
Abstract
E-health holds the promise of changing the delivery of health care by extending and enhancing its reach, and democratizing and improving the access of disadvantaged groups to health care services. This study investigated ethnic inequalities in access to e-health information, communication and electronic services in Israel. Based on the diversification hypothesis, we expected that disadvantaged ethnic groups would be more likely to use e-health services to compensate for their lack of social capital. Data gathered from a representative sample of Internet users in Israel (n=1371) provided partial support for the hypothesis, indicating that in multicultural societies, disadvantaged groups are more motivated than the majority group to use the Internet to access medical information. However, despite expectations, minority groups were less likely to access e-health services. Implications of the findings are discussed.
Keywords
The Internet has emerged as a valuable source for acquiring health information and accessing health services. According to recent surveys, 72 percent of US adults look online for health information. 1 A study of seven countries in Europe reports that the percentage of the population that has used the Internet for health purposes increased from an estimated 42.3 percent in 2005 to an estimated 52.2 percent in 2007. 2 A study in Middle Eastern countries investigated the use of the Internet to search for online information about the proper use of drugs, their side effects, and interactions found that 88 percent of those using the Internet reported using it to search for drug information. Two-thirds indicated that they searched for information on side effects, one-third looked for instructions about how to use the drug properly, and the rest sought guidance about the interactions of particular drugs with other drugs and food. 3 In addition to providing access to information, the Internet also links individuals with healthcare professionals and with those who share their health issues. Twenty percent of Americans have consulted online reviews of healthcare service providers, and 18 percent of Internet users say they have gone online to find others who might have health concerns similar to theirs. 1 In the same vein, a study conducted in Arab countries found that 67 percent of physicians reported having patients discuss health information they found online with them. 3
There is broad consensus that e-health, defined as the use of information and communications technologies in support of health and health-related fields, has enormous potential to benefit healthcare consumers. 4 Access to e-health services empowers patients, providing new opportunities to access and exchange health information, manage their health, and communicate with healthcare providers. 5 E-health also promises to benefit consumers through improvements in medication management and patient monitoring. 6
Studies have shown an increase in the use of e-health services over time. A recent longitudinal study in the United States investigated the use of three e-health services: buying medicines online, participating in online health-related support groups, and using e-mail to communicate with a doctor’s office. The use of any e-health service increased from 22 percent of the respondents in 2007 to 25 percent of the respondents in 2012, with online communication with physicians and the purchase of medicine showing the greatest increases. 7 One study in the Middle East documented an increase in the number of health-related websites in Arabic from 258 in 2006 to 335 in 2010. 8 However, the findings also point to social inequalities in access to such services, noting the persistent effect of limited education and income in perpetuating the lack of access to and use of e-health services by socially disadvantaged groups of the population. 9
Given that access to the Internet is becoming universal, it is important to determine how native-born individuals, immigrants, and disadvantaged minorities access e-health services and if this access varies based on their differential position in society and ethnic background.9–11 This study investigates these issues by examining the similarities and differences in the access to and use of e-health services by a disadvantaged minority (Arabs), recent immigrants (from the former Soviet Union (FSU)), and the native-born majority in Israel.
Theoretical background
Healthcare empowerment is defined as a mechanism by which individuals gain mastery over their health affairs. 12 The adoption of digital technologies to access online health information, communicate with health professionals, access health services, share experiences with others, and use digital devices to monitor their health are regarded as empowering healthcare consumers.12,13 Self-monitoring assumes an engaged patient who complies with requirements such as monitoring practices at certain times of the day and uploads personal experiences with medical treatment.
As Lupton 13 indicated, “Empowerment becomes a set of obligations” (p. 261) and compliance is dependent on existing social inequalities. Studies on e-health use among disadvantage minorities show that disadvantaged minorities are increasing the use of online health information and communication but remain disadvantaged in self-management and tracking behavior online.14,15
These e-health developments underscore the importance of assessing the extent to which the use of digital technologies for health empowerment improves access to information, health communication, and access to health services for traditionally vulnerable populations. These groups often suffer more from chronic diseases such as cancer, diabetes, and obesity than the general population. As access and use of online health information, communication, and services are critical for engaging in self-management, in this study we focus on the role of social inequalities in access to the antecedents of digitally based self-management and care.
As Internet access has increased worldwide, the literature on digital inequality has moved from a focus on the first to the second level of the digital divide. 14 Early studies centered on the socio-economic determinants of physical access to information and communication technologies (ICTs), generally reporting differences in access based on income, education, gender, and ethnicity. However, given that Internet access is reaching saturation in Western countries, scholars now focus on the extent and causes of differences in the use of digital technologies.14,15
The relevant literature posits two different and contradictory predictions. According to the stratification hypothesis, patterns of ICT use and adoption replicate existing social inequalities and may even exacerbate them.15,16 In the early and middle stages of technology adoption, users are more likely to be from higher income groups who have more education and technical skills. With time, the skills required for taking real advantage of the technology become more demanding, making it more difficult for later adopters to use it successfully.
This hypothesis relies on existing knowledge about the nature of association in stratified and multicultural societies and the expanding literature on social capital. 17 According to the literature on social stratification, multicultural societies are segregated according to ethnic and social class lines. In societies that reward individuals differently based on their income, prestige, and power, stratification systems result in the differential ability of individuals to gain access to residential locations and services because these services are allocated according to place of residence. 18 As a result, their choices in terms of access to health information and health services are limited to the ones that exist in their residential locations. Thus, residential segregation according to ethnic lines translates into limited opportunities for interaction with and access to the information that emerges from the social structuring of activities and location of services in society. 18 The social network perspective supports this argument, noting that a major source of social inequality is the persistent homophily or social similarity of social networks that replicates inequalities in access to information and social resources. Thus, the network similarity of disadvantaged groups is replicated in the information age in the form of inequality in access to valuable social capital including access to health services. 18
An alternative perspective argues that increasing adoption of digital technologies may reduce social inequalities including access information, communication with health practitioners, and access to health services. According to this argument, in post-industrial societies, the social profile of the online community will gradually broaden over time. 19 There is some recent evidence in support of this hypothesis, as the percentage of Internet use has increased over time. Furthermore, some studies conducted in recent years indicate that Internet use at home and work in the United States and certain European countries are associated with higher wages and increased access to health information, governmental, and financial services. 20 Specifically, the diversification hypothesis implies that computer-mediated communication provides a vehicle for overcoming existing social inequalities in access to information and social networks that results from the residential segregation in society. 21
The diversification perspective maintains that disadvantaged groups (due to migration status and ethnicity) will use the Internet to diversify their sources of information and social networks through computer-mediated communication. At the same time, majority groups will use the Internet more to maintain their existing levels of information, for example, through interpersonal communication and direct communication with health providers. 22 The evidence for this hypothesis is mixed. Some studies on ethnic differences in access to health information in the United States found that Hispanics reported a high level of agreement that the Internet is a helpful resource for health information, despite the fact that they were less likely than non-Hispanic Whites to have access to such information. 7 Only 35 percent of Hispanics in the United States obtain consumer health information from the Internet compared to 71 percent of non-Hispanic Whites. Another study did not find any differences between races in the search for health information search online but did find that Whites were more likely to communicate with their healthcare providers online. 23 Other studies have demonstrated that minority groups are more likely to search for health information online and be active participants in social networking sites. 24
Additional factors associated with the use of e-health resources
Several other factors must be considered with regard to the use of e-health resources.
Age
Our health deteriorates with age, and the need for health information increases. At the same time, age is a proxy for Internet skills. Studies have shown that individuals over 65 years old report less access to the Internet and find it harder than young people to use Internet browsers and search engines and navigate the Internet successfully. 25 Access to the Internet through mobile devices continues to be lower among the population over 65 years old than other age groups. A recent US report stated that only 12 percent of adults over 65 years of age have access to mobile devices compared to 32 percent over 50–54 years of age and 89 percent of adults over 30–49 years of age. 26 Consistent with this argument, studies on the effect of age on patterns of Internet use for health information show that age is negatively and significantly associated with the use of the Internet for health information and communication. 27 The use of mobile devices for access to health information for individuals over 65 years is still very limited. These results support the amplification effect, as age is negatively associated with Internet adoption and also with difficulties mastering basic navigation skills and might not be able to take advantage of the Internet as a source of health information and services. Therefore, in this study, we controlled for the effect of age.
Gender
Studies have shown that women are more likely to search for health-related information online and to use e-health services. 27 It is very likely that this effect reflects traditional gender role models that place higher expectations on women for providing care to family members.
Income
Studies on inequalities in access to online health information found that racial differences were less salient than socio-economic differences.24,28 Research has determined that regardless of race, the likelihood of accessing health information online is inversely associated with income.
Education
The level of education has important implications for the use of online health resources. Health literacy refers to the ability to understand medical information including drug prescriptions, the etiology of diseases, and the outcome of various health-related behaviors. Understanding the health information that is accessed online and assessing its validity require cognitive skills including the understanding of medical language. While we did not measure health literacy directly, it is generally accepted that education is a proxy for the cognitive skills needed for searching and evaluating health and medical information. Therefore, in this study, we controlled for the participants’ level of education.
Satisfaction with healthcare professionals
Some studies have argued that a lack of confidence in healthcare professionals may prompt the search for healthcare information online, leading to people replacing the advice they obtain online for consultations with healthcare professionals. 28 Therefore, in this study, we controlled for the participants’ satisfaction with their healthcare professionals.
Minorities and health in Israel
Israel is a multi-ethnic society. Approximately 79 percent of the population is Jewish, the remainder is Arab. Jewish immigrants have come to Israel in a sequence of waves. As a result, the Jewish population consists of various groups from different backgrounds. The Arab minority is a distinctive minority that became a minority after the creation of the State of Israel. They have a different language (Arabic), profess a different religion (the vast majority are Muslims), and preserve an autonomous cultural existence through a network of institutions (separate schools and religious institutions, mass media, and highly cohesive family units). 29 Israeli Arabs are full citizens of Israel but are economically disadvantaged in education and socio-economic status (SES) relative to Jews.30,31 In addition, most of the Arab population resides in peripheral areas of the country and in small localities in which they form the great majority of the population.
Another important group in the Israeli population is immigrants from the countries of the FSU. A large wave of migration started after 1989 shortly after the dissolution of the Soviet Union. Since then, it is estimated that 1 million immigrants from the FSU have arrived in Israel, constituting 15 percent of the total population and 20 percent of the Jewish population. The spatial distribution of the immigrants in the country is uneven, and they have become the majority of the population in many towns in Israel’s periphery.
Penetration of digital technologies into Israel
In Israel, Internet use expanded rapidly. In 1998, only 11 percent of Israeli households reported having access to the Internet; the figure had risen to 30 percent by 2002 and 71 percent in 2008. As Israel moves ever closer to becoming an information-based society, a central question for social scientists is the extent to which people from all the different groups in society are able to enjoy the benefits of new information technologies. Overall, 71 percent of the Jewish population report access to the Internet, but only 50 percent of the Arab population does so. The ethnic gap in Internet access is wider for low-income individuals of both groups and narrower for those with more than a high school education. 32 Research on the digital divide according to ethnic lines in Israeli society has concluded that Israeli Arabs have less access to and make less use of the Internet. 32 Studies to identify the causes of limited Internet access and use by the Arab population concluded that structural barriers associated with their disadvantaged status in society were the main source of the disparities. In sum, the multi-ethnic nature of Israeli society along with a high level of residential and social segregation of Arabs and immigrants makes Israel a perfect setting for conducting this study.
Method
Sample
Data for this study were collected in December 2009 and January 2010. The Statistical Unit of the University of Haifa created a random sample frame of a representative sample of the Israeli population. The sample was drawn from the list of communities in the country and was based on individuals with landline phone numbers in 361 geographic locations. Respondents 18–75 years of age were contacted by phone and asked to participate in the survey. Phone numbers where there was no answer were contacted up to seven times. Those who answered the phone but were busy were contacted again. Overall, 3500 individuals were contacted, and 2008 completed interviews were obtained for a response rate of 54 percent. The sample consists of 1371 individuals who reported using the Internet, 46.5 percent of whom are men and 53.5 percent women. Of the participants who indicated that they had access to a computer, 74.4 percent reported obtaining health information from the Internet.
Questionnaire
We gathered the data for the study using a questionnaire with 84 items that was translated into Russian and Arabic to include respondents who did not speak Hebrew. The questionnaire also asked for socio-demographic information, patterns of using the Web for health information, health status, attitudes about the trustworthiness of the information obtained online, and the respondents’ use of electronic health and communication services.
Study variables
The concept of e-health includes a variety of activities such as the use of digital technologies to access health services and health information, and communicate and share health experiences with other patients and health experts, as well as the use of digital devices to monitor and manage one’s health. While access to health services, online information, and communication are universal needs of healthy and non-healthy people, the use of digital devices to monitor and manage one’s health is specific to populations with medical problems. Furthermore, in Israel, access to health insurance is provided by different major insurance public companies. Insurance companies differ in the self-management technology that they provide. Given that we were focused on inequalities in the use of e-health services at the national level among ethnically disadvantaged groups, we did not investigate the use of digital devices to monitor and manage one’s health to avoid bias in the results that depend on the insurance provider. For that reason, the e-health services that we focused are the ones that are provided to all the residents of the country.
Statistical analyses were performed using Statistical Package for Social Sciences (SPSS) v20.0 software (SPSS Inc., Chicago, IL, USA). One-way analysis of variance (ANOVA) was used to determine whether there are any significant differences between the means of the three ethnic groups. As sample sizes were unequal, Tukey–Kramer’s post hoc tests were used for additional exploration of information on which means are significantly different from each other. After ethnic differences in access to health information and the use of health communication were identified, a multivariate analysis was conducted. The goal was to identify whether ethnic differences in this measures persist after controlling for background variables, medial conditions, and satisfaction with the physician. As dependent variables were defined as continuous variables, ordinary linear squares (OLS) regression was used to test the model.
Use of online health services
We assessed the use of online health services with a scale created from the sum of the participants’ answers to questions about their use of 13 services. Examples of these services include making an appointment with a doctor, with a specialist, with a nurse, checking online results of laboratory tests, and asking online for drug prescriptions.
Access to online health information
This variable was measured using a scale created from the participants’ answers to seven questions that asked them to indicate how often they searched for information on the Internet about vaccines, high blood pressure, doctors, quitting smoking, diet, healthy food, and protection from the sun. Responses were made on a 5-point Likert scale ranging from 1, indicating never, to 5, indicating very frequently. The scale’s mean was 12.25 (standard deviation (SD) = .43, α = .73).
Online health communication
We measured this variable using three questions that asked the participants how often in the last year they had participated in Internet forums on health-related topics, sent an email to a physician, or sent an email to a nurse. The variables were combined into a single scale by totaling all the responses (M = 2.25, SD = 1.04, α = .75).
Ethnic group
Respondents were asked for their country of birth. The answer “Israel” was cross tabulated with an item about the respondent’s religion to yield two variables. Israeli-born and Jewish was coded as a dummy variable, and Israeli-born and Muslim, Christian, or Druze was coded as a dummy variable. Immigrants were identified by means of two items. The first asked for the respondent’s country of origin. Those answering “FSU” were identified. Then their year of immigration was determined, and a dummy variable was created indicating FSU immigrants since 1989. In addition, in this study, participated individuals who were identified of Ethiopian origin (born in Ethiopia or from parents born in Ethiopia) represented 1.3 percent of the total sample reflecting their representation in the total population of the state. However, due to our sample size, this translates into 21 cases, too low to include in the multivariate statistics. For this reason, the cases were not included in the analysis.
Age
Age was measured as a continuous variable. In the study, we explored the possibility of a non-linear relationship between age, and two terms were incorporated: age and age squared, testing the possibility of a curvilinear relationship. Specifically with regard to the observation of the reviewer, please note that the age range in our sample was from 18 to 75 years old. Thus, the observation about the use of the Internet in the population older than 80 years is not relevant. As for the use of tablet computers, at the time of the study, the market penetration of this device in Israel was very low. When we conducted the study, 92 percent used a computer to access the Internet, 40 percent a mobile phone, and only 15 percent a tablet computer. While some people used more than one device, the use of mobile devices (mobile phones and tablets) was more common among the young.
Gender
Gender was measured by a dummy variable, with 1 indicating male and 0 indicating female.
Education
We measured the level of education as the total number of years of completed formal education.
Marital status
Married or living with a partner was coded as 1, and single or living alone was coded as 0.
Number of children
We measured this factor as a continuous variable.
Satisfaction with physician
The participants indicated the extent to which they felt that their family practitioner explained their health conditions, respected the patient’s complains, spent time explaining things, and involved the patient in his or her health. Responses were made on a 5-point Likert scale ranging from 1, indicating never, to 5, indicating always. The scores were combined in a single scale (M = 16.78, SD = 3.82, α = .80).
Health status
The participants were asked to indicate the extent to which they suffered from a chronic illness such as hypertension, diabetes, heart disease, cancer, or other medical conditions. The responses were entered as a series of dummy variables when the other category was the one omitted.
Frequency of Internet use
We measured this variable with an item that asked the participants to indicate the number of hours that they used the Internet daily for all types of online activities including leisure, communication, banking, and online commerce.
Findings
As Table 1 shows, the ethnic groups differ in their search for health information, online communication about health issues, and use of electronic services.
Descriptive statistics of entire sample according to ethnic origin (Internet users only).
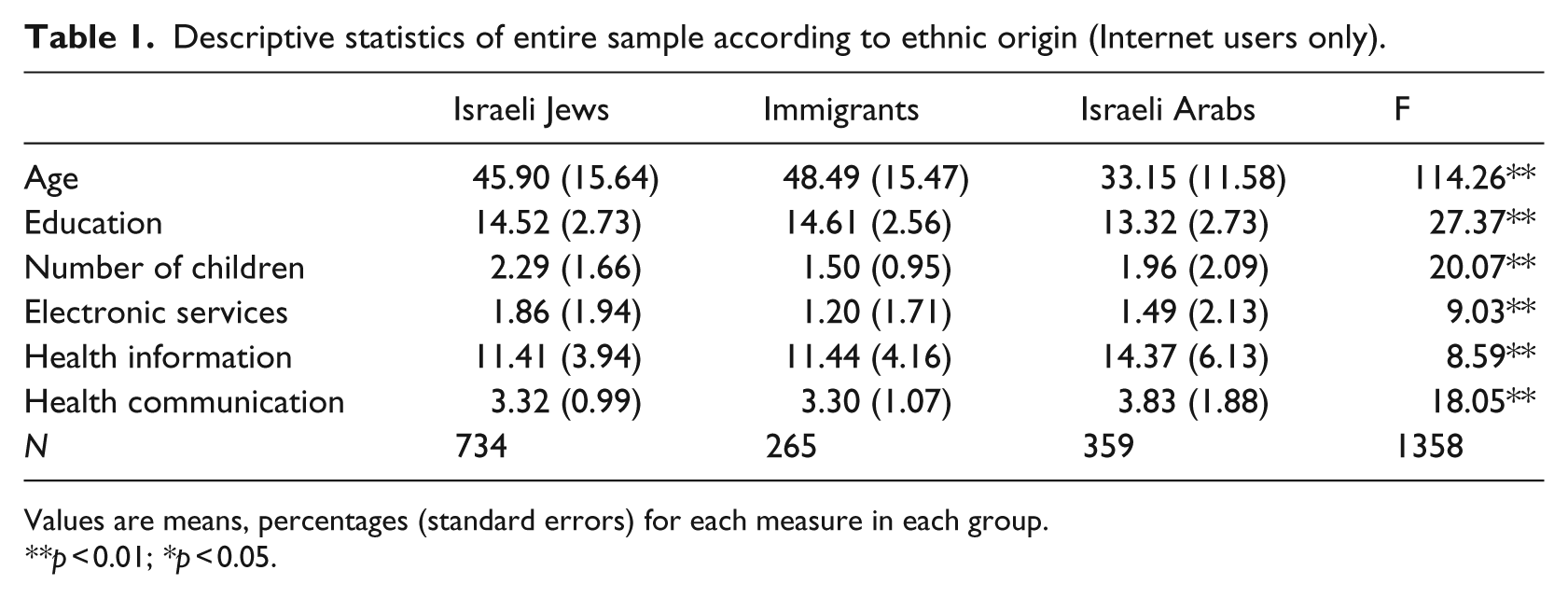
Values are means, percentages (standard errors) for each measure in each group.
p < 0.01; *p < 0.05.
Israeli Arabs are more likely than immigrants and Israeli Jews to search for health information and communicate online about health-related issues. However, and paradoxically, Israeli Jews use electronic services more extensively than Israeli Arabs. The findings indicate that consistent with the diversification hypothesis, the Arab minority is more strongly motivated to learn about health issues and communicate with healthcare professionals. Thus, the use of the Internet to obtain health information and communicate with others about healthcare issues does reduce some of the inequality in societies that offer inequitable access to health services. This finding is important, because one assumed outcome of the lack of access to healthcare services is poor health.
In the next step, we investigated the determinants of searching for health information online. The findings indicate clear socio-demographic differences (Table 2).
OLS regression analysis of the factors associated with searching for health information on the Internet.
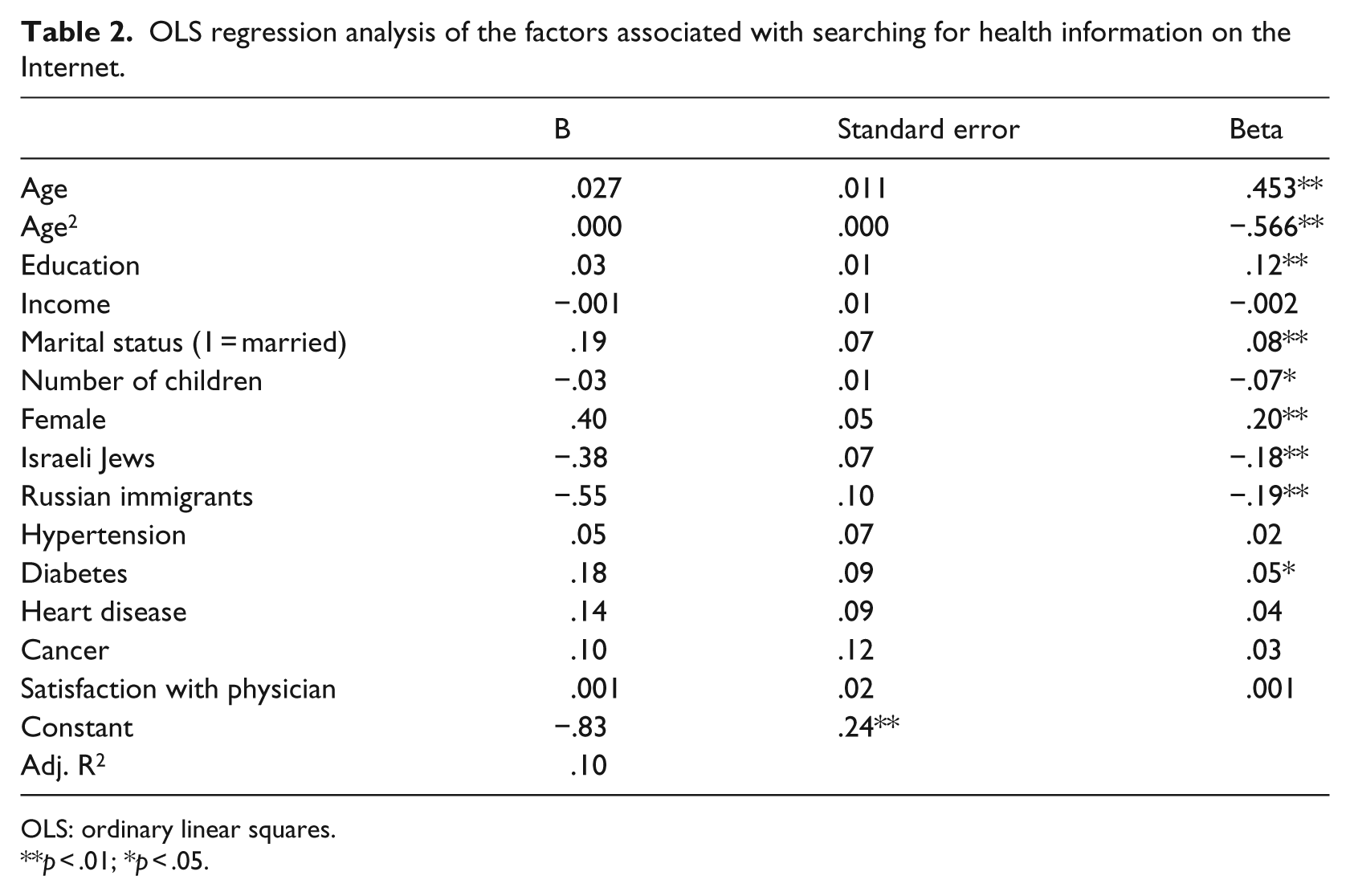
OLS: ordinary linear squares.
p < .01; *p < .05.
The relationship of age is curvilinear, indicating lower access to health information forthe young and old. Education is positively related to the search for health information, indicating that the higher the level of education, the greater the access to health information. Consistent with previous studies, women are more likely to access health information than men. With regard to ethnicity, the results provide partial support for the diversification hypothesis. Members of the Israeli Arab minority are more likely to access health information than members from the ethnic majority (Israeli Jews) and new immigrants. With regard to health status, those who suffer from diabetes are more likely to access health information.
To answer our main research question about whether the extent of access to e-health services replicates or reduces existing social disadvantages, we conducted an OLS regression. The first model is presented in Table 3 and predicts a combined scale of the use of e-health services.
OLS regression predicting use of e-health services.
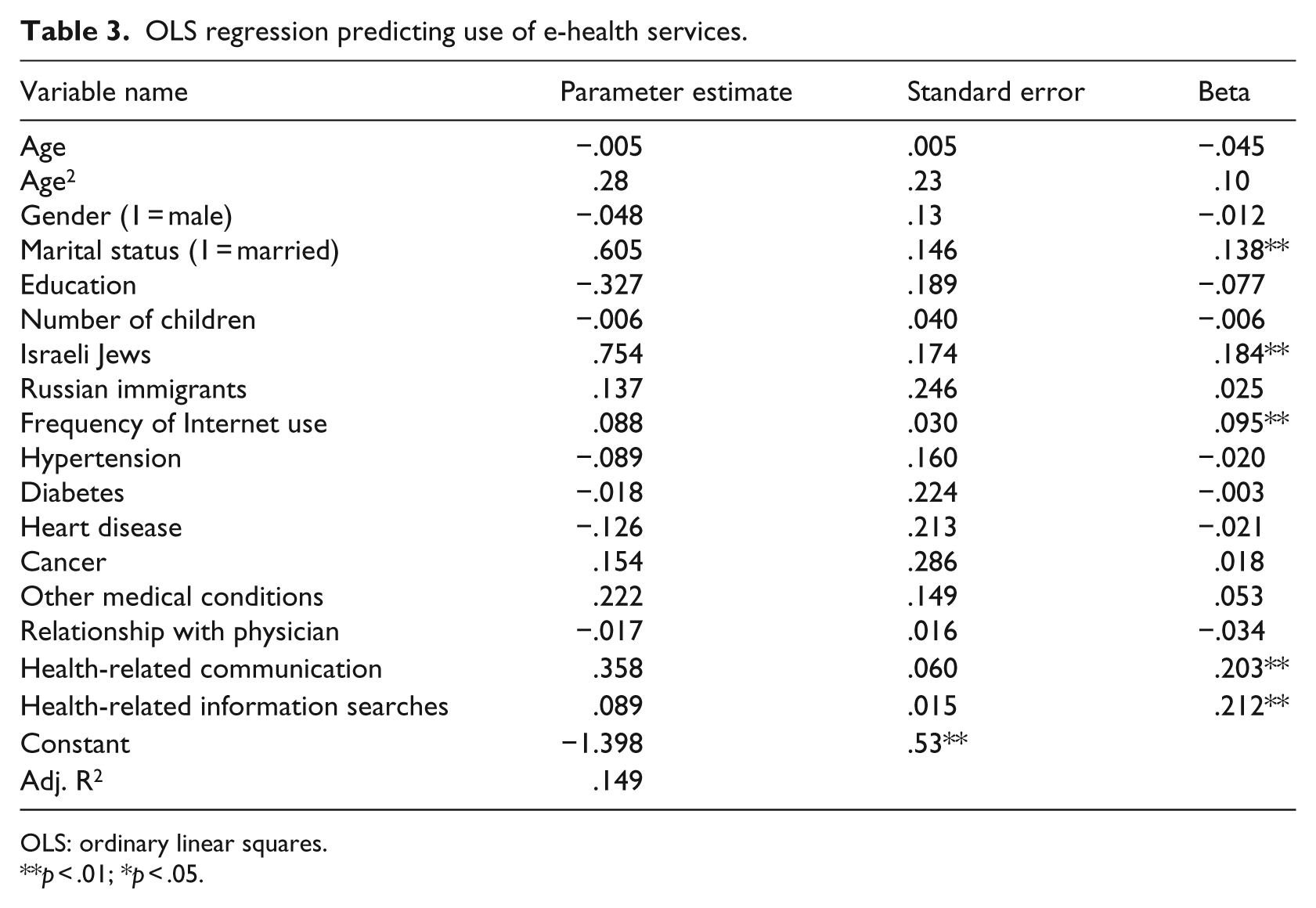
OLS: ordinary linear squares.
p < .01; *p < .05.
The findings indicate that most of the socio-demographic variables are not statistically significant. Regarding the effects of ethnicity and migrant status, the results show that inequalities in access to health services tend to be replicated online, because members of the ethnic majority group are more likely than members of the minority group to access e-health services. As expected, greater awareness of the possibility and benefits of using the Internet for health issues strongly affects the use of e-health services.
In the next step, we conducted an analysis of three kinds of e-health services—making an appointment with a doctor or a specialist and checking the results of laboratory tests. The results are presented in Table 4. While the effect of ethnicity differs from service to service, ethnicity does have a consistently negative impact. Members of the majority group, Israeli Jews, are more likely than Israeli Arabs to use the three different types of services, a finding that supports the stratification hypothesis. However, new immigrants are more likely than Israeli Arabs to use e-health services. Thus, the results are mixed, with some supporting the stratification hypothesis and some supporting the diversification theory.
OLS regression analysis of the factors associated with accessing e-health services.
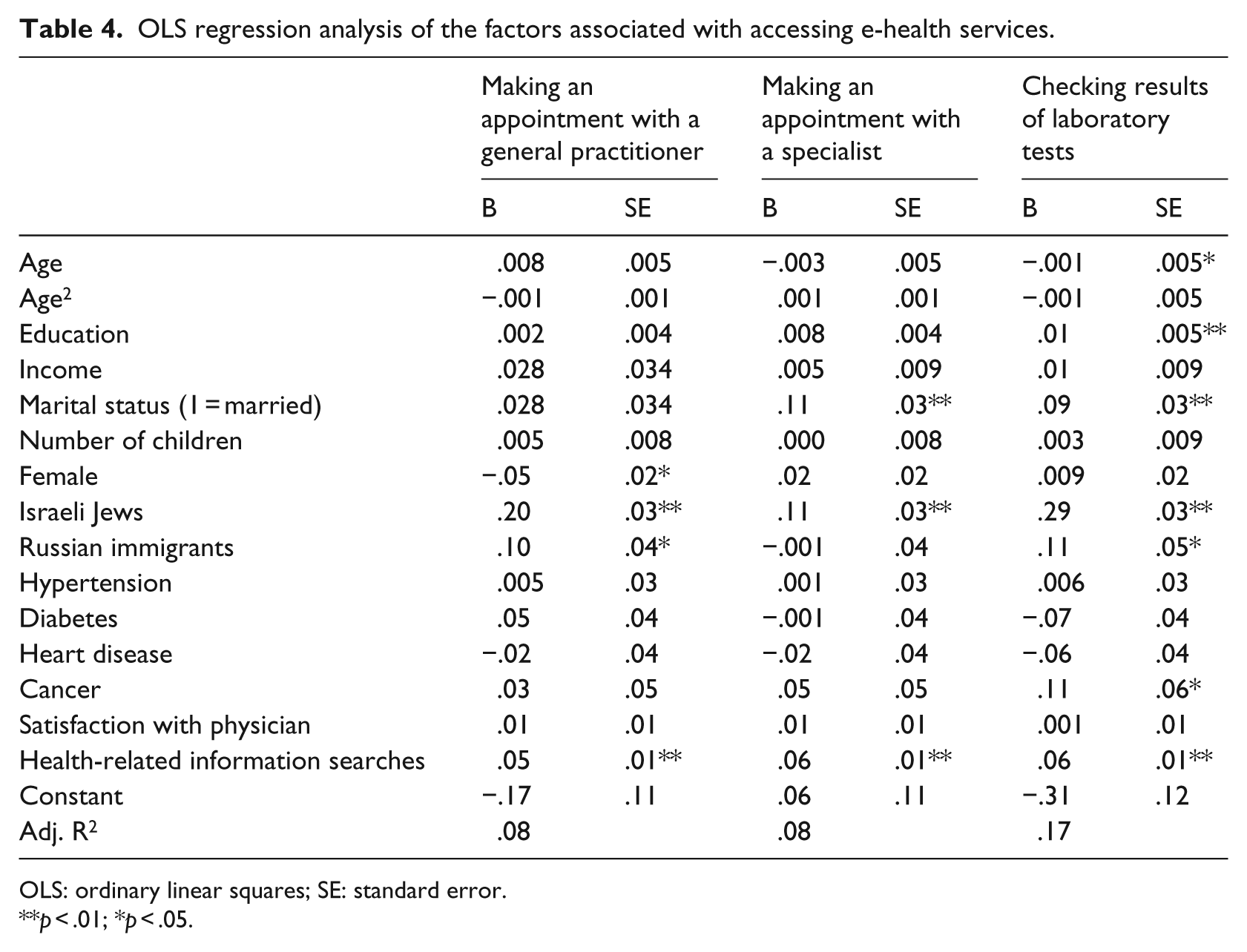
OLS: ordinary linear squares; SE: standard error.
p < .01; *p < .05.
Discussion
Empowerment is a frequently cited benefit of using the Internet to access health information and communicate with healthcare providers and with others with whom one shares a health concern. 4 The essence of empowerment is personal control, which is inextricably linked to the availability of information, acquired knowledge and the capacity to learn. Traditionally, the doctor–patient relationship is one in which there is a considerable power imbalance, where the doctor possesses medical knowledge, and the patient’s knowledge is often considered irrelevant. One of the underlying assumptions of patient empowerment is that providing access to health information and health services will rectify this imbalance. 4 However, such assumptions fail to take into account the social context that is stratified according to SES and ethnicity.
The purpose of this study was to investigate the extent to which access to e-health is associated with social conditions. The guiding theoretical perspectives were the stratification and diversification hypotheses. Consistent with the diversification hypothesis, we demonstrated that the most disadvantaged ethnic group in Israeli society used the Internet to access health information. The finding that SES had no significant effect on people’s access to e-health services is encouraging in that it holds out the promise that digital technologies can reduce some social inequalities. This finding is consistent with recent studies that indicate that among ethnic minorities that have access to the Internet, they are more likely than majority groups to access information and social networks that provide access to information. 33 However, consistent with previous studies, we did establish that there are still barriers to accessing e-health services. 23 In general, we found that social inequalities in access to health services are replicated in the access to e-health services. Given that our participants had a computer, our sample was biased toward those with higher levels of education and income. This effect held even when controlling for health-related communications and information searches. One optimistic note on this issue is the positive effect of health information searches and health-related communication on e-health services. Given that disadvantaged minorities are the most likely to seek health information online and communicate about health-related issues electronically, their ability to access e-health services might be greater through its effect on the antecedent variables of e-health services.
Consistent with previous studies, we found that education is positively associated with access to health information. 23 It is possible that education is reflecting variation in health literacy that is required not only to access but also to understand and evaluate online health information. As to access to e-health services, our study expands previous findings and shows that the effect of education might be dependent on the type of e-health activity. For example, it has no effect on making an e-appointment but has a negative effect on accessing laboratory tests and the personal patient file online. This difference calls for research in the future that looks closely at the sources of differential effects of education on access to different e-health services.
Conclusion
Recent developments in the area of e-health have prompted enquiries into the extent to which technology empowers patients and improves their health, particularly among socially vulnerable populations. Such empowerment requires the patient’s involvement in a number of processes including access to and understanding of online health information, sharing, and exchanging information with healthcare professionals and patients, accessing services online and utilizing wireless mobile devices to monitor and manage one’s health. Does the advent of e-health services help disadvantaged minorities, or does it simply replicate existing inequalities in society? The results of our study designed to answer this question were mixed and underscore the complexity of the process. We found that disadvantaged minorities are becoming engaged in and committed to their health, as they are more likely than the ethnic majority to access health information online. However, they still face barriers in using digital technologies to communicate with healthcare providers and access healthcare services. It is very likely that insurance and healthcare companies need to invest more in promoting these services to disadvantaged groups of society and encourage their use. Future studies need to monitor the extent to which these gaps close over time.
An important limitation of this study is that it did not investigate the use of wireless digital technologies to monitor and manage one’s health. Future studies should be designed to investigate this rapidly growing area in health care. Finally, the growing use of digital technologies for e-health requires more studies to evaluate the extent to which their use is achieving the goal of empowerment and actually improving chronic health outcomes among disadvantaged populations.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This study was funded with a research grant from Maccabi Health Services (2010).