
Abstract
The deployment of electronic health record systems is deemed to play a decisive role in the transformations currently being implemented in primary care medical practices. This study aims to characterize electronic health record systems from the perspective of family physicians. To achieve this goal, we conducted a survey of physicians practising in private clinics located in Quebec, Canada. We used valid responses from 331 respondents who were found to be representative of the larger population. Data provided by the physicians using the top three electronic health record software products were analysed in order to obtain statistically adequate sub-sample sizes. Significant differences were observed among the three products with regard to their functional capability. The extent to which each of the electronic health record functionalities are used by physicians also varied significantly. Our results confirm that the electronic health record artefact ‘does matter’, its clinical functionalities explaining why certain physicians make more extended use of their system than others.
Keywords
Introduction
The deployment and use of information technology (IT) artefacts play a critical role in the profound changes occurring in health care systems around the world. Among these artefacts, electronic health record (EHR) systems are designed to support the core activities of primary care physicians and other health care professionals in medical practices and ambulatory care settings. EHR systems aim to support patient-centred care, the coordination of such care, and the exchange of clinical information to improve quality of care.1,2
Despite the potential benefits associated with these systems, problems remain with regard to achieving extensive and mindful use by primary care physicians.3–5 This may be due to a lack of awareness, as a significant gap has been identified between the functionalities presently offered in EHR systems and those actually being used by physicians. 6 It may also be due to software vendors, medical associations, and health care authorities that emphasize the automational impacts of EHR solutions, 7 seeking to implement the ‘paperless’ primary care practice 8 at the expense of the informational and transformational impacts that would lead to the ‘smart’ medical practice. 9
While previous research has suggested than less-than-optimal use of the EHR artefact might be related to a lack of awareness of functionality or insufficient emphasis on the transformational potential of this type of system, we propose a third explanation which focuses on the differences among EHR artefacts with regard to their functional capabilities. As a fact, functional differences exist between the various EHR software products available on the market, 10 despite the creation by governments in recent years of EHR software certification and adoption incentive programs, 5 brought about by the push for more meaningful EHR use in the United States 11 or more extended use in countries with national health care systems such as the United Kingdom and Canada.12,13 Since EHR systems are not all created equal by software vendors,14,15 it becomes relevant and important to ask whether such differences in terms of system functionalities influence usage by primary care physicians.
In light of the above, this study aims to conceptualize the EHR artefact, and to do so in a comprehensive and multi-faceted manner in order to place it at the theoretical and empirical core of the medical informatics field. 16 Since EHR systems are highly contextualized due to their mission-critical nature, 5 we intend to generate empirically valid and useful findings on how these systems are characterized as IT artefacts from the perspective of their main users, that is, primary care physicians. To this end, we seek to answer the following research questions: What are the differences between the various commercial EHR solutions in terms of ease of use and context of use? What are the differences between EHR artefacts in terms of the clinical, communication, and administrative functionalities that are available to primary care physicians? And, most importantly, do these differences explain the extent of EHR use by family physicians?
Background
This study emanates from a body of work that has sought to define and characterize the IT artefact for Information Systems (IS) research purposes, focusing on its nature as a software application. 17 From this perspective, EHR systems are considered as software packages developed and commercialized by software vendors, whose design attributes are meant to support medical practices. 18 In conceptualizing and theorizing EHRs as an IT artefact, the ultimate aim is to better understand the extent of fit between the design of an EHR system and both the practice’s processes and a physician’s main tasks. 19
The fundamental differences between system designers and users were initially ascertained by researchers investigating business software design in general. 20 Users have been found to use software in ways not anticipated by designers, 21 to differ from designers in their satisfaction with design methodologies, 22 and to behave differently from what was expected by the designers when they access business Web sites. 23 Similar discrepancies have also been identified between developers’ and users’ appraisals of the technology-task fit of health IT artefacts such as PACS (picture archiving and communication systems) and EHR systems.24,25
The user’s perspective differs from the software designer’s perspective. The former is in the presence of an empirical – as opposed to a theoretical – artefact whose conceptualization is founded upon a functional configuration, that is, the functionalities of the EHR system actually being used; whether such a configuration has been designed by the software developer or has emerged from the user’s adaptations. Table 1 synthesizes the two research perspectives on the EHR artefact in terms of the research focus, the research variables, the basis for understanding the EHR artefact, and the implications for EHR research and practice. 26
Two complementary research perspectives on the EHR artefact.
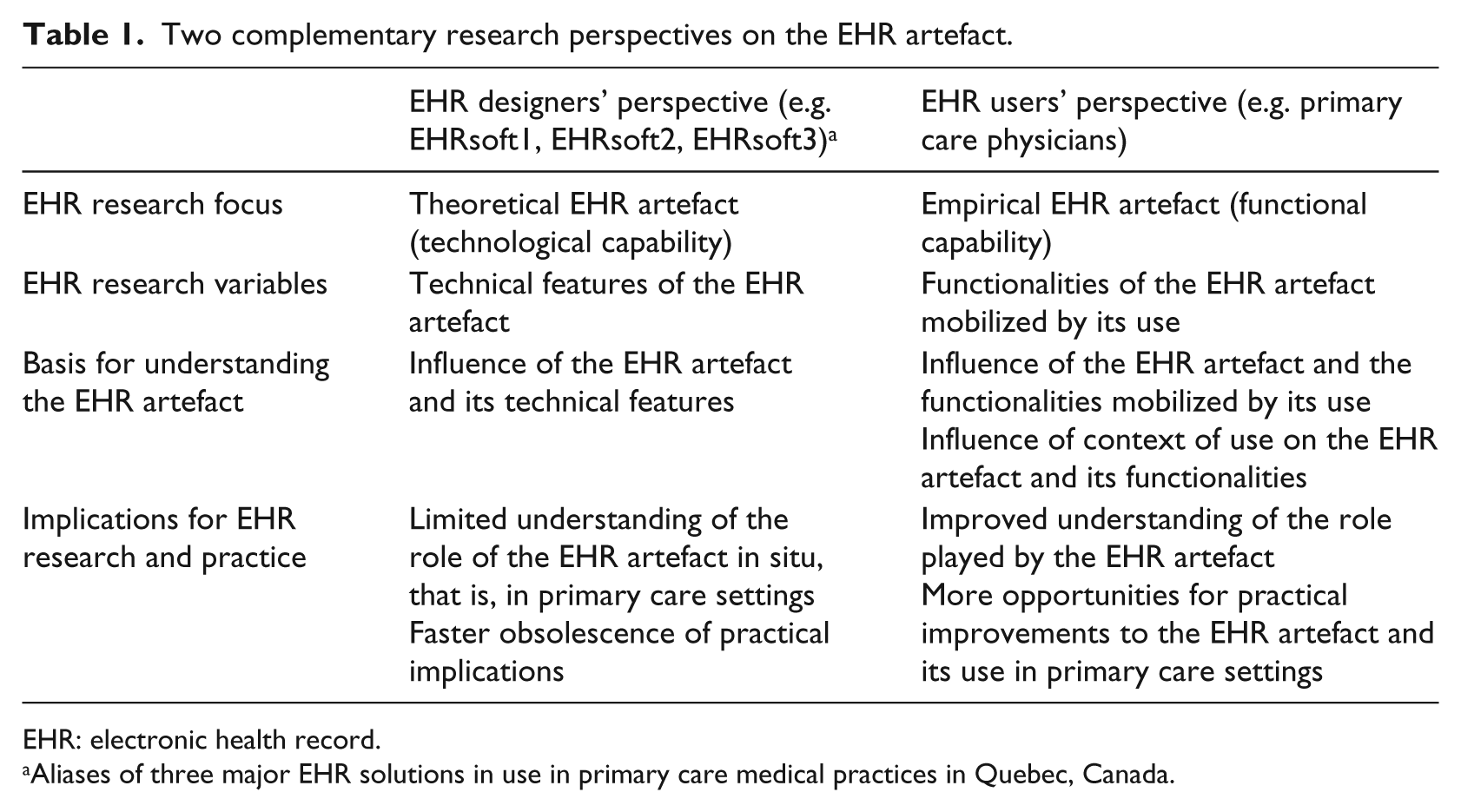
EHR: electronic health record.
Aliases of three major EHR solutions in use in primary care medical practices in Quebec, Canada.
The user’s perspective focuses on the why of the EHR artefact’s existence, on the needs of users (including how they change over time), and on how they can use and adapt this artefact in a complex and dynamic social context. 27 Implications for practice are thus centred on the artefact’s usefulness, that is, on the functional evolution (customization) of the EHR artefact, made in collaboration with the artefact’s vendor, in order to optimize its use by primary care physicians.28,29 In our previous work, 6 we reviewed the relevant literature30–34 to identify the functionalities required by EHR artefacts to fulfil their purpose in primary care settings. These functionalities were then classified along three dimensions: clinical, communication, and administrative.
Figure 1 presents the formative model of the EHR artefact that emerged from our previous study. 6 By characterizing an IT artefact in this way, we seek to represent the user’s perspective as founded on the functionalities actually used. 35 More precisely, the EHR artefact construct is operationalized through the three functional dimensions identified above, each dimension capturing a different aspect of the construct, and the combination of the three defining the construct. Hence, the EHR artefact is modelled as a formative construct in light of its composite and multidimensional nature. 36
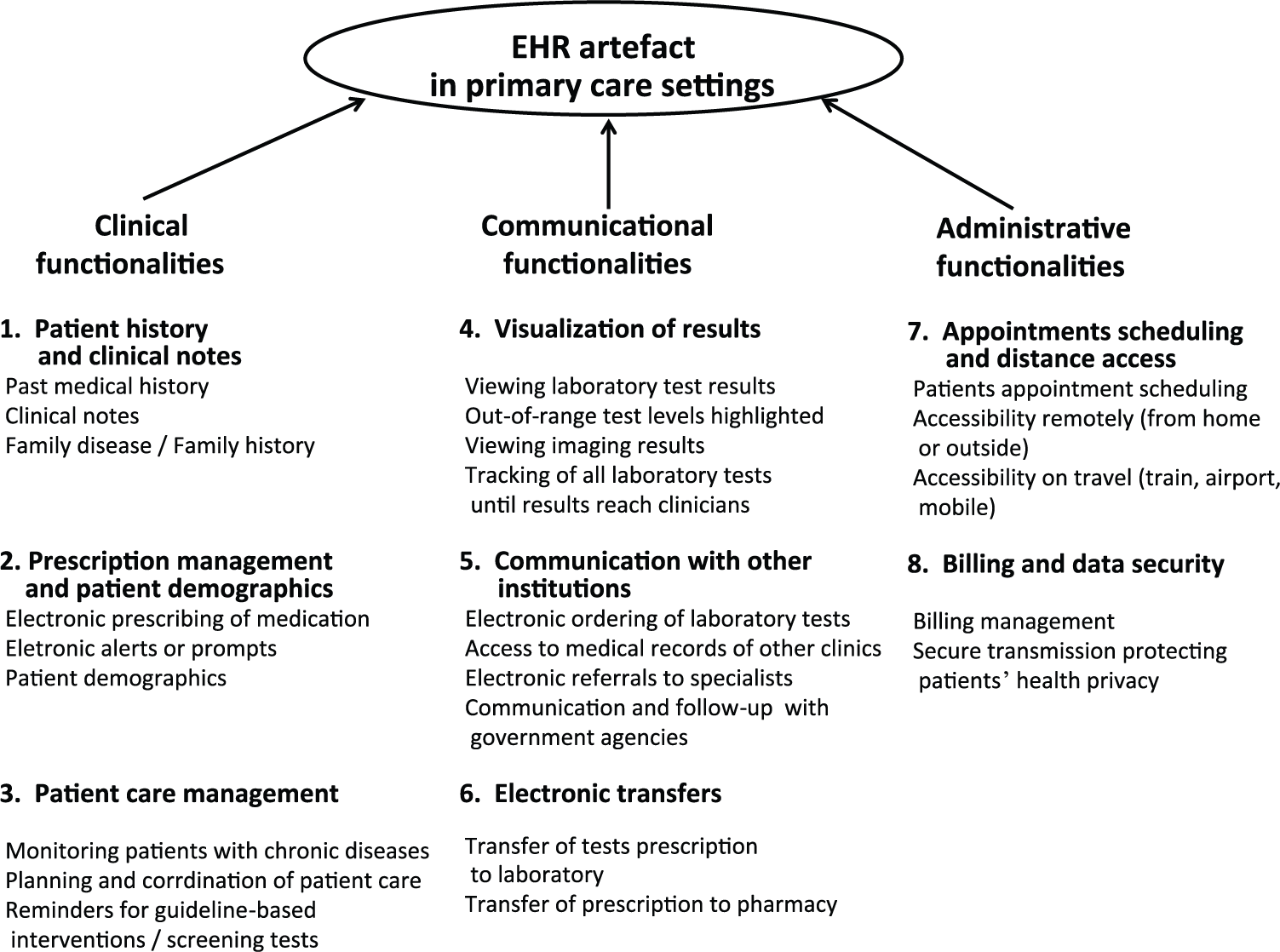
Formative model of the EHR artefact as used in primary care settings.
Method
We employed a Web-based survey to collect data for our research questions. We approached the 4845 members of the Quebec Federation of General Practitioners (QFGP), in the province of Quebec, Canada, who could be reached by email. Valid responses were obtained from 780 family physicians. While the survey’s 16 per cent response rate appears satisfactory, the potential for response bias was assessed by comparing the 156 late respondents (i.e. those who answered after receiving a reminder sent 1 week after the initial invitation to participate) with the 624 early respondents. As no statistically significant difference was found between these two sets of respondents on all attributes, response bias was deemed unlikely. 37 The sample was also confirmed to be statistically representative of the target population, that is, the QFGP’s members, in terms of age, gender, and years of professional experience.
While the survey initially targeted two different types of physicians – those working in medical practices with and without EHR systems – only the responses from the 331 physicians who were actually using EHR systems are of interest here. Using an initial list of 24 EHR system functionalities (see Figure 1), we asked our respondents to indicate whether each functionality was available (or not) in their EHR system, and if available, whether they actually used it (or not). We also asked them to indicate their level of satisfaction with each of these functionalities using a 5-point scale (1: very dissatisfied, 5: very satisfied). The EHR artefact’s ease of use, that is, the extent to which the respondent perceived its use to be free of effort, was measured with an instrument borrowed from the Commonwealth Fund’s international survey of primary care physicians, 38 composed of eight 5-point scales (1: unable to use, 2: difficult, 3: neutral, 4: easy, 5: very easy to use). We confirmed its reliability (Cronbach’s α = 0.81). Note that this measure is bi-dimensional, 6 as two items indicate ease of use in patient management (e.g. ‘List of all medications taken by an individual patient’) and six items indicate ease of use in communicating with care providers (e.g. ‘List of patients vulnerable or not vulnerable to specific diagnoses/disease cohorts’).
The context of use of the EHR artefact was ascertained by asking respondents to indicate the length of their experience (in years) as a family physician and as a user of EHR systems, as well as the size and EHR experience of the medical practice in which they worked (number of physicians and number of years since the first EHR implementation, respectively). Finally, given the nature of the initial research questions, the collected data were interpreted through analysis of variance (ANOVA) and analysis of covariance (ANCOVA), as well as through regression analyses.
Results
Out of the 331 primary care physicians who used an EHR artefact, 48 per cent were women. As for their age, 38 per cent were in their 50s, 28 per cent in their 40s, and 19 per cent in their 30s. They had an average of 22 years’ experience in the medical profession, with a minimum of 2 and a maximum of 45. They also had an average of 4 years’ experience using their clinic’s EHR system, with 56 per cent of the sampled physicians having 3 years of experience or less. Moreover, 167 physicians (50.5%) indicated using EHRsoft1’s EHR software product, 66 (20%) used EHRsoft2’s product, 48 (14.5%) used EHRsoft3’s product, while the 50 other physicians (15%) used a variety of other EHR software products. Note that all EHR vendor names in this study are aliases. Since answering our research questions requires making comparisons of the functional configuration of the EHR artefacts deployed in primary care settings, we analysed only the data provided by the physicians using the three main vendors’ EHR software products (n = 281) in order to obtain statistically adequate sub-sample sizes.
Given our study’s main objective and the ensuing formative model of the EHR artefact (Figure 1), our first analytical task is to describe and characterize this artefact from the family physician’s perspective. Concerning our first research question, the results presented in Table 2 indicate one significant difference in the contexts of use of the three EHR artefacts: the 167 physicians using EHRsoft1’s software product had significantly less experience using their EHR (3 years on average) than the 66 physicians using EHRsoft2’s product (5 years) and the 48 physicians using EHRsoft3’s product (6 years). This may be related to the fact that EHRsoft1 penetrated Quebec’s EHR market relatively recently when compared to the other two vendors. Furthermore, the medical practices that implemented EHRsoft1’s product had significantly more organizational experience with EHR systems (2 years on average) than those that implemented EHRsoft3’s product. Another noteworthy result is that all three EHR artefacts were characterized similarly in terms of ease of use, that is, all were perceived by their respective users to be equally difficult to use (2 on average, on a scale of 1–5), with regard to both patients and other care providers. This last finding clearly raises questions about the design quality of the EHR artefacts’ human–system interfaces, despite the fact that all three have been certified by Quebec’s health care authorities and Canada Health Infoway.
Characterization of the EHR artefact’s context and perceived ease of use.
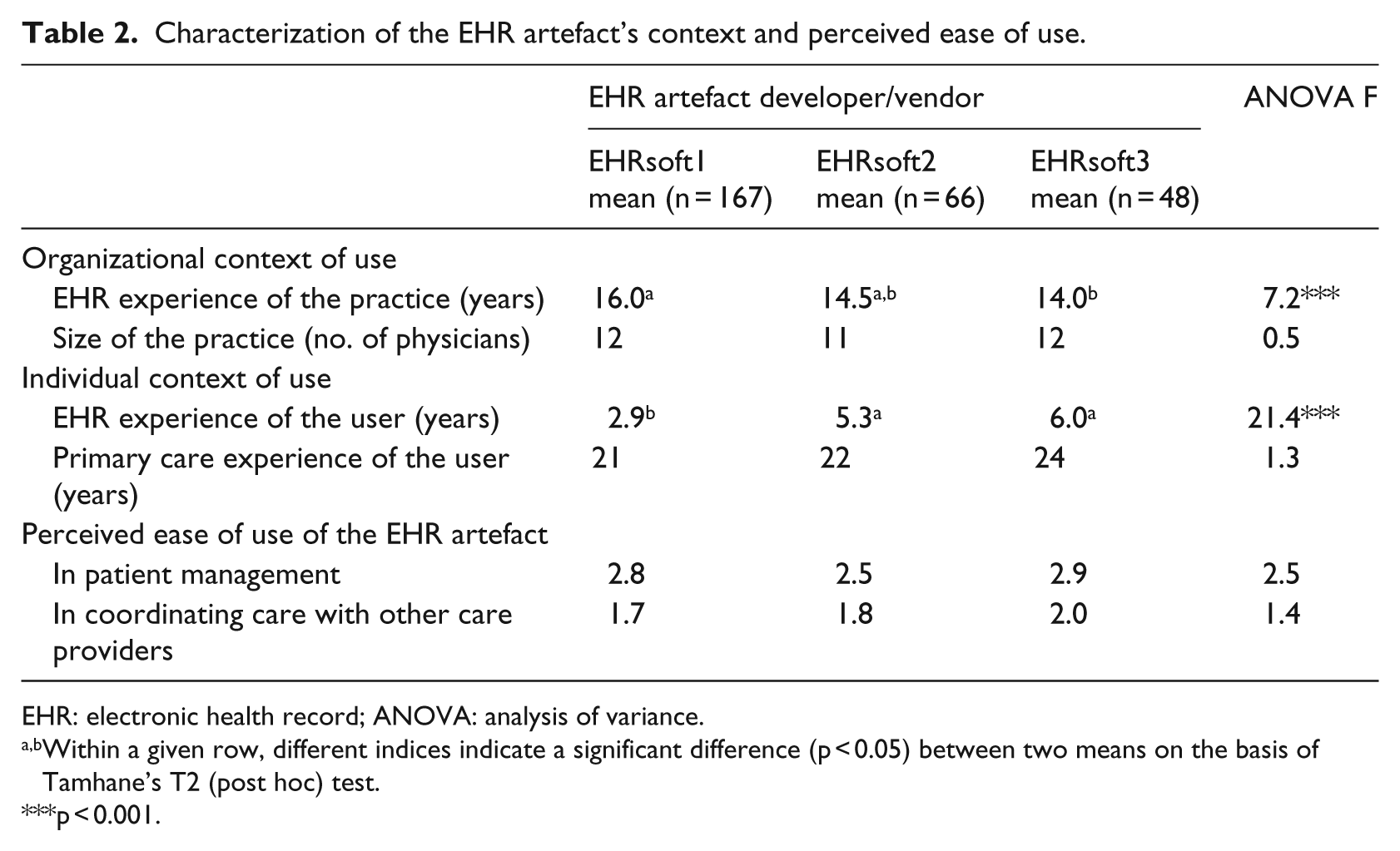
EHR: electronic health record; ANOVA: analysis of variance.
Within a given row, different indices indicate a significant difference (p < 0.05) between two means on the basis of Tamhane’s T2 (post hoc) test.
p < 0.001.
Table 3 presents the differences observed between the three EHR artefacts in terms of their functional capabilities, that is, the perceived availability of clinical, communication, and administrative functionalities, using our formative model of the EHR artefact as a benchmark. We first note that in the eyes of primary care physicians, EHRsoft1’s software product clearly dominates the other two solutions in terms of the availability of clinical functionalities. For instance, 66 per cent of EHRsoft2’s users reported that the ‘patient care management’ functionality is available in their EHR system, as opposed to 37 and 56 per cent of EHRsoft2’s and EHRsoft3’s users, respectively. All three artefacts are rather similar in terms of the perceived availability of communication functionalities, except for greater availability of the ‘communication with other institutions’ functionality in the EHRsoft1 software product (45%, vs 20% and 18% for the other two). Finally, EHRsoft3’s software product is found to be inferior in terms of the perceived availability of administrative functionalities and especially with regard to the ‘appointment scheduling/remote access’ functionality (65% vs 89% and 86% for the other two). Note that these differences remain significant when controlling for the primary care physician’s EHR experience and primary care experience, as well as for the EHR artefact’s perceived ease of use.
Differences between EHR artefacts with regard to their functional capabilities.
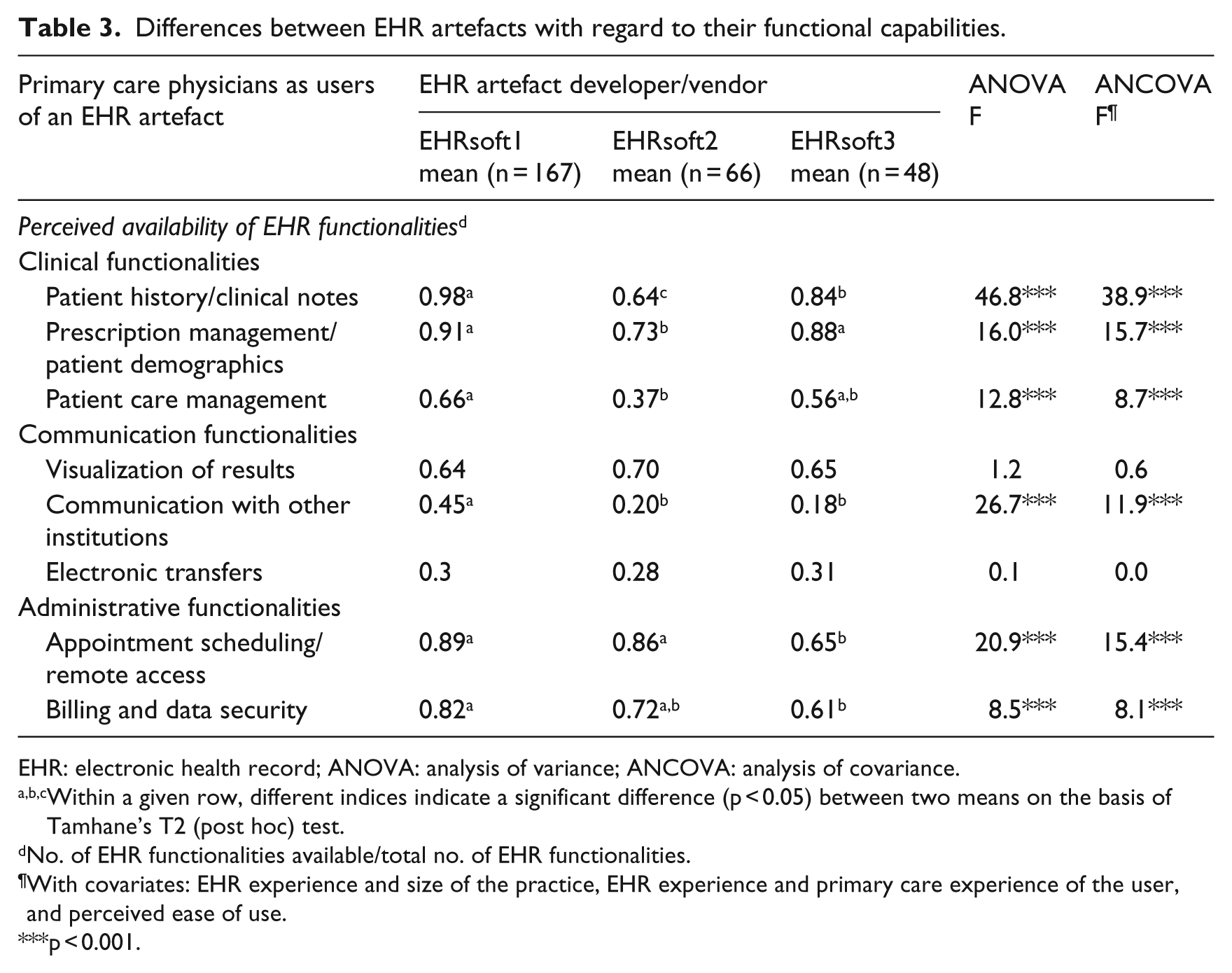
EHR: electronic health record; ANOVA: analysis of variance; ANCOVA: analysis of covariance.
Within a given row, different indices indicate a significant difference (p < 0.05) between two means on the basis of Tamhane’s T2 (post hoc) test.
No. of EHR functionalities available/total no. of EHR functionalities.
With covariates: EHR experience and size of the practice, EHR experience and primary care experience of the user, and perceived ease of use.
p < 0.001.
Next, we validated the preceding characterization of the EHR artefact from the user’s perspective, having ascertained that such a characterization is both relevant and useful to health IT theory and practice. To this end, we examined the relationship between the artefact’s design and its use in a primary care context. Our aim was to determine whether characterizing an EHR artefact from the user’s perspective can help us to predict and explain the nature and extent of its use and eventually assist in the design of EHR artefacts.
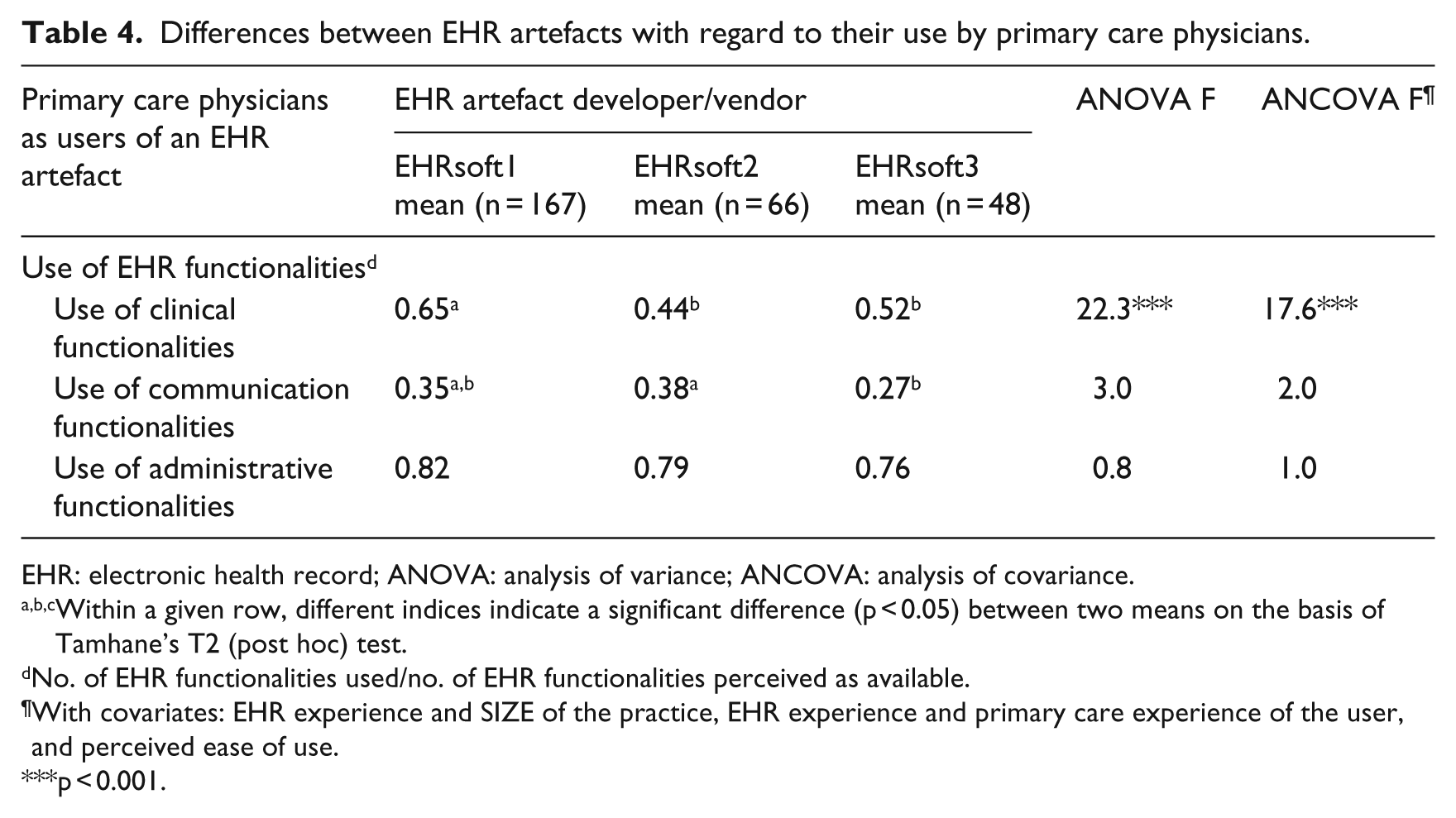
In response to our second research question, the nature of EHR use was defined through the three basic purposes for which it is assumed that primary care physicians use these systems: for clinical, communication, and administrative purposes. The extent of this use can range from none at all to full extended use of all available functionalities. The results presented in Table 4 clearly indicate that there are significant differences between the three EHR artefacts in terms of the extent of their use by physicians. More specifically, users of the EHR system developed by EHRsoft1 were found to use significantly more clinical functionalities than users of either the EHRsoft2 or the EHRsoft3 software products. For instance, physicians in the EHRsoft1 group make use of 65 per cent of the clinical functionalities they perceive to be available in their EHR system, as opposed to 44 per cent for the EHRsoft2 group. Moreover, physicians using EHRsoft2’s product use a greater number of communication functionalities than those in the EHRsoft3 group (38% vs 27% of the functionalities perceived as available). Once again these differences remain significant independent of the physicians’ EHR experience, primary care experience, and perceptions of the ease with which their system can be used.
Differences between EHR artefacts with regard to their use by primary care physicians.
EHR: electronic health record; ANOVA: analysis of variance; ANCOVA: analysis of covariance.
Within a given row, different indices indicate a significant difference (p < 0.05) between two means on the basis of Tamhane’s T2 (post hoc) test.
No. of EHR functionalities used/no. of EHR functionalities perceived as available.
With covariates: EHR experience and SIZE of the practice, EHR experience and primary care experience of the user, and perceived ease of use.
p < 0.001.
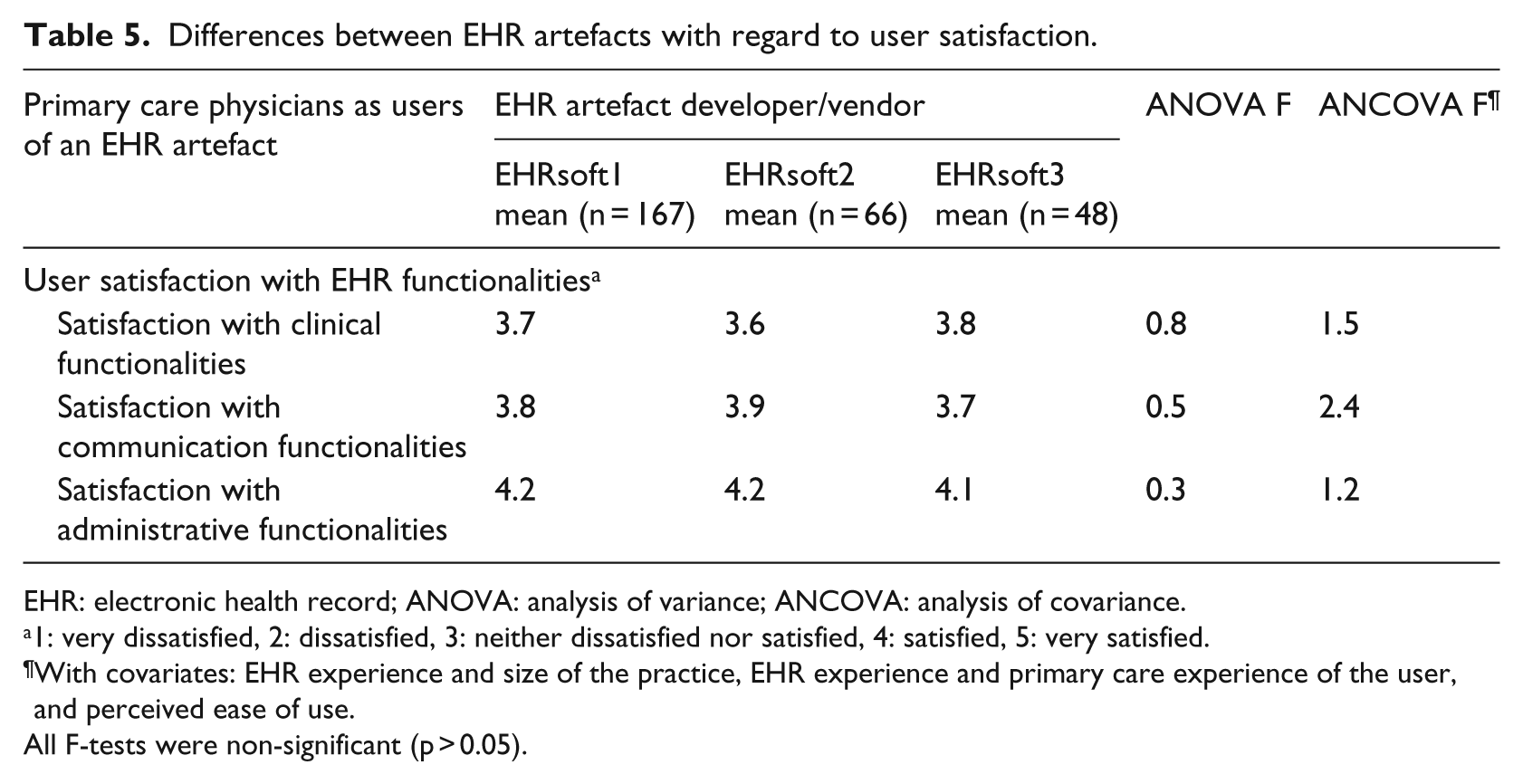
To further explore the differences identified above, the physicians’ satisfaction with their system’s clinical, communication, and administrative functionalities was compared among the three EHR artefacts. As shown in Table 5, no significant differences were found in this regard; users were equally satisfied, on average, with all three EHR software products. Considering that physicians using EHRsoft1’s product made more extensive use of their system’s clinical functionalities (compared to the other two groups) and that all respondents were equally satisfied with their EHR systems, we posit that more attention needs to be paid to the EHR artefact’s functional capability and physicians’ behaviours – rather than attitudes – towards EHR systems if clinical performance is to be enhanced by implementing this technology in primary care settings. 6
Differences between EHR artefacts with regard to user satisfaction.
EHR: electronic health record; ANOVA: analysis of variance; ANCOVA: analysis of covariance.
1: very dissatisfied, 2: dissatisfied, 3: neither dissatisfied nor satisfied, 4: satisfied, 5: very satisfied.
With covariates: EHR experience and size of the practice, EHR experience and primary care experience of the user, and perceived ease of use.
All F-tests were non-significant (p > 0.05).
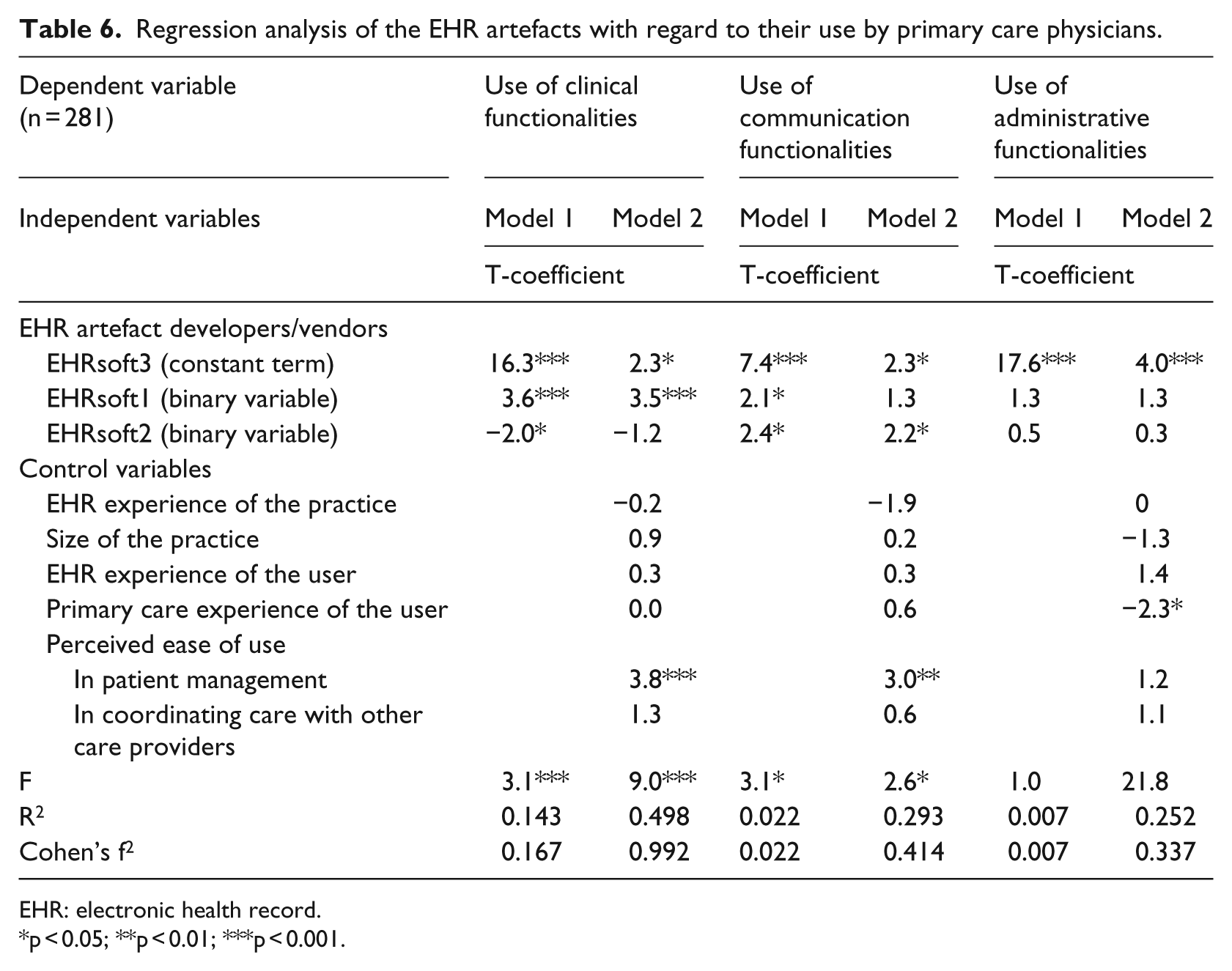
With regard to our third research question, the relationship between the EHR artefact as designed (by EHRsoft1, EHRsoft2, and EHRsoft3) and the EHR artefact as used (by primary care physicians) was ascertained through multiple regression analyses, as shown in Table 6. The independent variables were the EHR artefact group memberships, that is, two binary or dummy variables (1: yes, 0: no) indicating whether the physician was using EHRsoft1’s or EHRsoft2’s product, with EHRsoft3’s user group as a constant term (i.e. the base EHR artefact category against which the other two categories were assessed) in the regression equation. The dependent variables were the three indicators of EHR use: the extent to which clinical, communication, and administrative functionalities are utilized. Two regression models were tested for each dependent variable, the first (Model 1) included only the EHR artefact group membership variables, whereas the second (Model 2) also included the control variables.
Regression analysis of the EHR artefacts with regard to their use by primary care physicians.
EHR: electronic health record.
p < 0.05; **p < 0.01; ***p < 0.001.
The regression results for Model 1 show that EHRsoft1’s system is significantly associated with higher levels of clinical use by primary care physicians and that EHRsoft2’s system is significantly associated with higher levels of use of communication functionalities. Unsurprisingly, an EHR system’s ease of use is a significant predictor of clinical, communication, and administrative use when the control variables are factored into the regression equation (Model 2), increasing the percentage of explained variance from 14.3 to 49.8 per cent, from 2.2 to 29.3 per cent, and from 0.7 to 25.2 per cent, respectively. It is also important to note that the effect size of the EHR artefact when used by physicians is ‘medium’ in clinical terms (f2 = 0.167), ‘small’ in communication terms, and nonexistent in administrative terms. 39
In sum, these findings confirm the theoretical importance and practical relevance of characterizing the functional design of an EHR artefact in terms of both the different types of functionalities (administrative, communicational, clinical) and the different number of functionalities of each type that are made available to users. In such terms, the more comprehensive the commercial EHR solution provided by a vendor, the more extended will be its use by primary care physicians. More precisely, our results indicate that the functional design of an EHR artefact does matter in that it explains extended use in two ways. First and foremost, the greater availability of clinical functionalities explains why certain physicians use their EHR system more extensively because such functionalities would better support or ‘fit’ their main medical tasks than administrative or communicational functionalities. 24 Second, EHR systems that are more comprehensive within any of the three functionality categories are also used more extensively because physicians would perceive such systems to have more usefulness as more administrative, communicational, or clinical tasks would be supported. 6
Discussion
Starting with a tridimensional formative model of the EHR artefact, we developed an approach that characterizes this artefact in the context of its use by primary care physicians. In contrast to previous studies, our approach focuses on the use of the EHR in its material form (i.e. concrete EHR functionalities) rather than its conceptual form (i.e. collective idea found in a community discourse). 40 Thus, as its main contribution to the medical informatics literature, this study enriches our knowledge of the true nature and usage of EHR systems in primary care settings.
In terms of research implications, the conceptual approach adopted in this study expands the basis for comparing EHR artefacts in terms of their core capabilities, structuring this comparison process and rendering it more transparent. Furthermore, it allows for greater control of EHR artefact variables in relational analyses, including the influence of specific primary care contextual factors on the EHR artefact and its use, such that our approach can be combined with existing health IT research models designed to study IT artefacts in context by adapting and applying previously validated models focused on the ease of use, usefulness, and success of such artefacts. 38 Finally, by characterizing and documenting the EHR artefact from the physician’s perspective, researchers can avoid the conceptual disconnect that can occur when one attempts to link a theoretical artefact (the EHR as designed) to observed use (the EHR as used). 26
From a practical standpoint, our main goal was to determine whether characterizing an EHR artefact from the user’s perspective can help us to explain the nature and extent of its use, that is, the type (administrative vs communicational vs clinical) and number of EHR functionalities used by primary care physicians, and eventually assist in the design of such artefacts. For one thing, our findings reveal that all three EHR artefacts were perceived by their respective users to be rather difficult to use, despite the fact that all three have been certified by health care authorities. This clearly raises questions about the design quality of the EHR artefacts’ human–system interfaces and, hence, reinforces the role and importance of user involvement. 41 Furthermore, our study can guide the evaluation and improvement of existing EHR artefacts and serve in the development of benchmarks to guide physicians and other health care professionals as they select, deploy, and use such artefacts. If the development of an EHR system is to be consistent with its intended function, and if its usefulness is to be maintained in response to changing user requirements and usage contexts, EHR designers’ knowledge should be subordinated to users’ knowledge. Again, this implies that constant exchange between users and designers is critical for health IT artefacts such as EHRs, whose clinical value depends upon the quality of their fit with the tasks of physicians, nurses, and other professionals working in primary care settings.
Conclusion
This study revealed significant differences among three EHR artefacts with regard to their functional capabilities, that is, the provision of various clinical, communication, and administrative functionalities by their vendor. We were also able to observe that primary care physicians differed significantly in terms of the extent to which they made use of each functionality available in their EHR system. But most importantly, our results further confirm that the EHR artefact indeed matters to primary care physicians, as we found that the functional design characteristics of commercial EHR solutions, and especially their clinical functionalities, play a significant role in the extent to which physicians use EHRs in this context.
While the distinction between the ‘conceptual’ and the ‘material’ EHR artefact represents a key contribution of this study, we did not keep track of the actual functionalities that were available in each of the EHR solutions in use at the time of the survey. We therefore acknowledge that the lack of such a portrait represents a major limitation of our work. In this line of thought, we then recommend that future studies assess whether the perceived availability of EHR functionalities (by physicians) differs from the actual availability of these same functionalities (as embedded in the EHR software solutions). Future research should also help EHR vendors design systems that are aligned with the specific needs and requirements of primary care physicians. To this end, a classification framework is an indispensable tool for the study of EHR systems as well as the study of health IT in general. In response to calls made to adequately identify health IT artefacts in terms of their design, deployment, and use, a clear and precise characterization of EHR systems is even more important, given the great diversity of such systems brought about by the rapid changes in the IT and network infrastructures that enable them. Of particular interest for future research are the influence that can be exerted by EHR use, through feedback, and context of use, on the EHR artefact’s functional configuration (customization, emergence of new functionalities to preserve usefulness), that is, the process by which the artefact is assimilated by physicians, nurses, and other allied professionals.
Footnotes
Declaration of Conflicting Interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.