
Abstract
Advanced mobile devices allow registered nurses and nursing students to keep up-to-date with expanding health-related knowledge but are rarely used in nursing in Sweden. This study aims at describing registered nurses’ and nursing students’ views regarding the use of advanced mobile devices in nursing practice. A cross-sectional study was completed in 2012; a total of 398 participants replied to a questionnaire, and descriptive statistics were applied. Results showed that the majority of the participants regarded an advanced mobile device to be useful, giving access to necessary information and also being useful in making notes, planning their work and saving time. Furthermore, the advanced mobile device was regarded to improve patient safety and the quality of care and to increase confidence. In order to continuously improve the safety and quality of health care, advanced mobile devices adjusted for nursing practice should be further developed, implemented and evaluated in research.
Introduction
In nursing care, the steady increase of health-related information implies a need for useful, practical Information and Communication Technology (ICT) tools that easily provide access to accurate information. 1 Updated information is usually available on the Internet, but personal computers are rarely available at the patients’ bedside. Consequently, there is a need for applicable mobile devices, which can provide immediate access to accurate information.
Background
Mobile devices (also referred to as handheld devices or personal digital assistants) are small and portable, providing access to any information or any function that can also be found or executed on a desktop computer. 2 Mobile devices have revealed advantages in nursing practice for registered nurses (RNs)3–13 and nursing students (NSs).14–19 Among RNs in home care settings and acute care hospitals, the small size of the advanced mobile device (AMD) is appreciated, the mobile devices are considered to be useful 6 and they are also seen as increasing learning.11,13 By using a mobile device with a support system for preference-based care planning in rehabilitation and medical units, RNs’ work and responses are found to be more congruent with patients’ preferences. 4 RNs working in acute care, home care, long-term and correctional settings have improved their skills and awareness of research evidence when they have access to clinical information resources via a mobile device. 3 When used in the care of nursing home residents, a mobile device prepared with information relevant to dementia care improved the effectiveness and efficiency of the patient care. 5 Furthermore, RNs saved recording time when using a mobile home hospice information system. 7 A mobile decision support system supplied with a barcode reader has been proven to be useful in obtaining an overview of the patients’ medication, 20 and when used for patient identification, it increased the safety of blood transfusion.8–10 In addition, when RNs used a decision support feature that automatically calculated obesity-related diagnoses, they identified a larger number of diagnoses, and there was a lower false negative rate. 12
By using a mobile device, NSs were able to access necessary information and also to make notes, independent of time and place.21,22 The mobile device was found to improve self-efficacy14,21 by facilitating the access to drug and medical information,14,21 allowing NSs to access information more quickly15,21 and making the work of NSs more effective, as well as increasing their learning.15–19,21,22 The mobile device is regarded to improve patient safety and quality of care, and the encounter with the patient becomes more complete as the NSs do not have to leave their patients to look up information.21,22
In recent years, the technologies regarding hardware platforms, software and connectivity 23 have been changing rapidly, and smartphones have revolutionized what you can do with a mobile device. 24 In Sweden, today, a total of 89 per cent of the population (over 18 years) has access to the Internet. Furthermore, the mobile connection to the Internet has doubled in the past 2 years, and 55 per cent of the Swedish population is currently using the Internet via AMDs such as smartphones or tablets. 25 Based on the advantages we have found in previous studies of using mobile devices, and considering the development and availability of advanced mobile technology, it is obvious that RNs and NSs should have the possibility of accessing all of the information they need, independent of time and place. The National High-Level Group for eHealth 26 states that health-care personnel must have access to necessary information and must have effective and collaborative ICT support to facilitate their daily work and ensure high quality and safety. Despite this, AMDs are rarely used in nursing practice in Sweden.
There are a number of health-care software applications adapted for AMDs, but only few of these are adapted to Swedish conditions and nursing. To take advantage of mobile technology and to introduce AMDs in nursing care, it is important to secure an understanding of RNs’ and NSs’ views regarding the use of AMDs as a support in nursing, from a national perspective. This knowledge is important for decision-makers and developers in their efforts to meet the challenges of preparing future RNs and to continuously improve the quality and safety of health care. This study aims at describing the views of RNs and NSs regarding the use AMDs in nursing practice.
Method
A cross-sectional questionnaire 27 with a sample of RNs (attending graduate nursing programmes) and NSs was carried out, in May–June 2012, at two universities in Sweden.
Participants and process
All students attending the undergraduate and graduate nursing programmes, as well as those attending single courses during the spring term, were asked to participate in the study. The undergraduate nursing programme consists of six terms, while the graduate nursing programmes consist of two to three terms, including both theoretical and clinical courses. The single courses consist of 5–10 weeks of theoretical studies. A web-based questionnaire was distributed to all available email addresses in the universities’ administrative systems (N = 2057; Linnaeus University, n = 1074; Umeå University, n = 983) for the students registered on the programmes and courses during this term. In the email, together with a link to the questionnaire, participants received information about the purpose and the process of the study and their voluntary participation and were informed that all data would be handled anonymously. Participants who did not answer the questionnaire received two reminders, the first after 10 days and the second after another 10 days. Following the last reminder, there was an additional month to respond to the questionnaire. In total, 398 participants responded; consequently, the response rate was 19 per cent. The web-based questionnaire was conducted by using the Textalk Websurvey (Textalk, Mölndal, Sweden: https://websurvey.textalk.se/se/) programme. The first author (P.J.) received the email addresses from the administrators and created the questionnaire together with an ICT administrator. After this, the questionnaires and the reminders were automatically distributed to the participants by the Textalk Websurvey. It was not possible to identify the individuals making the responses, that is, the replies were anonymous.
Questionnaire
The questionnaire was developed for this study based on the questionnaire and results obtained from our previous research.20–22,28 Content validity 27 was established to test whether this new questionnaire had an appropriate sample of items and adequately covered the content of using AMD in nursing practice. A total of 48 NSs, who attended a course at a university, reviewed the new questionnaire during a class. Information was given to these individuals about the development of the questionnaire, including a request for comments about the construction of the items, choice of words and suggestions for changes. Then, the number of questions was reduced, certain questions were rephrased and the response alternatives were determined to comprise a 4-point scale. To test whether the questionnaire would measure what it was supposed to measure, face validity 27 was established. Nine academic faculty members and doctoral and master students with expertise in eHealth and/or nursing research and education were invited to review the questionnaire in its web-based form. Except for certain comments about minor changes, all agreed that the questionnaire was relevant in terms of exploring the views of using AMD in nursing practice. In addition to the demographic characteristics, the questionnaire included 7 questions about participants’ views regarding the current situation in terms of access to information and documentation: there were 3 questions with different alternatives for a reply and 4 with a 4-point scale. In addition, there were 21 questions about using an AMD in encounters with patients and relatives, as well as about the general usefulness of AMD with a 4-point scale for replying to these 21 questions. The 4-point scale response alternatives were from ‘totally disagree’ to ‘totally agree’. This limited number of alternatives was chosen as we wanted the participants to express a specific view, either positive or negative. 29 Furthermore, there was an alternative for ‘do not know’. There was also space for the participants’ comments.
Data analysis
Descriptive statistics were applied and the data were analysed using the Statistical Package for the Social Sciences (SPSS) for Windows, version 20.0.0 (IBM SPSS Statistics 20. United States). In the text, the percentages presented are taken from the 4-point scales (1 = totally disagree, 2 = partly disagree, 3 = partly agree, 4 = totally agree) as ‘disagree’ (grades 1–2) and ‘agree’ (grades 3–4). A compilation of the percentages, frequencies (n) and median (md) are presented in table form. Participants’ own comments were summarized and presented in text.
Ethical considerations
This study received approval from the Head of the School of Health and Caring Sciences, Linnaeus University and the Department of Nursing, Umeå University. The ethical considerations were made on the basis of the guidelines from the Ethics Committee of South-East Sweden.
Results
Demography
The participants (N = 398) were RNs attending graduate nursing programmes (n = 95) and single nursing courses (n = 16) and NSs attending the undergraduate nursing programmes (n = 287), 67 males and 331 females. The RNs were aged between 24 and 56 years (m = 34.7, standard deviation (SD) = ±8.0), had been RNs for 1–34 years (m = 7.4, SD = ±6.4) and worked in hospital wards (n = 46), emergency departments (n = 5), ambulance services (n = 15), operation theatre, anaesthesia units, intensive care, radiotherapy or delivery departments (n = 11), non-institutional care (n = 17), sheltered accommodations (n = 7), home care (n = 5), care hygiene (n = 1) and parental leave (n = 1); three RNs were no longer working in health care. The NSs were aged between 19 and 54 years (m = 25.8, SD = ±5.6), had previously been trained (n = 98) and had worked (n = 178) as an assistant nurse before they started their undergraduate nursing programmes. The participants estimated their level of computer skills as good (RN: n = 87; NS: n = 246), medium (RN: n = 24; NS: n = 38) or poor (RN: n = 0; NS: n = 3). In total, 294 participants were using an AMD in their private lives, and 94 were using an AMD in nursing practice (Table 1).
Participants’ (n = 398) demographic data.
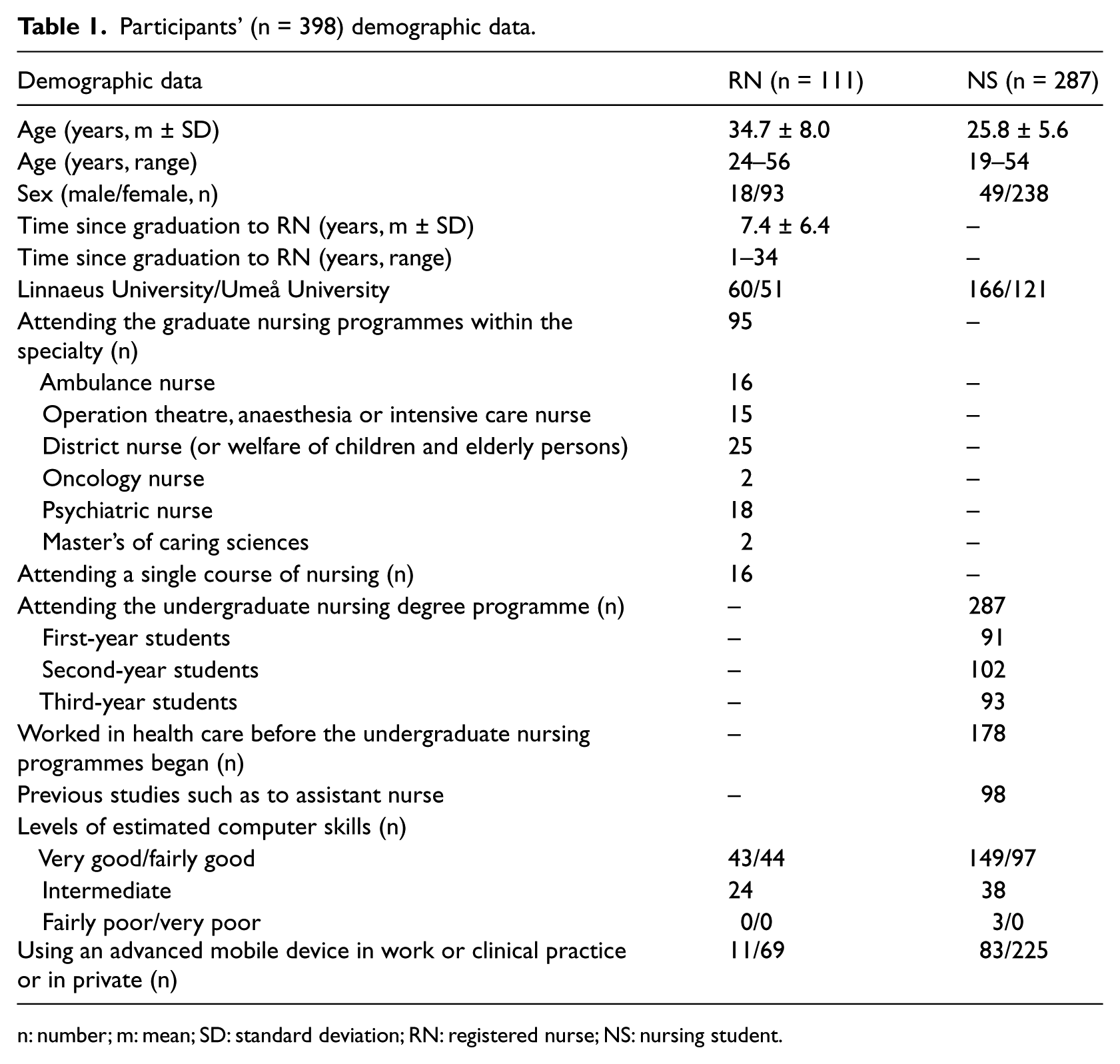
n: number; m: mean; SD: standard deviation; RN: registered nurse; NS: nursing student.
Current access to information and documentation
When asking about the participants’ views concerning access to information in their current work situation and/or in clinical practice, the majority stated that they usually had sufficient access to information to carry out their duties in a satisfactory manner (RN = 77%, NS = 70%), and slightly more than half of the participants stated that the information was easily available (RN = 62%, NS = 59%). To obtain access to information, the participants used Internet or Intranet (RN = 3%, NS = 5%) in combination with books, discussions with colleagues (RN = 5%, NS = 26%) and paper-based guidelines (RN = 95%, NS = 64%); some used paper-based guidelines, books and discussions with colleagues but not in combination with Internet or Intranet (RN = 6%, NS = 5%). The participants stated that they had occasionally (RN = 47%, NS = 47%) or several times (RN = 42%, NS = 21%) been in situations at point-of-care where decisions had been required to be taken based on deficient information, knowledge or experience. Nearly half of the participants (RN = 43%, NS = 48%) found that there is a lot of information available on the Internet but that it is difficult to determine which information is reliable. The participants made their notes on scraps of paper and in notebooks (RN = 63%, NS = 67%) in combination with writing in calendars (RN = 28%, NS = 19%); a few made their notes in AMDs (RN = 2%, NS = 1%) and in AMDs in combination with notes on scraps of paper (RN = 7%, NS = 14%). The majority considered the handling of their written notes to be reliable (RN = 82%, NS = 68%) (Table 2).
The registered nurses’ (RNs, n = 111) and nursing students’ (NSs, n = 287) views on current access to information and documentation and on using an advanced mobile device (AMD; smartphones or tablets) in the encounter with patients and relatives.
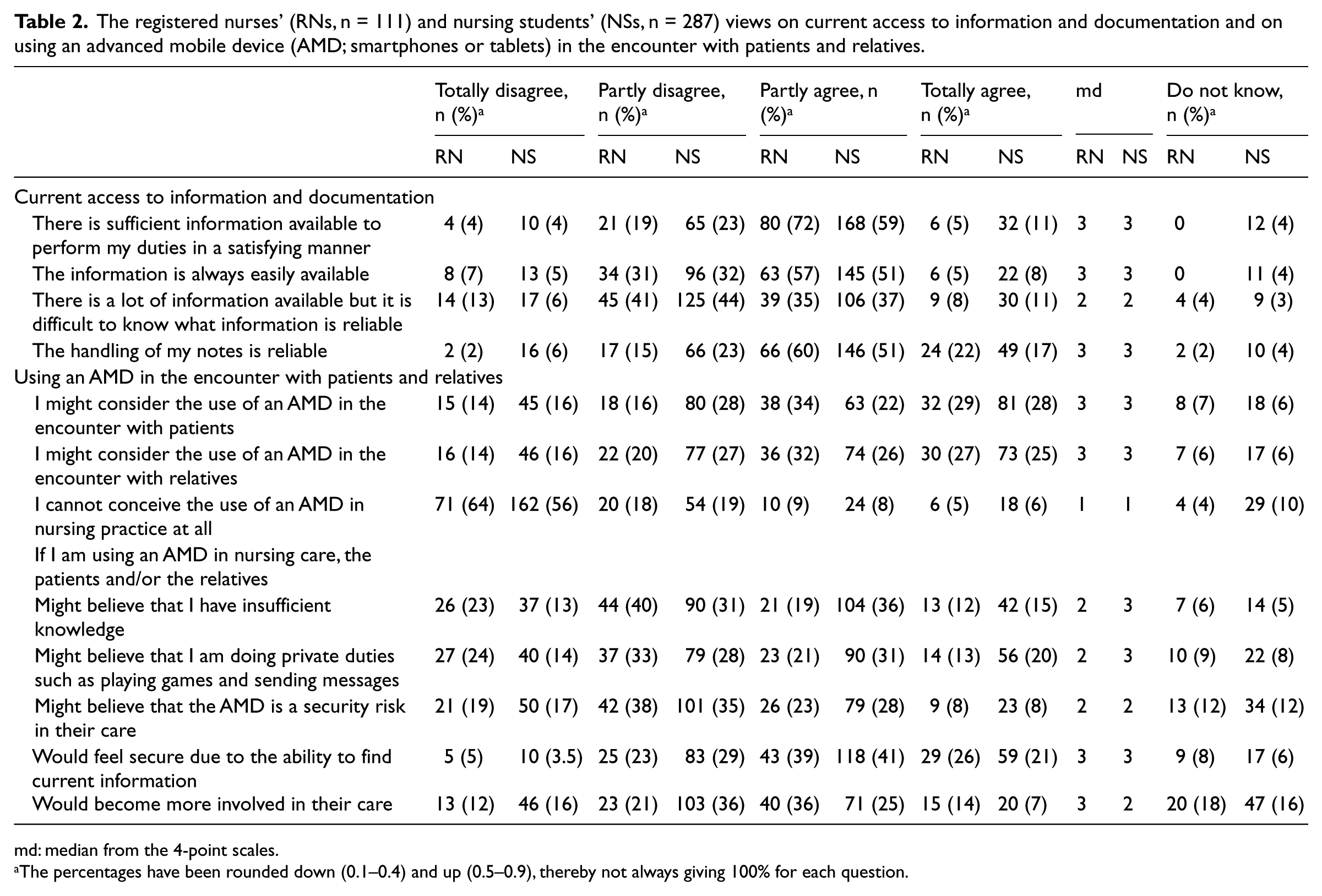
md: median from the 4-point scales.
The percentages have been rounded down (0.1–0.4) and up (0.5–0.9), thereby not always giving 100% for each question.
Using an AMD in encounters with patients and relatives
Approximately half of the participants (RN = 63%, NS = 50%) considered using an AMD in their encounter with patients and relatives, whereas 14 per cent could not conceive of using an AMD in nursing practice, at all. If they would use an AMD in nursing, slightly more than half of the RNs (65%) and NSs (62%) believed that patients and relatives would feel secure due to the ability to find current information and that patients and relatives would become more involved in the health care. However, if the RNs and NSs were using an AMD in nursing care, some imagined that patients and relatives might believe that they, the RNs and NSs, had insufficient knowledge (RN = 31%, NS = 51%) or were playing games and sending messages (RN = 34%, NS = 51%). Certain RNs (31%) and NSs (36%) also stated that patients and relatives might believe that an AMD could comprise a security risk in their health care (Table 2).
Usefulness
The majority (70%–82%) regarded an AMD to be useful in nursing practice in terms of accessing necessary information and handling notes in a reliable manner. The majority (66%–77%) regarded an AMD to increase confidence, save time and contribute to improving patient safety and quality of care resulting in a more complete encounter with the patient. Half of the participants expressed that an AMD might decrease stress and be a useful tool in communicating with colleagues. About half of the RNs (51%) and 72 per cent of the NSs believed that an AMD could facilitate their scheduling and could remind them of the duties or work they should do during a given workday (RN = 53%, NS = 77%). The majority (RN = 66%, NS = 70%) wanted to have an AMD in their forthcoming work (Table 3).
The registered nurses’ (RNs, n = 111) and nursing students’ (NSs, n = 287) views of usefulness of an advanced mobile device (AMD; smartphones or tablets).
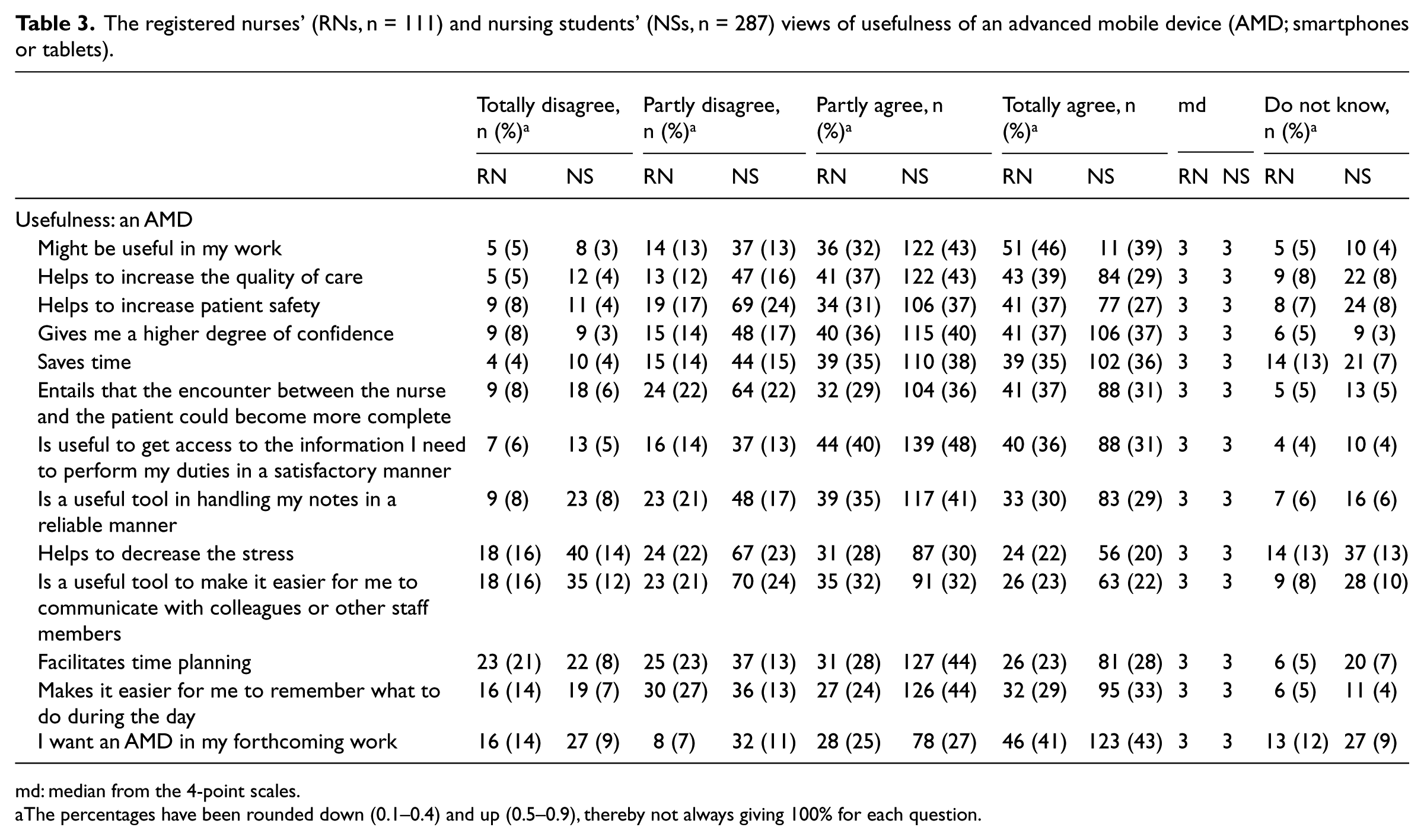
md: median from the 4-point scales.
The percentages have been rounded down (0.1–0.4) and up (0.5–0.9), thereby not always giving 100% for each question.
Diverse views of respondents to the open-ended questions
There were few comments on the open-ended questions, for example, about the current lack of access to accurate information. There is no time to search for information, instead, you are asking other personnel or try to act on what you already know; also, access to the patient’s health record is a requirement. On the contrary, one participant stated that there is a risk that too much available information could ‘drain the human brain’ as you do not need to train your memory, resulting in uncertainty and the possibility that there will be a decreased interest in learning.
An AMD is useful for mobile access to information and documenting on the go and to replace paper-based documentation. Compared to loose scraps of paper, an AMD would facilitate note-taking, and the notes can be saved in one place and protected from being read by others. Furthermore, an AMD could reveal advantages in terms of patient encounter, but it is important to explain to the patients why the AMD is being used. On the contrary, some participants doubted the use of an AMD in their encounter with patients because the focus on the patient might deteriorate, and the encounter might be interrupted.
In addition, an AMD might be a useful tool to use as a translator when communicating with patients speaking a foreign language, for taking photos to document wounds, for patient education, to locate patients’ addresses by using the Global Positioning System (GPS) and to facilitate communication between personnel as all personnel are equipped with a cell phone.
Discussion
This study aimed to describe the views of RNs and NSs with regard to the use of AMDs in nursing practice. The majority of the RNs and NSs regarded an AMD to be a useful tool in nursing practice to improve patient safety and the quality of care and to increase confidence. During the years 2006–2008, when we conducted our previous studies,20–22,28 desktop computers and some laptops were being used in health care, and the electronic health record was being introduced. Some personnel used cell phones, but there were only a few who knew about mobile devices. Since then, the technology has developed rapidly,23,24 and to handle the expanding knowledge base in nursing care,1,26 we believe it is necessary to improve the use of mobile technology in nursing practice. In this study, one-fourth of the participants were using AMDs in their work or clinical practice, which indicates that the use has increased. It seems that the use of AMDs is more due to the individual’s, RN’s or NS’s own sense of responsibility to support nursing practice than being a result of policies or practices implemented by nursing management.
In this study, required information was usually accessible and the majority of the participants obtained information via Internet or Intranet. However, it is notable that paper-based guidelines are, still, widely used in nursing practice and that some personnel rely only on paper-based guidelines, books and discussions with colleagues and do not use Internet or Intranet, at all. An AMD must be seen as a suitable replacement for the paper-based information, which might be out of date. Admittedly, it seems difficult to determine which information on the Internet or Intranet is reliable. Consequently, a national ehealth library with compiled verified and evidence-based information30,31 is a necessity. Furthermore, it is not uncommon, but alarming, that a large number of RNs make decisions with a lack of access to information, evidence, knowledge or experience. This jeopardizes patient safety, and personnel cannot be expected to fulfil the intention of the laws regarding safety and quality of care32,33 without proper access to information. No one should work under such conditions as advanced mobile technology is available and can help to counteract this risk.
More than half of the participants might consider the use of an AMD in their encounter with patients and relatives, but there were also a few critical voices against the use of an AMD in these situations. It seems that AMDs are taken for granted in peoples’ private lives but not in the context of nursing care. In general, the current technology is frequently used in other categories of work activities as well as in peoples’ private lives, and more than half of the Swedish population is connected to the Internet via AMDs. 25 This implies that not only health-care professionals benefit from the increasing amount of information but patients also have access to appropriate health-related information via the Internet. 1 This implies that patients are much more updated than ever and have higher expectations on their health-care provider. 34 Since technology is so common in health care, as well as in our everyday lives, patients and their relatives might regard it as very natural for RNs to use AMDs in patient–nurse encounters. The relationships with patients and relatives are of indispensable value and the role of the RNs can never be substituted by technology; 35 technology should be a support and not an obstacle.
Nursing practice is information intensive 36 and is in continuous change with increasing requirements on quality, cost and knowledge, 37 resulting in high demands on the nursing profession. An AMD could constantly supply RNs with the latest information, and by using an AMD, patient safety and quality of care might increase. Our results indicate that an AMD might be a support for RNs to uphold their responsibilities regarding the manner in which their work is performed. Half of the participants considered that an AMD might decrease stress. Newly graduated nurses are more likely to experience stress as they are novices and fear making mistakes while being expected to assume full responsibility for patients.38,39 NSs need rules and guidelines for support in their work, whereas RNs can rely on their experience.40,41 However, experienced RNs also need to continuously update their knowledge; RNs can also act and feel like a novice if they end up in a new clinical environment. 40 Teaching authorities must prepare students with the skills and competencies needed to meet current and future work requirements. 37 Today, instant and rapid learning are new pedagogical approaches and these should be considered. You learn all the time, and lifelong learning has come to stay.
A total sample selection from only two universities and a response rate of 19 per cent represented a limitation in the study. Consequently, the results should be interpreted with some caution. A web-based questionnaire is easy to use to reach many participants but often turns out to give a lower response rate than questionnaires delivered by mail. 27 It must be observed that the questionnaire was distributed to all available email addresses in the system, which is not in line with the actual number of students as many email addresses are not valid. The questionnaire was also sent out at the end of the spring term with students having their final exams and graduation, and some single courses had been completed earlier in the term, probably also contributing to the low response rate. Furthermore, there might be a certain lack of interest in responding to questionnaires in today’s society 42 due to information overflow, among other things. However, a descriptive design was, according to Polit and Beck, 27 considered as appropriate when the participants’ views of AMDs were to be captured. The questionnaires were distributed to participants when they were attending a programme or a single course at the universities, but the majority had clinical experience and were in a clinical environment during or shortly before or after the survey. In total, 398 participants responded, giving a moderate sample size, with a proportionately even distribution of the participants between the two universities. The questionnaire was developed from previous research; content and face validity were established. Consequently, we regarded the results of our study as being useful in describing RNs’ and NSs’ views of the application of AMDs in nursing practice.
Conclusion
We found that the majority of the RNs and NSs regarded an AMD to be a useful tool in nursing practice to improve patient safety and quality of care and to increase confidence. Although AMDs have been immensely developed and many participants are using them privately, the ‘acceptance’ in the nursing context was diverse. The National High-Level Group for eHealth states that health-care personnel must have access to the necessary information and must have effective and collaborative ICT support to facilitate their daily work and ensure high quality and safety. An AMD might be a useful tool in this context, and we believe that it is important to facilitate the use of AMDs to support nursing practice. Our findings might help decision-makers and developers to meet the challenges of preparing future health-care practices to use AMDs.
Footnotes
Acknowledgements
We thank the participants and the following individuals: Peter Diedrichs (ICT and Pedagogy Developer at the School of Health and Caring Sciences, Linnaeus University) for assistance with the questionnaire and Anders Ringnér (RN, PhD student, Department of Nursing, Umeå University) for assistance with email addresses and distribution of information at Umeå University. All authors were responsible for the study design. P.J. and G.N. were responsible for the data collection. P.J. was responsible for the analysis and writing of the article, supervised by G.N., B.-I.S. and G.P.
Declaration of conflicting interests
None exist.
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.