
Abstract
Intelligent cognitive assistants support people who need help performing everyday tasks by detecting when problems occur and providing tailored and context-sensitive assistance. Spoken dialogue interfaces allow users to interact with intelligent cognitive assistants while focusing on the task at hand. In order to establish requirements for voice interfaces to intelligent cognitive assistants, we conducted three focus groups with people with dementia, carers, and older people without a diagnosis of dementia. Analysis of the focus group data showed that voice and interaction style should be chosen based on the preferences of the user, not those of the carer. For people with dementia, the intelligent cognitive assistant should act like a patient, encouraging guide, while for older people without dementia, assistance should be to the point and not patronising. The intelligent cognitive assistant should be able to adapt to cognitive decline.
Introduction
With people living longer than ever, the incidence of dementia is rising steeply.1–3 Since two-thirds of people with dementia live in the community, 1 we need innovative solutions for supporting their independence and reducing the strain on carers. As dementia is progressive, these solutions should be able to adapt to changes in cognitive abilities.
Although assistive technology should be intuitive, easy to use, and robust, in practice, it is highly likely that people will encounter problems when using the system. This could be because they need rarely used functionality or because the system does not work as expected.
In the Cognitive Assistant with Dialogue to ENhance Communication and Engagement (CADENCE) project, we designed a high-fidelity simulated intelligent cognitive assistant (ICA) that helps users with and without cognitive impairment to navigate the simple calendar system. We chose a calendar application because orientation in time is important for people with dementia. 4 While previous work on ICAs has focused on helping people with tasks of daily living,5,6 the CADENCE ICA is one of the first ICAs that assists people with using technology.
In this article, we present findings from user requirements work with older people, older people with dementia, and carers who informed the design of our ICA. We focused on two research questions:
How acceptable are ICAs to people with and without dementia?
How should the ICA be adapted to cover the different needs of older people and people with dementia?
Assistants for supporting people with dementia
Why voice interfaces?
Dementia is an umbrella term for many conditions that cause cognitive impairment. Char-acteristic symptoms include progressive loss of memory, increasingly impaired reasoning, decision-making and visuo-spatial awareness, and increasing difficulty with communication and carrying out activities of daily living. The most prevalent form of dementia is Alzheimer’s disease (AD). 3
Since language comprehension and production is comparatively well-preserved in people with mild to moderate AD, 7 voice prompts can be helpful for this user group. So far, voice and text prompts have been mainly used in reminders and memory aids.8–13
Unfortunately, there is still comparatively little empirical work on designing voice interfaces for older users with or without cognitive impairment. It is difficult to extrapolate from knowledge of cognitive ageing to the usability problems that older users will encounter,14,15 not least because the trajectory of cognitive ageing is incredibly diverse. Existing work includes design patterns, 16 databases of interactions between older people and interactive voice response systems, 17 and voice interfaces for specific applications.10,18,19
ICAs for older people
ICAs improve upon traditional memory aids using sophisticated planning algorithms to adapt message content and timing to the user’s current situation. These algorithms can be statistical5,20 or rule based.6,21
An example of a working ICA is the COACH system, 5 which guides people with moderate to severe dementia through the procedure of washing their hands. Task progress is monitored using computer vision. If a person encounters problems, the ICA provides a prompt based on an explicit model of the hand-washing task.
The GUIDE system adopts a different approach. Users are led through the process of putting on a prosthetic limb through prompts and questions, and they can indicate success, failure, or problems with understanding the system using five one-word spoken commands.5,21
The timing and wording of prompts can be influenced by a number of factors, including the effectiveness of the prompts at facilitating the user to complete the task, the current state of the system, and the likely emotional response of the user. By weighting these factors in different ways, a range of strategies for helping people with dementia can be implemented. This allows us to tailor the support provided by the ICA to the extent of cognitive impairment, stress levels, and the number of tasks that users are carrying out at any one time. 22
COACH provides verbal prompts but cannot react to verbal user feedback. This is a major limitation. In recent trials, people with dementia sometimes responded to the prompts by asking for clarification or disputing an incorrect prompt. 5 While the GUIDE interactive assistant allows user feedback, speech recognition is limited to five words. GUIDE is designed for talk users through the whole process – unlike COACH, which intervenes only when needed – which makes dialogue design more difficult.
From a dialogue design point of view, COACH and GUIDE are situated on different points of the user initiative versus system initiative dimension. While GUIDE is completely system initiative and talks users through each step, COACH intervenes only when problems are detected. In addition, COACH is multimodal as it integrates sensor-derived input into its planning decisions, whereas the unimodal GUIDE system relies on verbal user feedback.
Scoping the design space
In the focus group work, we focused on three aspects of the ICA design space: timing of help prompts (system initiative vs user initiative), affective support, and the personality projected by the ICA. While COACH and GUIDE both use different approaches to timing prompts, it is not clear how their chosen approach interacts with the usability of the system and the user’s locus of control. Wolters et al. 23 showed that older users are more likely to use words that the system can understand when help is given at the beginning of a task. On the other hand, users who have a strong internal locus of control may prefer to ask the system for help themselves – an ICA that prompts at the first sign of a potential problem could be seen to be demeaning and patronising.
Affective support was included because people with dementia may show intense frustration when interacting with ICAs, 5 for example, when they fail to complete a task despite assistance or when they receive incorrect or misleading help. While providing appropriate assistance goes a long way towards avoiding frustration and distress, adequate affective behaviour may be just as important. 24 Since the personality projected by a spoken dialogue interface affects usability and user experience, 25 we also asked participants to comment on the persona projected by the ICA through its voice, the wording of its prompts, and the dialogue management strategies used.
Design and methods
We conducted three focus groups with people with dementia, family caregivers, and older people without a diagnosis of dementia on their views. Table 1 provides more detail about focus group composition and location. Groups lasted about 1.5 h. They were facilitated by a researcher who was experienced in working with people with dementia, a second researcher took notes and clarified technology-related questions. Groups were audio-recorded with participants’ permission and transcribed orthographically.
List of focus groups.
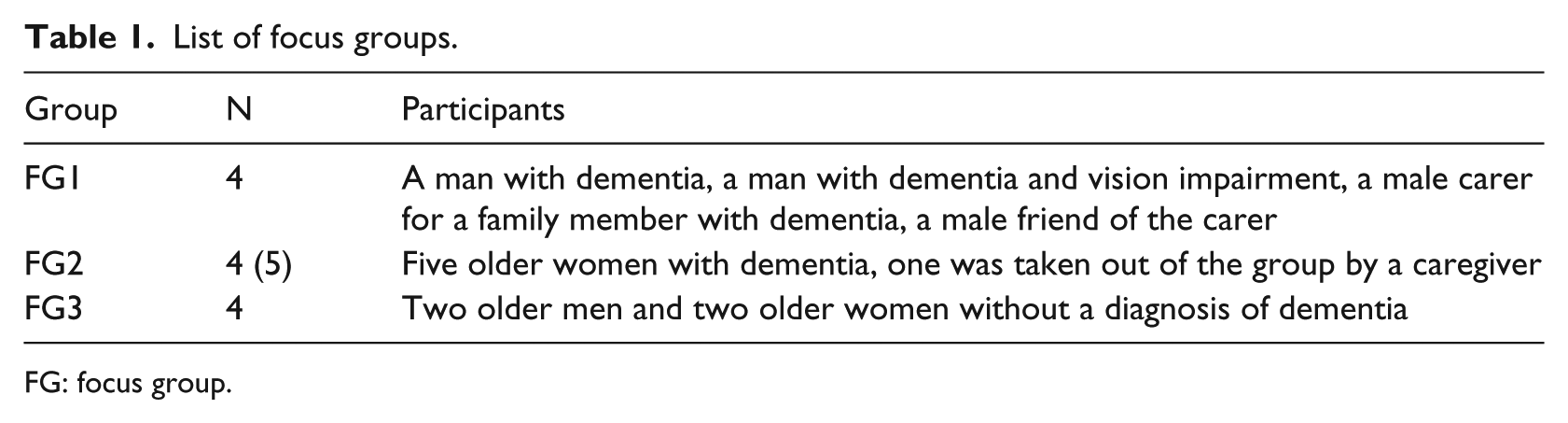
FG: focus group.
Recruitment, ethics, and consent
Ethical approval for the focus groups was obtained from the research ethics committee of the School of Applied Social Science, University of Stirling. Ethical procedures of informed consent, confidentiality, anonymity, prevention of harm, and secure storage of data were followed. Informal carers (family and friends) and people with dementia were recruited through a local Dementia Café; older people with no diagnosis of dementia were recruited through the University of Edinburgh Psychology Participant Pool.
The focus groups with people with dementia and carers were held in the familiar environment of the Dementia Café, the focus group with older people took place in a University meeting room. All six people with dementia were able to give informed consent and still lived in the community. Four lived on their own and two with their spouses. All group members had socialised with each other before at the Dementia Café, were comfortable with talking to each other, and had met the researchers on a separate occasion before the focus groups were conducted.
Participants without dementia were invited to read the information sheet and ask questions before signing the consent forms. People with dementia were talked through the information rather than reading it if they preferred. Once participants understood the information and had the opportunity to ask questions, they were invited to sign the consent form. Again, some participants needed guidance with this on an individual level. Consent was viewed as ongoing,26,27 in that the researchers were alert to signals of withdrawal of consent and accommodated these. While no participants withdrew consent themselves, one participant was removed from the focus group by a caregiver shortly after the consent procedure had been completed. Recording was stopped and restarted, and data from this participant was excluded from the analysis.
Structure of focus groups
All focus groups followed the same schedule, summarised in Figure 1. They were structured around a 2-min DVD showing a sample interaction with an ICA. A screenshot is shown in Figure 2. We chose to record a short film because we did not have a working demonstrator, we wanted to consult people with dementia in a familiar setting, which precluded the use of theatre, and we wanted to ensure that all focus groups received the same information about the abilities and limitations of the ICA.
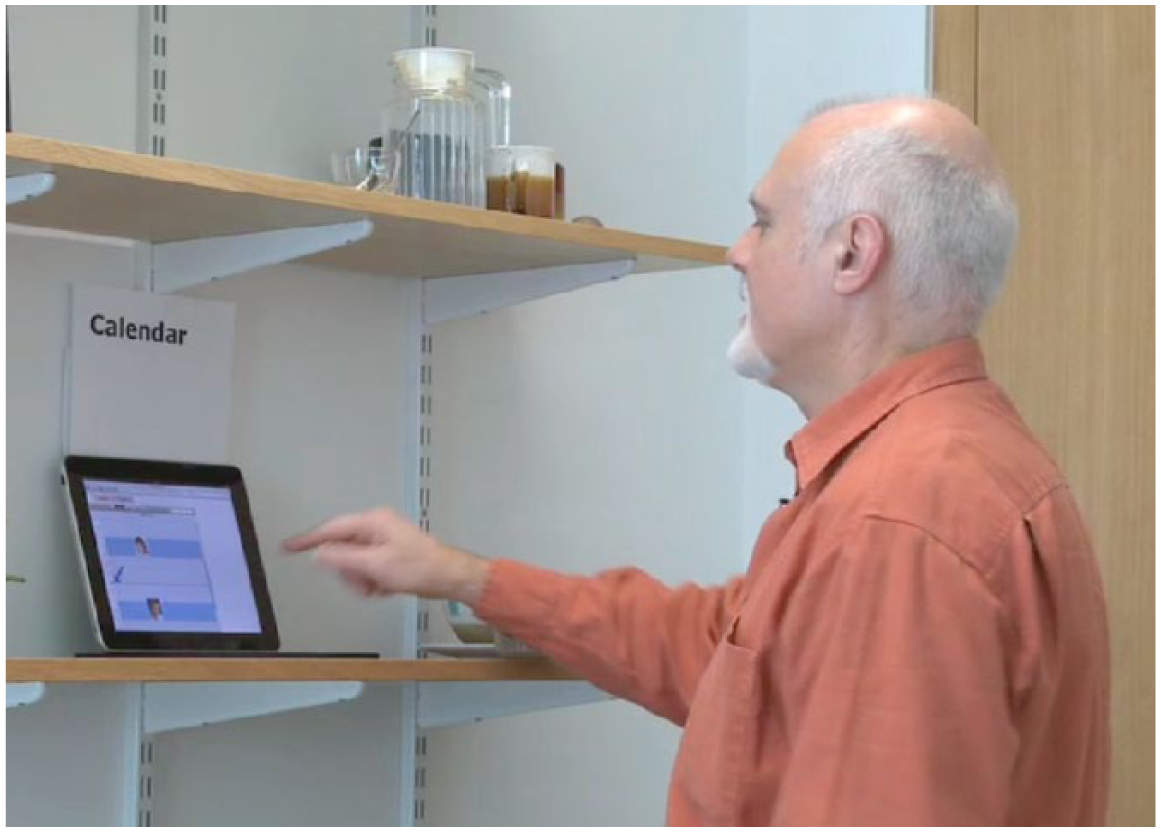
Screenshot of the video: The older user, played by an actor, is talking to the ICA while looking for information on the calendar, shown on the iPad.
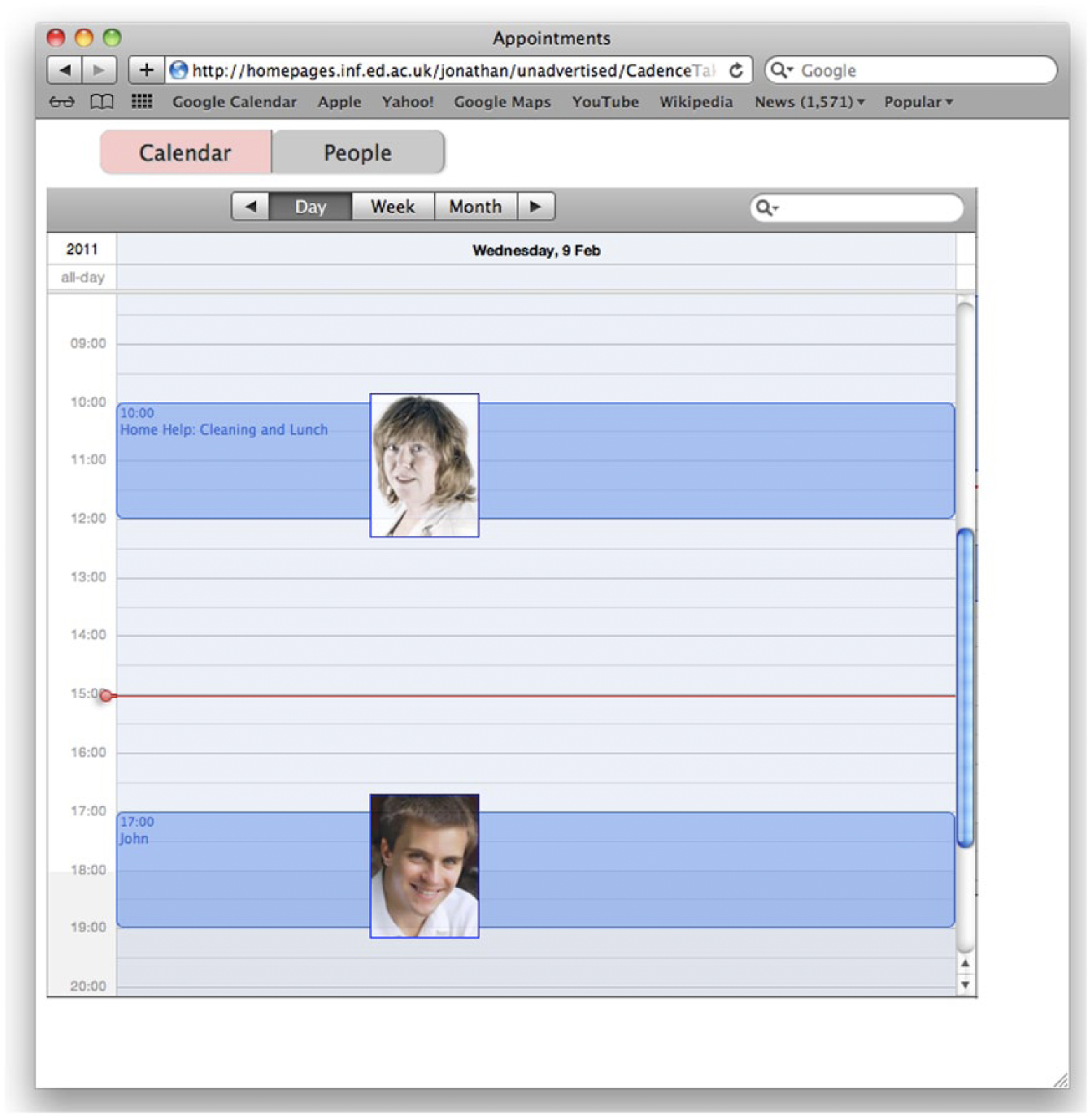
A view of the calendar, showing pictures of the people who are coming together with the appointment date and time.
In the film, a person with dementia, played by an older actor, asked the ICA for help in obtaining information from the simple calendar system (see Figure 3). Verbal prompts were accompanied by highlighting key interface elements on the screen. The ICA’s prompts were spoken by a computer-generated male voice with a local accent.
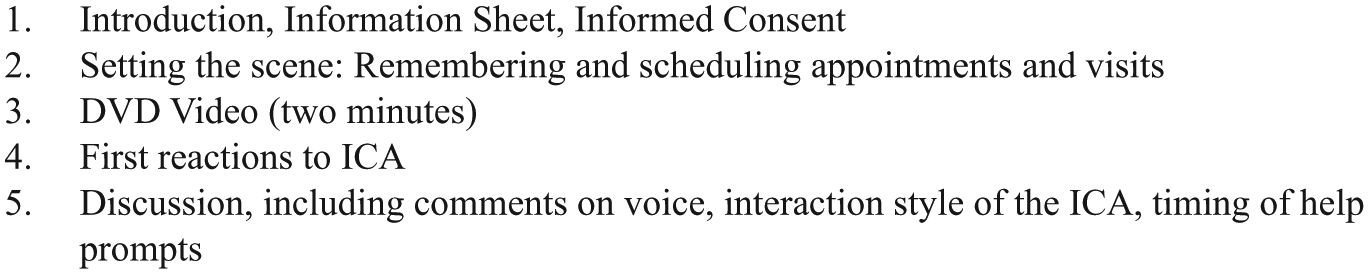
Overview of focus group schedule.
The script was carefully designed to show a realistic ICA with limited speech recognition and natural language understanding capabilities. In order to highlight problems that might occur during the use of ICAs, we included a segment where a problem with recognising the user’s speech was successfully resolved.
Analysis
Audio-recordings were transcribed verbatim and transcripts were examined and coded by one researcher using the topic guide for initial identification of themes; these were verified by the other researcher. Initial themes were refined further to capture subtle differences between participants’ views on technology and ICAs. All data were managed in NVivo 8. 28
Findings
Findings from the focus groups will be discussed under the following headings: participants’ views on technology, views on acceptability of ICAs, views on the three design aspects (voice, motivation, and help prompts), and suggestions for extending the ICA. Participant IDs consist of the focus group number (FG1, FG2, and FG3) followed by an indicator of gender (M/F) and an ID number.
Views on technology
Participants varied in the technology they owned, the technology they used, their sense of proficiency, and their attitudes towards technology. Both carers in focus group 1 used computers and other technologies such as smartphones regularly and were comfortable using them.
Two aspects emerge as important: being familiar with technology (‘used to using it’) and having successfully mastered the initial learning curve that comes even with very user-friendly devices:
So I’m very used to using that kind of stuff. So I’ve always used it. And now with the iPhone, it’s dead simple to use these kinds of things, you know – if you know how to use them, that is. But you need to know how to use them. (Carer, FG1M4) I mean the young grow up with it and the young can work computers and things … but for our generation there is this block and there is so many people that don’t actually use computers at all so they don’t have even that background of what is possible. (Person without dementia, FG3F1)
People with dementia vary markedly in their acceptance of technology. While one man with dementia in FG1 reported using his computer to play cognitively stimulating games, the other man with dementia, who also had a visual impairment, expressed profound frustration:
I’ve enough trouble with the phone. It beeps and I don’t know what it is. I haven’t a clue. (Person with dementia, FG1M2)
Although FG1M2 had state-of-the-art technology such as a computer and cable TV at home, he did not use them except when somebody else was there to help him.
Views on the ICA
Having watched the 2-min DVD, most carers and people with dementia reacted positively to the concept of the speaking ICA. Two participants with dementia felt they would prefer to stick with their paper calendars, although one of them did like the concept of an ICA:
What did you think of the actual idea of having a calendar that talks to you? (Researcher) It’s excellent. (Person with dementia, FG2F3) Yes, excellent. (Person with dementia, FG2F1)
The older people without dementia in FG3 were less enthusiastic. Two participants reported that they found the ICA to be patronising. The dialogue reminded one participant in FG3 of interactive voice response systems that are widely used in telephone-based services and that have negative connotations for her:
I agree, sometimes voice recognition is very, it can be patronising … and I find that it’s like these voice recognition when you phone somebody up, you know, press two, press three, and it doesn’t do me any good because I feel I just want to talk to somebody. (Person without dementia, FG3F1)
Timing of help prompts
Most participants felt that they would only want the prompt if they needed help:
If I was needing help I would appreciate the voice but I don’t think I would use it if I wasn’t needing help. (Person with dementia, FG2F4)
Participants doubted whether the ICA would be sufficiently proactive and identify what assistance would be required:
But if it says do you want help, the help has to be appropriate and that’s the difficult bit. (Person without dementia, FG3F1)
In all three groups, participants also highlighted that the ICA would need to respond appropriately to deteriorating cognitive or physical ability. For example, people with deteriorating vision and cognition might need to have the content of the screen magnified or read out to them:
Well, I wouldn’t know if I’m managing or if I’m not managing, or if I’m getting worse or not getting worse. How would it (the application) know? (Person with dementia, FG1M2) You know, her writing skills went first and then her reading skills followed soon after … That’s what I found. X couldn’t have done that. No, she couldn’t have read that to see if he was coming. (Carer, FG1M3)
Motivation to support learning
A major problem with using technology was the steep learning curve. Setbacks were experienced as very frustrating, and the technology was seen as requiring much concentration:
Aye, because well, I haven’t got a computer … but I don’t think I could content myself to sit and learn it, you know, I would get quite frustrated learning … I don’t think I would have the concentration to learn the computer. […] But I’m all for progress really but I would need to learn it. That’s the difference; I would need to learn it. (Person with dementia, FG2F4)
If a person fails to use an application successfully on their own, there is a substantial risk that the person might give up using the application altogether:
Well, that’s what happened with my video, you know. X (friend) showed me how to do it, the next day I tried and it didn’t work out exactly how it should do, and I never tried it again. (Person with dementia, FG1M2)
Another participant with dementia, however, reported a success story where she had successfully learned to use a simple assistive technology device after a social worker had set it up for her and shown her how to use it. FG1M2 felt that in his case, the key to success might be frequent repetition and ongoing support:
As I say, if someone was sitting with me and saying, right, do that, and they were back the next day to say right, we’ll do this again, once I had done it two or three times … I would be able to do it then.
Which voice, which interface?
While carers and people with dementia liked the ICA’s voice, in particular the local accent, the voice was not acceptable to participants in FG3 because it sounded too mechanical.
Most participants agreed that the ICA as shown in the DVD could be improved but disagreed on the improvements they would prefer. Participants also disagreed about the desired voice characteristics. Many suggested that the voice should sound familiar, speaking with a local or an acceptable standard accent. One participant with dementia suggested a local accent would be useful and another with dementia preferred an ordinary, clear voice ‘with no affectations’, while a participant without dementia suggested an accent that was ‘not strong for any region at all’.
While the carers agreed that the voice should be that of a spouse or family member, some participants with dementia were very clear that they did not want their spouses’ or children’s voices used:
I think that most people would feel better if it was a voice that they recognised on that, rather than a strange voice. (Carer, FG1M3) But it’s our like age groups, the age of our age groups we know them whereas the younger voice is like my son talking down, you know, not talking down to me, but you know what I mean it’s like … my son saying mum you should be doing this. (Person with dementia, FG2F1)
Another participant with dementia, when asked whether he would rather have his wife’s voice, was clear that whose voice it was did not matter to him; the important thing for him would be having the application.
Future perspectives
Some participants were not sure about the acceptability of a voice without a face. Specifically, one participant with dementia, FG2F4 felt that a voice would not be sufficient to hold her attention for long enough. She suggested that having a face to the voice – preferably ‘a very handsome face’ would be helpful. This stimulated a lively discussion about the merits of different actors’ faces and voices.
The original objective of the ICA was to talk with participants through the steps needed to complete simple activities on their own. However, many participants with dementia also suggested additional functionality that would go beyond the original remit of the ICA.
One participant would like a reminder functionality to ‘jog’ her into action when an important appointment was coming up:
It would have jogged my brain … I don’t think I would have got a fright cause by that time I possibly would be used to it, to the voice. But if somebody said to me remember … in a, not an unpleasant voice but a nice voice, that would definitely have shook me. And I thought, oh gosh, that’s like the alarm clock going off. (Person with dementia, FG2F1)
Another participant with dementia highlighted that users might come to view the ICA as a companion:
Cause just sometimes just having somebody to talk to … is a help because we can’t always say ‘my husband will be here or be there’ or some people haven’t got a husband … you know, but anyway with these things it could help them couldn’t it? You’d have somebody to talk to, maybe make a nuisance of themselves but there’s somebody there at the end of the line for them isn’t there. (Person with dementia, FG2F4)
Discussion
The design metaphor for the ICA interface that emerged from the theme ‘motivation to support learning’ was a competent, patient, and friendly guide that gives users the confidence they need to attempt the tasks themselves. This confirms the findings of O’Neill et al., 6 who modelled their GUIDE system on the verbal scaffolding provided by an experienced carer.
There were clear differences between the views of carers, people with dementia, and the older participants without dementia from FG3. While the older people from FG3 were on the fence about the idea of an ICA, and perceived it as patronising, the carers and most of the participants with dementia saw clear benefits. People with dementia particularly valued the independence an ICA would give them.
It is crucial that the user can personalise the ICA themselves. For example, while carers wanted a family member’s voice, people with dementia did not want to feel nagged by their family carers. The ICA’s main user should be able to choose from a range of familiar, clear voices, with a light regional or a standard accent that should sound as natural as possible.
An important aspect is having someone to talk to. Wu et al. 29 found that older people with memory problems identified cognitive stimulation as the most important function of a companion technology. But this is also a challenge, as users may not understand the limitations of the ICA and expect it to provide additional functionality, such as reminder prompts. Users may also fall into a chatty, sociable interaction style, 30 treating the ICA as a companion, which could be highly problematic for the speech recognition and natural language understanding components of the voice interface.
ICAs also need to be sufficiently flexible to accommodate users with different cognitive, motor, and sensory abilities. Most of our participants were sceptical that this could be achieved, given the range of ability encountered in people with dementia. However, the COACH system 5 has been used successfully for people with moderate to severe dementia without further adjustments. Through iterative development and participatory design, an ICA that is designed to learn from failure can easily accommodate changes in cognitive function.
This study is limited scope in that we only conducted three focus groups, there were no focus groups just with carers, and none with social workers and health-care professionals. We also do not know the exact diagnoses of the people with dementia who participated because we recruited through a Dementia Café, a setting where people knew each other, and felt comfortable, and not through the National Health Service.
Despite these limitations, the interface metaphor that emerged is supported by all three focus groups. While we did not consult with older people with minor cognitive impairment or self-reported memory problems, we would expect that ICAs for this group should use an interaction style that is geared towards older people without dementia, since they are more likely to see themselves as not needing help.
Conclusion
Our study provides qualitative evidence to assist with the design of voice interfaces to ICAs that support users with complex tasks, such as interacting with technology. The diversity of opinions we encountered further highlights the importance of including people with dementia in the requirement process. While this may seem daunting, it reflects best practice in the design of dementia services and policies31,32 and of technology for people with dementia.33–36
In our focus groups, we took care to present a realistic view of a voice interface that shows what can be achieved with the existing technology. The suggested design metaphor is a friendly, patient instructor, who adapts their interaction style to the needs of the individual user.
However, ICAs are not band-aids for bad design. In fact, within the range of tasks where users could benefit from assistance, 37 it appears that helping people with using technology may be just as hard as wayfinding, which has proved extremely difficult to automate, challenging even for experienced care professionals. 38 New learning, both for the underlying application 11 and for interacting with the ICA, should be minimal.
ICAs are not a free pass to deploy technology where it is not needed: If a person already has a tried and trusted system in place (such as the detailed diary kept by FG2F3, a participant with dementia), then replacing it with technology is likely to fail, even with ICA guidance.
Based on our focus group work, we have created a simulated ICA and tested it with users with and without cognitive impairment. 39 Results show that more mixed methods work is needed to flesh out the ‘friendly guide’ persona suggested in this article. Future versions of the ICA should also integrate multimodal prompts using voice and video or haptic feedback as and when appropriate.40,41
Footnotes
Acknowledgements
The authors thank those who took part in the focus groups and those who helped to make them happen. The idea for CADENCE was developed in consultation with Jesse Hoey from the original COACH team. The script for the probe video and the design of the study benefited greatly from the feedback of our colleagues on the CADENCE project, Myroslava Dzikovska, Jesse Hoey, Sarah MacPherson, and Johanna Moore.
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research was funded by Grant no. F/00158/CP from The Leverhulme Trust (Professor Johanna Moore, PI).