
Abstract
Increasing diabetes prevalence has led to the need for more sustainable and person-centred services. The diabetes self-care mHealth marketplace is growing, but most effective/valued features are unknown. This study gauges diabetes app user opinion to inform development work. An analysis of diabetes mHealth apps informed design of a questionnaire sent to a random sample of 400 patients stratified by diabetes type and age. Responses were analysed by sub-group, and preferences were compared with current diabetes apps. App features included data storage/graphics, exercise tracking, health/diet, reminders/alarms, education. Questionnaire response rate was 59 per cent (234/400); 144/233 (62%) owned smartphones. Smartphone users expressed preference towards mHealth (101/142 (71%)), although diabetes use was low (12/163 (7%)). Respondents favoured many potential features, with similar preferences between diabetes types. This study demonstrates that while mHealth acceptance is high, current engagement is low. Engagement and functionality could be improved by including stakeholders in future development, driven by clinical/user need.
Introduction
An estimated 385 million of the world’s 7 billion population have diabetes, over three quarters of whom live in low or middle income countries. 1 Diabetes currently accounts for 11 per cent of worldwide healthcare spending with projected costs set to increase, as the numbers affected are estimated to reach nearly 600 million by the year 2035. 1
The worldwide mobile phone market continues to grow year on year with over 1.3 billion units being shipped in 2014, 72 per cent of which were smartphones. 2 The World Bank 3 estimates that worldwide in 2013, there were 92 subscriptions to mobile phone providers per 100 people. Developing countries have demonstrated the largest increase in ownership in the past few years, and it was anticipated that ownership in these countries would exceed those in developed countries for the first time by the end of 2014. 4
The use of mobile devices to improve health outcomes, healthcare services or health related research has become known as mHealth. 5 Many different smartphone and tablet apps are available for managing diabetes, the number of which is rising exponentially.6,7 Functionality that is most prevalent included insulin and medication recording, data export and communication, recording of dietary intake and weight monitoring. 6 Very few apps are designed to improved diabetes knowledge (in contrast to published guidelines which emphasise the need for patient education8–10), and there has been no identified formal evaluation of the role of social media in diabetes care.
In general, web-based interventions aimed at improving the management of diabetes have been shown to improve clinical outcomes.11,12 It is more difficult to establish which components are important to achieve these improvements, however, due to the complex nature of each intervention. Published findings from studies that specifically report on mHealth-based interventions are mainly restricted to those interventions which predate the advent of smartphone technology, but have concluded that the use of mHealth can result in improved glycaemic control and patient self-efficacy and knowledge. 13
Local context
Diabetes care in Scotland relies on a series of managed clinical networks supported by a national informatics platform. 14 Despite an increase in diabetes prevalence, there has been a sequential improvement in quality performance indicators and the incidences of diabetes-related complications have decreased.15–17 The informatics platform has also enabled the creation of the Scottish Diabetes Research Network (SDRN) 18 – a national clinical trials infrastructure that comprises 10,000 registered patients to date. My Diabetes My Way (MDMW) is a national electronic patient health record (ePHR) that is integrated with the national diabetes informatics platform. 19 There are approximately 10,400 registered users to date. 20 Registration for SDRN and MDMW is not mutually exclusive; however, the similarity between the numbers registered with both is purely coincidental.
Project aims
This project aims to utilise the SDRN and MDMW patient cohorts to
Assess levels of engagement with web-based and mHealth technologies within the Internet-using Scottish diabetes population,
Identify demographic sub-groups that are more or less likely to use such technologies,
Draw comparisons between features that are currently available within the app market and features that are most desirable to those with diabetes.
Methods
Review of available diabetes mobile apps
Prior to questionnaire design, a search was conducted of the Apple app store in July 2014. This snapshot search was limited to the search term ‘glucose tracking’ and was principally aimed at developing a broad understanding of the diabetes app market; therefore, informing questionnaire content. Apps were included (regardless of price) if they specifically targeted diabetes. Search results were then downloaded and reviewed by a single reviewer (I.C.), who identified and categorised available features. The identified features were then incorporated into the questionnaire to assess user preference (see below). User preference was also sought for features not identified from the snapshot analysis, but thought to be relevant for future app development.
Diabetes patient mHealth Questionnaire
A 39-item questionnaire was designed in four parts: demographics, current use of technology in diabetes self-care, preference for mHealth and preferred features/functionality of mHealth applications developed in the future (questionnaire available on request). The questionnaire was written in an electronic format and posted online. No identifiable data were collected. All items utilised a categorical response in order to improve response rate and quality of data. Permissions to gather data were obtained from the local Caldicott Guardian. All patients contacted had previously given consent to be contacted via unsolicited email during the enrolment process for both SDRN and/or MDMW. Ethics permission was sought and deemed unnecessary as this work was related to ongoing service improvement.
The MDMW and SDRN datasets were randomly sampled in a stratified way (via a random number generator) to return 200 patients, consisting of 50 patients from the following four groups: T1D < 50 years old; T1D ⩾ 50 years old; T2D < 50 years old; T2D ⩾ 50 years old. Both samples were also mutually exclusive, that is, individuals in the MDMW sample were excluded prior to sampling the SDRN dataset. All individuals were resident in Scotland and had an active email address that was used to invite them to take part in the survey. This invitation email contained a link to the online questionnaire. The MDMW survey took place between August–October 2013 and formed the basis of an undergraduate student project. The SDRN survey took place between April and June 2014, in an effort to draw comparisons between the findings of the MDMW survey and the wider diabetes community.
Statistical analysis
Initial analysis demonstrated that mHealth preference was the same across both groups (see results) and so responses from both surveys were combined into one dataset. Preference for mHealth apps was measured via two questionnaire items that were conditional on the respondent owning a smartphone (respondents were asked to reflect on current diabetes management and were asked to agree with the following statements: ‘A smartphone app to manage my diabetes would be a positive development’ and ‘I would prefer to use a smartphone app to manage my diabetes’. Both items were agree/disagree questions that utilised a 5-point scale). The internal consistency of these items as a measure of preference for an mHealth app was tested using the Kappa statistic. The two items were then summed to produce a score (out of 10) that was used as a summary of an individual’s preference for the use of mHealth technologies – the mHealth preference scale. A higher score on the scale (0–10) was interpreted as an individual being enthusiastic about using mHealth technologies. Demographic variables (age group, gender and diabetes type) were crosstabulated with mHealth preference to identify sub-groups of interest. Categories within the demographic variables and mHealth preference were collapsed as appropriate, in order to achieve representation in each of the cells (see results). Denominators were adjusted to take into account missing data. Loglinear analysis was used to identify interactions between demographic sub-groups and mHealth preference. Cases with missing data were excluded from analysis of that data field. Significant inter-actions identified in the loglinear analysis were then explored in greater depth using Chi Square and odds ratios.
In addition to mHealth preference, respondents were asked about current use of technology. Responses were analysed with respect to demographic sub-groups that were found to be significantly associated with mHealth preference. Finally, all respondents were asked which of the features commonly found in mHealth diabetes apps would be most desirable with responses stratified according to diabetes type.
Results
mHealth apps
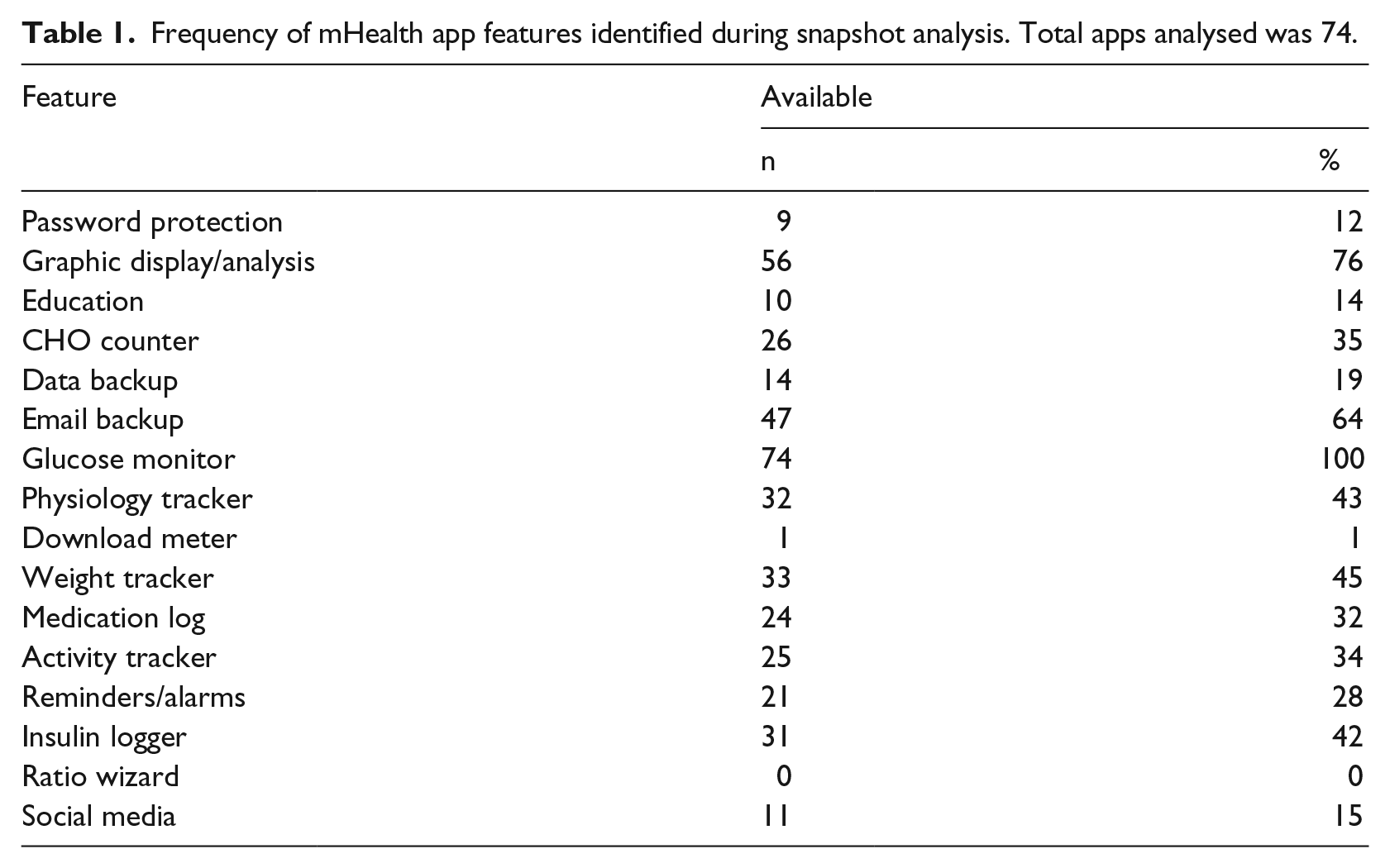
A total of 74 diabetes-related apps were identified through the Apple Store and analysed. Approximately half (39/74, 53%) were free, while the others ranged in price from £0.69 to £6.99 (€0.87–€8.83, US$1.09–US$11.06). In all, 16 separate features were identified. The median number of features was 5 (range 2–11). All apps had the facility to record blood glucose results, while only one incorporated a blood glucose monitor. The available features and the frequency with which they were available are listed in Table 1.
Frequency of mHealth app features identified during snapshot analysis. Total apps analysed was 74.
Demographics
Responses to the questionnaire were received by 121/200 (60.5%) of the MDMW sample and 113/200 (56.5%) of the SDRN sample. Data quality was good with very little missing data – for example, completion rate was 98–100 per cent for gender, diabetes type, duration of diabetes, treatment and phone ownership. Age group was completed by 218/234 (93%). When compared with MDMW respondents, the SDRN group were more likely to be older (SDRN median age group 56–65 years compared to MDMW median age group 46–55 years, U = 4232, z = −3.771, p < 0.001), male (SDRN: 79/112 (70.5%) male c.f. MDMW: 66/117 (56.4%) male, p = 0.029) and have T2D (SDRN: 80/109 (73.4%) T2D c.f. MDMW: 59/121 (48.8%), p < 0.001) (age categories were decades from the age of 16, i.e., 16–25, 26–35, etc.). There was no significant difference in smartphone ownership between both groups (SDRN: 75/112 (67%) c.f. MDMW: 69/121 (57%), p = 0.077). Similarly, there was no significant difference in prevalence of smartphone ownership when those with T1D (55/91, 60.4%) were compared with T2D (85/138, 61.6%). These similarities allowed for data to be pooled for subsequent analysis. The majority of respondents (176/229, 77%) use self-monitored blood glucose (SMBG) levels in their diabetes management.
mHealth preference
In all, 144/233 (62%) people owned a smartphone, of which 142 gave their preference for mHealth technologies. The majority expressed an interest in the use of mHealth apps to manage their diabetes − 101/142 (70.1%) agreed or strongly agreed with the statement a smartphone app to manage my diabetes would be a positive development, and 79/142 (54.9%) agreed or strongly agreed with the statement I would prefer to use a smartphone app to manage my diabetes. As expected, there was a statistically significant correlation between responses for each of these statements, which demonstrated moderate agreement (Kappa = 0.45, p < 0.001, 95% confidence interval (CI): 0.35–0.56). The responses to both of these items were then summed to calculate an individual’s mHealth preference score, available for 127/144 (88%) of respondents.
mHealth preference was skewed towards high preference (see Figure 1). The score was therefore collapsed into high (7–10) and low (2–6) preference categories in order to combine the low numbers of respondents at the lower end of the scale. When comparing mHealth preference categories for each of the demographic groups (age category, gender and diabetes type), there were no significant differences noted, although there was a trend for people ⩾56 years to express less preference (data not shown).
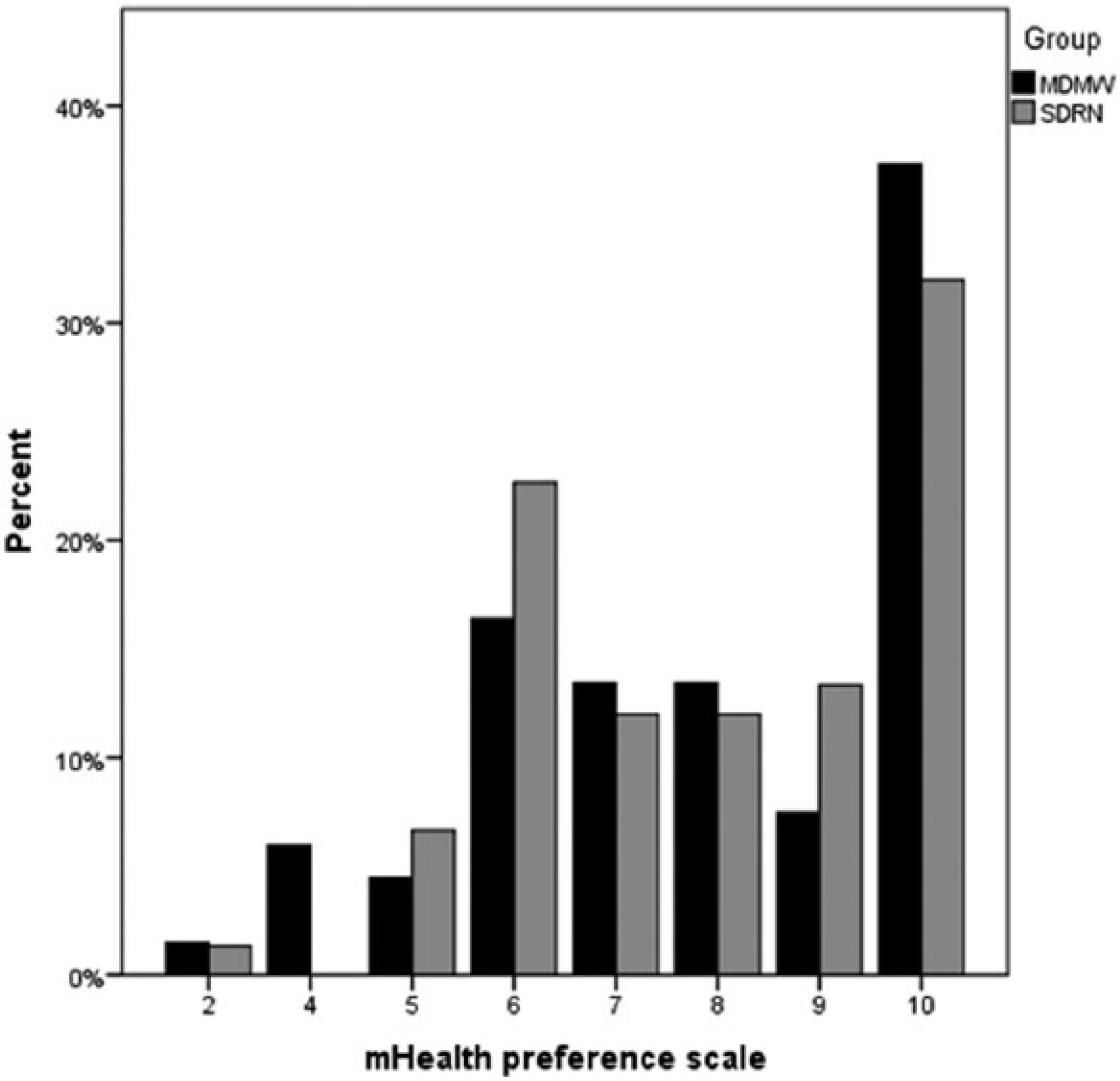
mHealth preference scale by respondents’ group. Percentages calculated using group totals (MDMW: n = 67, SDRN n = 75) as denominator.
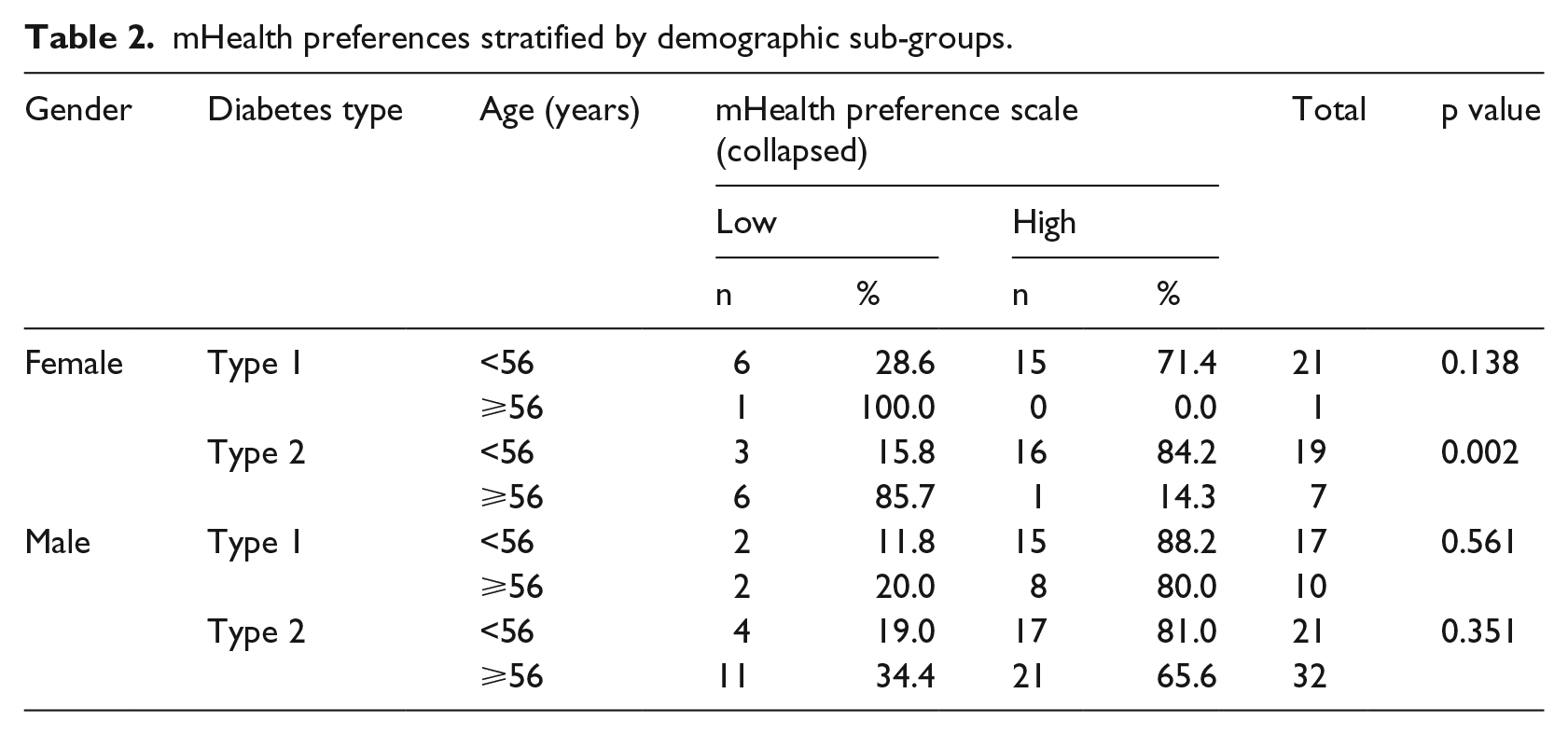
The four-way loglinear analysis produced a final model that retained the interaction between gender, mHealth preference and age (χ2 (1) = 4.16, p = 0.04) as well as diabetes type and age (χ2 (1) = 9.58, p = 0.02). The former was explored in greater detail. There was a highly significant association between age and mHealth preference for women with T2D (p = 0.002) but not T1D, whereas there was no such association in men – see Table 2. Odds ratios indicated that women ⩾56 years of age (with T1D or T2D) were 28 times less likely than younger women to express a preference for mHealth applications to help with their diabetes. In comparison, older men (with T1D or T2D) were only two times less likely to express a preference when compared to younger men.
mHealth preferences stratified by demographic sub-groups.
Smartphones and use of technology for diabetes
With regard to current use of technology, of the 144 people who owned a smartphone, 121 (84%) used their phone more than once a day. The use of the two main operating systems was roughly equivalent (Android: 69/144, 48%; iOS: 57/144, 40%). Both men and women ⩾56 years of age were significantly less likely to find the use of smartphone apps ‘enjoyable’ when compared with younger adults (females who found apps enjoyable: ⩾56 years 1/8 (12.5%) vs 26/41 (63.4%) < 56 years, p = 0.001; males who found apps enjoyable: ⩾56 years 20/44 (45.5%) vs 28/39 (71.7%) < 56 years, p = 0.042).
In all, 176/229 (76.9%) respondents reported that they needed to check blood glucose regularly as part of their diabetes self-care, including the majority of those with T2D (T1D: 89/90, 98%; T2D: 87/139, 63%). Of those who did use blood glucose monitoring as part of their diabetes self-management, the majority did not use any device to remind them to do so (116/163, 71.8% (NB. 13 individuals did not respond)) (response to the question: How do you remind yourself to take medication and/or check blood sugars? Tick all that apply from the following: Just remember without aids/I use an alarm/I have a set routine/I use my phone to set reminders/Someone Reminds Me/Somebody (carer, relative or friend) does it for me), with no significant differences between demographic sub-groups (data not shown). The most common way of recording the result was via the monitor device (87/163, 53.4%) or a written diary (56/163, 34.4%). Use of other technologies was minimal − 12/163 (7.4%) used their phone and 17/163 (10.4%) used their home computer (via a spreadsheet). The only significant difference between age categories for either gender was that women ⩾56 years were significantly less likely to use their home blood glucose monitor (HBGM) to record results (9/24, 37.5% women ⩾56 years vs 28/43, 65.1% women < 56 years, p = 0.027).
Preferences for mobile technology use and app features
Preferences were analysed with respect to diabetes type. Response rates for each of the suggested features varied between 84–87/91 (92–96%) for those with type 1 diabetes and 123–135/139 (88%−97%) for those with type 2 diabetes. If available, the feature that both types of users would most commonly use was password protection (47/84, 56% for T1D and 89/129, 69% for T2D) – see Figure 2. Thereafter, approximately 40–50 per cent of respondents indicated that they would use the various suggested features, irrespective of diabetes type, for example, preference for features relating to activity and exercise did not differ markedly between those with T1D and T2D.
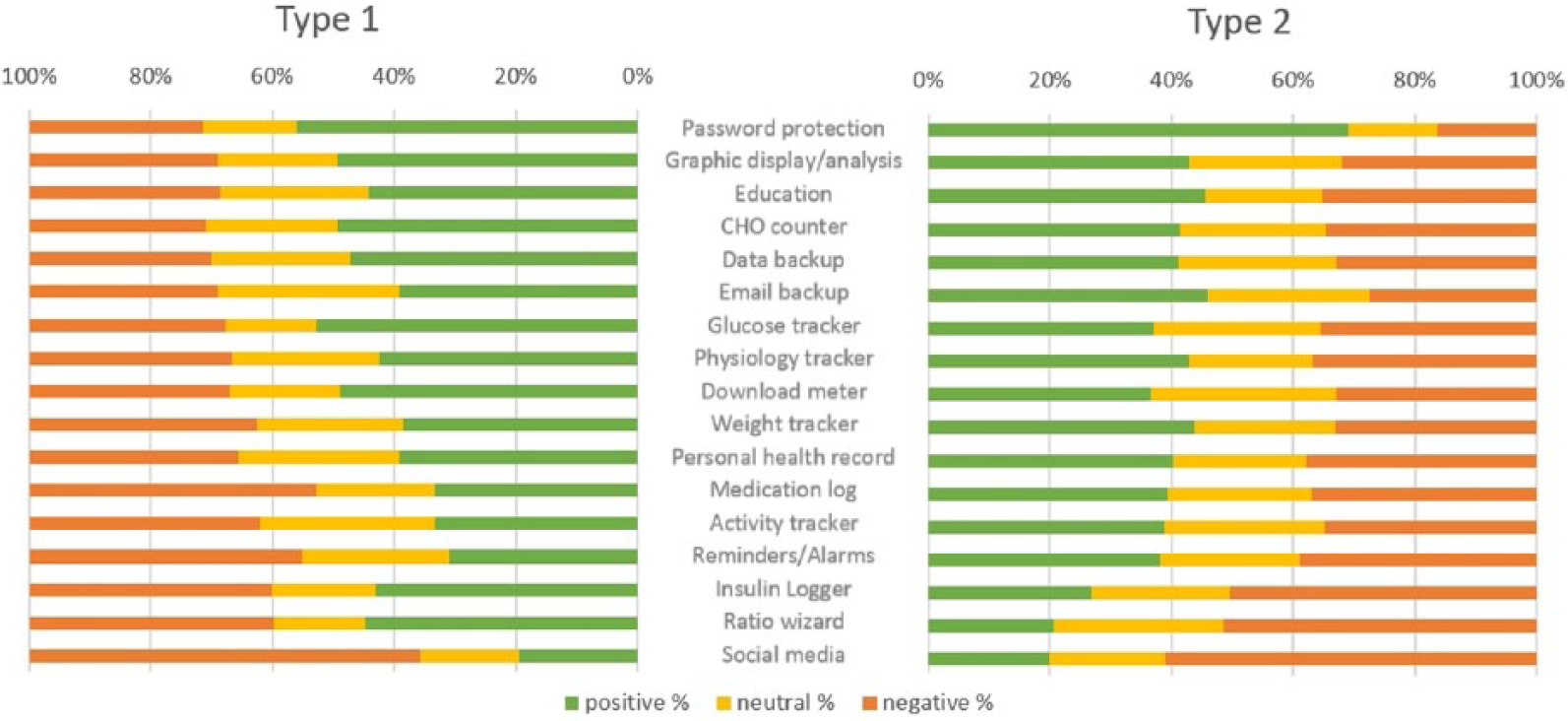
Preferred features of an mHealth app, stratified by diabetes type. Features are arranged in descending order of preference (T1D and T2D combined). Denominators for preference vary depending on number of respondents to each item (total n = 213–226). ‘Strongly agree’ and ‘agree’ were categorised as being positive responses. ‘Strongly disagree’ or ‘disagree’ responses were categorised as being negative.
Diabetes type did have some influence on the types of features that would be desirable, for example, those with T1D showed higher preference for a ratio wizard (39/87, 45% vs 25/122, 21%; p < 0.001) and logging of insulin (38/88, 43% vs 33/123, 27%; p = 0.02). If this comparison was restricted to only those who used insulin, this significance was lost or reduced (ratio wizard: 39/87 vs 10/40 p < 0.05; insulin logger 38/88 vs 13/39, p = 0.07). Preference for a glucose-monitoring feature was also higher for those with T1D (T1D: 46/87, 53%; T2D 50/135, 37%; p = 0.03). Again, there was no such difference between diabetes types if analysis was restricted to those who self-monitor blood glucose (46/87 vs 32/85, p = 0.1).
The lowest rated feature was social media integration (positive response: T1D 17/87, 20%; T2D 26/131, 20%). Preference for social media integration was compared with respect to age group, with those < 56 years demonstrating higher preference (30/97, 30.9% positive) to those ⩾56 years (14/108, 13.0%, p = 0.008). This significance was lost when stratified by gender, owing to smaller numbers.
Discussion
This study has demonstrated interesting insights regarding the use and preferences for mobile technology in a diverse diabetes population. In general, smartphone ownership and use was high and in keeping with UK usage. 21 However, users did not tend to use these or other technologies when managing their diabetes. For example, for those who use SMBG, approximately a quarter used some form of reminder (e.g. alarm on phone) to do so. Half of this group used their blood glucose monitor to record their results and a small minority used some form of other technology (e.g. spreadsheet on desktop computer). It is perhaps unsurprising, therefore, that when asked about preferences for app development, a minority felt that reminders and alarms in an app would be useful, and less than half felt similarly for the inclusion of the facility to record blood glucose data using an app. This contrasts with Dobson and Hall 22 who concluded that the majority of respondents would welcome the ability to track blood glucose data.
A comprehensive review of app features currently available concluded that usability is inversely correlated with number of features contained within the app. 7 In our study, there was a marked contrast between the availability of features on the apps included in the snapshot analysis and the features that users showed greater preference for. For example, the majority of respondents indicated that patient education would be a useful addition to an app, whereas this feature is currently only available in a minority of apps. There was a notable lack of enthusiasm for social media integration with any future app development – while younger people were significantly more likely to show preference for this feature, only one-fifth of respondents were positive overall.
The digital diabetes landscape has grown rapidly over the past decade and there is evidence that web-based interventions can lead to improved clinical outcomes.11,12 The use of mHealth applications has the potential to improve access to such services, thereby addressing a key component of the ‘digital divide’. 23 However, there is increasing evidence that Internet usage patterns reflect underlying demographic and socioeconomic differences, with the potential to increase health inequalities. 24 In this study, most respondents expressed a preference for mHealth apps to manage their diabetes; however, gender, diabetes type and age were significant confounders – women ⩾56 years were significantly less likely to express a preference for mHealth apps. This is in keeping with findings from elsewhere 22 Again, this has implications for future app development in terms of ensuring that population sub-groups do not feel alienated or become disenfranchised.
Limitations
There are a number of limitations acknowledged in this study. The sample size was one of convenience as opposed to the result of a power calculation. The use of stratified sampling from more than one dataset ensured that the respondents included sub-groups of the wider diabetes community in terms of diabetes type and age, although the number of those with T1D was over-represented when compared with national data. 20 In addition, low numbers in certain demographic sub-groups (e.g. older women) make it difficult to make robust statistical inference. Young people < 16 years old were not included, and it could be argued that this user group would provide a very different perspective on the use of mHealth technologies. It should also be noted that the MDMW and SDRN cohorts may have some inherent biases in that both datasets may represent a more engaged section of the diabetes community – they have all given prior consent to be contacted for research and all those contacted were Internet users (contact was via email address). In addition, subscribers to the online MDMW portal are probably more likely to be engaged with modern technology, tend to be younger and, by implication, have less comorbidities. While not being representative of the wider diabetes community, it could be argued that the sample demographic is a potential strength of the study as this population is more likely to use mHealth technologies. We did not gather data on questionnaire respondents’ ethnicity. The sample was drawn from a population who are 96 per cent White. 25 This limits the generalisability to other populations, given that ethnicity is associated with the likelihood of engaging with mHealth technologies. 26 Another potential shortcoming is that the use of categorical responses introduced limitations to the analysis. However, the relatively high response rate can in part be attributable to the ease in which the questionnaire can be completed, and so we believe this design was justified. The search strategy of available apps was limited in terms of search terms and marketplace (iOS apps only). The decision to limit the search in this way was a pragmatic choice that was primarily intended to inform questionnaire design. We believe the results to be representative of the wider app market.
Conclusion
The growing prevalence of diabetes accounts for an ever-increasing proportion of healthcare spending. There is a recognised need to improve the way that care is delivered to provide a more sustainable and person-centred service. The integration of mHealth technologies within existing informatics systems has the potential to empower patients, increase patient choice, improve outcomes and provide service in a different and sustainable way.
This study has demonstrated that in this sample of people with diabetes, most would welcome the development of mHealth technologies to help manage their condition. However, we have also shown that the functionality of existing apps does not currently meet the preferences of this potential user group. Both functionality and user engagement could be improved by including relevant stakeholders in future app development, which should be driven by clinical and user need as opposed to what is easiest to develop.
Footnotes
Acknowledgements
The authors thank the patients and staff of the Scottish Diabetes Research Network and also thank the patients and staff of My Diabetes My Way.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: I.C. was supported to complete this work via a Dundee Clinical Academic Track scholarship awarded by the University of Dundee.
Supplementary material
Access to research materials, including questionnaire and data, is available from the corresponding author.