2). Normality was checked using the Shapiro–Wilk test, and all variables accomplished with it. All of these analyses were performed with the IBM SPSS statistical package version 21.
Interviews were analyzed by two members (M.B. and I.B.) of the research team. An inductive, structured, content analysis procedure (following the classification in “Qualitative research and its place in psychological science” by Madill and Gough 39 ) was used to obtain qualitative data from the interviews.
Atlas.ti 6.2 was used to perform these analyses. After the codes were defined, the two members of the research team independently classified the qualitative data into these categories. Any disagreements were discussed until agreement was reached. We calculated the Cohen’s kappa coefficient for the seven codes interpreted (Table 2), and the inter-coder agreement was 0.95.
Results
Socio-demographic and pain characteristics
Mean age for the 17 children who completed the whole program and assessments at T0 and T1 was 11.23 years (range: 9–14 years), and 11 (64.7%) were girls. Most of them (as reported by their parents) had had pain for more than 12 months (94.1%).
Table 1 shows the pain characteristics at T0, T1 and T2. In general terms, the initial pain severity (assessed by the API) was low (less than 2 on a 0 to 4 scale). It is important to highlight that the mean global rating scores on the API reported by the children were lower than those reported by the parents at T0 and T1 (mean ratings were equal for children and parents at T2). There were significant differences when comparing the ratings of parents and children at T0 (t16 = 3.3; p = 0.004), but not at T1. Something similar occurred with the PedsQL mean scores: they were always higher for the children, showing that they perceived better quality of life, but these differences were becoming smaller with time. Apart from this observation about the descriptive scores, there were no significant differences when comparing mean PedsQL scores for parents and children at any of the assessment points.
Descriptive statistics for PedsQL, API at the three assessment points.
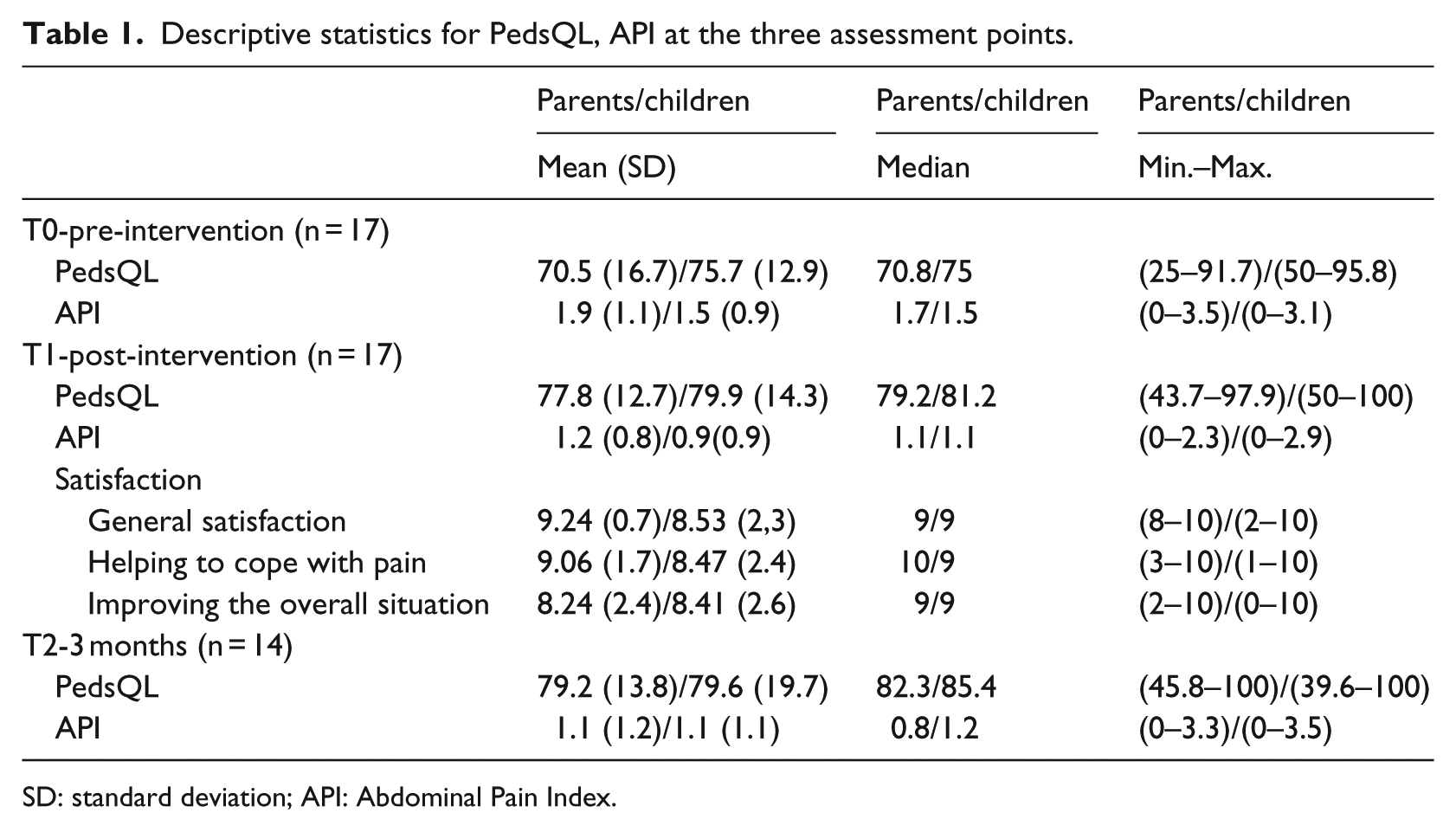
SD: standard deviation; API: Abdominal Pain Index.
Quantitative analyses
Quality of life
At a descriptive level, total scores on quality of life seem to improve from both the parents’ and children’s perspectives after completing DARWeb (T1), and they were relatively stable at the 3-month follow-up (T2) (see Figure 4). A detailed examination of t-test comparisons showed that there were no significant differences between T0 and T1 (t16 =−1.86; p = 0.08) and between T1 and T2 ratings provided by parents on quality of life (t13 = 0.96; p = 0.35); however, there was a significant difference when comparing T0 and T2 scores (t13 =−2.8; p = 0.015; Cohen’s d = 0.76). For children’s ratings, although descriptive data showed a similar pattern, there were no significant differences when comparing T0 and T1 (t16 =−0.97; p = 0.35), T0 and T2 (t13 = 0.16; p = 0.87) and T1 and T2 (t13 =−1.3; p = 0.21).
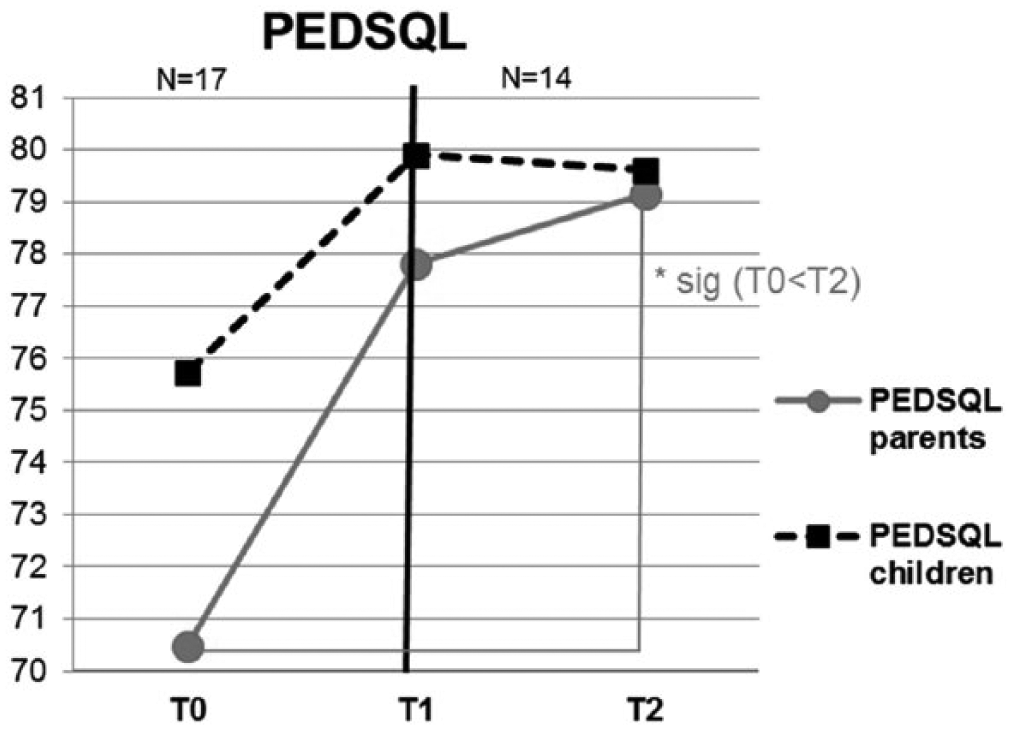
PedsQL scores on the different time assessments.
Pain severity
Total API scores at different assessment points can be seen in Figure 5. At a descriptive level, the severity was reduced for parents at T1 compared to T0 (i.e. they perceived that their children had less severe abdominal pain at T1), and it was reduced a little more at T2. Pair comparisons revealed a significant difference between T0 and T1 (t16 = 2.56; p = 0.02; Cohen’s d = 0.63) and between T0 and T2 (t13 = 2.6; p = 0.023; Cohen’s d = 0.68). There were no significant differences between T1 and T2 scores (t13 = 0.77; p = 0.45).
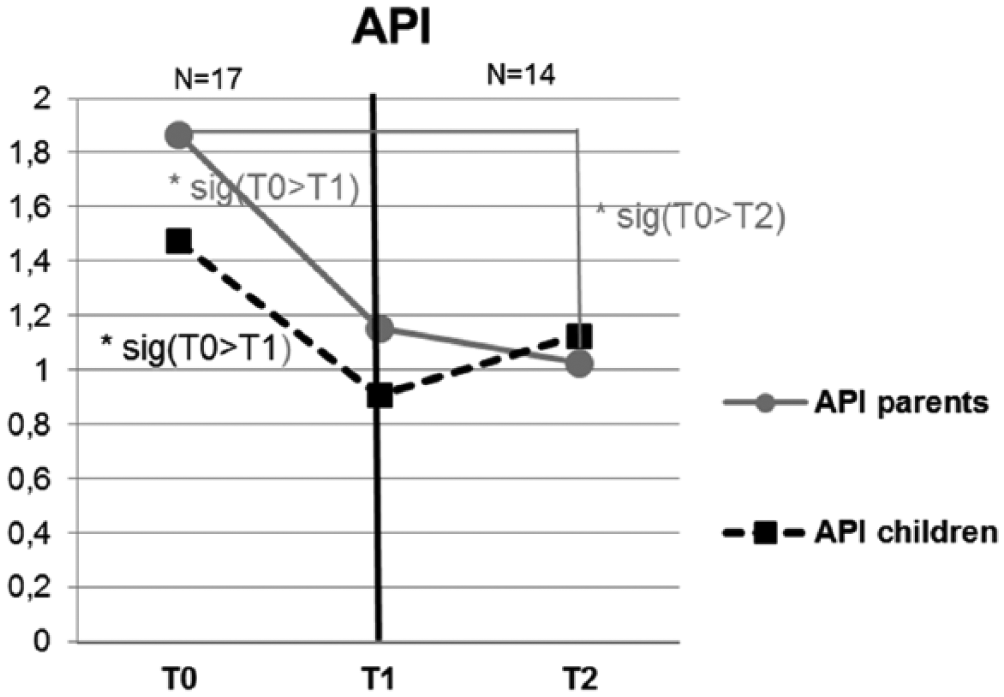
API total scores on different assessments.
For children, total API scores decreased at T1 (compared to T0), but scores at T2 suggested a slight worsening in pain severity (even so, levels of severity were lower than at T0). T-tests showed that the improvement from T0 to T1 was statistically significant (t16 =−2.33; p = 0.03; Cohen’s d = 0.57), but there were no significant differences when comparing T0 and T2 (t13 = 1.7; p = 0.12), or when comparing T1 and T2 (t13 = 0.53; p = 0.62).
Satisfaction with the intervention
Descriptive statistics for the three items about satisfaction with DARWeb (rated at T1) are presented in Figure 6. Results suggest that both parents and children were quite satisfied with DARWeb (all median ratings above 9); they considered that the program helped them to cope with pain, and they felt that the program helped them to improve their overall situation. There were no significant differences on any of the three global ratings given by parents and children.
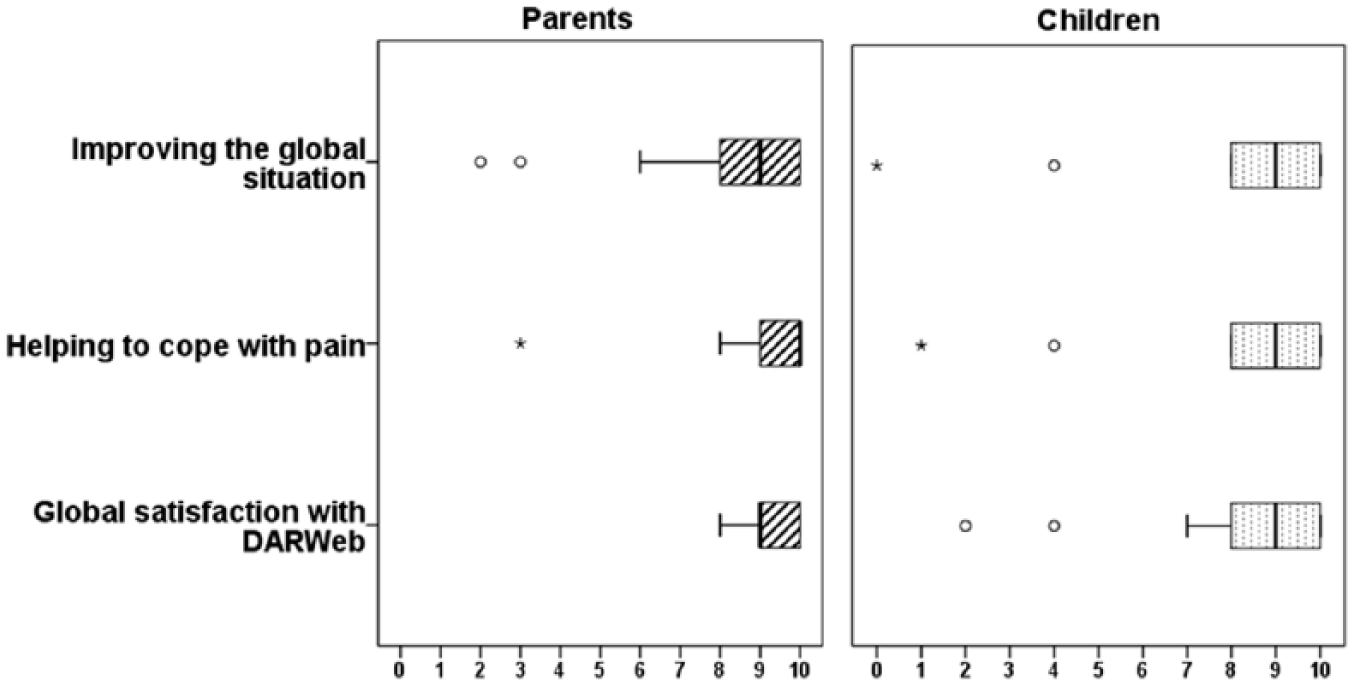
Satisfaction with the intervention.
Qualitative analyses
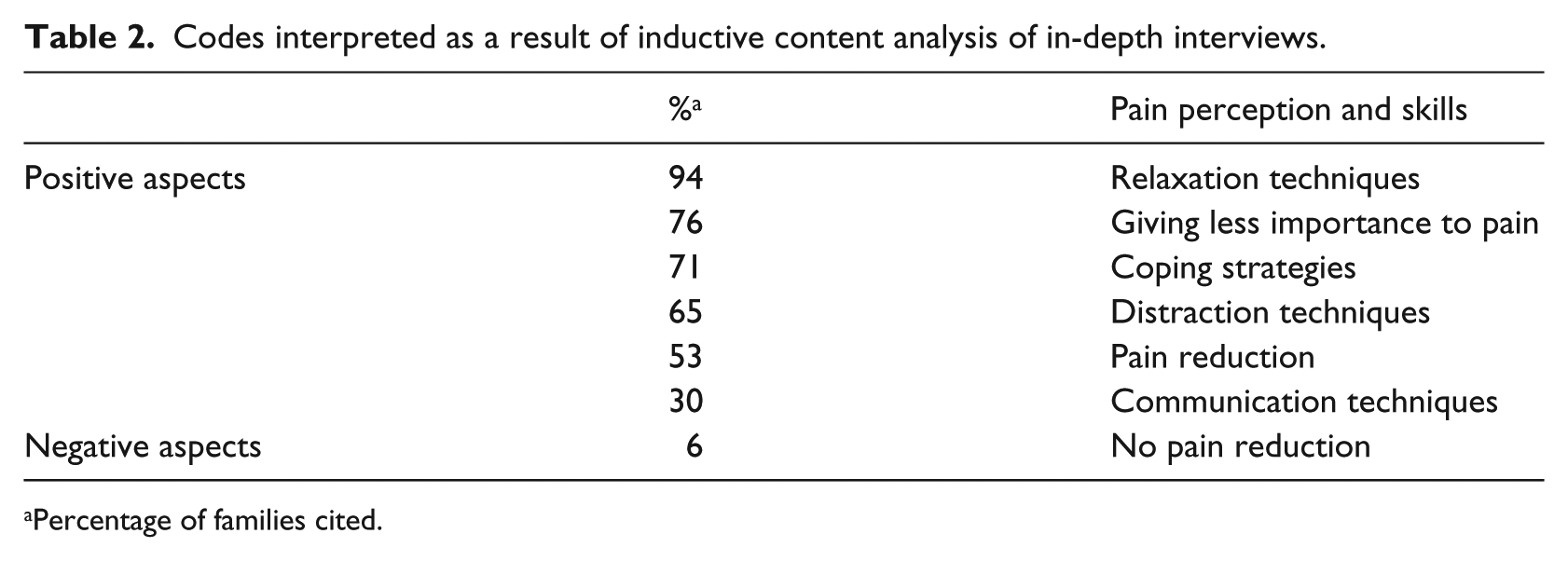
Table 2 presents the main codes identified through the qualitative analysis performed. They were also classified into positive and negative aspects.
Codes interpreted as a result of inductive content analysis of in-depth interviews.
Percentage of families cited.
In relation to pain perception, a high percentage of interviewed families (76%) suggested that DARWeb changed their pain perceptions because it helped them to give less importance to pain and to carry on with their usual activities (Giving less importance to pain code); as a mother expressed, The truth is that it helped us a lot also, because, basically for me … it allows me to not worry so much, I am not a suffering mother, but I am more relaxed … Because I said: she has a stomach ache, it doesn’t matter, it will go away.
In addition to giving less importance to pain, 53% of the families highlighted that DARWeb helped to reduce their pain or stop it completely (Pain reduction code). For example, a mother expressed a reduction in pain telling us, “My daughter is not having that pain. I was desperate because I didn’t know how to behave, and the doctor did all the medical tests.” A girl (10 years old) also expressed a reduction of pain in the following way: “Since I started DARWeb, my belly doesn’t hurt so much. […] now it’s not continuous, it’s from time to time” (P22: Pain reduction).
Only one family mentioned explicitly at the interview that they had not noticed any pain reduction (No pain reduction code).
In relation to the techniques and skills they learned, most of the families (94%) talked about relaxation (Relaxation technique code). This seems to be the most well-liked and useful skill for them, as one boy (13 years old) expressed: “What I have used is relaxation, but apart from abdominal pain, for other things, for exams, problems with people. It was useful for me.” In general terms, they explained that they found it useful, and some of them also stated that it was not only useful for abdominal pain, but also for other situations. An example was the following comment from a mother: “I also have stomach aches … and the relaxation topic, how to behave and … it’s useful, and it has been useful for me also.”
A high percentage of families (71%) also highlighted that they had learned to cope with pain effectively thanks to what they learned (Coping strategies code), but without referring to any specific skill, as one mother told us: “[…] her attitude, she is more open … and she knows how to manage her stomach ache. And I am noticing that she is getting better every day.” In general, they expressed that they had changed their minds about dealing with pain, as another mother expressed: My answer in dealing with pain has changed. Before I saw it as a specific situation and then you took care of them … “poor boy, stay home” … but when it’s recurrent pain it changes, my way of looking at it is different.
Apart from relaxation, another specific technique that appeared frequently in the interviews was attention distraction (65% of families mentioned this; Distraction techniques code) as one girl (12 years old) told us: “I try to focus more on what the teacher is saying, and then my pain goes away faster. Before I used to focus more on the pain.”
Finally, 30% of the families also mentioned that they found the communication techniques that they learned to be useful (Communication techniques code). For example, a father commented, “[…] assertiveness, learning how to say things to her properly … it‘s super-useful, and it is useful in life in general.”
Discussion
From the parents’ perspective, the children’s quality of life improved significantly 3 months after the intervention. A similar pattern was found in the children’s scores; but there were no significant differences in any comparison. The severity of abdominal pain was reduced significantly from the parents’ perspective (both after the intervention and at the 3-month follow-up, compared to pre-intervention scores). For children, there was a significant improvement after the intervention, but scores were not significantly different at the 3-month follow-up compared to pre-intervention scores. In any case, both parents and children consider that the program improved their overall situation after the intervention (through a numerical rating scale) and were highly satisfied with DARWeb.
Using the same questionnaires as we have used, there are previous studies showing significant improvement in both pain severity and quality of life. For example, Robins et al. 21 found significant post-intervention improvements in parents’ and children’s API ratings at both the 6- and 12-month follow-ups. Van der Veek et al. 22 also found an improvement in children’s reported API scores (parental data not available) after the intervention, again at both the 6- and 12-month follow-ups. In relation to quality of life, Wassom et al. 40 found a significant improvement in the quality of life of children with FAP after treatment (parental data were not gathered). Therefore, the existing results regarding pain severity coincide with our own except for children’s ratings of pain severity at the 3-month follow-up (no significant differences were detected in our study). However, our results differ from previous studies in relation to quality of life, since we did not find significant variations in children’s ratings. There are different reasons for the divergences in results. First, in relation to quality of life, our participants had high initial scores, which suggests that this area was not particularly affected in their opinion, making it more difficult to find significant improvements like those reported in previous studies. 11 Second, the small sample size also made it different to find significant results. Finally, in our study, there are less significant differences between pre-intervention and post-intervention measures from the children’s perspective. This is congruent with non-interventional studies that also support differences in the rating scores of parents and children with FAP, with parents’ reports suggesting worse outcomes. 41
Qualitative data help us to understand in greater detail the participants’ experience as well as the above-mentioned results, and they reinforce the beneficial effects of our intervention. This can be seen in the statement from most of the families that they had learned to give less importance to pain or that half of the families perceived a reduction in pain. Moreover, they appeared to have learned certain coping mechanisms for pain and were especially happy with the relaxation and distraction techniques as well as the communication strategies. This is related with the objectives of our intervention. These objectives were in line with the principles of CBT for pain management, which have been shown to be effective for children with FAP.18,31–33 From this perspective, our aim was to help families to cope effectively with their pain by managing their maladaptive thoughts, using relaxation and distraction techniques, and modulating parents’ responses to their children’s pain. We also intended to help them to communicate adequately within the family because communication can be difficult when there is a family member with recurrent or chronic pain. In fact, CBT-based programs for children and adolescents frequently include the family in the intervention, and a module is dedicated to improving communication and, especially, to providing training in assertive communication. 42 However, in our program, although developed from a CBT perspective, and then focused on the teaching of coping strategies, we also give importance to transmitting the idea that pain is not everything in life and that they have to carry on with their lives despite having pain. For this reason, we dedicated content to transmitting these ideas at the beginning in order to teach them to establish their SMART goals and to work toward accomplishing them in spite of having pain. To some extent, this perspective can be considered compatible with the principles of acceptance therapy (AT). AT has been less studied than CBT in children with pain (there are no available studies specifically designed for children with FAP), but available studies support the effects of the so-called “Third-Wave” of cognitive-behavioral therapies, which include acceptance.43,44 As mentioned above, families in our study highlighted the importance of learning through the program that they have to get on with their lives in spite of having pain, but they also appreciated learning how to cope with pain. We consider these views interesting because they suggest that it could be useful to combine strategies from AT and CBT to help families with children in pain. Traditionally, studies have been developed exclusively within the framework of one of these two waves of psychological therapy, but from our point of view, there is no reason not to combine elements from each of them (as we have attempted to some extent).
Another point that merits attention is that DARWeb is a self-directed program (the research team only contacted participants to send reminders). We think this point is at least partly responsible for the greater proportion of dropouts in our study, compared to previous studies that included children with FAP and had a person who periodically contacted the families to talk about their assignments and/or progress. However, we think it is interesting to maintain the self-administered system, for three interrelated reasons. First, the results of our intervention (mixing qualitative and quantitative data) are positive and in line with results in the literature for testing self-administered, Internet-based intervention for other health problems (DARWeb is the first one without therapeutic support for pediatric pain that has been filed to our knowledge). For example, Chiauzzi et al. 45 provided a totally self-directed, Internet-based intervention for people with back pain, obtaining positive results. Second, most of the families who dropped out of the program explained that they did so because of lack of time (please see our previous study for a more detailed analysis of this issue 29 ). Based on these results, we think that a step forward would be to create more elements that allow us to tailor the intervention to each family’s specific needs. For example, some families may already have suitable communication skills and therefore might not need our unit to focus their efforts on this area. By working along these lines, we could probably reduce the duration of the intervention, facilitating its follow-up and making it more meaningful. 46 Finally, self-directed intervention is the best option in terms of cost. This approach’s only required costs are software maintenance and the salary of a person (hired part-time) to assess, give access to, and monitor families.
Our study has some limitations. The first is the sample size, which is small, making it difficult to generalize the results, and probably the reason for not finding significant differences in some of our results. Second, we did not perform a randomized controlled trial, which is the “gold standard” design for testing the preliminary effects of interventions. However, our purpose in this study was to have a preliminary evaluation of the effects of our intervention. Therefore, the next step in DARWeb testing will involve performing a randomized controlled trial with a larger sample to confirm these results.
In sum, our study is important because it is the first Internet-based intervention, designed specifically for children with FAP and their parents, which can help to provide a better adaptation to the needs of this population. Moreover, it is completely self-directed, which can contribute to its future applicability in a real context. Participating families reported improvements in quantitative data, but in qualitative interviews they also suggested that they had learned coping strategies and how to live in spite of having pain. Overall, if DARWeb is shown to be effective in future studies, it can be a good alternative for children with FAP and their families.
Footnotes
Acknowledgements
We are very grateful to the individual professionals and collaborating centers that facilitated contact with participating families and helped us with the project. They include ABS. Girona 3; CAP Castellar del Vallès; CAP Cunit; CAP Montilivi. Girona; CAP Taradell; CAP Sant Vicenç de Montalt; CAP Sardenya; Center Clínic Menorca, Barcelona; Center Sanitari de l’Anoia; Centro de Salud Alcañiz; Centro de Salud García Noblejas; Centro de Salud Doctor Castroviejo; Centro de Salud María Jesús Hereza; Consorci d’Atenció Primària de Salut de l’Eixample; Corporació de Salut del Maresme i la Selva; Fundació Althaia, Manresa; Hospital de Nens, Barcelona; Hospital Vall d’Hebrón; Hospital Trias i Pujol; Hospital de Figueres; Hospital Verge de la Cinta de Tortosa; Hospital Mútua de Terrassa; Hospital General de Granollers; Hospital Sant Joan de Reus; Paidodex. Hospital Quirón-Dexeus; PIUS Hospital de Valls; Policlínica Comarcal de El Vendrell; SAP Alt Penedès–Garraf–Nord. We are also very grateful to the families who participated in this study. We acknowledge that some sections of DARWeb are based on myWHI (an Internet-based CBT intervention for youth with headaches, led by Drs McGrath and Huguet) and the Strongest Family Program (distance family interventions for youth, led by Drs McGrath and Lingley-Pottie). Finally, we want to acknowledge the anonymous reviewers who helped us to improve this paper with their comments.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was funded by Fundació La Caixa (Recercaixa, 2012–2013) and the “Ministerio de Economía y Competitivad” (Spanish Government, reference: PSI2013-42413-R; 2014–2016).