
Abstract
Background
In Oromia, Ethiopia, the process of digitalization is being hindered by the underutilization and inadequate understanding of electronic medical records (EMRs) systems among healthcare professionals. This is impeding the expected advancement of digitalization.
Objective
To look at how EMR affects to digitalize healthcare initiatives, find obstacles, and ways to overcome them, make workflow more efficient, and increase patient happiness through digitalization.
Method
The study employed a qualitative case study methodology, which involved observations and interviews with medical staff. Data was analyzed using Maximum Qualitative Data Analysis (MAXQDA 2020) for content analysis.
Results
This study highlights four key thematic areas: knowledge assessment or EMR proficiency (such as awareness creation, skills, and training were low), under-utilized EMR technologies, possible advantages, and obstacles to implementation. Even though there are several opportunities for the systems to progress toward full-scale implementation, the lack of thorough knowledge assessment led to implementation issues. Despite their limited proficiency, many users recognize its benefits and remain interested in using it. Nevertheless, they are skeptical about its long-term sustainability.
Conclusions
All participants fully supported the benefits of digitalization of healthcare through the use EMR and perceived positively. They expressed concerns about its continuity. Further studies on system, information, and service qualities are needed to improve overall health system digitalization process in Oromia, Ethiopia.
Implications
It requires institutional dedication, security concerns, and direct policy interventions to reduce the obstacles that hinder the development of developing countries.
Introduction
Healthcare organizations in developing countries face significant challenges and inefficiencies, partly due to their continued reliance on paper-based systems for both clinical and administrative functions.1,2 To address it, many healthcare organizations have adopt electronic medical records (EMRs) to enhance the quality, continuity, and efficiency of healthcare delivery.3,4 EMRs are typically defined as “web-based, computerized medical information systems that collected, stored, and displayed patient information in a paperless format,” accessible only to authorized personnel.5–7 As one of the most widely adopted digital technologies in healthcare, EMRs are prevalent not only in developed nations but are also increasingly used in resource-limited settings to support clinical consultations, decision-making, and patient management. 8 However, the implementation of EMRs varies between high-income and resource-constrained environments. 9 For instance, wealthier nations often integrate advanced technologies, while resource-limited settings tend to adopt more basic systems focused on patient record-keeping and disease surveillance. This disparity underscores the need for context-specific EMRs solutions that align with local capacities and priorities to drive meaningful improvements in healthcare delivery.10,11 Digital transformation has provided low-resource countries in Sub-Saharan Africa with the means to utilize emerging digital health technologies to modernize their healthcare services. 12
Despite these advancements, the full-scale implementation of EMRs as a foundational platform for healthcare digitalization has encountered significant challenges. 13 However, improvements in network infrastructure and broader internet access across the continents have supported progress toward digital healthcare systems. 14
Nevertheless the successful integration of EMRs into clinical practice remains uneven, hindered by barriers such as limited technical capacity, inconsistent policy enforcement, high costs, and resistance from end-users.15,16 Overcoming these challenges requires strong coordination among governments, healthcare providers, and development partners, in collaboration with the World Health Organization's global digital health strategy. 17
To better understand the dynamics of this transition, both the driving forces and the obstacles, this study adopts a theoretical framework to assess how EMRs contribute to healthcare digitalization in resource-constrained settings. Specifically, it draws on established models such as the Unified Theory of Acceptance and Use of Technology (UTAUT)18–21 and the DeLone and McLean Information System (IS) Success Model. 22 These frameworks help evaluate and guide digitalization initiatives, including the effective implementation of open medical record systems (OpenMRS). 23 However, achieving success requires moving beyond project-based approaches by embedding continuous evaluation and adaptive mechanisms.24,25 These strategies are informed by both global and local evidence, aligning with the key policy documents of WHO's, the African Union's agenda for e-services in health, 26 Ethiopia's National Digital Strategy, 27 and the Ministry of Health's digital health blueprint. 28
In many instances, the required infrastructure to support EMR systems is not economically viable, resulting in limited accessibility and insufficient system coverage. 29 Consequently, the incomplete implementation of EMRs has adversely affected service quality and slowed progress toward comprehensive healthcare digitalization. 30
In Ethiopia's Oromia regional state, institutions such as Adama Hospital Medical College (AHMC) and Ambo University Referral Hospital (AURH) have taken steps toward digitalization by implementing the Open Medical Record System (OpenMRS). These efforts aim to overcome challenges such as the inefficient paper records and inflated treatment costs, which have undermined patient trust and satisfaction.
Building on this context, this study specifically assesses the extent to which EMRs are being implemented at AHMC and AURH. It explores both the opportunities and challenges associated with EMR adoption, with particular attention to knowledge gaps and utilization levels among healthcare professionals. The study also investigates challenges faced by various healthcare workers during the implementation process.
A qualitative research design was used, involving in-depth interviews and on-site observations at selected health facilities. This approach enabled a deeper understanding of EMR acceptance and its role in advancing healthcare digitalization. Data were coded and analyzed to identify recurring themes related to EMR adoption. Participants included physicians, nurses, Information Technology staff, administrators; system integrators selected through purposive sampling reflect diverse roles and contexts. Semi-structured interviews and field notes documented experiences, workflow, and contextual factors affecting EMR use. Using Maximum Qualitative Data Analysis (MAXQDA) (version 2020), researchers conducted a qualitative content analysis. Key barriers identified included limited computer literacy, poor user orientation, and lack of training, all of which hinder EMR adoption in low-resource settings like Ethiopia, specifically in selected hospitals in Ethiopia. These challenges have contributed to the low implementation rate as investigators have identified persistent obstacles that hinder the full adoption of EMR in developing countries, particularly those related to economic and infrastructural constraints.
Despite these issues, the study highlights significant opportunities EMRs offer: shorter patient wait times, more efficient resource use, increased institutional revenue, reduced information loss, and potential for remote consultations, all supporting a more sustainable healthcare system. These findings enhance the current understanding of EMR implementation and advocate for broader adoption across healthcare facilities. Promoting healthcare digitalization in Oromia not only benefits the region but also offers valuable insights for similar low-resource settings across Sub-Saharan Africa. This study aims to assess the influence of EMRs on the digitalization of healthcare services in selected health facilities of the Oromia region in advancing of the digitalization efforts.
Methods and materials
Study design
This study employed a qualitative multiple-case study design grounded in an interpretive research paradigm, 31 which perceives reality as socially constructed and shaped by multiple perspectives. Guided by inductive reasoning, the study investigates the complex impacts of EMRs on healthcare digitalization efforts within hospital settings. The exploratory nature of the research justified the purposeful selection of cases, 32 enabling a thorough, context-specific examination of the organizational and technological dynamics in actual healthcare environments. 33 This approach facilitated the discovery of emerging insights valuable to both practitioners and researchers in the field.
Study site
The study was conducted in Ethiopia's Oromia Regional State, one of the largest and most populous regions in the country, compared to other regions like Amhara, Tigray, Southern Nations, Nationalities and Peoples (SNNP), Afar.
Case selection
A purposive case selection strategy was employed to gather data from institutions actively engaged in digital transformation, enhancing the relevance of the findings. 34 Based on this, AHMC and AURH were selected from 110 regional hospitals due to their partially implemented EMR systems and early adoption stages. Out of these hospitals, one has demonstrated strong performance in implementing the Smart Care system piloted by Tulane University, with 10 years of experience.35,36 They later began deploying EMRs using Bahmni open-source software, 37 developed by Digital Health Activities under John Snow Inc. (JSI) and funded by the United States Agency for International Development (USAID. 38 Despite lacking inpatient wards and paper records at the time, their inclusion aligned with the study's objectives.
Study duration
This study was conducted at AHMC and AURH from February, 2023, to November 30, 2024. AHMC implemented the system earlier, beginning in major outpatient departments, while AURH lagged behind and only began implementations at the end of 2024.
Participants selection and sampling strategy
Twenty-nine participants were selected through purposive sampling, targeting individuals directly involved with or knowledge about EMR systems and their role in digitalization. Participants included administrators, clinicians (doctors and nurses), IT personnel, health information officers, and machine-to-machine integrator. They were chosen based on their relevance to EMR implementation, with some having received training ranging from 20 minutes to 2 days at the selected health facilities.
Inclusion and exclusion criteria
Inclusion
The researcher convened experts in EMRs and digitalization efforts from multiple levels, including the Ministry of Health, Oromia Regional Health Bureau, Digital Health Activities, and various health professionals. These professionals are actively engaged in EMR systems and contributed to data collection to facilitate system expansion.
Exclusion
The researcher excluded several departments from interviews due to a lack of understanding and lack of knowledge about EMRs during data collection, including the Inpatient department, finance, logistics, human resources, and Pharmacy and Imaging from AURH.
Sample size and justification
The study's sample size was determined using information power, allowing for a total of 20 to 30 participants. 39 This number was chosen based on the study's focus, which included interviews with participants who had relevant expertise.
Data collection
The study utilized semi-structured interviews to collect data on EMR systems and digital health transformation. This was guided by existing literature to ensure content validity. The literature was reviewed by more than three qualitative research experts, as suggested by previous studies.40–42 Their feedback helped refine the language, improve clarity, relevance, and alignment with questions covering topics such as knowledge proficiency, perceptions of its benefits, challenges, workflow impacts, and support for digital change.
In-depth interview
The principal investigator dedicated over 10 months to evaluating site observations, which were subsequently corroborated with data from 29 study participants across two hospitals. Participants were intentionally selected, scheduled, and provided verbal consent. The Interviews took approximately 1700 minutes in total. Data collection ceased when no new themes emerged. This suggests that data saturation was achieved within the participant groups. The majority of interviews were conducted with audio-recording, for which consent was obtained, and these recordings were transcribed verbatim for analysis. However, a small number of participants declined to have their interviews recorded.
Data quality control methods
The quality of data is maintained through steps taken by individuals. These steps include transcribing recorded audio interviews into textual data by listening to them multiple times, thoroughly writing and reading the text, and then having linguists edit it to ensure data quality. 43 This process increases trustworthiness by assigning a code to each theme found in the textual data by four personnel. The manually coded themes are then imported into MAXQDA 2020 and recorded into several sub-themes for analysis of the frequency of each thematic data for further analysis.
Qualitative data analysis
To investigate and comprehend individual and group definitions that are attributed to societal circumstances, a theory was employed to inductively synthesize the data.33,44 The researchers then employed data visualization, formed conclusions, and validated their findings to analyze the data qualitatively, 45 to investigate how respondents’ viewpoints were impacted by the EMR.
The analysis of the interviews occurred in two stages: initially, transcribed documents were identified by four individuals for each theme of codes to ensure credibility. These interview documents were then imported into qualitative analysis software, specifically MAXQDA version 2020, 46 for recording, as they were initially coded manually by the personnel to maintain reliability and consistency with the manually coded themes to establish a pattern. Subsequently, the researcher referenced and applied qualitative methods to connect content analysis to the coded themes of respondents’ perspectives based on Merriam work that was cited.45,47 Finally, the researcher calculated and determined the Sociology-demographic status of each participant from (Table 1). They discovered that the majority of participants were doctors, with an average age of 34.35 and 9.4 years of experience. Every respondent, except one participant, had a degree or higher in their educational background. Additional knowledge might be offered by the “Results and discussion” sections of this article.
Detailed information of each study participant (N = 29).

The study results
The study identified four themes through in-depth interviews: knowledge, EMR utilization, benefits and challenges of EMR in digitalization projects or efforts. Sub-themes included awareness, computer skills, training, and benefits for medical facilities, staff, patients, system bottlenecks, and human difficulties.
Evaluation of EMR proficiency in digitalization initiatives
This study evaluates the impact of EMRs on healthcare digitalization of healthcare, focusing on computer use, awareness, and training. Participants’ opinions reflect their perspectives: “The implementation of new technologies may face challenges due to a lack of familiarity with them,” Respondent 2, 2023. “In my opinion, it can be done with continuous training. It would be good if at least on-the-job training was given to accelerate this work. This issue of healthcare digitalization requires a lot of training,” Respondent 3, 2023.
“Some healthcare professionals are not typing quickly on the computer, which is seen as an obstacle due to lack of basic computer skills,” Respondent 4, 2023.
“Many health professionals have low computer skills, making clinicians consider the digitalization of health records impractical. It is difficult to implement them without enough training in my opinion,” Respondent7, 2023.
“The pressure on the staff is even higher, as there is a lack of readiness to accept this change due to a lack of basic computer training and strengthening of basic skills in information communication technology (ICT),” Respondent 9, 2023.
“Among the various obstacles we have been facing so far is the lack of ICT professionals, with only a few people receiving training, and so on,” Respondent 16, 2023.
“Short training is not entirely enough. It is more of an orientation. They were given, but the training is not qualified to continue this work. However, people do not have the same understanding of computers, and it is difficult to implement them without enough training in my opinion,” Respondent 7, 2023.
Finally, the summary of the participants’ responses on knowledge assessment, shown in Figure 1, explained the factors hindering EMR implementation.
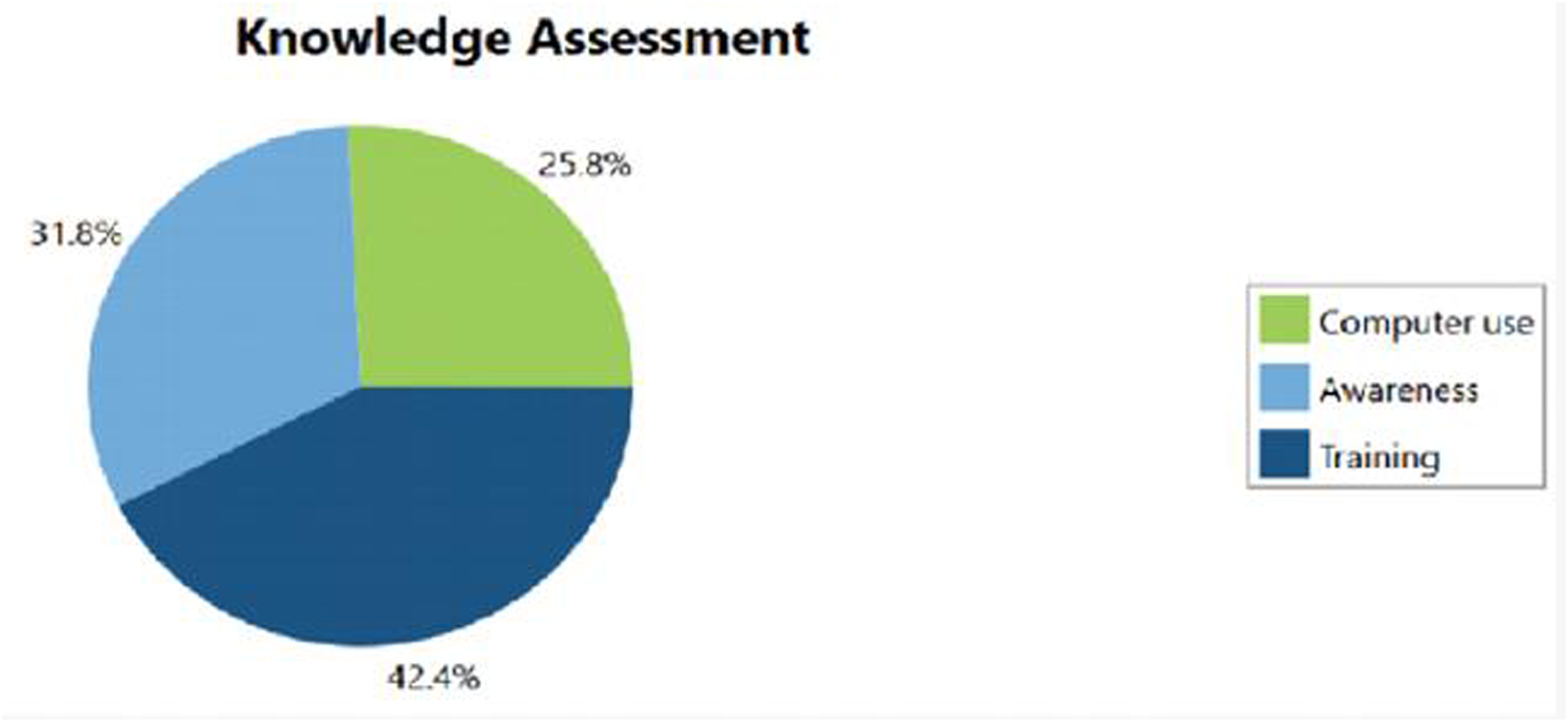
Knowledge assessment of EMR implementation on the way to digitalization process.
This study identified considerable knowledge gaps among participants regarding certain concepts. It is imperative for relevant organizations to intervene and address these deficiencies. One effective approach is to raise awareness among all healthcare personnel, including non-health professionals such as security guards and cleaners who are integral to the system. It is important to update computer usage during in-service training and offer advanced training on EMR for healthcare professionals.
Utilization levels
The implemented of EMRs in digitalization efforts is currently limited due to lack of knowledge, computer skills such as typing speed, funding, and training. This indicates that most department usage levels were very low during the EMR digitalization initiative while researchers were collecting data for this study. This is supported by the respondents’ feedback:
“A laboratory can be seen as an obstacle because the results are not immediately available for reversal. It requires the commitment of professionals, staff, and management at outpatient, laboratory, pharmacy, and imaging,” Respondent 2, 2023.
“This is good as we do paperless in the “Central Triage,” and it would be nice if other departments like pharmacy, laboratory, and all departments or majors did it especially if this work was expanded and the paper issue was left out completely,” Respondent 3, 2023.
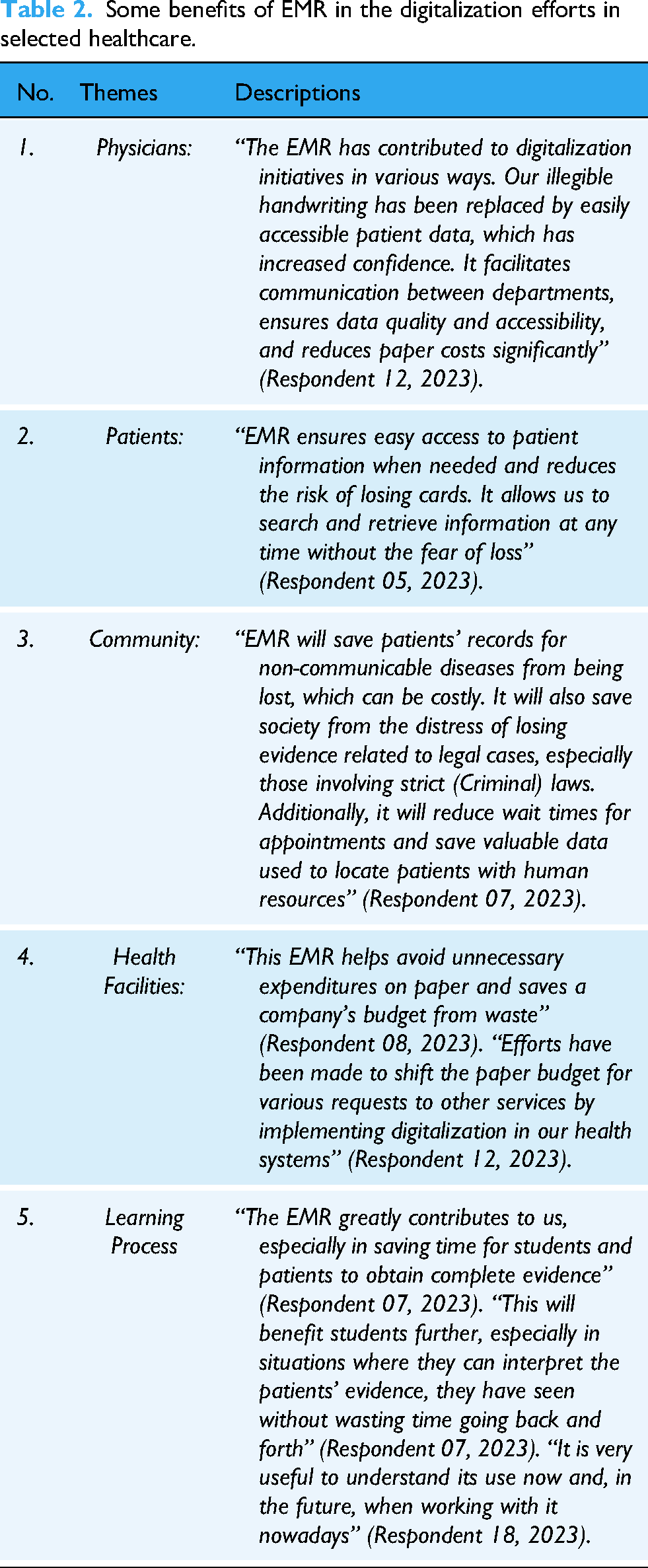
Benefits of EMR in digitalization efforts
The benefits of EMR in healthcare digitalization efforts were analyzed across five sub-themes: Physicians, Patients, Community, Health Facility, and Teaching-Learning. This analysis is comprehensively detailed in Table 2.
Some benefits of EMR in the digitalization efforts in selected healthcare.
EMR's difficulties in digitalization efforts
This theme addresses two primary sub-themes related to obstacles in EMR obstacles in digitalization projects for EMRs: system bottleneck and human issues.
Human-factor challenges
For example, respondents highlighted lack of training as a primary factor in their more accurate perception of the difficulties. One respondent stated, “From our perspective, our inability to write quickly is making us feel unwell. This is not sustainable given the number of our patients, so we need to practice using the computer” (respondent 2, 2023).
Another respondent mentioned, “The reluctance of some healthcare workers to engage in activities due to the high patient flow and work overload” (Respondent 8, 2023).
System challenges
However, these challenges were mitigated by the involvement of all stakeholders in the implementation process of the system initiatives. The majority of Ethiopian hospitals have no up-front costs associated with their EMR digitalization goals. This was supported by participants’ viewpoints: “It is not advisable for computer supplies to be disrupted,” (Respondent 1, 2023). “While these improvements enhance existing services in the future, there are still some challenges that remain. The digitalization of medical records has the potential to greatly enhance various aspects, including services, if practitioners prioritize its implementation” (Respondent 2, 2023).
Additionally, another participant from the AURH said that system obstacles are
“Some of the obstacles or challenges we have encountered include interruptions in internet connection, power outages, and delays in generator start-up. These issues not only lead to wasted resources, such as reagents like Gene Xpert in our test results but also result in errors in laboratory test results and inconveniences for our clients” (AURH respondent1, 2024).
“Moreover, this system's barriers to digitalization include system interruptions due to internet connection issues, a lack of information technology experts in hospitals (we had to call them from the main campus), long patient waiting times, and slow generator response during power outages” (AURH6, 2024).
Discussion
This study found that AHMC and AURH had initiated efforts to implement EMR systems, but only a few activities focused on computer literacy, and even fewer on creating awareness. Despite the lack of understanding and positive attitudes toward EMR, only a small number of healthcare workers were enrolled in training. Understanding gaps in EMR implementation is crucial, according to research done by Janssen et al. and Akwaowo on EMR deployment in digital health,8,48 which seems to our study result of the low knowledge assessment, and low level of service coverage.
A previous study by Ayaad et al. that showed how EMRs can reduce handwriting errors, 49 the same as our findings benefits of EMR on digitalization efforts in this study. Bisrat et al. and others found that insufficient infrastructure, lack of managerial dedication, and inadequate training are key causes of EMR non-operation in resource-constrained countries like Ethiopia.6,19,36,50 These factors contribute to implementation challenges. Inversely, many stakeholders, including doctors, patients, communities, healthcare facilities, and the teaching-learning process, benefit from the use of EMRs in digitalization initiatives. Among these advantages, in addition reduction of handwritten errors, were ease of access to medical records, 51 improved communication among healthcare workers,52,53 and patients, timely care, accurate time allocation, 54 improved safety, quality, and cost efficiency,54,55 and patient privacy, confidentiality, and accurate information.53,56 The finding of this study aligns with the research of Ref., 57 referenced by Ibrahim et al., which highlights the importance of treating patients holistically, which improves comprehension of their problems and promotes easy communication between patients and healthcare professionals.48,58
Nonetheless, insufficient system design and poor user training are blamed for physicians’ difficulties using EMRs, which were consistent with the study.59,60 The development of a smart environment for all patients involved has advanced, enabling medical professionals to treat patients more effectively and enabling people to anticipate high-quality care from medical facilities. 61 Furthermore, according to a study by Setyadi and Nadjib, healthcare organizations could save operational expenses and boost revenue by efficiently using the EMR for routine procedures. 62 The advantages of EMRs in digitalization initiatives mark a significant turning point and a solid basis for further research and nationwide implementations that were inconsistent with the findings of. 63 It also helps patients by reducing the length of time they must wait for the findings of investigations. There are still issues, though, like the absence of an EMR manual or suggestions for the digitalization procedure that align with the research. 64 Writing recommendations that address particular problems with EMR adoption requires a professional and interesting approach to overcome these obstacles. 65 Every participant said that the system ought to change from being dependent on donors to being based on the government. Implementing EMR in all of the nation's remaining healthcare facilities is essential, as is making the data easily accessible for new technologies. System sustainability is an issue unless the administration makes a commitment to reform and pays attention to formulating Information Communication Technology (ICT) policy with incentives.
Limitations
There were some issues with our research. First off, the training was limited to front-line medical staff members. Secondly, the system has not been extended to include inpatient care also considered as another drawback. Thirdly, it was challenging to compare the selected case with others because it only included two hospitals in the area that had adopted an EMR system. Male respondents were also over-represented in comparison to female respondents. Lastly, this study was carried out too early in the hospital's EMR adoption process to pinpoint factors pertinent to the maturity level of EMR use.
Recommendation
In order to uncover profound insights into the digitalization of healthcare, one must study diligently to gain a comprehensive understanding of systems, information, and service qualities for future work.
Conclusions
EMR practitioners are responding favorably to the current evaluation of the EMR influence on healthcare digitalization initiatives. Approximately 29 medical professionals have expressed how much they enjoy using EMRs as opposed to paper records. However, because of inadequate knowledge assessment, there was a low degree of EMR implementation, which was caused by both system and human issues. For as long as the system was maintained and sustained, it was thought to be crucial that medical personnel could access patient data anytime they needed to through authorization.
Footnotes
Acknowledgments
To everyone who took part in this study, the authors would like to thank you for your assistance, especially Dr Abebe Megerso, Mr Ibrahim Mohammed, and Mr Hagos Birhane assistance.
Ethical approval
The study has been approved by Jimma University, Institute of Technology (Ref. No: Comp/JiT/019/2015 E.C). Later, this letter will be forwarded to the study site. We have obtained permission from relevant authorities to meet with interviewers, schedule interviews, and to gather data from respondents with data collectors. Once respondents have given their consent and confirmed their interest verbally and written format.
Contributorship
The manuscript has been read, approved, and confirmed by all named authors. There are no other individuals who meet the criteria for authorship other than those listed. The order of the authors was confirmed by all listed authors and approved for submission to the journal for publication.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This research received a grant from Jimma University, Institute of Technology for data collection (grant number Comp/JiT/019/2015).
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Guarantor
Jimma University, Institute of Technology was guarantor of my work.