
Abstract
Obesity has commonly been addressed using a ‘one size fits all’ approach centred on a combination of diet and exercise. This has not succeeded in halting the obesity epidemic, as two-thirds of American adults are now obese or overweight. Practitioners are increasingly highlighting that one’s weight is shaped by myriad factors, suggesting that interventions should be tailored to the specific needs of individuals. Health games have potential to provide such tailored approach. However, they currently tend to focus on communicating and/or reinforcing knowledge, in order to suscitate learning in the participants. We argue that it would be equally, if not more valuable, that games learn from participants using recommender systems. This would allow treatments to be comprehensive, as games can deduce from the participants’ behaviour which factors seem to be most relevant to his or her weight and focus on them. We introduce a novel game architecture and discuss its implications on facilitating the self-management of obesity.
Introduction
Close to two-thirds of American adults are currently facing a reduced quality of life (QOL) as a result of being overweight or obese.1,2 The already significant associated health-care costs are expected to reach 860–960 billion US dollars by 2030 if the epidemic continues to progress. 3 This progress is a significant risk for two reasons. First, no interventions have resulted in significant and sustainable weight loss. 4 Second, these interventions may face an even harder situation since ‘the current economic crisis is likely to intensify the obesity epidemic [as we] have fewer options for care available and as healthier, high-cost foods become increasingly unaffordable’. 5 It is thus necessary to re-think the ways in which we have approached weight management.
The first important aspect to consider is that a wide array of factors participates in causing weight gain. This is typically oversimplified by viewing obesity as a mere matter of diet and exercise,6,7 despite a wealth of evidence indicating that diet and exercise are more symptoms than they are causes (cf. Giabbanelli et al. 8 and references therein). The second aspect is to acknowledge that there are tremendous individual differences in which factors cause weight gain.9,10 Generic interventions overlook this aspect and thus may only be effective for the few individuals who, by chance, match the ‘average’ profile assumed in the study design. 11
It is challenging for primary care practitioners to efficiently navigate the ‘maze of factors’ and find what matters most to their patient, due to the prohibitive amount of time required to perform a comprehensive assessment of the large number of factors, 12 and sometimes a lack of familiarity with such factors. 13 This situation fuels the growth of self-management, where individuals decide what matters to them, design an action plan, measure the results of the actions, and update what now matters. This can favourably contribute to behaviour change. For example, theories of self-regulation 14 highlight the benefits of empowering individuals in making decisions about their health.
A number of online tools have supported individuals in the use of self-management for conditions such as obesity15–17 or alcohol abuse. 18 However, such tools do not currently support all these key aspects: (1) finding what factors matter, (2) providing evidence-based actions and/or (3) facilitating the involvement of a practitioner in collaboratively setting up actions, and finally (4) tracking progress. Designing a solution that satisfies all these requirements is a wicked problem. 19
Over half of American adults play video games, 20 which makes them an interesting vehicle to promote self-management in health. An increasing number of health games has been developed, with a focus on improving knowledge and intrinsic motivation. While this led to some noticeable successes, 21 it only satisfied some of the four requirements aforementioned. In this article, we propose to satisfy all requirements via a framework that innovatively combines games and recommender systems. This supports a cycle of self-management which starts with factors selected by the participant, rather than the current approach in which games decide for the participant.
Contributions of this article
The principal contributions of this work can be summarized as follows:
- We examine the adequacy of recent health games in supporting the self-management of obesity.
- We introduce a novel game framework that reverses the direction of learning used in health games.
- We discuss the technical details of the framework and how it empowers patients in managing their weight.
Designing health games
What are health games?
McGonigal 22 has suggested that games have four defining traits: a goal that players want to achieve, rules that guide the ways in which the goal can be attained, a feedback system that motivates players in reaching a goal that seems achievable, and voluntary participation as players accept the three elements aforementioned. These traits are found in definitions proposed by other scholars: Lieberman’s 23 definition includes goals and rules, while Caillois’ 24 definition includes rules and voluntary participation. We use the definition of McGonigal as it explicitly highlights the need for feedback, which will be central for the themes discussed here. Furthermore, other definitions impose restrictions that do not apply to our context. First, self-management may have to be ongoing, counter to Lieberman’s inclusion of a defined ending. Second, Caillois separates the virtual worlds created by games from the ‘real-world’, whereas mixed reality can be used in modern games (e.g. using biosensors while playing 25 ) and health games aim at changing participants rather than their avatars (e.g. what patients learned about nutrition in the ‘virtual world’ can change food purchases in the ‘real-world’).
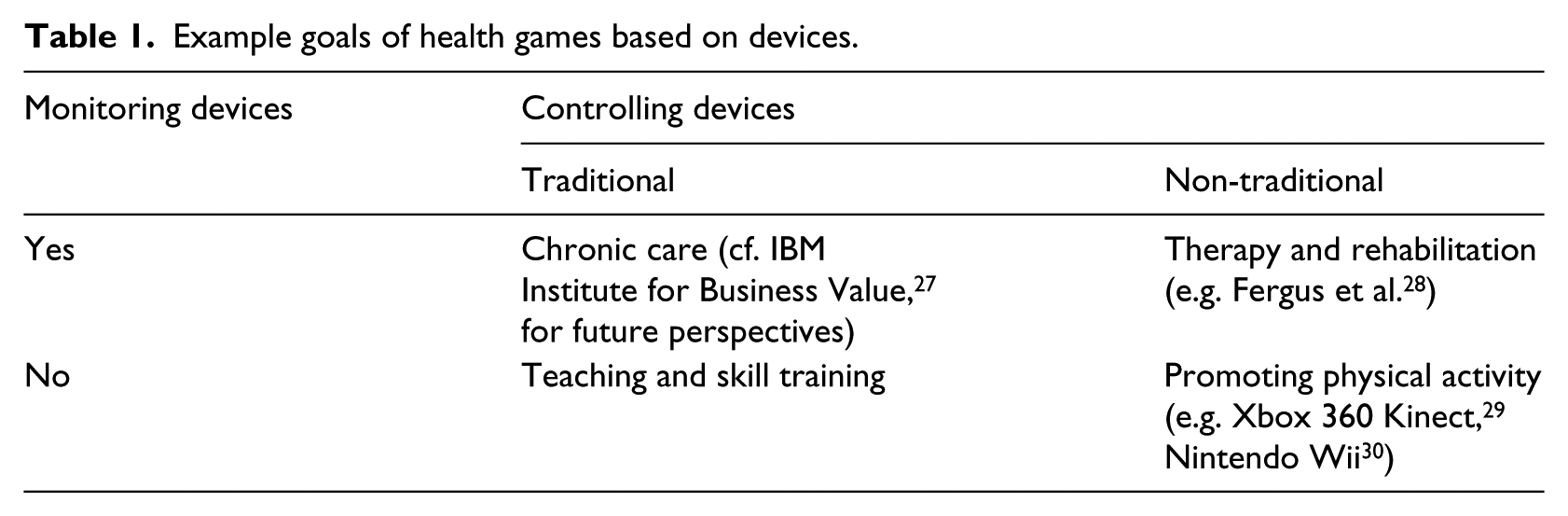
In health games, the game improves a dimension of health, such as physical, emotional, or social. 26 The objectives of health games are strongly linked as to whether monitoring devices (e.g. sensors) are required, and whether controlling devices are traditional (e.g. keyboard, mouse) or non-traditional (e.g. controlling the game via the body). Using these two binary variables results in four different objectives (Table 1). In this article, we focus on health games that use traditional controllers and do not require monitoring devices, which from here on we will refer to as ‘games’.
Example goals of health games based on devices.
An emphasis on information management
Games have predominantly approached self-management as a matter of information management. In other words, games are built to teach players how to carry on tasks that have been deemed important at the design stage. Two elements are key to the teaching part. First, the game prompts individuals to rehearse and repeat a behaviour multiple times, which is part of the theories of self-regulation. 14 Second, games provide a direct feedback, which is also known to be important for behaviour change as it rewards players within a short time interval for performing the desired behaviour. 31 These two elements will be illustrated in health games as follows.
In the example of diabetes self-management, the desired learning outcome is to maintain appropriate blood sugar levels by balancing (the sugars in) food and insulin. The strategy game Power Defense teaches balancing skills by asking the player to manage a power station, where the energy of the station stands for blood sugar level. 32 Waves of excess energy (standing for food) must be fought repeatedly using defense towers (representing insulin), and the ‘battle’ provides immediate feedback as to whether the appropriate balance was in place. In the case of obesity (which can lead to diabetes type II), the main learning outcomes are commonly to improve knowledge regarding nutrition and physical activity. A variety of nutrition games have been developed, with companies such as Nourish Interactive offering more than 20 games for children using a wide variety of genres (e.g. puzzles, action, arcade). Games have also been developed to address nutrition and physical activity jointly, such as the adventure game Escape from Diab where the player and virtual friends are trapped in a nightmarish kingdom in which social control is exerted by refusing exercise to the population and feeding it unhealthy food exclusively. 33 Thus, the player’s escape depends on his or her performance in tasks such as repeatedly differentiating healthy and unhealthy foods.
Successes and challenges
These games exemplify that the development has focused on delivering health-related information. 34 The actions learned or reinforced through larger games are often evidence based, as the design stage involves interdisciplinary teams using health promotion theories and models. 35 Games less commonly contribute to building a dialogue between participants and health practitioners. For example, in the ETIOBE system, the game is part of a Home Support System that serves as a vehicle for therapists to deliver tasks to their patients. 36 This direction is reversed in the game Time after time, which enables participants with localized prostate cancer to assess the expected impact of treatments’ side effects on their preferred QOL. 37 This assessment can later be used in consultations to clarify side effects or reduce the feeling of being overwhelmed by new information. In order to move the field forward, we suggest to capitalize on successes in communication and evidence-based recommendations, and to address the two challenges highlighted in the remainder of the section.
Research rarely examines whether health games result in sustained behaviour change. For example, the impact of the diabetes game Balance 38 and the exercise/nutrition Fitter Critters 39 was evaluated by administering questionnaires once, after having played. Repeatedly assessing the participants’ behaviour can be difficult since games developed for research are not funded to be marketed to the public, and thus often cease to be available upon completion of the research project. 40 However, repeated assessments would be valuable to strengthen research evidence via longitudinal studies, and they would also benefit players. Indeed, a repeated assessment can be seen as self-monitoring, and the mere act of measuring can already result in behaviour change. 41
This was confirmed by research showing that interventions with a single assessment were less effective in terms of long-term maintenance compared to interventions with repeated assessment. 42 The theories of self-regulation consider that monitoring must be of specific behaviour (e.g. food behaviour rather than weight) and that data should not only be collected but also interpreted and used. 14 Consequently, games should be consistently equipped with tracking abilities that allow for progress to be monitored at multiple points in time and use this to further support behaviour change.
Furthermore, most games focus on a handful of aspects, such as diet and exercise. However, a chronic condition such as obesity and its later development into diabetes is affected by a wide array of factors that interact in complex ways. Theories from health behaviour change suggest that, in the case of complex conditions, finding factors that are relevant to the individual is key to success. For example, the reasoned action approach provides support for the expectancy-value model of attitudes. 43 In this theory, a person’s attitude towards a given behaviour depends on the subject’s beliefs regarding this behaviour and whether these beliefs are perceived as being personally relevant. This theory first elicitates beliefs about the behaviour, and then models attitude as a multiplicative function of belief strength and attribute evaluation (i.e. relevance). This is further supported by observing that tailored interventions that identify what matters to a participant are more effective than generic interventions. 42 Therefore, the key design question is how the game will support finding relevant factors, rather than which factors should be selected beforehand.
Mindbloom Life Game’s support to find relevant factors among a wide array of choices stands in sharp contrast to the narrow possibilities of most games. In this game, the player is in charge of a tree where each leaf corresponds to one dimension of health (Figure 1(a)). The tree is grown by taking actions to improve a dimension (Figure 1(c)), or by finding ‘inspiration’ (i.e. motivation and goal-setting), for example, by browsing through a set of images and quotes (Figure 1(b)). The game also provides tracking capabilities (e.g. journal, calendar) and accomplishments can be shared with friends. However, this game faces a new issue: the number of possible factors offered to the user can be overwhelming, as one could have to be browsing a large number of irrelevant factors in order to pick only a few. Thus, the challenge is to find the balance between missing the player’s interests by offering too few factors and overwhelming the player by having too many factors. The game Time after time faces the same challenge: participants reported a need for personalization, but adequately describing personal life situations and lifestyle preferences would lead to an overwhelming number of questions, thus defeating the focused purpose of the game. 37 The solution to this challenge lies in using a technology designed for narrowing down choices based on user profile: recommender systems.
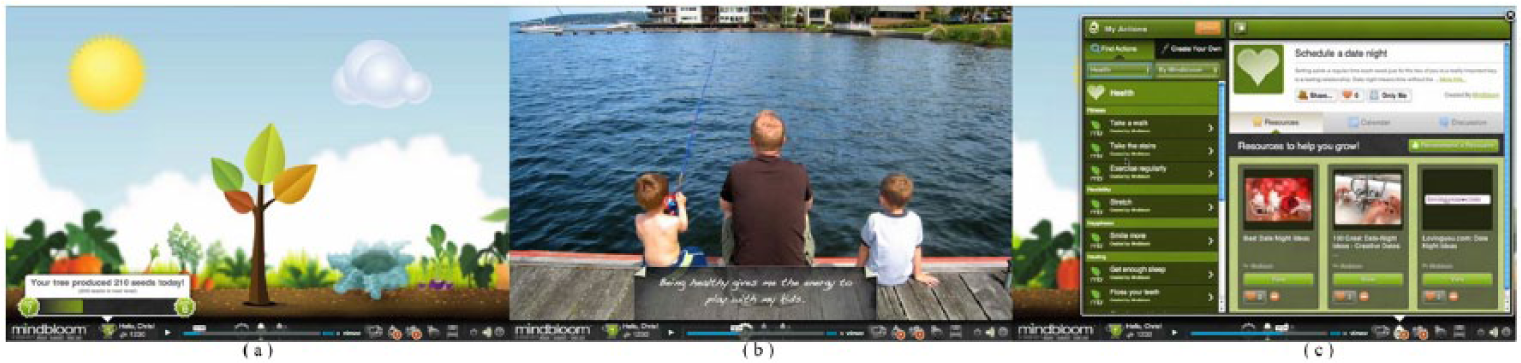
The central activity in Mindbloom is (a) to grow a healthy tree (b) by clarifying motivations (c) and/or taking actions. Images are the sole intellectual property of Mindbloom.
From games that teach to games that learn
Which feedbacks do we need in a game?
In the previous section, we identified four features that should be part of the design of games: (1) finding what factors matter, (2) providing evidence-based actions and/or (3) facilitating the involvement of a practitioner in collaboratively setting up actions, and finally (4) tracking progress. The last three features have been addressed in different games, and thus the effort is about combining existing design practices. However, the first feature is the key step in what we envision as a paradigm shift. Indeed, finding relevant factors means that the objective is not to reinforce the accomplishment of set goals by the player, but to support the player in setting the goals. According to goal-setting theory, working on goal-directed behaviours ‘leads to better performance because people with goals exert themselves to a greater extent, persevere in their tasks, concentrate more, and if necessary, develop strategies for carrying out the behaviour’. This improved performance is further supported when the player chooses the goals (which contributes to a sense of commitment) and when goals are within the player’s skill level. 44
Current games focus on delivering information and have set goals for players (Figure 2(a)), such as increasing the player’s knowledge about serving sizes. Such games often provide feedback on what players did (i.e. outcome feedback) rather than how or why they did it (i.e. process feedback). This may be partly explained by the historical emphasis on outcome feedback in management research. 45 An example of outcome feedback can be found in the framework for an adaptive game system proposed by Charles et al.,46,47 for whom the feedback is on performances. However, this approach faces two shortcomings. First, research has showed that traditional media such as pamphlets and websites can be more effective at delivering information than games. 48 Second, health behaviours are complex, and research on human performance suggests that outcome feedback have little to no benefit in complex tasks; 45 such feedback may even decrease performance by directing the player’s attention to goals that are irrelevant to the condition that the player seeks to manage. 49
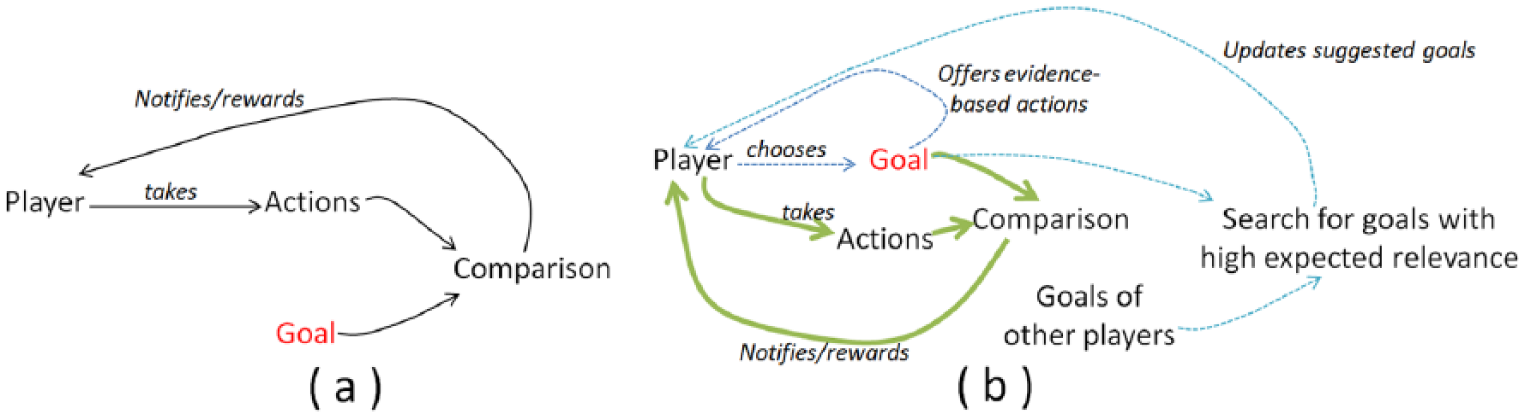
(a) Games that teach to set goals for players and (b) games that learn from players and support them in setting goals.
These two issues could be addressed by moving from games that teach to games that learn from players and support them in searching for goals. Instead of being rewarded to repeatedly accomplish set goals (Figure 2(a)), rewards can be provided to support players in setting new goals after comparison with an initial goal (Figure 2(b), bold arrows) such that higher goals are automatically unlocked when the player succeeds, whereas goals that can be deemed more achievable are suggested when the player struggles (Figure 2(b), dotted arrows). Giving players a feedback on their strategy (i.e. process feedback), for example through rewards, can affect performance positively for complex tasks because the direction role of process feedback better supports task strategy than outcome feedback. 45 In particular, Deck 50 has highlighted the potential of moving from outcome feedback to process feedback in the self-management of obesity. Furthermore, process feedbacks are computationally intensive and games can be utilized to implement them.
How to support process feedbacks?
A number of techniques have been used to support learning in games. A review of the constraints imposed by games on learning techniques, together with solutions such as neural networks, can be found in Galway et al. 51 Additional information on the broader field of personalization in e-Health can be found in a recent special issue of User Modeling and User-Adapted Interaction. 52 As we have suggested before, 53 recommender systems have potential in finding relevant factors, especially when there is a large number of potential factors. A recommender system is a software that uses an individual’s known behaviour on past activities to infer the interest in future activities. 54 An example of application is in e-Commerce, where a customer’s past purchases are used to recommend items that are most relevant for future purchases.
Practically, recommender systems create a database of the behaviour of previous participants. Then, they differ on how new participants are handled (i.e. cold start problem), and how the database is used to infer future behaviour. The former can be approached in two different ways. First, a participant may not have explicitly stated interests yet, but may have viewed web pages or undertaken activities previously. This implicit information can be collected using either the history of the participant’s web browser (i.e. client side) or that of the server (i.e. server side), and it can be used to build user profiles. Second, we might assume no prior information and explicitly ask participants about what interests them. Examples of both strategies can be found in Zanker and Jessenitschenig. 55 While implicit information may have value in understanding what factors are important to one’s weight management, that would complement rather than replace explicit information. Explicit information could be elicited via advisory dialogues that welcome and guide new participants, as a primary care practitioner who meets a patient for the first time. The key difference is the system’s ability to build on its database to navigate the maze of factors linked to one’s weight, which is challenging for practitioners. 12
For a given participant, similar ones will be found using the database. This could be achieved by performing correlations between the target participant’s (few) answers and the answers of all other participants (e.g. using Pearson’s correlation coefficient or the often more efficient cosine similarity). However, comparing with all participants is a very time-consuming operation, which is impractical for large e-commerce websites. It may lead to issues on both client- and server-side, with participants waiting a significant amount of time while the server is overwhelmed. Techniques have thus been developed to ensure real-time answers and modest hardware requirements. Intuitively, these techniques spend time organizing the data (e.g. when there is a low load on the server) so that recommendations can be quickly performed (e.g. at peak time). When using the system, the participant’s expected interest in a given factor of weight management is estimated using his interest in other factors and the similarity of these factors to the one we want to predict. Then, the most relevant factors can be selected. The overall operation (Figure 3) is very efficient and used by websites such as Amazon. 54
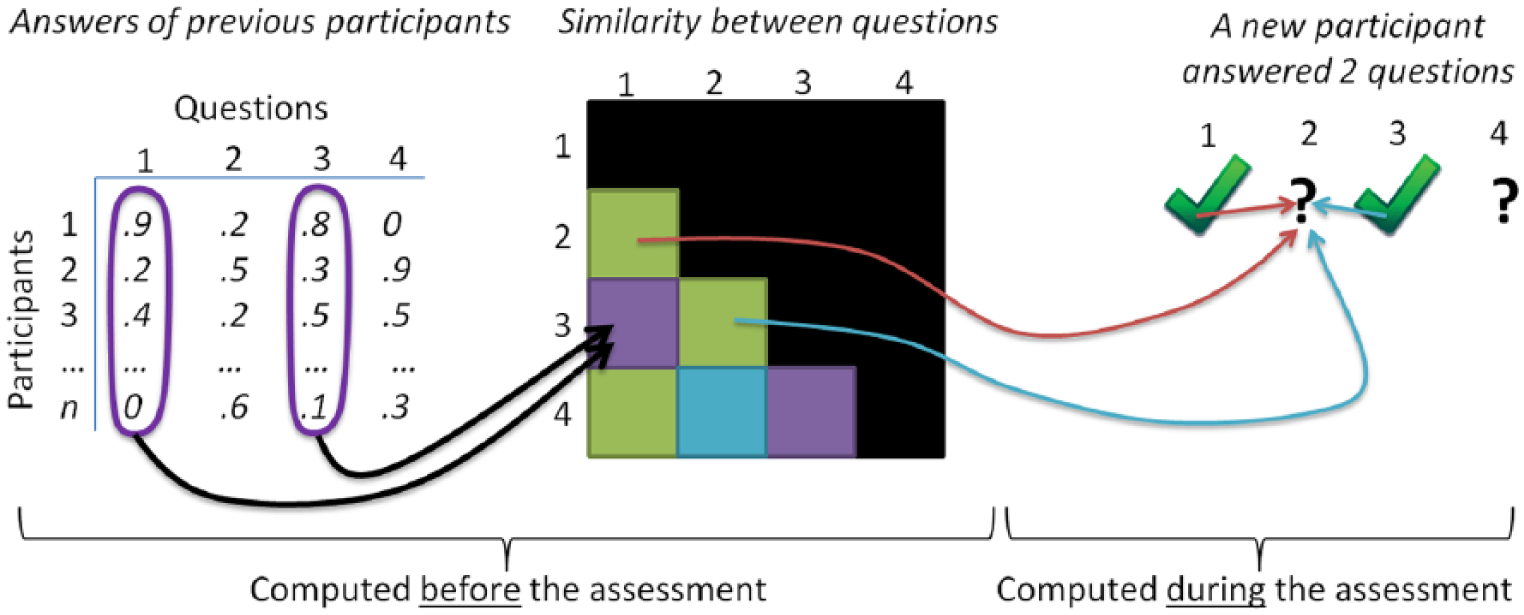
Key steps in an item-based nearest-neighbour recommendation system.
The broader system: satisfying all four requirements
We identified a change from outcome feedback to process feedback as the key paradigm shift. Technical solutions were exposed above. In this section, we summarize the architecture of the overall system so that it can also satisfy the three other requirements set in section ‘Introduction’: facilitating communication with practitioners, suggesting evidence-based actions, and tracking progress. The intermediate-level architecture presented in Giabbanelli et al. 53 (Figure 4) addresses these requirements as follows. First, when factors relevant to the weight management of the player are identified by the recommender system, a report should also be generated and passed on to the practitioner associated with that participant (if any). This allows practitioners to start their next discussion with a patient based on what is important, without having to perform the initial assessment. Second, the recommender system can be matched with a database of evidence-based advice. For example, if players suggest that stress tends to be very present in their lives and that they cope with it by eating energy-dense food, then alternative coping strategies might be introduced. This exemplifies that the goal should not be to tell individuals to simply eat less, but to find the drivers on which to intervene. Finally, activities in the game can contribute to monitoring progress and adherence, which can be for the sole usage of the player or shared with a practitioner to further support a rich conversation.
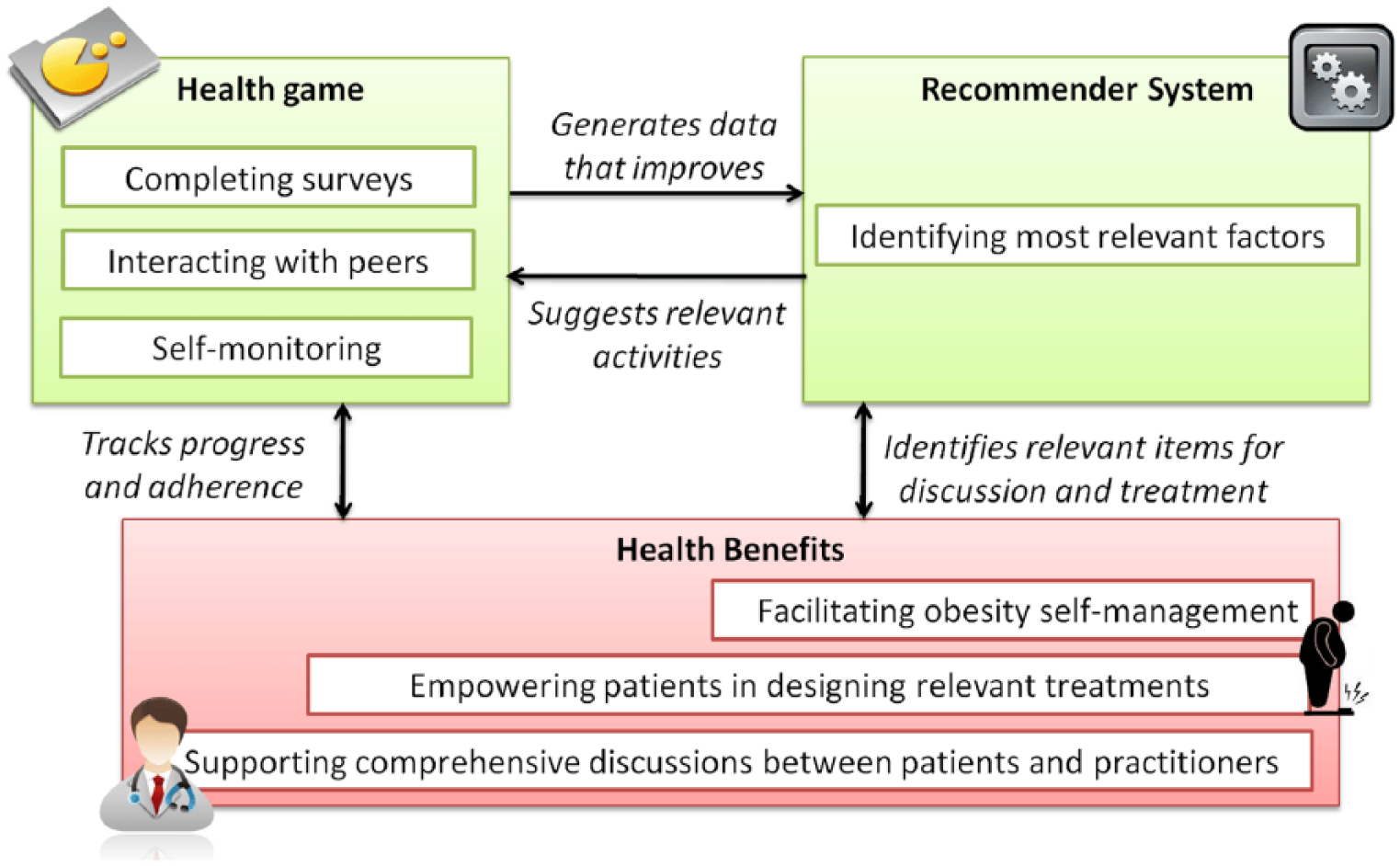
Intermediate-level architecture.
This architecture includes a number of feedbacks. The central feedback between game activities and the recommender system is based on the design introduced in Figure 2. The feedback between the recommender system and practitioners facilitates the patient–practitioner interaction, which is further supported by a feedback between a practitioner and the patient’s progress report. The time taken by a feedback is known as the delay. Delays are important when managing a system, especially in the case of the complexity inherent to weight management because they can create oscillations which may run out of control. 50 Figure 5 summarizes the feedbacks together with the time scale. This reminds users of the system that, in accordance with recommended practices for weight management, changes in a participant’s weight should be gradual (i.e. slow rather than drastic). It also highlights that even if recommendations can be computed swiftly, their consequences on user behaviour will take additional time.
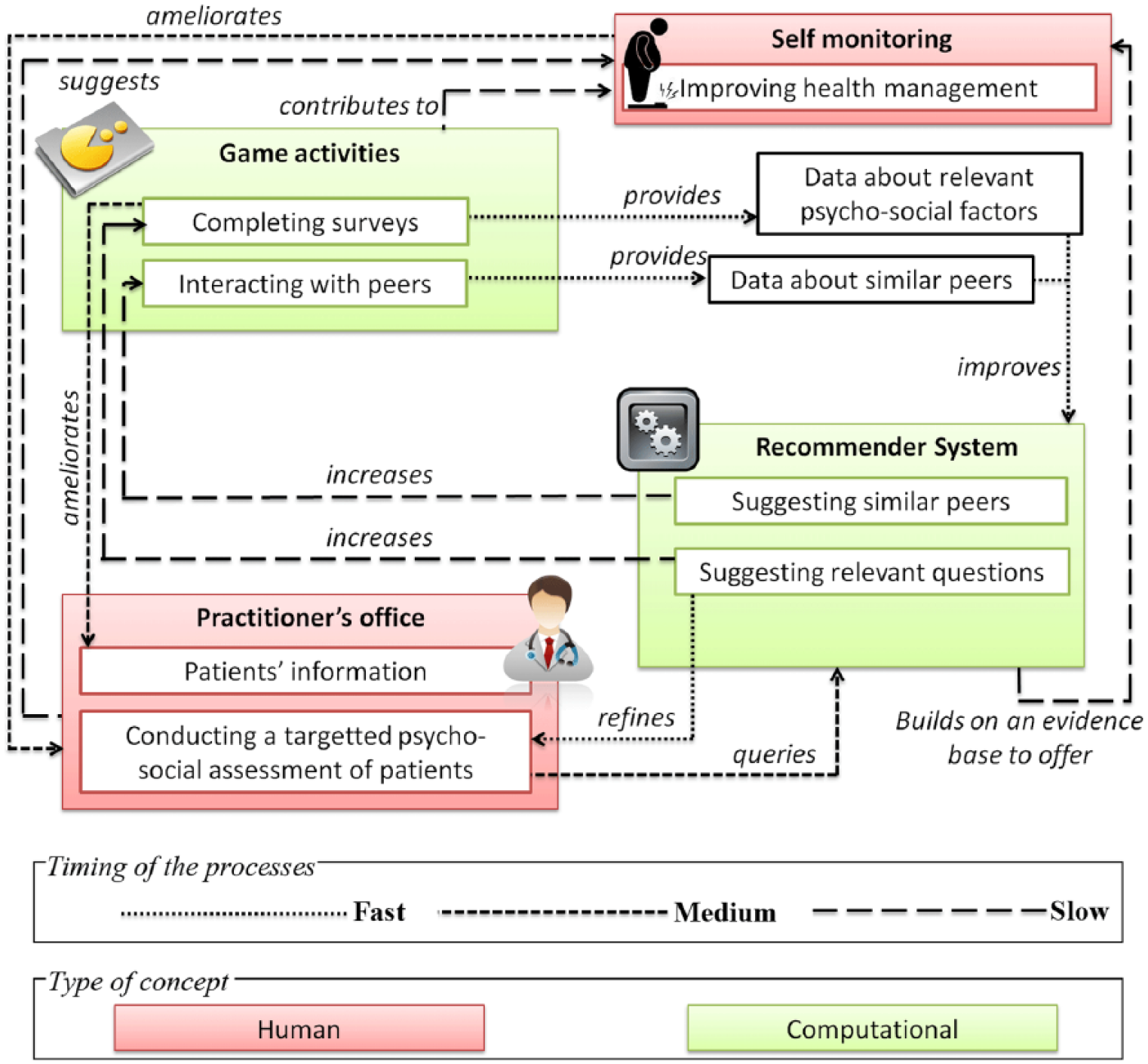
Detailed architecture.
Discussion
Obesity is a prevalent condition in North America, associated with a reduced QOL for individuals and health-care costs in billions of dollars for society. Generic interventions do not result in sustained weight loss for most participants, 56 suggesting that novel solutions are needed. The growing area of self-management offers potential for interventions that are comprehensive as well as cost-effective. In this article, we examined how health games have been currently used to support self-management. In particular, we reviewed how they currently support four mechanisms key to successful weight management: finding what matters to individuals (rather than imposing predetermined goals), suggesting evidence-based actions, facilitating meaningful conversations with practitioners, and tracking progress. As no game currently satisfies all four requirements, we proposed a new architecture via a focus on the design of interactions (i.e. feedbacks). Given that the development of health games for obesity is still in its infancy, 57 such improvements in architectures are now needed to move the field forward. Technical solutions to implement this design were highlighted, with an emphasis on the role of recommender systems. While providing highly customized interventions is normally a substantial problem that leads to increased costs, 58 our use of recommender system makes it possible to automatically deliver a high degree of customization in a scalable and cost-efficient manner.
Computerized interactions can face the need to impart a ‘human touch’. 59 When this is the case, practitioners may have to be involved, which limits the cost-effectiveness and scalability of the intervention. This is addressed in two ways by our architecture. First, recommender systems support participants in navigating through a large content so they can focus on what matters most to them. This can contribute to a high perceived personal relevance. Second, the feedback from the recommender system should be delivered in a way that makes the reasoning transparent (cf. Explanations in recommender systems in Jannach et al. 54 ) and personal. For example, a participant would not be told ‘You should now complete this activity’ but rather ‘John, most of those who share your history of dieting found this activity to be very useful’. Personalization together with a high perceived personal relevance can be very persuasive, 60 thereby making the intervention at least as effective via technology as in person. 49
Smartphones can also be used to increase the effectiveness of the games by embedding them into the player’s routine. Indeed, smartphone apps are increasingly used to develop augmented reality games where the player’s actions in the real-world impact the outcome of the game. This creates a new use for monitoring devices to support teaching and skill training, instead of their historical use in the clinical setting (Table 1). For example, the camera is used in Time to eat where virtual pets remind adolescents to eat healthy meal and change mood based on pictures of the meals. 61 Similarly, the phone’s ability to act as a pedometer is leveraged in Fish’n’steps which promotes physical activity by using the player’s daily food step count to impact a virtual pet. 62 Consequently, smartphones can contribute to decrease the barrier to self-monitoring, thereby reinforcing the potential of health games to improving health management (Figure 5).
Our architecture fits into the paradigm of self-management by allowing practitioners to learn about their patients 19 from what they do in the game. However, the ongoing implementation of our architecture in collaboration with IgnitePlay has pointed out the need for further studies on the communication between practitioners and patients in health games. On one hand, we know that efficient communication can contribute to improved outcomes 63 and satisfaction, 64 and that health games can facilitate communication as was demonstrated in the case of Time after time. 37 On the other hand, we do not know how to best use health games to support efficient communication. It is thus necessary to create recommendations about what a game should report on and how. For example, practitioners may suggest that automatic reports should be delivered biweekly rather than weekly or monthly, as the former is too short to reflect on one’s behaviour change while the later may be too long. Similarly, players know that the games may use all available information on their behaviour to infer how to best support them, but may want to select what information they feel most comfortable in disclosing to their practitioner. Qualitative studies could play a valuable role by giving a voice to both practitioners and individuals in need of support for weight management. Further studies could involve interviews using interpretive description, which would allow us to extract patterns in an iterative way (i.e. by starting with relatively open-ended question and then narrowing the object of study) in order to understand how to impact practices regarding the design of health games. 65
Ongoing evaluation and user testing will be necessary to refine this architecture. Three aspects should be monitored. First, we should evaluate adherence by applying metrics from Internet-based interventions, which focus on ‘how frequently the tool is used, for what period of time, by which subgroups, and for what reason’. 66 Second, we should examine the impact of this architecture on cognitions, that is, the reaction of participants to their interaction with the health game. This includes attention and persuasion, 58 which can be assessed, for example, by asking participants whether they feel that activities are personally recommended to them, and manipulating argument quality as in Dijkstra and Ballast. 60 This manipulation checks the extent to which participants see the distinction between strong and weak arguments to engage in an activity, under the assumption that arguments are examined carefully by participants when they feel that information is personally relevant. 60 Finally, evaluating the impact of our architecture on behaviour change can be performed by measuring behaviour change and how it altered the underlying health problem measured by QOL. Measuring both is important given that the delay between behaviour change and its impact on QOL can be long in the case of chronic diseases. Specifically, the classic evaluation process of games using QOL measurements 67 can be adapted to one that relies on health-related quality of life (HRQL). 68 Conducting this evaluation will be key to situate our architecture among other solutions in terms of cost-effectiveness, particularly compared to Internet-based interventions that may increase the frequency of personal contact. 69
Conclusion
A novel game architecture was presented to support the self-management of chronic conditions such as obesity, by shifting from the traditional approach aiming at increasing players’ knowledge of a few select factors to a comprehensive approach that supports players in the design of their own well-being.
Footnotes
Acknowledgements
The authors would like to thank Dr Thecla Schiphorst for providing thorough feedback on this study. P.J.B. is indebted to Dr Diane Finegood for sharing her interests in studying the heterogeneity of obesity and to Penny Deck for her insightful suggestions. Facilities were provided by the Modelling of Complex Social Systems (MoCSSy) program at Simon Fraser University.
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.