
Abstract
While text messages or short messaging service programs are increasingly utilized for delivering health education, few studies have explored the unique challenges of recruiting and retaining participants in such programs. This study utilizes survey and focus group data from Text2BHealthy, a short messaging service–based nutrition and physical activity promotion program, to examine barriers to enrollment and facilitators of retention among parents of elementary school students. Results show that participants were hard to reach with recruitment materials, had difficulty with self-enrollment, and were apprehensive about program costs. However, 89–90 percent of participants were retained. Results suggest that providing manual enrollment options, alternative program delivery methods (e.g. email messages), and opportunities to reenroll may facilitate participation in short messaging service–based health education and promotion programs.
Introduction
There is growing evidence that text messaging or short messaging service (SMS) is a powerful tool for delivering health education. Using SMS for program delivery has several benefits. SMS has the potential for wide reach: 85 percent of Americans own a cell phone, 80 percent of cell phone owners send and receive text messages, and SMS is used by traditionally underserved and hard-to-access populations, such as low-income and minority individuals. 1 SMS is relatively inexpensive, easily sent to large audiences and tailored to individual people, and perceived as personal and informal, which may increase participant engagement. 2 Data about message content, when messages were sent, as well as message receipt and response can be recorded automatically for later analysis. SMS is also well-suited for delivering regular reminders, which are associated with behavior change. 3
Although SMS has been used for health education and promotion since only 2004, 4 programs that include a text message component have already been shown to effectively modify a range of health behaviors, such as smoking cessation,5,6 safe sex practices, 7 weight loss,8,9 improved dietary habits, 10 physical activity, 11 and diabetes management. 12 SMS has also been successfully used as appointment reminders, 13 to encourage participant retention, 14 for self-monitoring health behaviors, 15 to collect outcome data, 16 and to facilitate peer support for disease management. 17 SMS is an acceptable and effective means of program delivery for a range of populations, including low-income families, 18 parents, 19 and African American women. 20
For an SMS program to be successful, participants must enroll and remain in the program. In general, participants are enrolled in one of three ways: (1) participants self-enroll by texting a keyword to a phone number (usually five digits) or entering their phone numbers into an online form, (2) program staff manually enroll participants by entering their phone numbers into a message delivery system, or (3) participants are given cell phones to receive program messages.
Although crucial aspects of any program, there is limited research examining recruitment and retention for SMS programs. What little research exists suggests that recruitment is challenging. Text4Baby, a national initiative to improve maternal and infant health funded by a public–private partnership, fell 550,000 participants short of their goal to enroll one million mothers by the end of 2012.21,22 Similarly, only 38 percent of the 756 people who were offered an SMS smoking cessation program enrolled and used the program for at least 4 days. 23
Participants may struggle with self-enrollment in particular. In a study of Text4Baby enrollment, only 69 percent of the low-income women who attempted to self-enroll were successful. 24 Text4Baby now recommends that their partners enroll women on-site where they can provide in-person assistance. 24 Similarly, Aguilera and Muñoz 25 found it necessary to teach some of their low-income participants to use SMS.
The limited literature on recruitment to SMS programs suggests several factors associated with successful enrollment. Individuals who actively pursued an SMS program (rather than receiving an unsolicited invitation) and were contacted by phone (rather than email) were more likely to manually enroll in an SMS smoking cessation program. 23 Additionally, higher levels of education, higher household income, living in a household with fewer people, 24 and higher levels of health literacy 26 were linked with successful Text4Baby self-enrollment.
Retention may be less challenging than recruitment. A recent systematic review of type 1 diabetes interventions for children and teenagers that included a text message component found that only one of the seven programs reviewed had a retention rate below 80 percent. 27 Another systematic review of 12 health behavior change interventions where SMS was the primary program delivery mode found that only three programs retained fewer than 75 percent of their participants. 28 Additionally, in a study of Text4Baby retention (n = 209), 95 percent of the participants reported continuously receiving messages for at least 2 months. 24
SMS programs may share some recruitment and retention challenges with programs that use more traditional means of delivering health information. However, there are unique recruitment and retention challenges associated with SMS programs. This article makes an important contribution to the literature on SMS programs and provides useful information for program planners by exploring the barriers to enrollment and facilitators of retention encountered during the first 2 years of Text2BHealthy, an SMS-based nutrition and physical activity promotion program for low-income parents.
Method
Program description
Text2BHealthy is provided through a partnership between the Maryland Food Supplement Nutrition Education (FSNE) program and Title I elementary schools. Parents receive two to three SMS messages each week that promote behavior change and are targeted to their school. During year 1 (a pilot year from February 2012 to May 2012), six schools participated, and participants self-enrolled by sending an SMS to the program phone number or were manually enrolled. During year 2 (September 2012 to May 2013), 11 schools participated (five year 1 schools and six new schools), and the option to self-enroll online was added. An evaluation study of Text2BHealthy, including the measures described below, was approved by the appropriate institutional review board.
Recruitment efforts
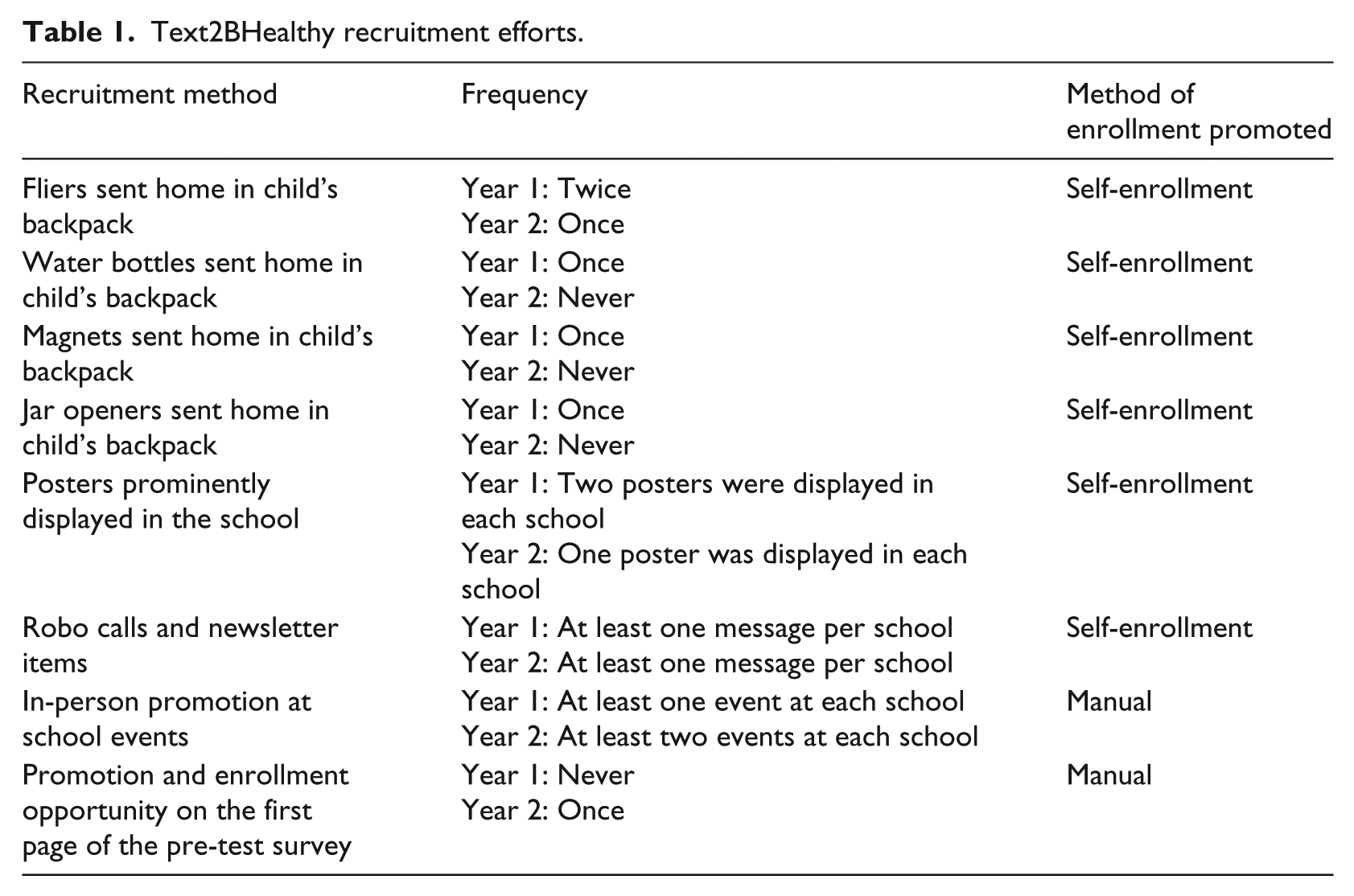
During year 1, parents received promotional materials explaining how to self-enroll, and FSNE educators promoted Text2BHealthy and helped parents enroll during school events (see Table 1). During year 2, parents were also able to enroll by providing their phone number on a pre-test survey. All recruitment efforts included information about potential program costs (regular SMS fees) and how to stop receiving messages. To avoid charging participants, individuals whose cell phone plans did not include unlimited SMS messages for a flat monthly rate were encouraged to receive messages via email.
Text2BHealthy recruitment efforts.
Measures
Post-Test Survey
In May of 2012, all parents with a child at a Text2BHealthy school received a Post-Test Survey (PTS) that measured program awareness, program satisfaction, enrollment barriers, cell phone and SMS usage, and program outcomes. PTSs were sent to parents and returned to the school through children’s backpacks. In all, 140 parents returned a PTS (5% response rate) (see Table 2).
Parent demographic characteristics.
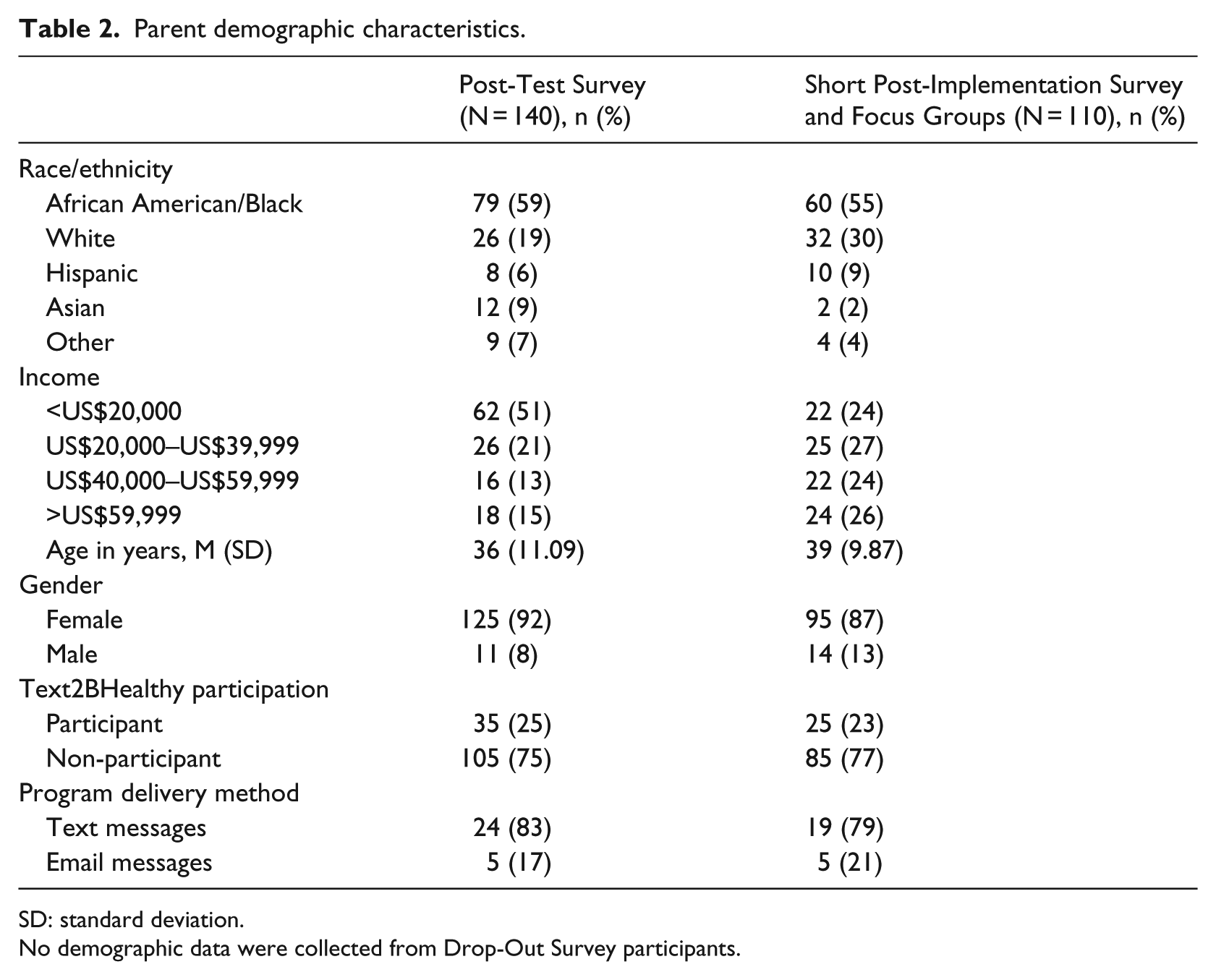
SD: standard deviation.
No demographic data were collected from Drop-Out Survey participants.
Short Post-Implementation Survey
To supplement the PTS, in May and June of 2012, Short Post-Implementation Surveys (SPISs) were administered to a convenience sample of parents at all six schools during end-of-the-year events. The two-page SPIS measured program awareness, program satisfaction, enrollment barriers, and cell phone and SMS usage. A total of 110 parents completed a SPIS (see Table 2). PTS and SPIS responses were not combined because parents who completed a PTS may have also completed a SPIS.
Post-Implementation Focus Groups
Four focus groups were conducted with parents at three schools in May and June of 2012. The focus groups generated detailed information about how parents learned about the program, program satisfaction, and why non-participants did not enroll in the program. All focus group participants also completed a SPIS.
Drop-Out Survey
During both program years, participants who left the program were called to determine why they left the program, program satisfaction, and whether they wanted to reenroll. Drop-Out Survey (DOS) response rates were 52 percent in year 1 and 44 percent in year 2.
Analysis
Frequencies, means, and standard deviations were calculated using SPSS version 17 (SPSS, Inc., Chicago, IL). Thematic analysis was used to analyze the qualitative data from the Post-Implementation Focus Groups (PIFGs). 29
Results
Enrollment rates
During year 1, 206 parents enrolled in Text2BHealthy, a 14 percent participation rate. In all, 19 parents manually enrolled, and 187 self-enrolled. During year 2, 1149 parents enrolled, a 25 percent participation rate. In all, 367 parents self-enrolled by sending an SMS to the program phone number, 4 parents self-enrolled online, and 778 parents were manually enrolled.
Barriers to enrollment
In all, 31 percent of PTS respondents and 51 percent of SPIS respondents who did not enroll reported that they had not heard of Text2BHealthy. In addition to program awareness, we identified three barriers to enrollment that are specific to SMS programs.
Inability to enroll
In all, 26 percent of PTS respondents and 4 percent of SPIS respondents reported that they were interested in the program but did not know how to enroll. During the PIFGs, we learned that some participants did not know how to send an SMS to someone who was not already in their cell phone’s address book, which is necessary to self-enroll. Also, some parents had disabled short codes from their cell phone plan, meaning they could not send an SMS to a shortened phone number, which is necessary to self-enroll. Disabled short codes may be an especially salient barrier for programs targeting parents, as our respondents reported disabling short codes so that their children could not accidentally enroll them in an SMS program that charges a fee.
Apprehension about SMS programs
During the PIFG, we learned that some parents did not enroll because they were apprehensive about signing up for an SMS program. These parents, who saw recruitment materials but did not speak with program staff, reported worrying about how much the program would cost them, how long they would have to remain enrolled, and the exact content of the messages.
Enrollment of non-parents
During the PIFG, we learned that people who were not parents at participating elementary schools had enrolled. We anticipated that some teachers and school administrators would sign up because our promotional materials were displayed in the schools. Unexpectedly, grandparents who were not their grandchildren’s primary caregivers and parents of preschool-aged children also enrolled because they wanted to learn more about events at their grandchildren’s school or their children’s future school, respectively.
Facilitators of retention
We had more success with retention than recruitment; we retained 90 percent of our participants in year 1 and 89 percent in year 2. The DOS improved retention by providing an opportunity to reenroll parents who had unintentionally left the program. During the first year, only one person was reenrolled, but during the second year, 30 parents (50% of DOS participants) were reenrolled after mistakenly removing themselves from the program.
Discussion
Using data from the first two years of Text2BHealthy, a nutrition education and physical activity promotion program, this study examined barriers to enrollment and facilitators of retention that are specific to SMS-based health promotion programs. We found several barriers to enrollment. Consistent with the extant literature, some parents had trouble self-enrolling in Text2BHealthy.24,26 Although 80 percent of cell phone users send and receive SMS, 1 it should not be assumed that participants will know how to self-enroll, especially if the target population is likely to have low levels of education or health literacy.24,26
A concern about program costs prevented some parents from enrolling. Despite clearly stating that only regular text message fees would apply on all recruitment materials, some parents reported not enrolling because they were concerned about program costs. Others reported disabling short codes so that their children could not unintentionally enroll them in expensive SMS programs. Recruitment materials should clearly state any program costs and how and when participants can leave the program. This information should also be provided in multiple forms (e.g. on a poster, flier, and in a newsletter).
Similar to other SMS programs, Text2BHealthy had a high retention rate. 28 However, more research is needed to determine how participants use the information they receive and whether they understand how to leave the program. Our experience conducting the DOS suggests that program planners should contact participants who leave SMS programs to find out why they left and give them the option to reenroll.
Limitations
There are some limitations to this study. Only a small proportion of parents who were offered Text2BHealthy and/or participated in the program completed a survey or participated in a focus group. These low response rates likely introduced bias. Additionally, our participants were parents of school-aged children and our findings may not generalize to other groups of SMS program participants, such as adolescents.
Implications for practice
Our results suggest several ways to improve enrollment rates for SMS programs. We found that potential participants struggled with self-enrollment, specifically sending an SMS to a phone number that was not already in their address book. SMS program planners should consider using manual enrollment and in-person recruitment when possible. Additionally, assistance with self-enrollment can be provided through a help phone number or email address that is answered by program staff or a website that provides detailed instructions for enrolling. Well-funded smaller programs may also consider giving participants cell phones and teaching them how to use them.
Offering an alternative to receiving messages via SMS, such as email messages, may also alleviate some concerns about the cost of the program. However, using another delivery mode may sacrifice some of the benefits of an SMS program (e.g. messages are seen as personal and casual and appear immediately on the phone’s screen, rather than being sent to a spam folder), but may retain other benefits (e.g. messages can be easily and inexpensively sent to multiple people).
Finally, program developers who allow self-enrollment should expect that people outside of their target population will enroll. Screener questions can be used to determine whether new enrollees meet inclusion criteria. This information can be analyzed later and may provide the opportunity to develop additional programming. For instance, Text2BHealthy messages could be developed for grandparents of elementary school children. SMS-based programming has the potential to elicit behavior change by providing relevant, personalized health education to participants’ cell phones; however, as detailed in this article, there are unique recruitment and retention issues to be considered.
Footnotes
Acknowledgements
The authors would like to thank Lisa Lachenmayr, Erin Braunscheidel-Duru, and Laryessa Worthington for their work designing and implementing Text2BHealthy.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: Text2BHealthy was funded by the United States Department of Agriculture’s Supplemental Nutrition Assistance Program in cooperation with the Maryland Department of Human Resources and the University of Maryland.