
Abstract
When collecting data from a single electronic medical record (EMR), few studies of Intensive Care Unit (ICU) patients admitted directly from an Emergency Department (ED) focus on observational methodologies examining occupancy of both the ICU and the ED, and population characteristics. This quantitative study design and analysis, with a sample size of 1433 cases using regression techniques, suggested odds of mortality were more likely with a higher ICU occupancy/census and if uninsured. There was no statistical difference based on ED occupancy/census at time of decision to admit to an ICU and no difference whether admitted on a weekend or weekday. Inpatient ICU occupancy is one of the variables that impacts waiting time and overcrowding in the ED, and, in this study, inpatient occupancy in the ICUs impacted patient outcomes. As all healthcare providers make up the interprofessional team and work within complex systems, ease of retrieval of EMR data can hasten decision support to improve quality outcomes.
Keywords
The entry point for many patients admitted to a hospital is through an accident or emergency room. Patient data critical to decision support is collected and documented in various modalities, such as a computerized system or a mix of computerized and paper documentation. Many of the computerized systems do not interface easily with in-hospital data systems housing various data elements. These elements pertain to patient information documented from all healthcare practitioners, including nursing documentation, demographics and, in many instances, payer sources within the electronic medical records (EMRs). When attempting to do outcomes research to investigate indicators which may improve outcomes, retrieving data can present challenges in dealing with multiple data systems. The resultant difficulty in retrieval of data may impact the effectiveness of care decisions during a hospital stay. Nurse informaticians work closely with information systems, developing and integrating practitioner generated data within the EMR including methods for retrieval of date. This study highlights the retrieval of data from a single EMR of an acutely ill population admitted to the intensive care unit (ICU) from an emergency department (ED) or accident and emergency room. The study hypothesis was: there is no difference in outcomes of ED patients admitted directly to an ICU on individual characteristics, factors, or ED and ICU fluctuations in occupancy. This study examined and investigated various characteristics, time-sensitive interventions, other factors, and occupancy in both the ED and ICU settings on outcomes of hospital mortality for the ICU admission originating from the ED. All of the data for this study was retrieved from a single database system known as Microsoft Amalga®.
Study aims
This study accessed and collected data from the EMR of a large urban hospital located in a busy metropolitan area in the eastern USA from Microsoft Amalga, the clinical information system. The aims of this study were twofold: (i) to collect all of the data from a single database repository system housing the medical record; and (ii) to investigate these data to determine the impact of specific characteristics and other factors of the critically ill admitted from the ED to the ICU on hospital in-patient mortality. The goal of this study was to discover potentially subtle issues of this specific population to further explore and/or recognize indicators for faster recognition to decision for ICU admissions from the ED, thus subsequently building on further research questions and providing opportunities to improve quality outcomes.
Framework
Many factors influence the length of time a patient may spend in the ED before moving to an ICU. Moving patients from one unit to another depends on many factors, such as decision support, communication, staffing and occupancy. In the ED setting the flow of the patients through the system is measured as input–throughput–output. This approach is also reflective of the organizational flow, which can be characterized as structure–process–outcome. 1
On an organizational level census or occupancy reflects the number of beds filled, whereas capacity is the number of beds available: occupied or vacant. The occupancy rate, as well as whether all beds available are occupied, provides a snapshot measure of a given unit at a given time. Crowding changes this measure and is a distinct problem in the ED measured by ‘greater input (numbers and/or acuity of arriving patients), inefficient throughput (ED operational processes), and diminished output (downstream obstacles to moving patients out of the ED)’. 2 Comparably, structure–process–outcome can be used to extrapolate the impact of the system on the flow and outcome of the patient. According to Herald et al., 3 organizations tend to focus more on the structure and outcomes with limited inclusion of the impact of processes. Yet, processes are driven by structure, such as policies/procedures and protocols. The outcomes of the processes must be evaluated by that structure to initiate and implement quality improvements.
In terms of characteristics, investigating other factors and subtleties can include not only demographics but also the ED and in-hospital occupancy at a given point in time. This, in turn, may impact decision and implementation of interventions. In a study of ICU admissions Clark and Normile4, 5 discussed implications of timely interventions while still in the ED prior to transfer to ICU and the influence on hospital course. The outcomes measured were length of stay in the critical care unit for the hospitalization and mortality. While there are a multitude of factors to consider within the ED setting, few studies have focused on the ICU population admitted specifically from the ED to an ICU. 6 More recently the National Quality Forum 7 has endorsed quality measures such as length of stay in the ICU and in-hospital mortality rates of the ICU population, as observational data and not just risk-adjusted data.
Overcrowding in the ED, high occupancy of in-patient beds and staffing can influence decision-making, even at patient presentation. Recognition of these factors can generate data to promote identification of subtleties, implications of nursing practice, interprofessional practice, and potential to examine and or modify systems to facilitate improved outcomes, thus evaluating, defining, refining and implementing changes to improve outcomes.
Literature review
The second aim of this study investigated various aspects and characteristics of the overall critical care population originating from the ED. Simpson et al. 6 in a descriptive study found 26% of ICU admissions in England originated from the ED. Furthermore, Simpson et al. indicated of their publication that ‘no studies had considered all critically ill and injured patients as a group’. 6 This study examined differences on outcomes of mortality of those patients admitted to ICUs originating from the ED and those that came to ICUs from other sources. The management at the multidisciplinary (interprofessional) level was highlighted to involve many healthcare professionals, including nurses, physicians and others.
Clark and Normile4, 5, 8 collected data from one database system EMR, known as Azyxxi, in a single cardiac referral tertiary medical center. The study focused on critical care admissions from the ED during a two-year period (2003 and 2004). The entire population of those admitted to the ICU from the ED in that period were included in the study. Approximately 3% of the total ED visits were admitted from the ED directly to one of the several ICUs. Other reports 9 from the US Centers for Disease Control (CDC) found that, based on the number of ED visits in the USA nationwide for 2003, 1.3% were admitted to the critical care units. Nawar, et al. 10 found approximately 1.9 % of all ED visits for 2005 were admitted from the ED to ICUs.
Regarding time-sensitive management of critically ill patients to be admitted from the ED to the ICU, Lucas, et al found ‘ED length of stay was correlated with the number of admissions and census (occupancy rate) of higher acuity nursing units such as in the critical care areas, more so than the number of ED patients each day. It was further suggested that improving the availability of in-patient critical care beds may reduce ED length of stay’. 11 The importance of time-sensitive interventions related to delayed admissions to the ICU from the ED effect outcomes of mortality and length of stay. 12 Admission stays of greater than six hours in the ED while waiting for an ICU bed increased the likelihood of ICU length of stay and mortality. 12 Clark and Normile 4 examined outcomes of mortality investigating time of recognition in the ED to time of implementation of interventions of the ICU population originating from the ED. Using logistic regression and log transformation of time-sensitive data the ‘time period from the admission order for an ICU bed while in the ED to leaving the ED for the ICU the more likely the mortality of the hospitalization’. 4 They also found the mean time for the length of stay in the ED for the critically ill was 4.9 hours. 4 Time to interventions, such as the ‘time to first medication suggested the longer it took to dispense the first medication once arrived in the ED, the longer the hospital stay‘. 5 Patient visits on weekends resulting in ICU admission were more likely to have a longer hospital stay and increased likelihood of mortality.4, 5 Additionally, it was suggested ‘the use of a hospital wide integrated database system would facilitate outcomes research’. 5
The first aim of this study was to collect all of the data from one data repository. According to Geisler, et al. 13 when analyzing data use of EMR systems in EDs across the country they found there were differences in the use of these data based on what was considered meaningful data within the EMRs. What can be just as problematic is that systems within many hospitals are proprietary and one system may house some variables of the medical record and the other houses different patient variables. The adoption of the American Recover and Reinvestment Act (AARA) in the USA specifically identifies steps to engage in the full use of the EMR throughout the healthcare system.
Meaningful use of healthcare data is foremost in improving outcomes of care. 14 The ability to retrieve meaningful data from an EMR for research can further improve outcomes, provide the opportunity to generate further questions which can facilitate nursing research as part of the interprofessional team and support the validity of integrating nursing data with other more comprehensive patient medical records data and systems. 15
Methodology
This study was a quantitative, retrospective, exploratory, comparative analysis specifically of the ICU population originating directly from the ED. Techniques similar to data mining were used to explore within Amalga, which runs on a Microsoft Windows Server and a SQL server, the many thousands of data elements associated with each given patient within its repositories. This system provides the researcher with access to the numerous data elements for each patient. Minimal research is available that focuses on clinicians’ abilities to query systems such as this, as well as to visualize results within the system. 16 This study was of patient data from 2004 and 2005 in a tertiary level 1 trauma cardiac referral center which had several ICUs. All ICUs were included in this study. Inclusion criteria were those aged 18 years and older, all admission diagnoses, co-morbidities up to nine, uninsured, insured, male, female, all races categorized within the hospital and admitted to one of the ICUs directly from the ED. Exclusion criteria were those under 18 years of age, deceased in the ED, traumas which were received from other facilities by helicopter or ambulance, any case that was transferred from other facilities for a higher level of care to the ICU, and cases that went to the operating room before arriving in the ICU from the ED. Transfer cases which received care from other facilities were excluded because they had received prior ED or hospital-based interventions outside of the study facility. Cases that went to the operating room after leaving the ED had subsequent interventions outside of the study ED and data were unavailable as to the number of cases that were identified as ICU admissions that were changed post-operatively to a surgical bed. The minimum of traumas in the field received interventions based on trauma care protocols and were excluded from this study. Institutional review board approval was obtained from the participating hospital and an academic university. Data were accessed remotely using a Cisco VPN client, user name, password and encryption. Data were collected from a single database repository, Microsoft Amalga. Complex and temporal queries with filtering when searching within the system provided the mechanism for retrieval of data. The process optimized search techniques of elements investigated in this study. Furthermore, this system allows for the ‘interactive query interfaces for researchers and clinicians to explore data that have specific temporal patterns in both numerical and categorical data will dramatically increase the benefits of EHR databases’. 16 With the exploratory nature of this study all cases admitted to all the ICUs which met the inclusion criteria were included with a final number of 1433 cases. SPSS was used to analyze the data. Data were time-sensitive, requiring initial access to personal identifiers. Once data were collected, cleaned and confirmed, personal identifiers were removed and data were organized for analysis. Patient characteristics, times, occupancy and mortality were tested using regression techniques. Log transformation was used for time sensitive data elements as this function transformed the time-sensitive data to more normal curves for analysis between groups. Multiple and logistic regression investigated predictive associations along with descriptive techniques.
Results
Using the regression model, the longer the time period from arrival in the ED to the time of the order for an ICU bed, the more likely the mortality with an odds ratio of 1.288 (Table 1). The higher the ICU occupancy at the time of decision to admit to the ICU the more likely the mortality with odds at 1.091 and significance at 0.026 (95% CI 1.011–1.77). The occupancy of the ED at the time of decision to admit did not impact mortality in this population. The uninsured and those arriving at the ED by ambulance and admitted from the ED to the ICU had higher mortality with odds ratios of 1.577 (sig. 0.036, 95% CI 1.030–2.414) and 1.829 ( sig. 000, CI 1.330–2.516) respectively.
Logistic regression: Predictive associations of Emergency Department (ED) admits to Intensive Care Units (ICUs) on hospital mortality
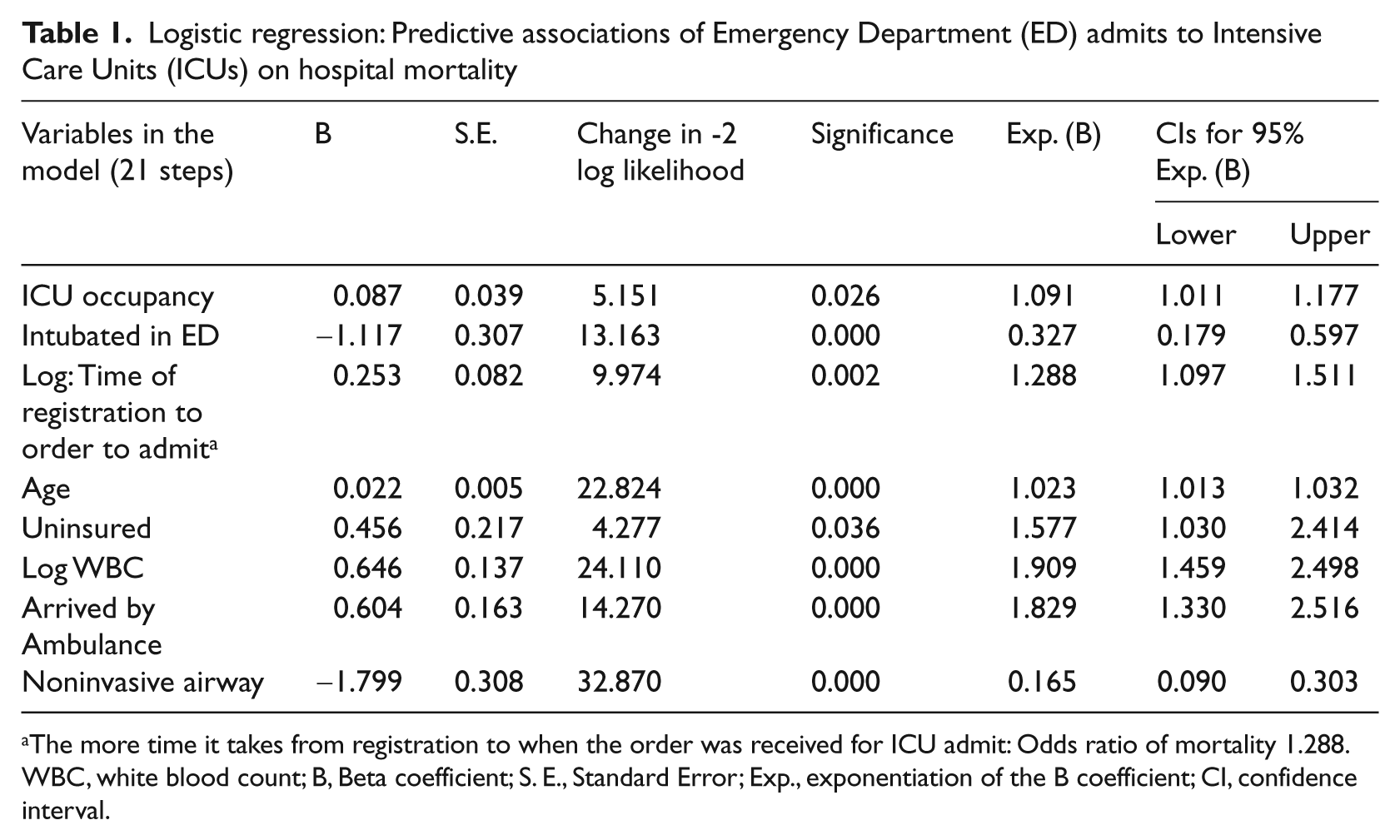
The more time it takes from registration to when the order was received for ICU admit: Odds ratio of mortality 1.288.
WBC, white blood count; B, Beta coefficient; S. E., Standard Error; Exp., exponentiation of the B coefficient; CI, confidence interval.
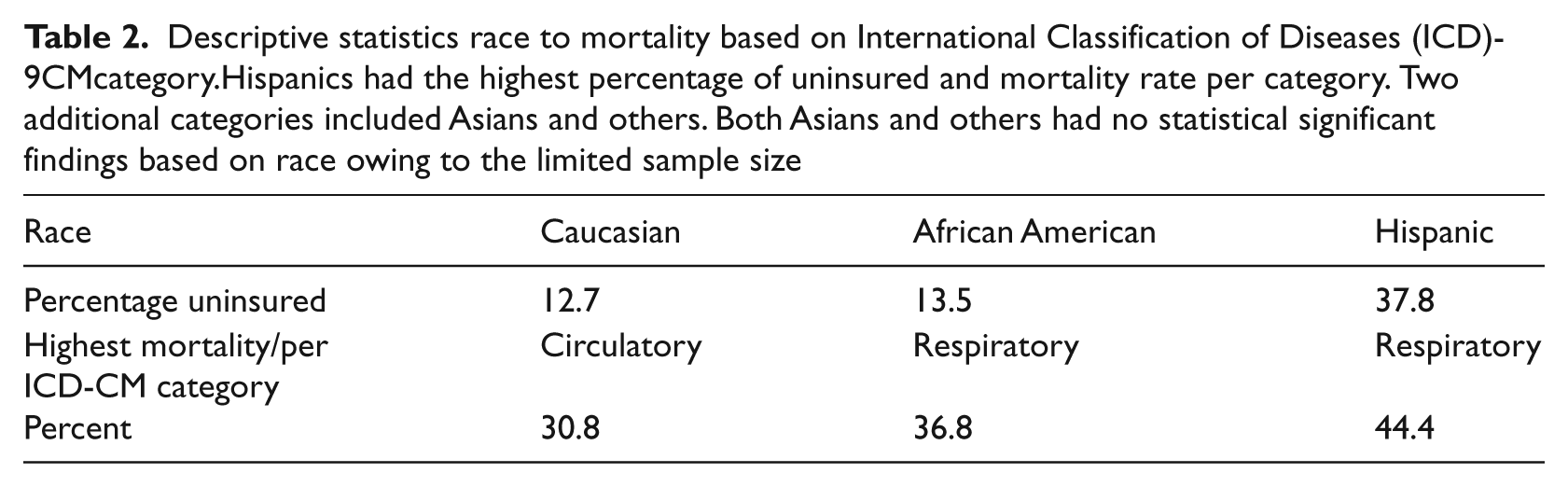
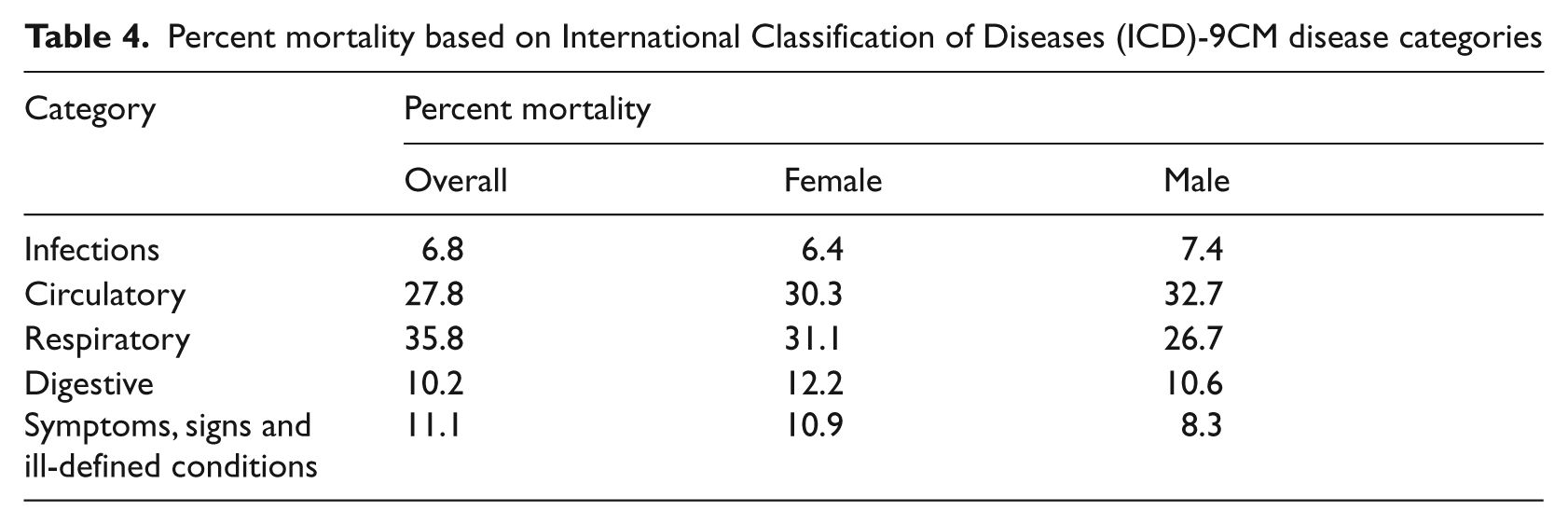
Descriptive statistics found approximately 29% walked into triage and 60% arrived by ambulance. The mean length of stay in the ED was 5.89 hours. Thirty four percent were intubated after arrival in the ED. When comparing numbers of co-morbidities, increased co-morbidities increased the likelihood of mortality, and those with nine co-morbidities had a mortality rate of 78.7%. With further descriptive statistics based on the International Statistical Classification of Disease (ICD-9CMs), the percentage of mortality for Hispanics was highest for respiratory disorders among the races reported in the data (Table 2). Mortality by race and age reported in this study varied (Table 3). In relation to gender females had the highest mortality rates for ICD-9CM categories of respiratory, digestive, and signs and symptoms ill-defined. Males had the highest percentage of mortality in the categories of infections and circulatory ICD-9CMs (Table 4). There were more males than females (approximately 52% to 48%) admitted to the ICUs and more African Americans than other ethnicities were admitted. When comparing healthcare coverage and mortality, the uninsured had the highest mortality at 24.9% and, based on odds ratios in the model, were 1.55 times more likely to die during the hospitalization (p = 0.036, 95% CI 1.02–2.4).
Descriptive statistics race to mortality based on International Classification of Diseases (ICD)-9CMcategory.Hispanics had the highest percentage of uninsured and mortality rate per category. Two additional categories included Asians and others. Both Asians and others had no statistical significant findings based on race owing to the limited sample size
Age of race and percent mortality
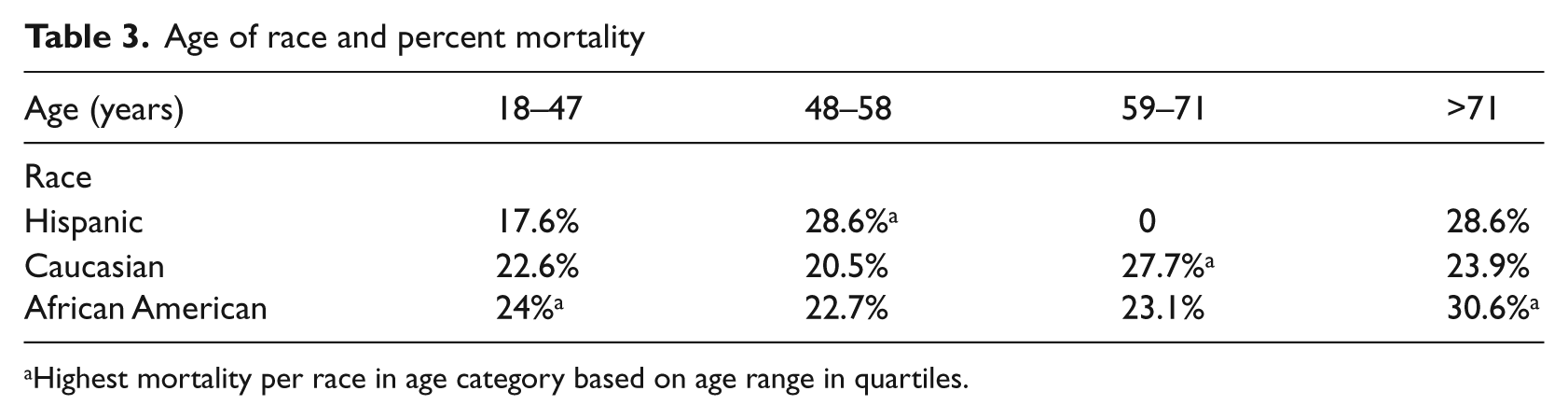
Highest mortality per race in age category based on age range in quartiles.
Percent mortality based on International Classification of Diseases (ICD)-9CM disease categories
Discussion
One of the major variables that impact wait times in the ED is inpatient occupancy translating to decreased availability of beds for ED admissions. 17 Reduced available beds affect how long it takes for an ICU admission to physically leave the ED for the inpatient bed. This can be further complicated by the volume or number of patients in the ED, which, in some instances, is more than the ED can accommodate based on number of beds or stretchers available. This overcrowding (delayed throughput) can impact outcomes of care and has broad-reaching effects to the point of ambulance diversions, which could be deleterious to patient outcomes. 18 Studies on overcrowding have found associations with an increase in mortality and surmised patient outcomes to be impacted by system issues, as well as immediate decisions based on presentation in the ED. 19 Lucas et al. 11 indicated that episodes of high occupancy can delay the movement of patients through the system. Prompt movement is dependent upon swift access to data and collaborative communication within the system to facilitate placement of patients from the ED to an ICU setting.
Fluctuations of occupancy in the ED for this population was not associated with hospital mortality. However, the higher the ICU occupancy (fewer available beds) at the time of decision to admit was associated and suggested increased mortality. When addressing weekend or weekday admissions, observational studies have found that weekend admissions to the ICU had a higher mortality rate for hospitalization than weekday admissions to the ICU. 4 Patients admitted on weekends with myocardial infarctions were associated with higher mortality rates. 20 In this study, cases admitted to the hospital at the weekend experienced a mortality rate of 24.6% versus 21.8% for weekday admissions; yet, there was no statistically significant difference on the outcomes of mortality.
Remembering that the population of this study was exclusively all critical care admissions arriving from the ED, limited data were available for this specific population for comparison with other studies. However, a study published in 2010 retrospectively investigated over 154,000 adult discharges in the USA with the diagnoses of myocardial infarction, stroke and pneumonia. 21 This study found that the uninsured mortality of the adjusted odds ratios was 1.52 for acute myocardial infarction, 1.49 for stroke and 1.21 for pneumonia. A study focusing on uninsured hospitalized children 22 analyzed 23,000 hospitalizations and found the odds of mortality to be 1.60. Both of these studies investigated overall hospitalizations versus ICU admissions directly from the ED specifically. Thus, the severities of illness in those studies were applied to those specific populations for the hospitalization. The inclusion criteria for this study were only cases that were directly admitted to the ICU from the ED. Minimal literature exists comparing ICU admits from an ED on odds ratios of mortality. However, considering the study of admissions of children with a higher odds ratio and the study of the three diagnoses odds ratios nearly as high the results of this study can only suggest the level of acuity was much higher in this population, which impacted the odds ratios for mortality.
Lack of insurance is a known factor in mortality and morbidity based on the reduced episodes of care due to decreased access to healthcare. 23 The Institute of Medicine (IOM) report from 2002 of ‘Care without coverage, too little too late’ indicated that the uninsured's life expectancy and quality were distinctly different. More recently, the Urban Institute examined the IOM’s findings, as well as several other studies of outcomes for the uninsured and found that, overall, of the data reported by the IOM, deaths of those uninsured between the ages of 55 to 64 could have been lowered by as much as 27% if they had been insured. 23 The uninsured rate in the USA has climbed to 17.7% as of January 2012. 24 In Hispanics the uninsured rate was 40.7%, for those aged 26–64, for all demographic groups it was 19.5% and for Asians it was 14.7%. 25 The findings of this study could be reflective, as 37.8% of Hispanics in this study were uninsured. Forty four percent of the mortality of those Hispanics was from the category of respiratory disorders.
The total number of co-morbidities were examined and compared between the two groups: those with healthcare coverage and the uninsured. At four co-morbidities approximately 3% of cases had healthcare coverage and 9.8% were uninsured. When examining the overall average of co-morbidities in this population the uninsured had twice as many co-morbidities as those with coverage.
When addressing weekend admissions of the uninsured versus weekday admissions to the hospital in the literature, a higher percentage was admitted from the ED on the weekend versus the weekday, and the mortality rate was higher for those admitted to the hospital on weekends versus weekdays. The suggested association was that patients admitted on the weekends tend, overall, to be more critical than those admitted on weekdays. Yet another suggested association was that access to all services varies on weekends versus weekdays. When examining admission rates on weekends in this study, 38% of the uninsured were admitted on the weekend versus 27.1% for those with healthcare coverage; thus, 10.9% more of the uninsured were admitted on the weekend to the ICU from the ED than those with healthcare coverage. For admissions during the weekdays the rate was 62% for the uninsured and 72.9% for those with healthcare coverage. Even with the differences between the uninsured and those with healthcare coverage there were no statistical differences in mortality whether admitted on a weekend or weekday to the ICU for the uninsured or those with healthcare coverage.
Overall, for cases admitted directly from the ED to an ICU in this study, if uninsured, mortality was more likely for the hospitalization versus those with healthcare coverage. Examining more closely the uninsured specifically, the more co-morbidities the more likely the mortality (odds ratio of 1.296, significance .007, CI 1.072–1.568). Therefore, the higher mortality for the uninsured could be attributed partially to the greater number of co-morbidities.
Many studies found in the literature discuss severity scales or measures. 26 In this study the level of measure that was accessible for this population (reported in the database) was the triage system assessing the severity of the cases documented by nursing. There are several different triage systems used around the world and the one employed in this study was the five level triage scale, similar to both the Canadian and Australian systems. Limited data were entered into the database documenting the triage levels. When investigating further, minimal to no documentation was retrievable from the dataset for either nursing triage (as above) or Apache II scores that were assigned to the in-patient ICU population.
Minimal literature was found specifically on the entire ICU population originating from the ED and length of hospital stay. In this study the mean length of hospital stay for this critically ill population was 10.89 days. The mean length of stay in hours in the ED for this population was 5.89 hours, whereas a previous study at the same facility noted mean length of ED stay for the critical care population to be 4.9 hours. 4
Strengths and limitations
This study collected data from one database system repository housing thousands of variables of the patient record. The initial ED charts were paper documentation and scanned into the system. Many elements or data points from the scanned charts were also entered into the database by hand. Manual entry of data is a known factor that can impact the rigor of any retrospective study. This is a known risk identified in the literature. 27
For any nursing informatics approach to documenting and retrieving data, information technology support is essential and was an invaluable strength in this study, and impacted validity and reliability of the data. The collaborative interprofessional group involved in this study included medicine, nursing and information technology experts. Few institutions in the USA allow access remotely because of interpretations of the Health Insurance Portability and Accountability Act when research involves patient data. Therefore, with the security measures, confidentiality and removal of patient identifiers, a definite strength was clearly the ability to access the EMR remotely, as opposed to the time required for onsite visits to collect data.
This database system was built on a Microsoft sequal server platform. When logging in to access the EMR, a virtual private network (VPN) connection was used with a username, password and built-in encryption. Initial access to personal identifiers was required because of the time-sensitive sequencing of variables per case based on interventions and outcomes. Clinical experiences and insight utilizing nursing knowledge of ICU and ED expectations was crucial in this research. These insights and skills provided key expertise in the development of criteria to explore the variables. Informatics experts provided support with their expertise in searching with filters/queries to collect the critical data for this study. SPSS was used to control for extraneous variables during the analyses.
A limitation in this study was that data was collected from a single, large, urban hospital and therefore the results are not generalizable. Though few specific nursing variables were included in the database the findings from the data can generate further nursing researchable questions. If one considers the available data from a single comprehensive database, the research questions that could be generated if all EMR data were available in one accessible database would potentially increase the rigor and value of detailed outcomes research.
Conclusion
One of the aims of this study was to collect all of the data from one database system. In a previous study at this same facility the database repository system was called Azyxxi, which is now Microsoft Amalga. At this facility Microsoft Amalga and Cerner MedConnect is in place as a record documentation system. This system is hospital-wide and includes outpatient clinical information systems. 28 It provides the opportunity to potentially merge Nursing Quality Indicators 29 as key components of nursing care delivery. Inclusion of the nursing indicators can provide interconnected access in database systems to study questions based on nursing and the interactivity of all healthcare practitioners’ experiences.
Findings in studies such as those from the Kaiser Foundation 30 report demographics of the uninsured. Those studies note that because of many of the disparities and decreased access to care, once hospitalized they are more likely to die earlier than those with healthcare coverage. These disparities impact care sought by the uninsured when interventions would be most beneficial to include not filling prescriptions which may provide management of chronic or acute illnesses. 30 Therefore, when the uninsured do seek care, they are likely to be more acute with co-morbidities which have not necessarily been diagnosed. This population experiences more complications with managing their health though management of this population is not directly under the control of hospitals subsequent discovery of quality measures can provide valuable insights.
An observational study of the entire ICU population can potentially lead to specific quality measures. These measures can provide information to improve outcomes. 7 Such discoveries could potentially modify protocols (for potential earlier recognition and system responses) in addition to the many outcomes studies using risk-adjusted data. 31 Within this study the findings implicate the necessity for improving access to care for the uninsured to reduce the complications experienced by this population leading to earlier interventions and management. This lens could be instrumental in recognizing factors that impact the flow through the system which otherwise are not as visible to address. Additionally, exploring the entire data for ICU admissions as a population can provide information relating to variables which can be further defined or refined to develop new or modified risk-adjustment tools. This exploration would promote future studies.
Researching the data to discover characteristics with the inter-related time intervals of actions and responses can provide valuable data to create or modify approaches to the ICU population presenting in an ED. One of the findings in this study looking at associations of high occupancy of the ED at time of decision to admit to an ICU on odds of mortality was not statistically significant. However, high occupancy in the ICUs at the time of decision to admit was statistically significant. This finding suggests the movement of patients through the system is more problematic than the length of stay in the ED for the critically ill population while waiting for an available ICU bed. Another finding was the outcome of mortality in the uninsured population in this study. Limited literature exists focusing on the ICU population as observations, although studies were found which identified significant odds ratios suggesting high mortality for the uninsured in children and adults risk adjusted for myocardial infarctions, stroke and pneumonia. Further studies retrieving EMR data, including nursing indicators, may provide further recognition of methods and or protocols to improve outcomes.
As continued development and implementation of comprehensive EMR systems take place, all practitioners are part of the collaborative interprofessional team. Nursing and nursing informaticians are integral to the systems for documentation and retrieval of nursing-generated data important for decision support, improving outcomes and collaborating as part of the interprofessional research and clinical team. Merging nursing data and medical record data into one system will provide opportunities for exploratory outcomes research, thus transitioning all healthcare professionals’ data into a single system or interfaced communicative systems to provide a platform for ease of retrieval of data important for outcomes research. The ease of access to data translates to quicker decisions.