
Abstract
Vital sign documentation is crucial to detecting patient deterioration. Little is known about the documentation of vital signs in electronic health records. This study aimed to examine documentation of vital signs in electronic health records. We examined the vital signs documented in the electronic health records of patients who had suffered an in-hospital cardiac arrest and on whom cardiopulmonary resuscitation was attempted between 2007 and 2011 (n = 228), in a 372-bed district general hospital. We assessed the completeness of vital sign data compared to VitalPAC™ Early Warning Score and the location of vital signs within the electronic health records. There was a noticeable lack of completeness of vital signs. Vital signs were fragmented through various sections of the electronic health records. The study identified serious shortfalls in the representation of vital signs in the electronic health records, with consequential threats to patient safety.
Keywords
Introduction
Of the patients who suffer from in-hospital cardiac arrest, 80 per cent exhibit clinical signs of deterioration in the hours preceding the event.1–5 Early detection of these clinical signs has been shown to reduce the risk of in-hospital cardiac arrest.6–9 These critical signs indicate failing respiratory, cardiovascular or neurological systems and are identified by abnormal recordings of respiratory rate, heart rate, systolic blood pressure and temperature and altered mental state. The most important signs are related to deterioration in respiratory or mental functions. 10 Measuring and recording vital signs is the mainstay of detecting patient deterioration: accurate documentation is essential.
However, detecting deterioration and preventing cardiac arrest is a complex process and hospitals could benefit from adopting a ‘Chain of Prevention’. 11 This chain has five rings representing, staff education, monitoring, recognition, call for help and response. Monitoring vital signs can be defined as ‘the on-going assessment’ of a patient with the intention of (1) detecting an abnormality and (2) triggering a response if an abnormality is detected. 12 Given the increase in acuity of hospital patients today, close monitoring is more essential than ever. Hence, there is increasing use of early warning score (EWS) systems to aid effective monitoring and identify patients whose clinical condition is deteriorating.
Reasons for failure to recognise patient deterioration include infrequent, incomplete vital signs, lack of knowledge of the values of normal vital signs and poor design of vital sign charts. 13 Vital signs charts should be user-friendly to ensure that data are accurate, legible and easy to access,12,14 in order to support clinicians in decision-making. 12 It has been shown that the design of vital sign charts has an impact on the ability of clinical staff to detect patient deterioration.15–17
Electronic health record (EHR) systems are increasingly used for all aspects of clinical documentation, including vital signs. However, we were unable to identify any studies that specifically focused on the documentation of vital signs entered manually into an EHR, although there have been reports on vital signs entry into an EHR using a personalised digital assistant.14,18,19 A qualitative study aimed at exploring nurses’ perceptions of using an EHR in everyday practice found that there were difficulties encountered in documenting vital signs. 20 Thus, there is a need to identify features that are essential for facilitating clinical documentation to an acceptable level. Given the importance of vital sign data, there are the following two important research questions:
How is this clinical information presented in electronic systems of documentation?
Do these systems have any impact on detecting patient deterioration?
The overall aim of this study was to examine the documentation of vital signs in the EHRs of patients who subsequently had a cardiac arrest. More specifically, the objectives were to
Identify the extent to which vital signs were recorded in the EHR in the last 24 h prior to cardiac arrest in an acute hospital;
Compare the documentation of vital signs with respect to VitalPAC™ Early Warning Score (ViEWS) (Table 1), a track and trigger system (TTS);
Establish the extent to which this EHR supported the documentation of vital signs.
ViEWS. 21
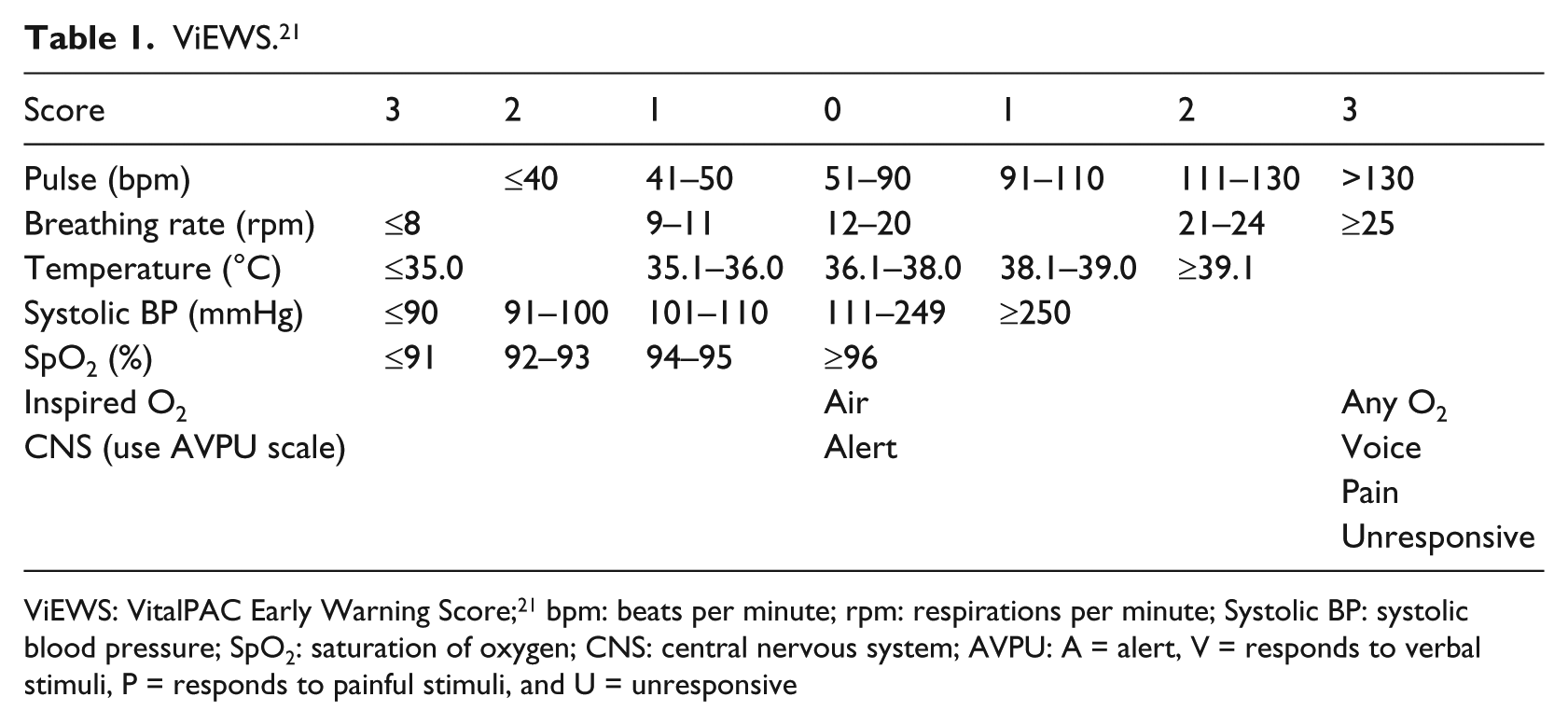
ViEWS: VitalPAC Early Warning Score; 21 bpm: beats per minute; rpm: respirations per minute; Systolic BP: systolic blood pressure; SpO2: saturation of oxygen; CNS: central nervous system; AVPU: A = alert, V = responds to verbal stimuli, P = responds to painful stimuli, and U = unresponsive
Methods
Study design and hospital setting
We undertook a retrospective population-based study in which we examined the electronic records for vital signs for all patients who had suffered a cardiac arrest at the study hospital from 2007 to 2011. The reason for choosing these patients was that we wanted to examine the records of patients who had been at risk of deterioration; patients who had suffered a cardiac arrest would thus be an appropriate group. The study hospital was a district general hospital of 372 beds in southeast Sweden. The study comprised all patients from this hospital who had suffered an in-hospital cardiac arrest and on whom resuscitation had been attempted (n = 228). These patients were identified using the Swedish Register for In-hospital Cardiac Arrest. 22 This register is for patients who have had resuscitation attempted following cardiac arrest in hospital. From the information in the register, each patient’s EHR was located.
Implementation of the EHR
The EHR (Cosmic; Cambio Healthcare Systems, Stockholm, Sweden) was implemented at the study hospital in June 2007. The health board had undertaken a pilot implementation in the Psychiatric Department of the hospital. Some changes were made before implementation at the main hospital. Ward staff were given training prior to implementation in the form of 3 days of classroom instruction during spring 2007, with a half-day follow-up during autumn 2007.
Data sources
We collected the following data from each patient’s EHR: demographic information (i.e. gender, age), level of care, type of ward and all data on traditional vital signs documented in the 24-h period prior to cardiac arrest. The vital signs selected for collection were based on the parameters used in an aggregated weighted scoring system, ViEWS, 21 as shown in Table 1. ViEWS comprises heart rate (beats per minute), respiratory rate (breaths per minute), body temperature (°C), systolic blood pressure (mmHg), oxygen saturation (%), administration of supplementary oxygen (yes or no (Y/N)) and conscious level, measured using the AVPU scale (A = alert, V = responds to verbal stimuli, P = responds to painful stimuli and U = unresponsive).
We also recorded where each of the vital signs was located within the EHR. There were three possible locations: the journal, the template and the report sheet. The journal was used by nursing as well as medical staff for all types of documentation, including patient history, management plan and progress notes. Most recent entries were at the top of the page in a scrolling system. The template section was used by both medical and nursing staff and included the headings temperature, pulse, respiratory rate, blood pressure and oxygen saturation. The report sheet was used exclusively by nursing staff. The most recent entries were at the end of the report sheet. To find this information, the appropriate date was entered into a calendar system.
Data analysis
The Statistical Package for Social Sciences (SPSS) version 19 was used for descriptive analyses to determine the completeness of vital sign recordings when compared to ViEWS and the location of vital signs within the EHR.
The TTS used as a model for data collection in this study was the aggregated weighted scoring system, ViEWS, 21 as shown in Table 1. ViEWS was adopted as the National Early Warning Score (NEWS) system in Ireland 23 and is used as the basis for the NEWS system adopted in England. 24 Thus, using ViEWS provided an audit standard and would demonstrate whether vital signs had been recorded to this recommended standard. ViEWS contains seven vital parameters, each one being given a score between 0 and 3 depending on a graded scoring system. Scores of 3 or more are triggers which indicate the need for escalation of care, such as increasing the frequency of clinical monitoring or notifying medical staff. As BAS (B: ‘blodtryck’ (systolic blood pressure), A: ‘andnings frekvens’ (respiratory rate) and S: ‘saturation’ (oxygen saturation)) was used as the TTS at the study hospital, this system is also described.
Hospital policy on minimal vital signs monitoring
According to hospital policy, BAS should be recorded on admission and at least once per day. The Swedish BAS/90-30-90 system had been implemented in the study hospital in 2007 (BAS). 25 The values 90-30-90 denote the threshold levels for these vital signs, respectively. BAS is a single-parameter TTS, primarily derived to detect sepsis, in which one (or more) of the signs deviating from the 90-30-90 parameters indicates patient deterioration. Thus, either a systolic blood pressure of less than 90 mmHg or a respiratory rate of more than 30 min−1 or an oxygen saturation level of less than 90 per cent would be triggers for action to prevent further deterioration. Although aimed towards detection of sepsis, BAS duplicates three of the parameters used in ViEWS although the threshold for respiratory rate is different.
Ethical approval
We received approval for the study from the Regional Ethical Review Board, Linköping University, Sweden.
Results
Demographics
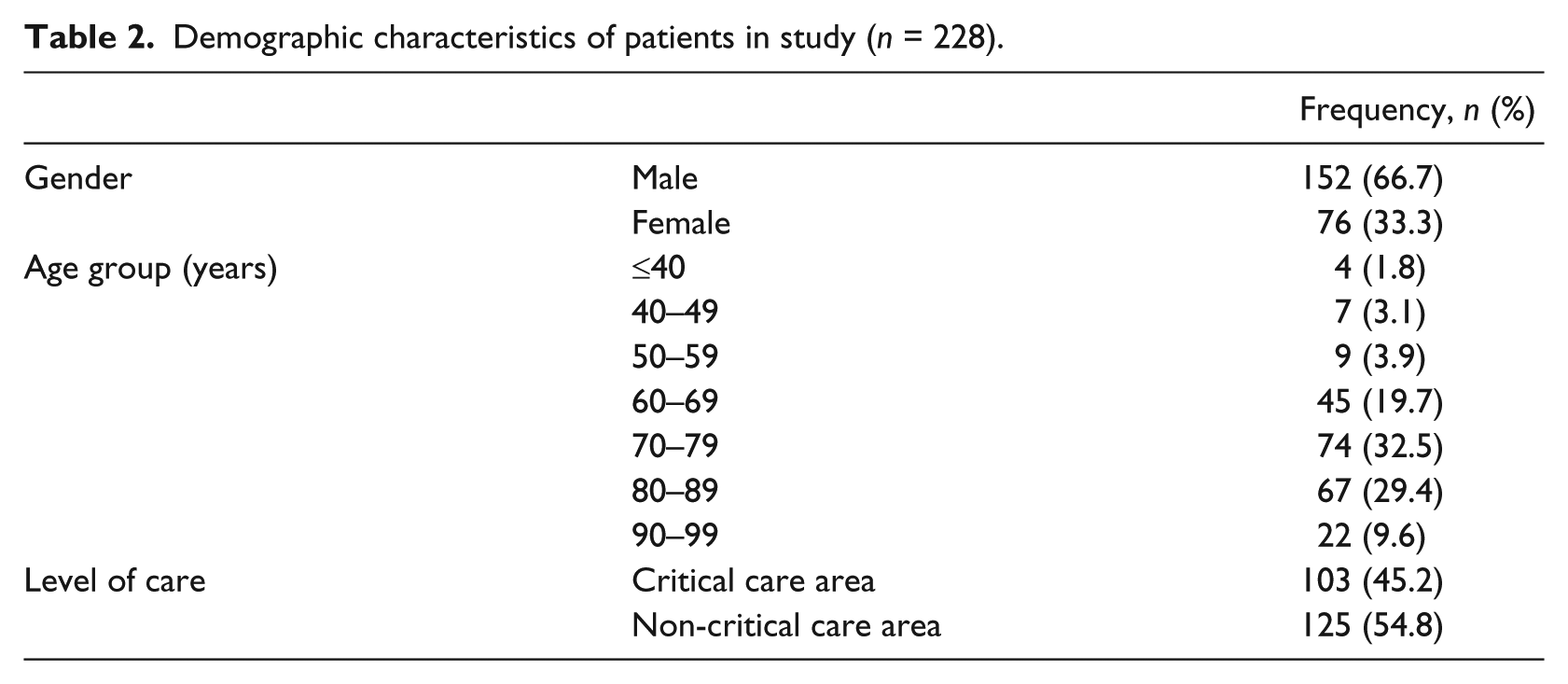
Table 2 shows gender, age and level of care for the 228 patients who had suffered an in-hospital cardiac arrest and on whom cardiopulmonary resuscitation had been attempted between 2007 and 2011. Patients were from both general wards (54.8%) and critical care areas. The critical care areas included the cardiac catheterisation laboratory and the coronary care unit (CCU), but not the intensive care unit (ICU) as no cardiac arrests were reported to the register from there during the study period.
Demographic characteristics of patients in study (n = 228).
Extent to which vital signs were documented
We calculated how many patients had vital signs recorded in the EHR at least once in the 24-h period prior to cardiac arrest. A total of 35 patients (15%) had no vital signs documented. Just over 30 per cent had two or fewer vital signs documented (n = 76). Only seven patients had all seven vital signs documented.
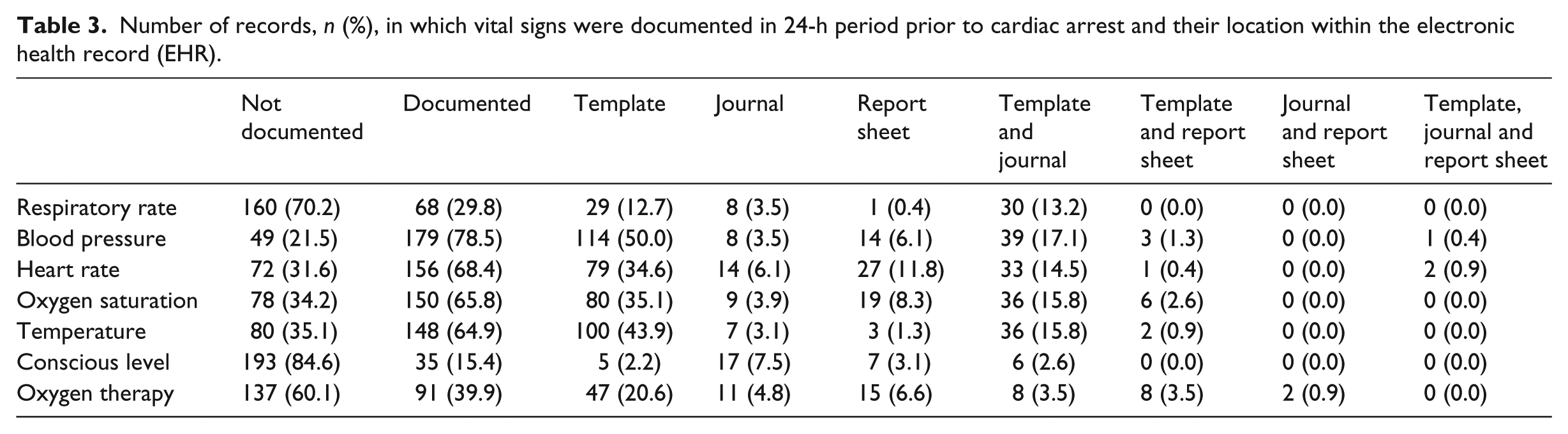
We calculated the percentage of patient records that included each of the vital signs at least once in the 24 h prior to cardiac arrest (Table 3).
Number of records, n (%), in which vital signs were documented in 24-h period prior to cardiac arrest and their location within the electronic health record (EHR).
Completeness of vital signs in 24-h period prior to cardiac arrest based on ViEWS
Table 3 shows the completeness of vital sign documentation (Column 3) and the omissions (Column 2). The percentage of records within which the vital signs were recorded at least once varied from 15.8 per cent (conscious level) to 78.5 per cent (systolic blood pressure). Heart rate, oxygen saturation and temperature were each documented in approximately two-thirds of all patients.
Location of vital signs in the EHR
Table 3 also shows the distribution of vital signs within the EHR. There was no graphical presentation of any of the parameters; all information was presented in numerical text form. Of the three locations in which vital signs were documented, the most frequent was the template section. However, the most frequent location in which conscious level was recorded was the journal section. Table 3 also makes clear the fragmentation of the recording of vital signs throughout the EHR. For example, of the 68.4 per cent heart rate entries, approximately half were found in the template, nearly 12 per cent in the report sheet and 14.5 per cent in both the template and journal.
Extent to which vital signs were recorded in relation to type of clinical area
There was a higher percentage of all recorded vital signs in general wards than in critical care areas, with the exception of conscious level (Table 4). This may be explained by the closer surveillance of patients in critical care areas, where there is often continuous monitoring. This could mean that the vital signs were measured, but were not always documented.
Number of records, n (%), in which vital signs were documented in 24-h period in CC areas and general ward areas (Ward).
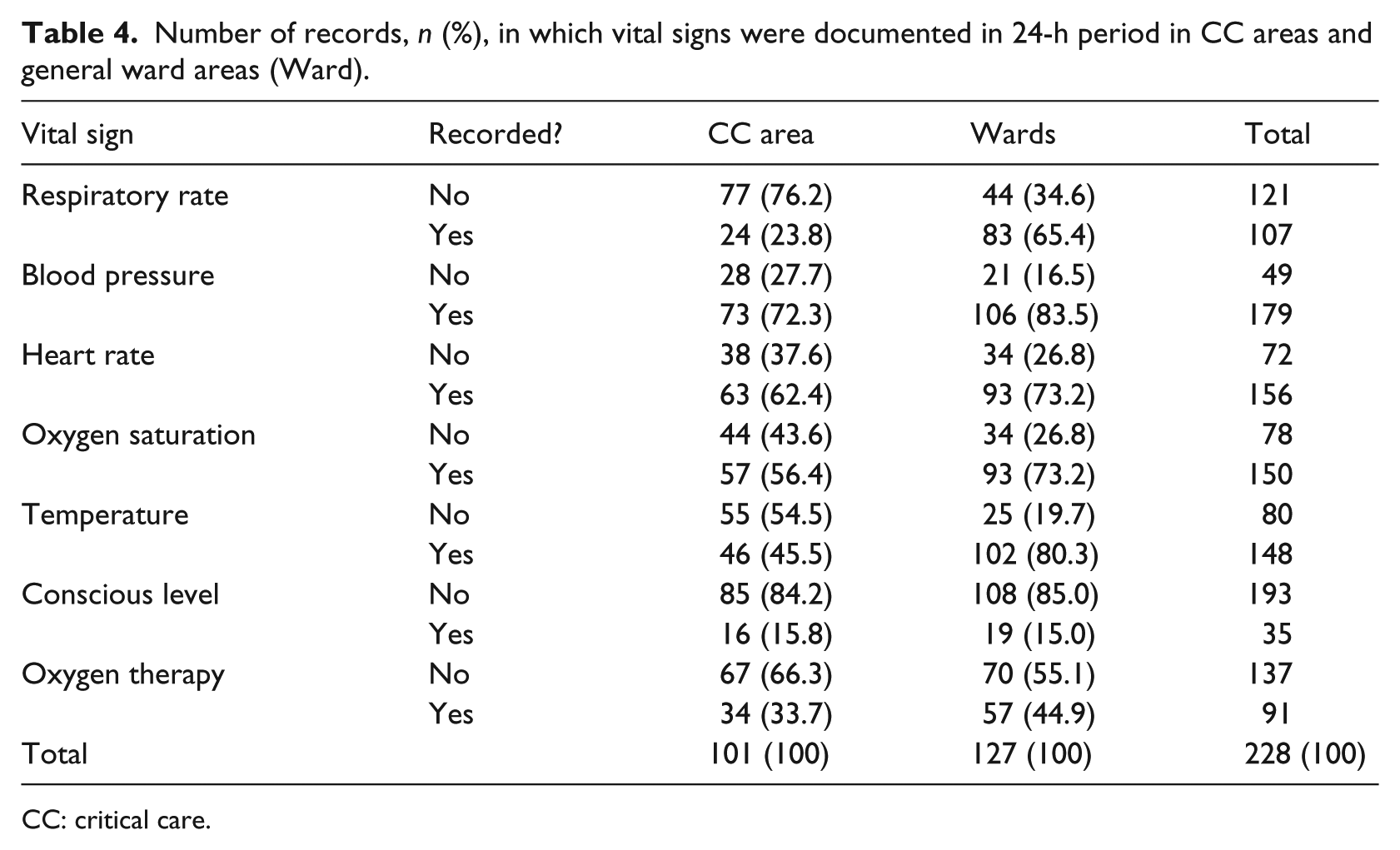
CC: critical care.
Discussion
Summary of key findings
The objectives of this study were to identify the extent to which vital signs were recorded in an EHR, in relation to recommendations for the observation of acute patients, and to establish the extent to which this EHR supported the documentation of vital signs. There were two key findings in this study. First, there was a noticeable lack of completeness of vital sign documentation in the EHR. Second, the location of vital signs within the EHR was fragmented and inconsistent.
Completeness of documentation
The results of this study demonstrate a clear lack of documentation of vital signs in the 24-h period prior to sudden cardiac arrest, when compared to recommendations for the observation of acute patients.21,23,24 According to other studies, reasons for incomplete vital sign documentation could include lack of resources, for example, not enough staff and lack of time;26,27 lack of training and lack of knowledge regarding the importance of vital sign documentation1,2,28–30 and lack of explicit routines for vital sign recording. 31 Moreover, there could be cases where vital signs had been measured but not documented; this study only shows what was documented. There is also the possibility that some of the patients who suffered cardiac arrest were actually expected to die, and although a clear decision for ‘not for resuscitation’ had not been made, staff had decided to not measure and/or record vital signs.
In this case, there may have been a lack of routines for monitoring patients. 31 The hospital did use BAS as a TTS, which, according to hospital policy, should be measured and documented on admission and at least once per day. As BAS includes the monitoring of respiratory rate, the frequency of respiratory rate recordings might have been expected to be higher. However, BAS had been implemented at the hospital in 2007, and since then there had not been any further in-service education. This implies that there may be a need for further staff training.
Effective monitoring of vital signs and detecting deterioration is a complex, challenging process. First, vital signs must be measured regularly and accurately. Second, these measurements must be documented promptly and precisely, and third, the vital signs must be presented in a way that allows interpretation of any deviation from the norm. This is not a new concept, rather it has been around since the time of Florence Nightingale and since Harvey Cushing and Ernest Codman first used charts to document patients’ vital signs during surgery. 32 These charts have seen little variation in the last 150 years and thus have been the backbone for documenting and interpreting vital signs by clinical staff.
However, because of increased attention on patient monitoring in the last two decades, there has been a new emphasis on the design of observation charts.13,26,29,33,34 Clear visual representation of vital signs have been shown to improve early detection of patient deterioration.15,16 Important features are that plotted charts are more easily interpreted than written numerical values,
15
and colour-coded TTS charts outperform non-colour charts. Subsequently, the design of observation charts has dramatic effects on both the ability of individuals to detect abnormal vital signs as well as the time taken to make those judgments … [thus] the way that observation charts are designed is likely to have a substantial impact on patient safety.
16
This has led to calls for standardised charting systems, which incorporate these features.15,16,31,35 These appeals have resulted in the development of standardised paper charts for early warning systems such as the Scottish Standardised Early Warning Scores (SEWS) 36 and NEWS in England and Ireland.23,24 Recording vital signs on paper charts has stood the test of time. Clearly, if documentation of vital signs is going to shift from a paper to an electronic system, lessons should be drawn from what is known about documentation on paper charts.
Is the documentation of vital signs supported in this EHR?
Superficially, the EHR did appear to support the documentation of vital signs inasmuch as it is possible to record this information in the system. However, our study revealed that the vital signs could be found in any one or more of three different sections of the EHR and this suggests that there was confusion about the specific location in which they should be documented. There was no consensus between different wards, and sometimes within the same ward as to which of these three sections was correct. Some nurses believed that the template was the correct place and others thought that vital signs should be in the report sheet. 20 The hospital did not have a policy for where vital signs should be documented. Thus, the choice of where to document vital signs was an option largely left to bedside staff. This is a possible explanation for the haphazard documentation of vital signs in this EHR.
In addition to confusion about the correct location for vital signs, there were usability issues. We realised during the data collection that entering data on vital signs was a complex process as it would involve multiple screen changes for each sign to be documented.20,37–40 Some nurses have indicated that ‘… it takes rather many clicks in order to make a template, it certainly takes ten’. 20 A previous study found that it was possible to produce a visual graph of the vital signs if these data were entered into the template section. However, producing a graph required further complicated steps and most nurses did not know how to do this or found the system too awkward to use. Furthermore, it may have been deemed not worth the extra effort and time as each vital sign could only be viewed as numbers on separate screens, so they could not obtain an overview of consecutive recordings, 20 an issue reported in previous studies.37,41–43 This meant that users would have to remember each of the vital signs as they clicked from one screen to another to be informed about variations and trends. This would place additional demands on memory and cognition, thereby reducing the ability to interpret data and detect changes, for example, deterioration. This indicates that the design of this system was awkward to use, not intuitive and increased the workload of staff. In a busy ward environment, this may have deterred staff from documenting the vital signs, even if they had been measured. Moreover, we observed that finding vital signs was difficult and staff may have felt there was little point in entering vital signs if they were to be ‘lost in the system’.
Because of these usability issues, there was no apparent means of viewing a patient’s clinical status effectively or efficiently. Thus, we suspect that the EHR in this study could impede the identification of clinical deterioration because of the difficulty in accessing essential patient data required when making life-saving decisions. For instance, if the first action taken by doctors when assessing an acutely ill patient were to inspect the ‘observation charts’, 44 it was not clear whether a patient’s vital signs could be quickly assessed from this EHR. Clearly, this poses potential threats to patient safety and contradicts the aim of technology to complement clinical care. 45
Problems may also be related to implementation of the EHR. Unsuccessful implementation of information technology in health care is not unusual. 46 Successful implementation is dependent on system design and staff training. 47 The EHR should be user-friendly, facilitate clinical work and be easily modified. 47 User-friendliness implies that the system is easily navigable and that patient information can be viewed at a glance; this was not evident in this EHR. Second, facilitating clinical work requires a system to take account of work routines so that it seamlessly fits in with the working patterns of clinical staff. For this to happen, clinical staff should be involved in the design of EHR. As nurses pointed out in a previous study, no one asked them what they required, 20 which is not unusual. 43 Developers need insight into everyday work patterns before attempting to design a system for which they lack understanding. 48 Systems should be easy to modify but in this system it was hard to change things as users were not invited to share their opinions. 20 Lack of consultation with clinical staff may have led to poor facilities for the documentation of vital signs in this EHR.
Staff training of 3 days and technical support for 1 week after implementation may have been insufficient given the demands of changing from paper records to EHR. Staff experienced that their complaints about the system were rarely acted upon, so instead, they found ways to work around the system, for example, taking notes in pocket books and having more verbal reports. 20 Consequently, the design of this EHR and its implementation may have been inadequate and may have inadvertently had a negative impact on patient safety.
Interestingly, in the study hospital, the staff in the ICU did not accept the EHR for documentation of vital signs and made the decision to retain their paper charts. As the charge nurse said, ‘We decided not to use the EHR for documentation of vital signs as you can’t get an overview of vital signs in the EHR’ (K. Rommedahl, 29 November 2013, personal communication). They appear to have had the same view as Coiera 49 when he suggested that ‘It is possible for a well-designed set of paper forms to be far more effective in improving the quality of a medical record than a poorly designed computer-based one’.
What lessons can be learned from this study?
If the facility for documentation in an EHR is not user-friendly and does not fit in with the work patterns of users, it is likely that documentation will be poor. Thus, manufacturers have a responsibility to understand the work patterns of users. At an organisational level, managers have a responsibility to insist on a design that will complement care, assist clinical staff in their work and which is legally accountable. Therefore, the process of procurement must include assurances for patient safety and regard to the requirements of clinical staff. Minimal essential features of an optimal system include easy entry and retrieval of information, and that trends and variations can be identified at a glance, thus detecting any clinical deterioration early and promoting patient safety. An EHR which does not facilitate good documentation could potentially lead to legal problems in cases of medical liability – ‘if it isn’t documented, it isn’t done’. 33
Ideally, it should be possible to record vital signs at the bedside, for example, using a palm top or tablet that is automatically relayed to a central system. For instance, VitalPAC utilises handheld devices in which vital signs can be entered at the bedside and sent directly to a computer at the nurses’ station. VitalPAC is combined with a TTS so that abnormal EWS scores are flagged to alert staff to deviations from normal. 19
Whichever software is used, it would be beneficial if a TTS could be incorporated into the EHR and abnormal vital signs flagged to alert clinicians of patient deterioration.
Strengths and limitations
A strength of our study is that we know each of the patients whose records we examined had suffered a cardiac arrest and therefore may have deteriorated in the final 24 h prior to arrest. The fact that they had had a cardiac arrest indicated that they belonged to an at-risk group and we presumed that they may have been under close monitoring, have additional vital signs documented and, thus, provide rich data about vital signs in the EHR. A limitation of the study is that we cannot be sure whether documentation would have been more complete if paper charts had been used as we did not carry out a study before the implementation of the EHR. The study is also limited in that it only includes one medium-sized hospital and a relatively small cohort of 228 patients. Furthermore, we only investigated the use of one EHR system, so the results could not be generalised to all EHRs.
Conclusion
However, although our results may not be generalisable, this study does identify and clarify issues that manufacturers should take into account in design and that organisations need to consider before purchasing an EHR. We believe that it can assist organisations in making decisions about which type of EHR to adopt. It can help to identify features which are essential for facilitating clinical documentation to an acceptable level. Moreover, this study deduces the potential benefits that an EHR which incorporates a TTS could have for patient safety. A user-friendly facility in the EHR could enhance adherence to policies regarding routines for measuring and recording vital signs. It may also be time to introduce a more robust TTS that is in line with documented recommendations for monitoring acute patients, for example, a validated system such as ViEWS, which incorporates additional parameters, for example, conscious level. The educational needs of staff caring for acute hospital patients would be inherent to this development.
As this research only examines one EHR, further research is required to examine facilities for vital signs recorded in other systems. However, this system is widely used in Sweden, and therefore, facilities for documenting vital signs in these systems should be reassessed as a matter of urgency.
Importantly, this is a study of patients who have suffered a cardiac arrest, not a group of general patients; therefore, an urgent question is whether improved documentation facilities and closer monitoring of vital signs would result in fewer cardiac arrests.
Footnotes
Acknowledgements
The authors would like to acknowledge the cooperation of the study hospital and the Swedish Register for In-hospital Cardiac Arrest for allowing us to collect data from the electronic health records and register, respectively. Furthermore, we would like to thank the Information School, University of Sheffield, the United Kingdom; eHealth Institute, Linnaeus University, Sweden and Kalmar County Health Authority, Sweden for supporting this study.
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.