
Abstract
Patient information is one aspect of meeting the needs of health service users; it is meant to empower patients and their carers in making informed decisions and managing their health needs. Mary Dixon-Woods described two types of discourse in patient education: the first is more concerned with making patients comply with their doctors orders and the second is about empowering patients and rejecting direction. This article looks at the aims of the two and shows that neither is capable of supporting highly successful best practice within medicine. Instead, a hybrid set of strategic aims are proposed for patient education created by merging the two discourses in the same way that John Dewey merged the child-centred and child-led schools of thought in education. These hybrid strategic aims for patient education are then used to develop requirements for an information system to support patient education, using a mixture of system centric and user centric approaches.
Introduction
In 2001, an article by Mary Dixon-Woods on patient information leaflets highlighted a strong challenge to traditional patient education. 1 It described a patient education discourse characterising patients as incompetent and passive, and invoking a mechanistic model of communication concerned only with how printed information might affect biomedically important outcomes. This was contrasted with the new and better discourse of using information to empower patients.
Dixon-Woods’ article has been very well received in information science in that it mirrors the debate between system-centred and user-centred information behaviours, 2 and supports the move towards user-centred models for the design of computer systems to support patient information needs.
Aims of this study
This article aims to demonstrate that neither discourse highlighted by Dixon-Woods is suitable for developing a successful patient education intervention that will meet the needs of health service users. This will be done by taking the aims of two very successful community-based programmes and contrasting them with the aims of the patient education and patient empowerment discourses described by Dixon-Woods. This article will then make an argument for a hybrid discourse based, in no small part, upon the arguments used by John Dewey against the child-led excesses of the progressive education movement. 3 This middle course will be used to describe the requirements for a patient education information system to solve challenges created by the merging of these two discourses.
The final aim of this article is to explain that information provision is not education and that while supporting patients who are seeking information is an important aim it is not and cannot be a replacement for education.
Historical context
Patient education, choice and empowerment are popular themes in the media currently, with the suggestion that the era of ‘Doctor knows best’ is over, 4 and that patients will benefit from being better educated and more active in the choice of their treatments. The problem with this suggestion is that patients actively involved with their treatment are not automatically benefited, with some studies showing active groups being harmed compared with passive groups. 5 There is also some evidence that just increasing the information level of a patient can reduce their compliance with health protecting behaviour. 6 At the very least, patient information delivered in an unbiased way often has no effect on patients making informed choices. 7 A closer look at these studies seems to show patients being unhappy with available treatments/tests and either rejecting them or being poorly compliant with them based upon their personal analysis of the information. The contrast to these disengaged or engaged but challenging attitudes to the doctor–patient relationship is where patients are sharing responsibility with their doctor, learning, and effectively and responsibly taking part in their treatment. These (modern) patients are benefited above passive patients. 8 Enabling the patient to use information to make good, informed choices is within the domain of patient education.
Interestingly, this convergence between doctor and patient roles owes a great deal to our current society and education system. In the western world the changes to the way that society views patient education have mirrored the changes in the way society has viewed educational aims. Plato first argued that in an ideal state the rulers (doctors) would need a much more thorough education than those ruled (the patients). 9 With the industrial revolution this moved to the masses being sufficiently well educated to be able to be productive without rebelling against the differently educated ruling classes who would tell them what to do (public health education where doctor knows best). Finally, the modern idea that all are educated equally and are served by the democratically elected rulers would be the modern, patient-centric approach, with patients using the information and skills that they have been given to choose doctors/treatments, and make good choices and improve their health.
In the early 1900s there was a rebellion in education called the ‘progressive movement’, a rebellion that is still being integrated into education to this day. 3 This rebellion led to the benefits of more child-centred education (building the learning experience around the child’s interests, ability level and ways of learning), the folly of a purely child-led education (only teaching a child what they want to learn) and the compromise from this rebellion can be seen by mainstream adoption of the idea that although there are population level aims to education, each child is an individual and that education should be individually targeted for that child within the constraints of those population-based aims.
The paper by Mary Dixon-Woods highlights another such rebellion, no less critical and rejecting of the past than the early progressive movement, but this time rejecting a medical or behavioural change agenda for patient information and replacing it with a purely patient-led agenda.
What is the aim of patient education
Aims of real world education
Modern patient education faces those problems found by the educational establishment, such as how to educate a diverse population, how to include those with special educational needs, disengagement by sections of the population, political interference, as well as differing aims of those being educated from those of the educators. As such, it should be expected that patient education would develop along similar lines to population-based education.
When faced with the question ‘What is the aim of education?’ a good answer would be that of Dewey: ‘Education as such has no aims. Only persons, parents and teachers, etc., have aims, not an abstract idea like education.’. 10 This answer can also be applied to patient education in that there can be no intrinsic aim to patient education other than the aims of those providing and receiving the education. As there is no intrinsic aim to education itself, any educational intervention must therefore meet the aims of those providing the education along with the aims of those receiving it.
Aims of educational discourses according to Dixon-Woods
Table 1 summarises the aims of patient education in the two discourses according to Dixon-Woods.
Education and empowerment discourses
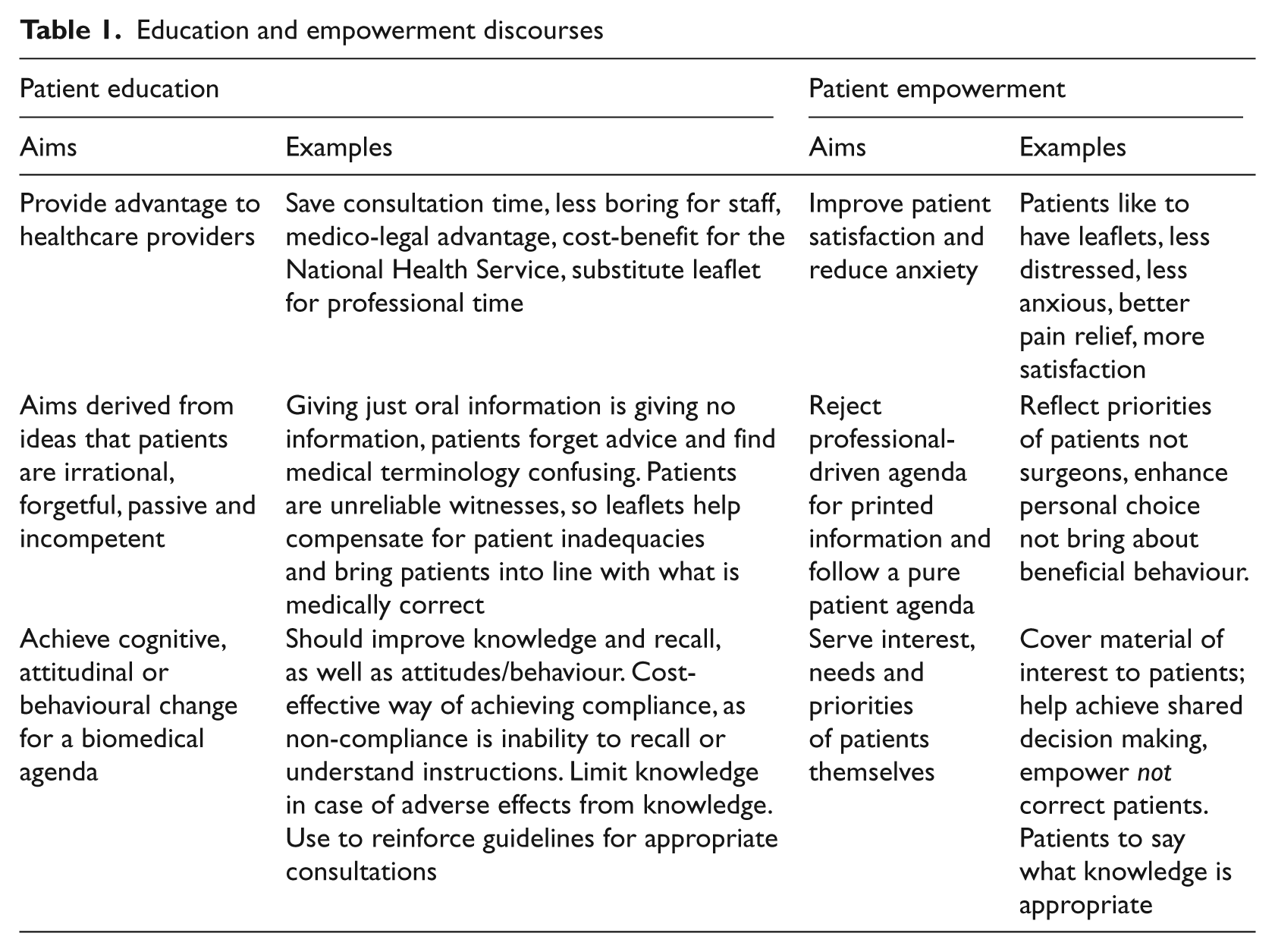
The aims in Table 1 have been classified by Dixon-Woods and show extremes of intention behind the creation, content and use of the materials, reflecting in the materials themselves.
Aims found in UK healthcare
The expert patient programme
In England the modern patient educational approach has been enforced by the National Health Service (NHS) constitution, 11 as well as clarified and implemented UK-wide through the highly successful expert patient programme (EPP) for patients living with chronic disease. 12 The EPP is a variant of the chronic disease self-management course developed in the USA in the 1970s, which is now used throughout the world in various forms. The EPP is not just about increasing patients’ knowledge of their condition, it is based upon improving patients’ skills, motivation and knowledge.
Table 2 shows the areas of knowledge and expertise between patients and professionals as defined in the EPP, and shows that a successful patient education should empower the patient to make decisions alongside the clinicians, but tailored to the individual patient’s knowledge and expertise. For this to happen the patient must understand enough of the clinician’s side of the equation to be able to effectively use their knowledge and expertise. An example of this would be a woman about to undergo chemotherapy trying to decide if she should use emergency contraception and worrying that doing so would be contrary to her views on abortion.Finding out that this is not technically the case 13 would satisfy quite a large number of women. However, if the woman’s personal view was that stopping the implantation of a fertilised embryo was abortion, the technically correct argument that the drug does not cause abortion would be inadequate and only through her understanding the mechanics of the process or the medical practitioner fully understanding her values could she make an informed choice.
Areas of knowledge and expertise
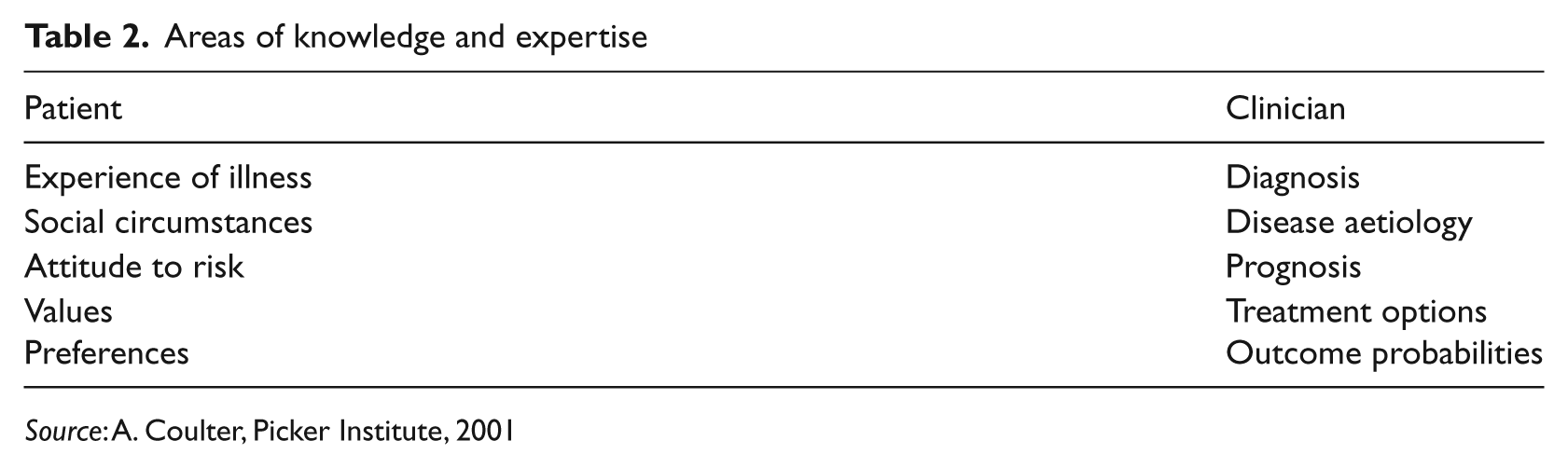
Source: A. Coulter, Picker Institute, 2001
The vision for the expert patient programme has the following thirteen desired outcomes: 12
Many more patients with chronic diseases improve, remain stable or deteriorate more slowly.
Many more patients can manage effectively specific aspects of their condition (e.g. pain, complications, medication use).
Patients with chronic diseases who become expert are likely to be less severely incapacitated by fatigue, sleep disturbance and low levels of energy.
Most patients with chronic diseases have the skills to cope with the emotional consequences of their disease.
Many people with chronic disease gain and retain employment.
Many more patients with chronic diseases successfully use health-promoting strategies (e.g. improving diet, exercise, weight control).
Most patients with chronic diseases are effective in accessing appropriate health and social care services.
People with chronic disease make greater use of adult education and employment training programmes.
Many more patients with chronic diseases are well informed about their condition and medication.
Many patients feel empowered in their relationship with healthcare professionals and have higher self-esteem.
People with chronic diseases spend fewer days a year as hospital inpatients or attending outpatient clinics.
People with chronic diseases contribute their skills and insights for the further improvement of services.
People with chronic disease work as counsellors, information workers and advocates for others.
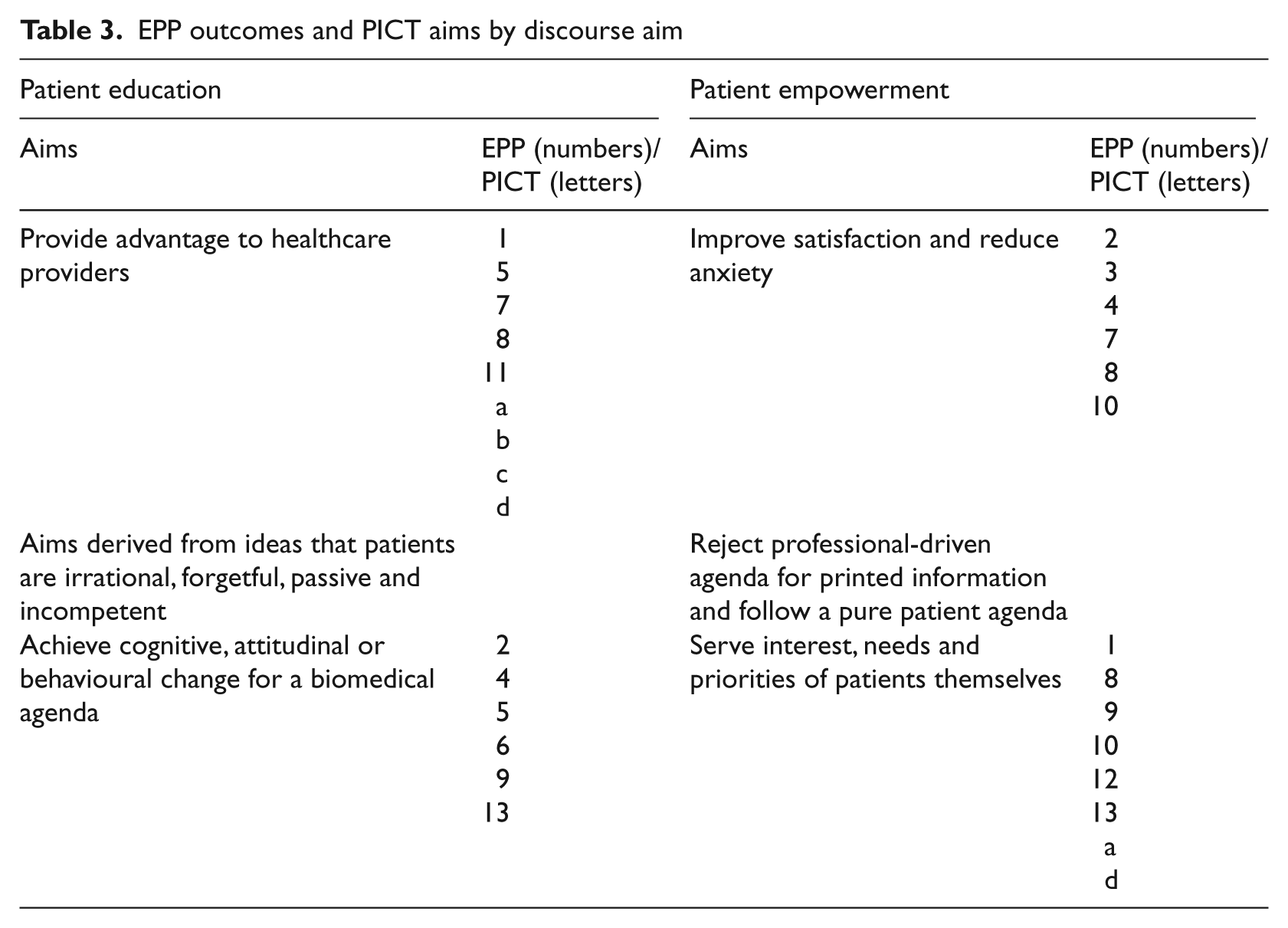
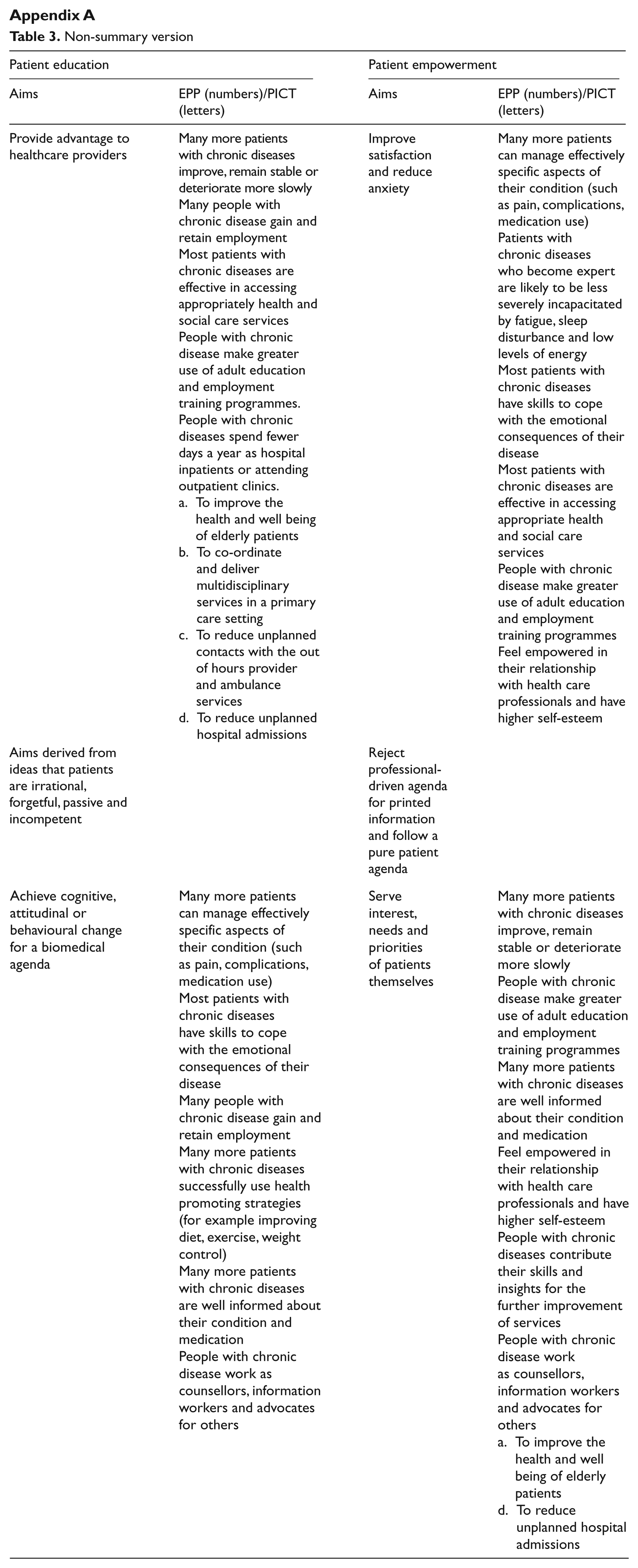
Table 3 shows a classification of these outcomes by discourse aim.
EPP outcomes and PICT aims by discourse aim
The Penarth Integrated Care Team
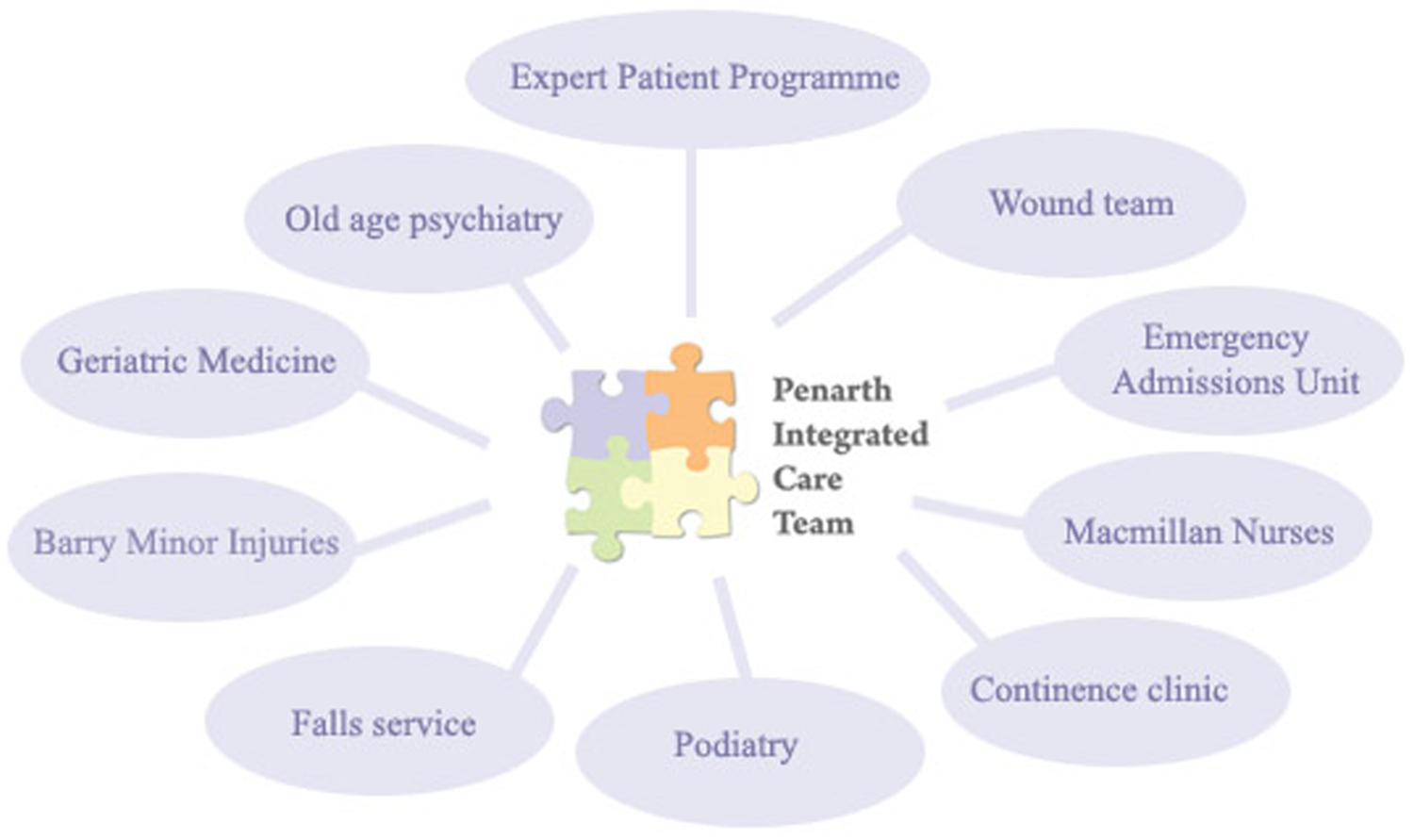
As shown in Figure 1 the Penarth Integrated Care Team (PICT) has a complex referral structure, managing patients in the community with one, or many, potentially complex condition(s). In a reply to the Welsh Audit Office the Chief Officer of the Community Health Council cited PICT as a best ‘example of a service or aspect of a service that helps a citizen access swift, seamless and appropriate unscheduled care’. 14 PICT is real world team-working to support patients in the community and working closely with the EPP. As such, the aims of the PICT are an example of the type of current best practice that patient education needs to support.
Integration and referral pathways
The aims of the PICT are:
to improve the health and well being of elderly patients;
to co-ordinate and deliver multidisciplinary services in a primary care setting;
to reduce unplanned contacts with the out-of-hours provider and ambulance services;
to reduce unplanned hospital admissions.
The position of these aims within the two discourses is shown in Table 3.
Methods
The aims of the patient education and patient empowerment discourses detailed in Table 1 are used to classify the real word desired outcomes of the EPP, as well as the aims of PICT. The purpose of this classification is to select those educational aims from the two discourses defined by Dixon-Woods that are necessary to support education within two highly regarded and successful programmes supporting patients with chronic conditions. This classification took place during a multidisciplinary literature review conducted by a computer scientist who is also an experienced teacher, alongside a PICT general practitioner. Both researchers agreed the classification, which was then presented to the other authors for agreement and comment.
This research has been done in the context of educating UK patients within the NHS, where the healthcare provider is also the national government and healthcare is free. In this scenario, reducing unnecessary consultations saves the government money rather than taking funding from medical providers. Ensuring that patients are able to work or obtain skills that help them gain employment decreases the welfare costs of patients with chronic conditions and can turn them into productive taxpayers rather than benefit receivers. Countries with different systems of medical and social care may have some significant differences in Table 3; however, as the aims of education are those of society and individuals each society would be expected to have their own aims.
Classification of aims
Incompleteness of either discourse
Classifying the outcomes for a successful EPP within the aims of the two discourses (Table 3) is very enlightening, demonstrating that neither discourse is individually capable of producing patient information to meet the needs of the EPP or PICT, and also clearly highlighting the fact that the motivation difference between the discourses is not a requirement of good patient information literature.
It is not surprising that as both discourses describe providing information to patients that both cover some aspects of an effective programme. The reason that both fail to describe all aspects of a successful programme individually is that the first labelled ‘patient education’ is an outmoded discourse concentrating upon making patients comply with their ‘doctors orders’, while the second is not a fully thought out educational method but a rebellion against the first discourse.
The patient education discourse
The first discourse was the state of patient education before the modern patient-centric care idea. While it can still be found in the literature today, services and interventions, such as the PICT and the EPP, are clearly not based solely within this discourse. A good example of this discourse is in modern health promotion, where those who smoke are not empowered to make up their mind based upon the evidence, but are instead pressured and encouraged to give up a harmful ‘bad habit’. Here, it is seen that the medical opinion is correct and dissention from that opinion should be challenged, and that such challenge is in the patients’ best interests.
While having a poor view of patients’ ability and competence is not a requirement for this discourse, it does inherently accept that patients’ ability to cope with, and understand or seek information at a particular time may be limited. This discourse is not interested in patient factors, but rather in giving patients the best evidence-based treatment, regardless of their values. As such, this discourse tends to oversell medicine—it does not talk about how the patient will interact with the treatment. It defines ‘best’ solely in terms of evidence, not in terms of patient values. The reason that this discourse has been rebelled against is that it does not treat patients as allies, but as people with no right to make decisions.
The patient empowerment discourse
The second discourse is everything that the first discourse is not. It assumes that there is no best view of evidence and that the patients should make up their own minds based upon information that is useful to, and of interest, to them. This discourse explicitly rejects a professional-driven agenda for patient information, even to the point of letting patients decide if information is harmful to them as opposed to holding back potentially damaging information. It assumes that patients should be given information on medical conflicts, but does not consider the harms that may come from doing so, such as the recent autism and measles-mumps-rubella (MMR) debate. 15
This discourse does not explicitly consider the impact of non-ideal decisions upon the individual, especially those of low health literacy.6, 16 It expects patients who realise a gap in their knowledge to seek information to fill that gap, and does not take into account the fact that patients may misunderstand information who or may not know there is a gap in their knowledge.
Criticism of older user-centric information models has highlighted the failure of these models to consider cases where patients may deliberately avoid information 17 or mistakenly believe they do not need to seek information. Education based upon this discourse has no built-in safeguards and, as such, is an agenda for an active, high health literacy population, leaving behind those who need advice and support, but also those who misunderstand information, regardless of health literacy.
Discussion
Hybrid strategic aims
Before embarking upon education it is vital to decide upon the aims of the education and on how the achievement of those aims is to be measured. As we have seen from the analysis of the aims of the two discourses neither is sufficient to fulfil the aims of the two successful programs. In the same way that Dewey argued to merge the benefits of the progressive and traditional education methods to create a new theory of education harnessing the strengths of both theories, 3 we propose that the best features of the two discourses to be merged into a set of hybrid aims capable of supporting those best practices found in PICT and the EPP.
Therefore, these hybrid strategic aims are to:
Provide advantage to the healthcare provider through methods such as improved population health, better appointment keeping, reducing inappropriate service use, etc.
Achieve changes in patient attitude, behaviour or understanding to improve health, such as by stopping smoking, taking prescription drugs correctly or reducing depression.
Improve patient satisfaction and reduce anxiety.
Serve the interests, needs and priorities of the patients themselves.
Aspects of all four of the hybrid aims can be seen in the following response from the UK Department of Health (DoH) to the question ‘What are the aims of patient education?’
The reason for patients to learn more about their long-term illnesses is to improve their confidence and sense of control through greater understanding of their condition and its treatment. This will enable patients to take care of themselves, be better able to take their medicines correctly, and possibly spend less time at their GP surgery.
18
We then have a set of strategic aims that are comprehensive enough to satisfy the requirements of excellent current practice, as well as the informal requirements of the DoH. These aims are very extensive, varying from assisting the patients to change their behaviour in ways that will benefit their health, helping patients remember appointments, helping to reduce their anxiety and serving their myriad complex needs and priorities.
Lessons from education
Education is not a static process that is done to a person or by a person. It is the process of ensuring a person gains knowledge and then is empowered to apply and build upon that knowledge in a way that benefits the individual.19, 20 The word ‘ensuring’ is an important term and the only way to be certain that the patient has been effectively educated is to assess that education. This is achieved by measuring the learning of individuals against set educational objectives, tailoring the learning to the ability level of the individual and, finally, using learning support to assist those not achieving the objectives to achieve them. Clinicians informally follow this process when they meet with patients, gauging the level of understanding of patients and trying to explain the condition to them. Patient education leaflets, however, have no such ability levelling or feedback, but interactive learning technologies can offer learner tailored content with integrated communication and assessment.
The first thing to realise from educational theory though is that there are three domains within which aims can be placed. 21 Giving a patient educational material and assisting them to understand it is within the cognitive domain dealing with knowledge, recall and intellectual skills. Most of the hybrid strategic aims deal with values, attitudes and behaviour. This type of aim falls within the affective domain and explains why so many studies measuring the attainment of cognitive targets fail to also achieve those affective patient outcome targets or achieve the outcome targets without increasing knowledge. The third domain is the psychomotor domain, which concerns physical skills, coordination, etc.
What then is the point of learning for patients within the cognitive domain? The most important reason is that many patients want to be accurately informed about their condition (although some seek to avoid disturbing information 17 ). Also, a core of evidence-based knowledge allows the learner to better judge the correctness of information found in other places, such as on the internet. Finally, it allows the health professionals to concentrate upon satisfying the patient’s needs within a consultation, reducing the amount of time spent discussing factual information and using that time instead to meet the educated patient’s needs, 22 resulting in better patient satisfaction.
Patient education system design
It is clear that designing an education system containing enough information to fully satisfy Aim 4 is not really plausible as we cannot know exactly what information each individual patient needs and wants. This is very similar to trying, in education, to fully educate a population on everything they need to know. Instead, what is done (in theory) in education is laying the groundwork, giving people a framework to become self-learners throughout their lives. The importance of the framework is that without core knowledge, individuals struggle to identify or understand information they are missing, or rate the validity of information that they find.
Harland and Bath summarise the differences between a system-centric and user-centric approach to understanding how to satisfy the information needs of patients and carers, and conclude that user centric approaches are the ideal. 2 However, while it is true that we cannot satisfy patients’ and carers’ full cognitive or affective domain aims through system-centric approaches, we can cover an evidence-based core of cognitive domain information, satisfying the cognitive aims of the educators (remembering that overall educational aims are the aims of both educator and educated) and giving the educated that core of knowledge to empower them to achieve their own aims. There is a danger here though that information science seeks to address: we cannot know the way that this information will be understood and used by the individual. As such, this core information provision must be embedded within an educational program that assists the individual learner to use the new information in a beneficial way, to avoid or minimise harm during the education. A system-centric approach alone will not be able to support the learner in finding the additional information that they require, so any system to support the hybrid strategic aims will need to be designed using a mixture of system-centric and user-centric approaches.
In terms of patient information, a system should help teach patients, carers and families an evidence-based core of information targeted to their condition and differentiated according to health literacy, empowering them to increase in health literacy and then supporting them in seeking additional information. The system must also be part of a formal education program, with patients, clinicians, educationalists and other stakeholders continually working to improve the programme and keep it relevant to both the users and healthcare policy. Ideally, the system should enable patients to discover new resources, share learning resources with their carers, ask questions of health professionals to support learning, as well as offering health literacy building optional ‘modules’ such as basic statistics, to support patients in building their health literacy.
Conclusion
In the past, patients were often considered to be passive, somewhat stupid beings needing to be told what to do. 1 This was contrasted with the ‘better’ idea that simply providing information empowers patients to make informed choices. The problem, of course, is that providing information leaflets guarantees no such thing 7 and unless the information in those leaflets is sufficient, believed and understood to a level where the information can be applied, then it cannot empower the patients and may even harm them.
The problem with entirely rejecting the educational approach of telling the patient what a good decision is and replacing it with an approach of providing unbiased information for the patient to make sense of is that it ignores ability and the way people learn.Some patients are capable of a great deal of self-directed learning, while others need support—especially in the building block concepts needed to interpret the unbiased information (statistics, probability, quality of evidence, etc.), termed ‘health literacy’.
Even those patients capable of a high level of self-directed learning have to identify gaps in their understanding and seek information/correctly interpret information to fill those gaps. This cannot be an error-proof process and requires quality control.Patient information should not be separated from the principle ‘First do no harm’; however, we also cannot go back to a time where patients simply followed their doctors orders. The four hybrid strategic aims can effectively guide the creation of patient education programs; however, giving patients more access to information will not achieve these aims for all patients. Instead, the information provision must be part of a patient education programme. This programme must ensure that the patient progresses in relevant, evidence-based understanding of their condition, and requires that their understanding is assessed and misconceptions corrected during the process of patient education. The educational aims chosen for the patient education programme must also help to support the four hybrid strategic aims.
Further research is needed in both targeting differentiated information to patients to directly improve their understanding of their condition, as well as supporting patients seeking additional information above and beyond the evidence-based facts about their condition and treatment.
Footnotes
Appendix A
Non-summary version
| Patient education | Patient empowerment | ||
|---|---|---|---|
| Aims | EPP (numbers)/PICT (letters) | Aims | EPP (numbers)/PICT (letters) |
| Provide advantage to healthcare providers | Many more patients with chronic diseases improve, remain stable or deteriorate more slowly Many people with chronic disease gain and retain employment Most patients with chronic diseases are effective in accessing appropriately health and social care services People with chronic disease make greater use of adult education and employment training programmes. People with chronic diseases spend fewer days a year as hospital inpatients or attending outpatient clinics. a. To improve the health and well being of elderly patients b. To co-ordinate and deliver multidisciplinary services in a primary care setting c. To reduce unplanned contacts with the out of hours provider and ambulance services d. To reduce unplanned hospital admissions |
Improve satisfaction and reduce anxiety | Many more patients can manage effectively specific aspects of their condition (such as pain, complications, medication use) Patients with chronic diseases who become expert are likely to be less severely incapacitated by fatigue, sleep disturbance and low levels of energy Most patients with chronic diseases have skills to cope with the emotional consequences of their disease Most patients with chronic diseases are effective in accessing appropriate health and social care services People with chronic disease make greater use of adult education and employment training programmes Feel empowered in their relationship with health care professionals and have higher self-esteem |
| Aims derived from ideas that patients are irrational, forgetful, passive and incompetent | Reject professional-driven agenda for printed information and follow a pure patient agenda | ||
| Achieve cognitive, attitudinal or behavioural change for a biomedical agenda | Many more patients can manage effectively specific aspects of their condition (such as pain, complications, medication use) |
Serve interest, needs and priorities of patients themselves | Many more patients with chronic diseases improve, remain stable or deteriorate more slowly |
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.