
Abstract
The incorporation of an electronic medical record into patient care is a priority in developed countries, but faces significant obstacles for adoption in developing countries. The goal of our study was to define and assess the efficiency of a personalized intervention on village physicians’ use of electronic medical records in rural community health services of underprivileged areas. Six towns were selected with two bordering local health stations from each town. One was randomly given to the intervention group and the other to the control group. A structured on-site intervention was provided to village physicians in the intervention group, for 7 months. The results showed that in the intervention group, the percentage of households with complete records increased. The percentage of clinic medical records and complete child vaccination in the intervention group also increased from 2 to 14 percent (p = <0.05) and from 10 to 23 percent (p = 0.05), respectively. Our investigation demonstrated that on-site education, supervision, and technical support directly correlate with improved use of electronic medical record. Our results report the challenges in implementing such a system and the steps being taken to enhance likelihood of sustainability.
Introduction
Medicine is an information-rich enterprise. The incorporation of an electronic medical record (EMR) into patient care is a priority in developed countries, given the popular, although not well-proven, belief is that it can improve public and population health outcomes by making it easier for health organizations to collect standardized, systematic data that improve the reporting capabilities which can help health officials monitor, prevent, and manage disease. A more efficient flow of information within a digital healthcare infrastructure created by EMRs incorporates and leverages digital progress and can transform the way patient care is provided and compensated. Historically, EMRs have played an important part in strengthening the medical health system in the United States, both clinically and academically.1,2 Closely monitoring the success of health systems in developed countries with EMRs, 3 in 2010, our Regional Health Commission (RHC) of the Bonao County in the Dominican Republic started a countrywide EMR initiative in order to improve regional access, quality, cost-effectiveness, and collaboration. The goal was to establish EMR usage in 30 percent of the rural medical facilities and in 50 percent of urban medical facilities by the end of 2012. Long-term goals were to establish cohesive, effective, and high-quality EMR systems by 2018 throughout the region.
While EMRs have great potential for improving quality of patient care and practice efficiency, adoption of EMRs is a challenge for clinicians. Barriers include the purchase and support of high-priced hardware and software, while simultaneously allocating ample personal and staff time to training and managing their medical practices.4,5 Efficiency advantages of EMRs are not instantaneously evident as different workflows and procedures must be learned. Moreover, choosing a system can be difficult, as well.4,5
After a recent study, which assessed the impact of ambulatory EMR on physician productivity after the implementation of a commercially available ambulatory EMR system in a multi-specialty physician population, productive uses of EMR were well demonstrated. Fear of productivity loss remained a major concern for practitioners, which inhibited system adoption. However, provider productivity modestly increased for physicians who adopted a commercially available ambulatory EMR. The productivity gain appeared to become even more pronounced after several months of system experience. These objective data helped persuade apprehensive practitioners that EMR adoption need not harm productivity. 6 Thus, fear of productivity loss among practitioners and healthcare delivery organizations should be looked upon, and their concerns should be addressed adequately.
In acknowledging the benefits of looking beyond the mere technology aspects of EMR implementations, we investigate the rationality regarding electronic health record (EHR) implementations. Our team conducted a pilot investigation of an intervention to enhance EMR usage by rural physicians in Bonao County, Dominican Republic. The intervention encompassed administration, technical support, and education. Here, we report the effect of this intervention using data obtained from the online EMR to establish a foundation for further implementation of EMR in rural regions.
Materials and methods
This study was conducted with institutional review board approval.
Study population
Six towns in Bonao County were selected as investigation sites, based on their gender, age, and population distribution. Two bordering local health stations (LHS) were selected from each of these towns. One of them was randomly assigned to the experimental group and the other to the control group. In all, 18 families’ EMRs from each LHS were selected by simple random sampling.
Intervention
Our team conducted six monthly visits to the LHS in experimental group. The team included public health authorities, software specialists, and officials from the County Bureau of Health. The intervention comprised three facets:
Supervising the efficiency of the physician’s EMR use, which included data entry and extraction of patient health information (medication, surgical history, allergies, social history, and so on) for continuing care;
Technical support on using EMR tailored to the physician’s situation and needs;
Teaching/educating EMR policies and benefits in person, including hands-on training in the proactive and timely use of EMR.
The control group was not subjected to intervention but was simultaneously observed.
Data extraction
The survey was conducted in October 2011. In total, 18 families from each LHS were randomly assigned, and the investigators conducted an assessment of each family’s online EMR. The information on these family members (1385 residents at baseline and 1461 residents at follow-up) was gathered online using a structured data extraction form by the investigators. The final evaluation was conducted in April 2012.
The data extraction sheet determined the entirety of the records in the EMR of the following: personal health information, health examinations, health education, child health and immunization, management of the elderly, and basic clinic care. Assessment of these indicators was based on integrity of the file records at the time of last entry. If the record was ⩾75 percent complete, we categorized it as “complete”; ⩽74 percent were categorized as “partially complete,” and no information in the record was categorized as “absent.” The pre- and post-use of EMR was then evaluated in order to assess whether on-site education, supervision, and technical support tailored to the individual needs had an impact with improved use of EMR.
Statistics analysis
All analyses were performed using R—free software for statistical computing and graphics. Chi-square tests were used to estimate the difference of gender and age of respondents before and after the intervention. Two-sample t-test was used to estimate the difference in age of physicians between experimental and control groups. Mann–Whitney U test was used to evaluate the difference in the completeness of the public and basic health records. A significance level of α = 0.05 was used for all comparisons.
Results
Demographic analysis
Each LHS has at least one physician. There were seven male and three female physicians in both the experimental and control groups. The mean age of the physicians was 41.0 and 35.2 years, respectively, with no significant difference in age (p = 0.852) between control and experimental groups.
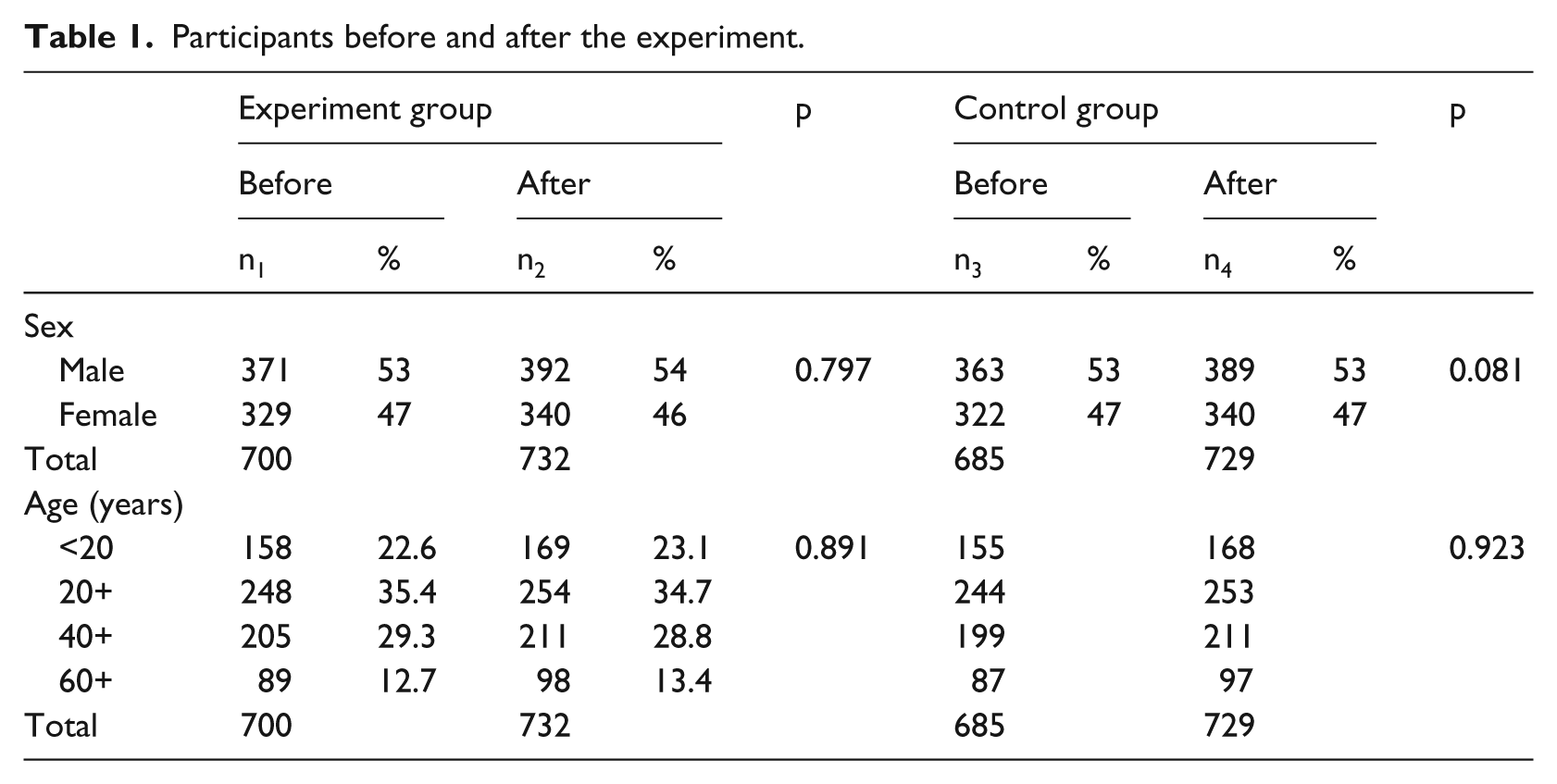
The demographic profile of residents is presented in Table 1. Prior to the experiment, 700 and 685 residents were selected, with an average age of 36.9 and 36.8 years in experimental and control groups. After the experiment, 732 and 729 residents were selected; the mean age was 37.7 and 38.1 (standard deviation (SD) ± 25) years, respectively. We did not observe any significant difference in gender between the experimental and control group (Table 1).
Participants before and after the experiment.
EMR in general population
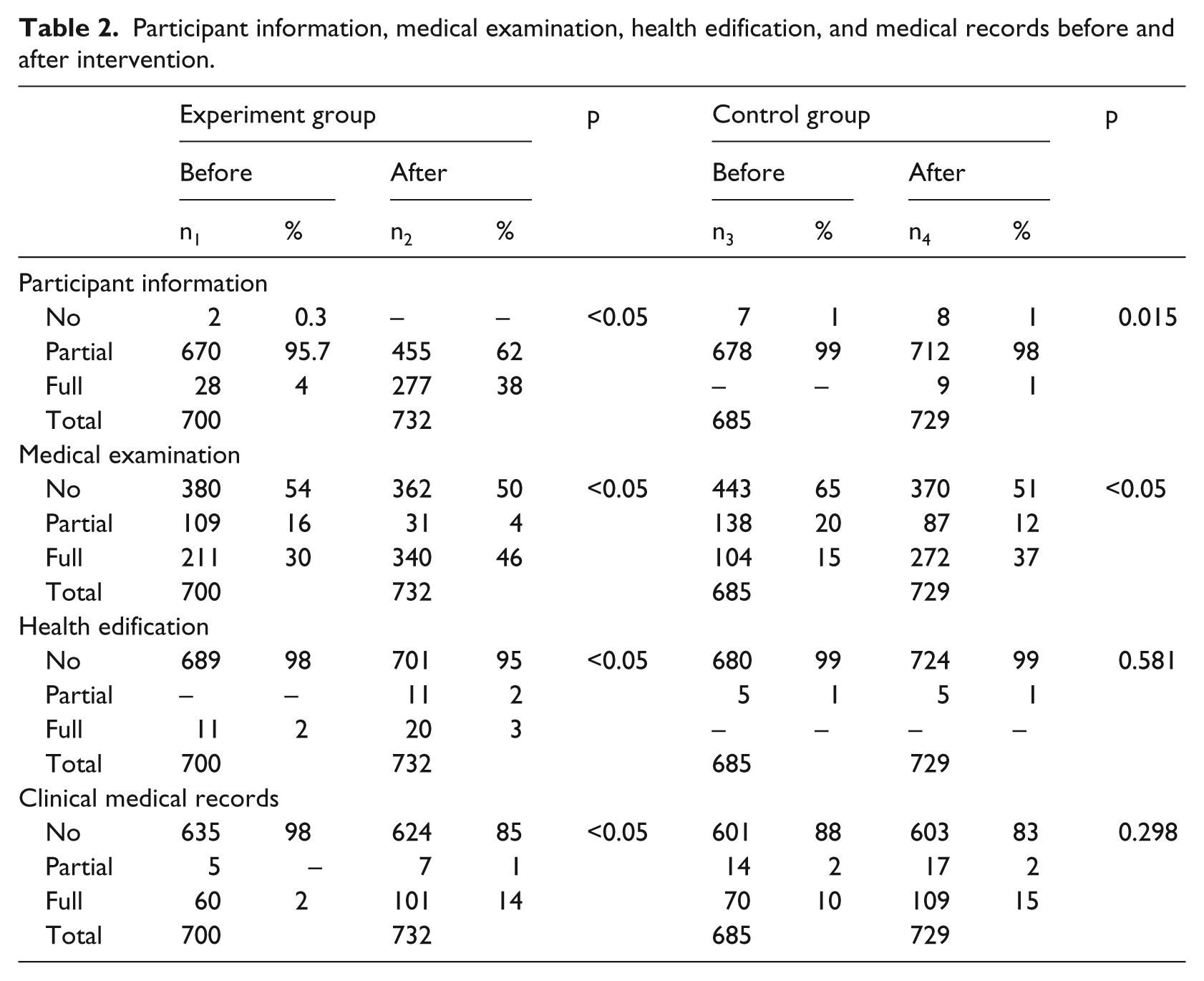
In the experimental group, the percentage of individual residents’ records with complete basic personal information increased from 4 to 38 percent (p < 0.05) after the intervention. In the control group, we observed a small percentage of change compared to the experimental group (0%–1%, p = 0.015). In the experimental group, the percentage of complete health examination records increased from 30 to 46 percent (p < 0.05). In the control group, it also increased from 15 to 37 percent (p < 0.05). In the experimental group, the percentage of complete health education records increased from 2 to 3 percent (p < 0.05). In the control group, there were no complete health education records before or after the intervention. In the experimental group, the percentage of complete residents’ medical records increased from 2 to 14.1 percent (p < 0.05). In the control group, there was no significant change (10%–15%, p = 0.298) (Table 2).
Participant information, medical examination, health edification, and medical records before and after intervention.
Children health and vaccination records
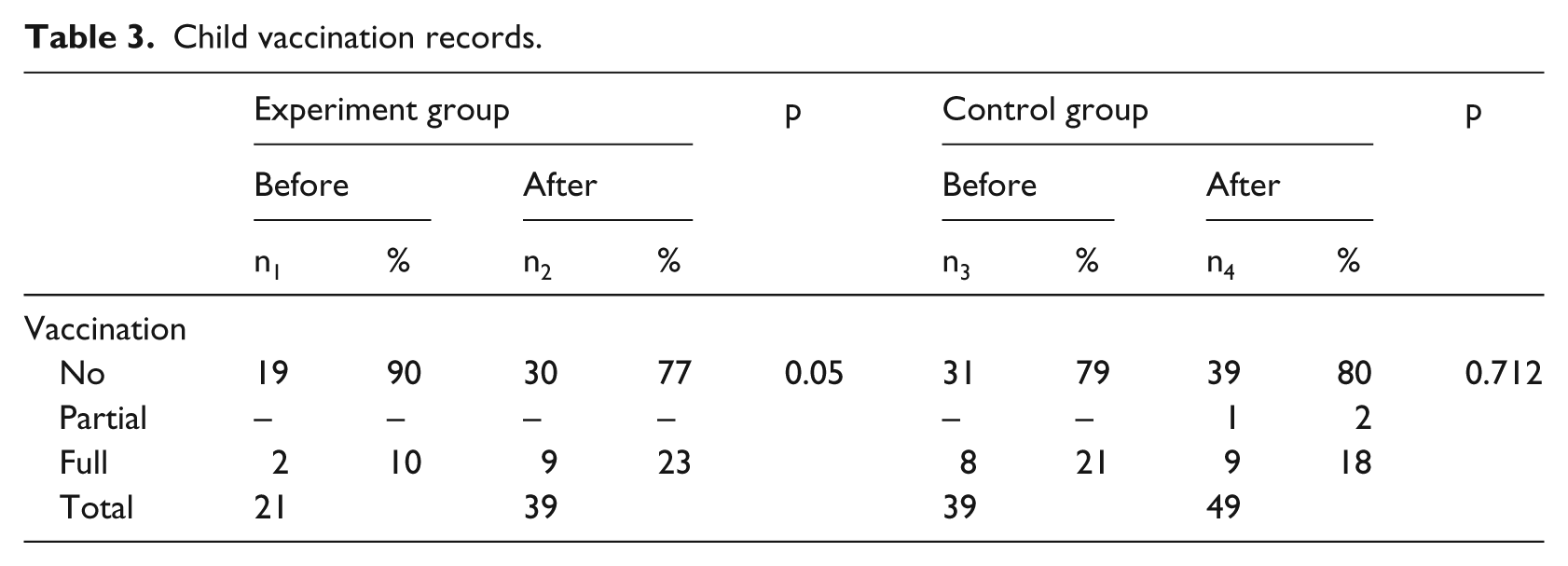
In the experimental group, after the intervention, the percentage of complete child vaccination records increased from 10 to 23 percent (p = 0.05). In the control group, we did not observe any change (21%–18%, p = 0.712) (Table 3).
Child vaccination records.
Health management of the elderly
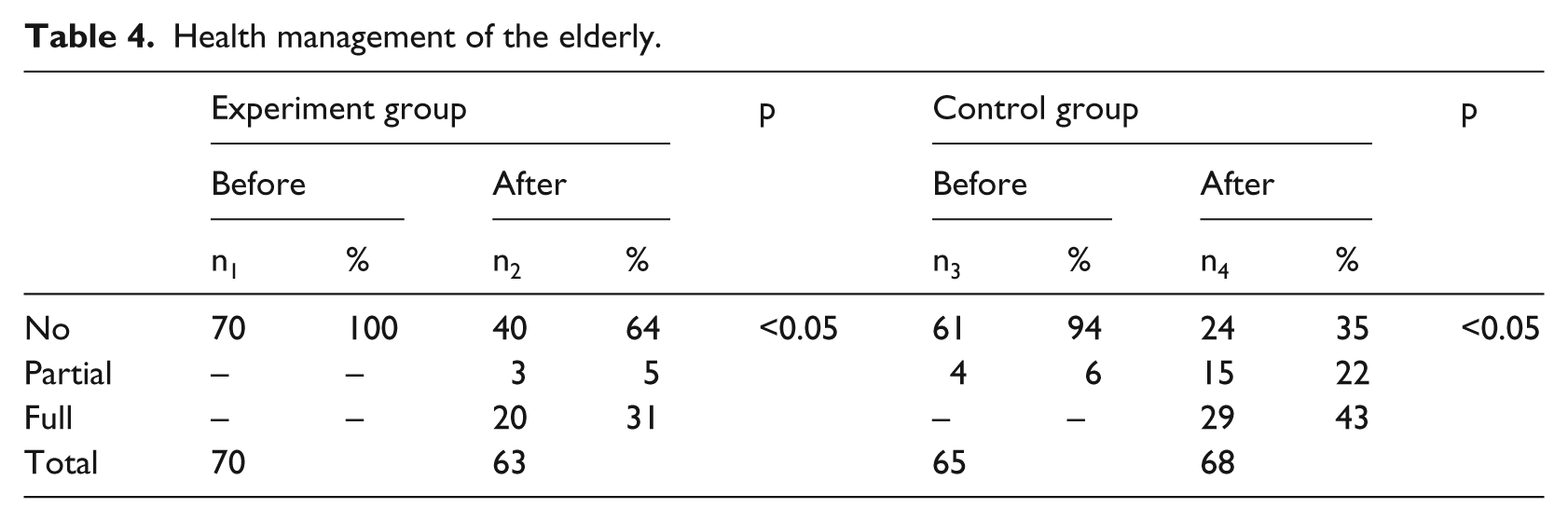
There were significant increases in the completeness of records of health management of the elderly patient population in both the experimental (0%–31%, p = <0.05) and control (0%–41%, p = <0.05) groups before and after the intervention (Table 4).
Health management of the elderly.
Discussion
The EMR has been proposed as a means to significantly improve the quality of health care for community residents. Implementation of EMR would aid primary care providers in better tracking the changes of health status of the local community. 7 The improved comprehension of the trends in illnesses can lead to timely and proper preventive measures and interventions, which would contribute to an overall improvement in the health status of the community. Complete and accurate EMRs have shown to improve efficiency and quality of clinical practice. 8 For example, Wilson 9 reports a 40 percent time reduction for clinicians using EMR as opposed to running a medical practice using traditional paper records to extract patient information.
Current literature about the United States, United Kingdom, and Spain shows that the barriers in the developing and the developed countries are very similar, and they are facing the same challenges although the developed countries have more potential to overcome these challenges due to socioeconomic factors. 10 Nations such as the United Kingdom, Australia, and the Netherlands have shown to have coverage rates of EMR at over 90 percent, but the sharing of records between services was reported suboptimal.1,11 In less developed nations, research on EMR has been limited and focused almost entirely on knowledge and satisfaction of healthcare providers with EMR.
In 1996, Partners In Health (PIH) started an open-source web system in Peru that was backed by an Oracle database. The medication order entry system showed 17.4 percent fewer errors than the previous paper approach. 12 In 1999, PIH began an EMR system in parts of rural Haiti. These rural areas have virtually no roads, electricity, or telephone service. This system displays how EMR systems can overcome great challenges in remote areas with virtually no infrastructure and limited technical expertise. 12 Similarly, in Kenya in 2001, the Mosoriot Medical Record System (MMRS) was developed, as a result of which patient visits were 22 percent shorter, provider time per patient was reduced by 58 percent, and patients spent 38 percent less time waiting in the clinic. 12 This shows the strength and flexibility of a web-based approach in poor developing countries like Dominican Republic.
There are numerous reasons why the medical personnel in the Dominican Republic are hesitant in exploring and utilizing EMR. The three essential issues that need to be addressed among rural physicians include the following:
Primary care physicians are not aware of how EMR can facilitate them in improving the quality and efficacy of their day-to-day operation.
Older physicians are often not computer savvy and report that they struggle to operate the EMR system proficiently.
Physicians feel that recording all data into the EMR opens them up to bureaucratic oversight.
Thus, these problems raised a few questions regarding the technical aspects of the difficulty in operating the system among physicians. This holds true especially in underprivileged areas where even the basic infrastructural needs were lacking. There has not been much attention devoted to descriptive studies evaluating the before and after effect of intervention with a control group. This study attempts to bridge that gap while complementing previous research.13–16
Public health records
Our study distinguishes the training of rural physicians in the use of EMR as it was associated with improvements in recording personal health information, health examination, health education, management of the elderly, and child health management.
In the intervention program, physicians were educated by project members on the basic public health services policy and funding program to highlight the importance of public health work in rural areas. In addition, the project team also provided technical guidance in installing and using EMR to record public health services as well as motivating and eliminating any obstacle preventing the physicians from carrying out the EMR work. After the intervention, the proportion of complete basic information and vaccination records increased significantly in the intervention group.
Health management of the elderly
There were significant increases in the completeness of records of health management of the elderly patient population in both the experimental and control groups, before and after the intervention. This could have been the result of early pretesting by local authorities in order to assess feasibility of starting the initiative. During this period, residents (mostly elderly) were given regular physical examinations and arrangements were made to enter the results into the EMR.
Clinic medical records
There was some improvement of note in clinic medical records in the intervention group but not in the control group. Further questioning demonstrated that the shortcomings in implementations were often due to organizational issues around the implementation process as well as some technological concerns.
Primary care physicians were initially faced with a conflict of interest with the introduction of the EMR. On one hand, they wanted to utilize the EMR as an effective tool to conduct the day-to-day operation of running their clinic and improve their own efficiency and quality of work. On the other hand, updating and standardizing basic clinical information left their medical business practices open to scrutiny at every administrative level. Finding themselves in such a conflicting situation, 59 percent opted not to use EMR. Our team was able to overcome some of these issues by demonstrating the overall benefits to be accrued from using EMR.
Study limitations
This particular study was conducted with the limited sample size of a few households within six towns of rural Bonao County. One of the strengths of the investigation is that control and intervention groups were similar in respect to socioeconomic conditions, age, gender of participating residents, and healthcare providers, which did not change significantly over the course of the investigation. Thus, confounding effects of these factors were minimized between the two groups. Not all participants were willing to share information on whether or not they owned a computer, which creates a challenge in assessing previous knowledge of computers. Only a narrow range of aspects of public health recording and medical service provision could be assessed. It would be beneficial to conduct comparable studies to gain further understanding.
A comparative study of 19 EHR systems in terms of security and usability of these systems within the context of the developing world based on a number of dimensions such as development environment, system platform, type and access control standards found in the National Institute for Standard and Technology (NIST), and Certification Commission for Health Information Technology (CCHIT) indicated that all the systems evaluated required online access control decisions. Solely relying on an online access control system is limiting, particularly in developing countries where access to the server can be disrupted by a number of disastrous events. 17
An ideal approach will include needs assessment as well as education and training opportunities for the workforce. Successful local examples can be expanded into larger networks whose scale can be leveraged to more rapidly and effectively disseminate the efforts. Such an approach should also foster the establishment of academic partnerships and centers of excellence in education and research in developing countries for sustainable capacity building while still being responsive to local needs. 18 However, the development of appropriate and scalable EMR systems in developing countries has been difficult to achieve because of certain limitations inherent in the technological infrastructure.
Conclusion
The designed intervention with village physicians led to improved public health and basic clinic records. This indicates that a reasonable intervention can increase village physicians’ use of EMR provided that it is tailored to their practice. Other medical entities should consider implementing EMR in their day-to-day operations to create an efficient flow of information within their respective healthcare infrastructure. It also suggests that on-site education, supervision, and technical support tailored to the individual needs of the physicians directly correlates with improved use of EMR.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.