
Abstract
Implementation of e-health in mental health services requires that we are aware of stakeholders’ concerns. We ascertained the views of mental health professionals and mental health service users through the (1) development of 12 topics based on the research literature, (2) presentation to 31 participants (19 mental health professionals and 12 mental health service users) and discussion in three 1-week programmes, (3) thematic analysis of transcripts, and (4) comparison with the literature to identify areas requiring attention in e-health implementation. This method of engaging mental health service users and mental health professionals was effective. We identified areas that (1) should be the first to implement (e.g. discussion forums, email, and Skype), (2) where further education and engagement are necessary before e-health methods could be used (e.g. unsupported computerised cognitive behavioural therapy, computer–patient interviewing, and patient access to online medical records), and (3) for further research (e.g. the impact of bad online experiences).
Background
E-health innovations have been effective in trials but, like other health service innovations, this has not always led to wider implementation. Implementation of e-health services requires consideration of local circumstances and the views of relevant stakeholders. 1
All methods of obtaining stakeholders’ views have limitations. Interviews are expensive and lack the debate engendered within groups. Face-to-face focus groups may present practical difficulties in organisation, and some participants, particularly if a mix of service users and professionals, may feel inhibited to contribute. Online focus groups, where service users and professionals can discuss issues in a structured anonymous environment, may be cost-effective.
In this study, we aimed to (1) educate mental health stakeholders and (2) identify their concerns over e-health services. We were successful in getting comprehensive discussion between mental health service users (MHSUs) and mental health professionals (MHPs) on given topics. The pilot study of recruitment, engagement, and possible impact on participants is described elsewhere. 2 This article describes views expressed by stakeholders and exemplifies how we might compare with published research and identify areas for further research or stakeholder education prior to implementing e-health services.
Methods
Ethics
This study was reviewed and approved by the South West 2 Research Ethics Committee of the National Health Service (NHS) (Ref: 10-H0206-38).
Design
There were four stages, as follows: (1) development of 12 topics for discussion, (2) recruitment of stakeholders and three 1-week ‘courses’ in which participants discussed topics online, (3) thematic analysis of the discussion transcripts, and (4) comparison with the literature.
Topics for discussion
We developed discussion schedules selecting topics from a rapid review of the literature 3 relevant to mental health practice. Examples of research findings were included in the introductory webcast or in later discussion. The 12 topics were as follows: (1) computerised cognitive behavioural therapy (CCBT) for depression,4–9 (2) discussion forums, 10 (3) lifestyle change intervention websites,11–13 (4) webcast group therapy,14,15 (5) videophone, (6) email,16–19 (7) computer–patient interviews, 20 (8) Map of Medicine, 21 (9) patient access to their online medical records,22–24 (10) barriers to greater use of the Internet in mental health,25,26 (11) groups who would benefit from the Internet, and (12) implementation and requirements for supporting the Internet uses.
Recruitment and online discussion
The target population was MHPs interested in learning more about e-health services and MHSUs with experience of the Internet use in their mental health care. Potential participants were invited to visit the project website where they could learn more about this study, consent, and register online.
Each course ran for 1 week starting with a 1-h evening live interactive webcast 27 presented by a MHP and the project lead. A PowerPoint presentation was used to describe successful uses of the Internet for mental health, with breaks for participant discussion. The first five discussion topics were introduced in this webcast.
After the initial webcast, a discussion forum was available 24/7 via the project website. Webcast topics and chat transcripts were posted to the forum for continued discussion. On the final day of the course, participants were invited to another 1-h live interactive webcast, were presented with summaries of the week’s topic discussions, and introduced to the remaining topics.
Thematic analysis and comparison with the literature
Each topic within discussion transcripts was thematically analysed using the approach of Braun and Clarke. 28 E.A. read the transcripts to gain a sense of discussion flow, patterns, and recurring themes. Quotes were numerically coded, and summary notes were made in the margins, which were then extracted and arranged and grouped by common meanings. Themes began to be defined, and quotes, noting whether MHSU or MHP, were then re-examined, reviewed, and rearranged for appropriateness of thematic categorisation by both the authors. Both the authors compared themes from the stakeholder discussion with the initial and a further literature review to seek evidence to support or refute stakeholder claims. We identified issues raised by stakeholders, which contrasted with the literature, as well as issues that were concordant but that seemed important and of concern in implementing e-health services.
Results and discussion
Participant characteristics
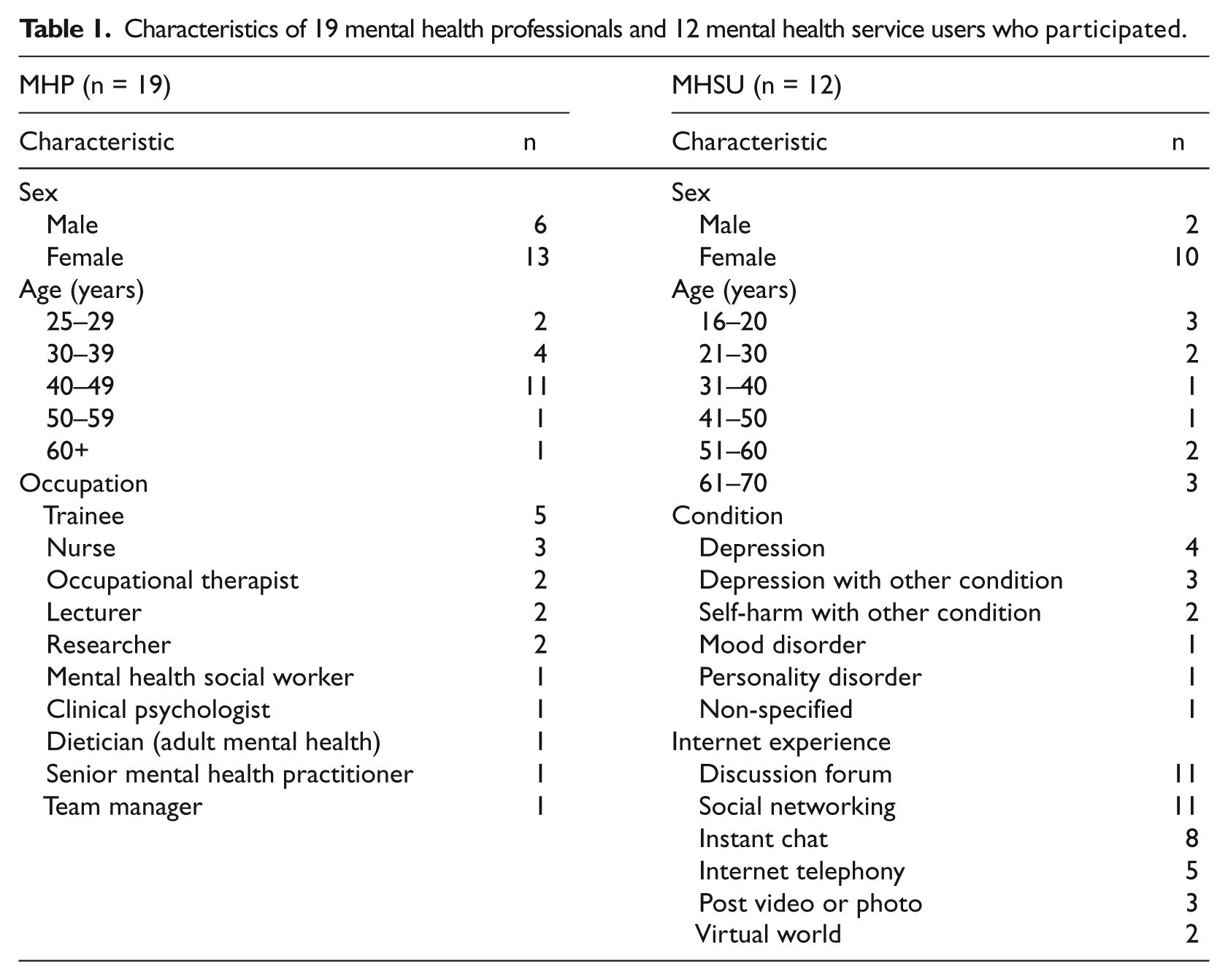
Nineteen MHPs and 12 MHSUs participated. Four MHSUs participated in more than one course. MHSUs were predominantly female (10 women and 2 men) but all with age of under 20 years to over 60 years. There were more female MHPs than male MHPs (13 vs 6) with modal age of 40–49 years (Table 1). 2 Contributions to each topic ranged from few (4/31 participants discussed Map of Medicine) to many (29/31 participants discussed Skype).
Characteristics of 19 mental health professionals and 12 mental health service users who participated.
Participant views of e-health services
Thematic analysis is presented within each discussion topic and includes comparison with the literature. Selected quotes are presented verbatim as figures (usernames have been changed for additional anonymity). We have not compared MHSU with MHP views in this article but presented elsewhere a discourse analysis of their interaction. 29
CCBT for depression
CCBT was introduced in the context of websites such as Moodgym7,30 and Living Life to the Full 8 and its use for people with depression or anxiety. The following six themes arose from the discussion: (1) Support: Concerns of CCBT usage without professional support and guidance; (2) Online therapy range: A need for choice of online therapy types, not just cognitive behavioural therapy (CBT) online; (3) Individual differences: No clear guidance on which patients CCBT might benefit; (4) Severity: CCBT should be aimed at mild-to-moderate severity; (5) Usability: A need for more user-friendly CCBT websites; and (6) Access: Concerns, common to all discussion topics, about exclusion of those without Internet access.
Generally, the literature suggests that although supported CCBT has better impact than unsupported CCBT (e.g. effect size of 0.6 vs 0.2 9 ), unsupported CCBT was nevertheless effective and worth recommending when other services were unavailable. 31 However, among our stakeholders while some expressed views supporting that position, others disagreed. One MHP expressed concern that more harm could come from a negative CCBT experience without support than not offering it at all (Figure 1) and a MHSU likened it to offering unsupported antidepressants.
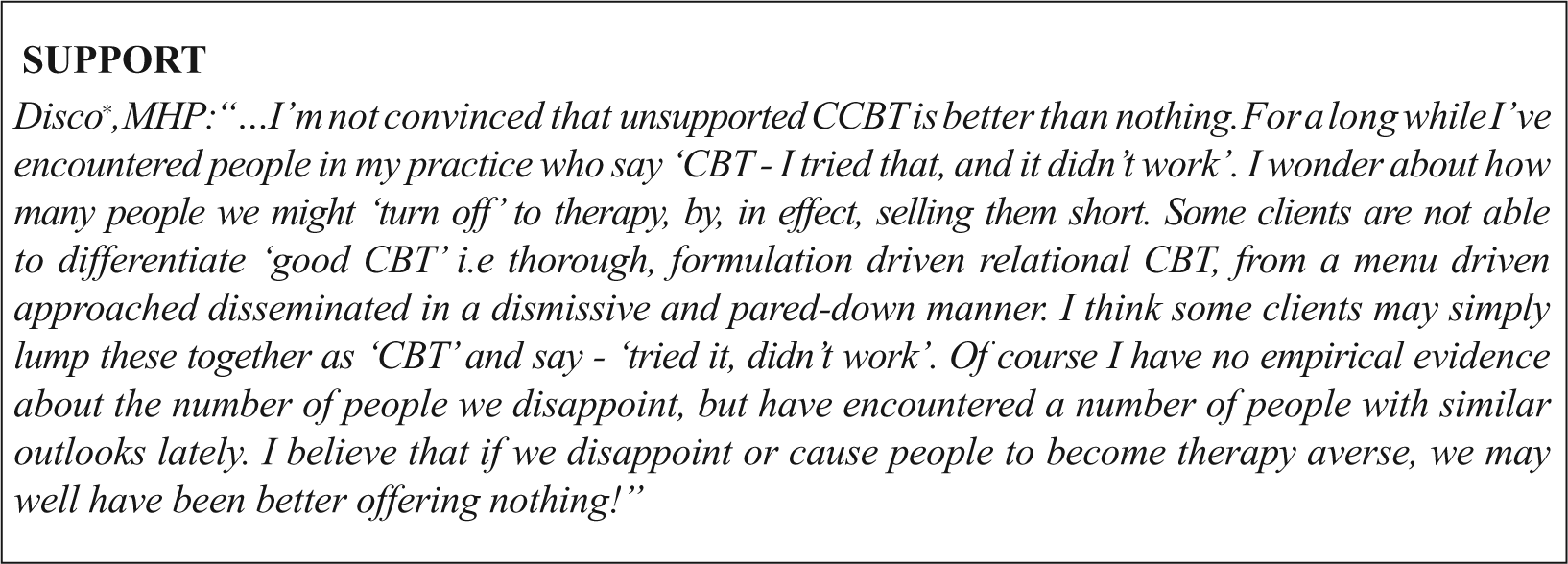
Stakeholders’ views on support for CCBT.
E-health research has tended to focus on CCBT. For example, a 12-study meta-analysis 9 found no differences between CBT oriented and other forms of computerised treatments, but the studies were mainly CCBT so the comparison was unbalanced and the evidence was weak. Some MHPs suggested that CCBT should be one of a range of options, and that other approaches, such as transactional analysis, 32 rational emotive behaviour therapy, 33 and solution-focused brief therapy, 34 should be available online. Individual differences and negative experiences of two MHSUs supported the need for other options and for research into which therapies might work for different patients.
Most research into CCBT,9,35 and National Institute for Health and Clinical Excellence (NICE) guidelines,4,5 recommends its use for mild-to-moderate severity and both MHPs and MHSUs agreed. Some MHSUs and MHPs reported experiences of poor interaction with CCBT, finding it awkward to use, impersonal, complex to navigate, and not user-friendly. Rates of attrition from studies of CCBT (as with other online treatments) can be high,13,36,37 and although motivation and supported use may be part of the answer, more study may be needed on interface design.
Discussion forums
Numerous discussion forums for mental health exist,38,39 and most MHSUs and some MHPs reported prior use. Stakeholder views on forums were mixed; benefits and disadvantages were raised under each of the following eight themes identified: (1) Support: Forums may provide mutual support or add to feelings of loneliness and lack of support (Figure 2); (2) Social contact: Forums may provide or reduce social contact and inclusion; (3) Timing: Forums may be useful at certain stages of treatment and condition but not others; (4) Size: Forums may be easier to find and get responses if large, but be more personal if small; (5) Anonymity: Forums make it easier to share information because of anonymity but may lead to disinhibited, irresponsible, and unhelpful posts by some; (6) Moderation: Forums need to be moderated; (7) Recommendation: Forums could be recommended by MHPs but there were mixed views about MHP involvement in forum discussions; and (8) Style of communication: Forums may be useful for MHSUs who prefer written communication rather than verbal communication.
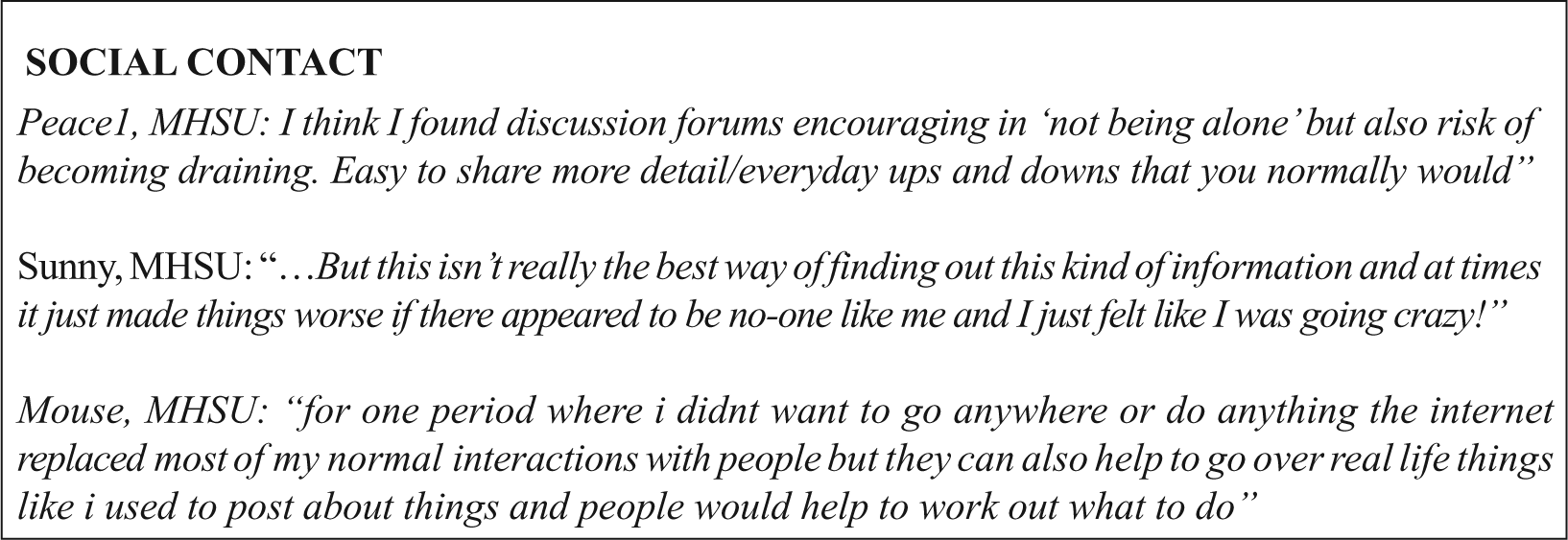
Stakeholders’ views on social contact and discussion forums.
How do stakeholders’ views compare to the literature? Research evidence on the benefits of online peer–peer support is also mixed, often complicated by being part of other interventions 40 or using methods that may be inappropriate. 41 There seem to be studies supporting most of the stakeholders’ views: (1) Forums may provide mutual support 42 or greater satisfaction, 43 and others found no evidence of increased social support.40,44 Some studies report negative experiences.45,46 (2) Others suggest that expressing emotions and developing social relationships online is an unmeasured benefit of empowerment, but this online empowerment can cause distancing from face-to-face communications. 47 (3) We found no studies of when, in the course of someone’s condition, membership of a forum would be most useful. (4) The need to get forum size ‘right’ has been reported. 42 Forums that are too small ‘die’ through lack of interaction, but small forums can be more personal. (5) Without anonymity, many people would not make use of discussion forums for mental health purposes. 42 However, anonymity may lead to deception. 48 Barak et al. 47 suggest that online disinhibition can not only facilitate more open and honest discussions offering therapeutic benefits but also may lead to criticisms of others and rude behaviour. (6) In some studies, unmoderated forums had no improvement in well-being, 44 and others found positive effects. 43 We found no studies directly comparing the effects of unmoderated and moderated forums. (7) In some studies, clinicians recommended websites,49,50 but we have not found mental health studies. Professional involvement changes the nature of forums, for example, reducing emotional and self-disclosure contributions 51 but may have positive impact with users asking more questions and professionals guiding more constructive discussions such as facilitators for change. 52 (8) Users may prefer to type, finding discussing issues on the phone difficult. 42
Lifestyle change intervention websites
There are many lifestyle change websites including those aiming to reduce drinking levels,12,13 increase exercise, 52 lose weight, 53 and quit smoking. 54 There is evidence that such programmes may result in improved short-term understanding, lead to improved diet, tobacco and alcohol abuse, and sexual behaviour. For example, undergraduate students with harmful levels of alcohol consumption allocated to use a website had lower alcohol consumption frequency and quantity at 6 months. 12 However, most studies are on too short a timescale to show improved health outcomes, or maintenance of changes in lifestyle. 3 We argued that such programmes were relevant as mental health problems often need to be considered in the context of lifestyle issues. Only one MHP indicated prior experience using such websites.
The following five themes were identified in the transcripts: (1) Motivation: Such websites are only useful for self-motivated patients; (2) Lack of human contact: Effectiveness may be limited because of the absence of important non-verbal communication and the social inclusion of face-to-face methods (Figure 3); (3) Professional role: In reviewing and recommending sites; (4) Self-assessment: Perhaps useful as a self-assessment tool, but some patients may not be truthful with themselves; and (5) Concern about cost cutting: Participants saw potential benefits for recommending moderated websites in addition to established mental health treatment but were concerned if the intention was to replace face-to-face methods.
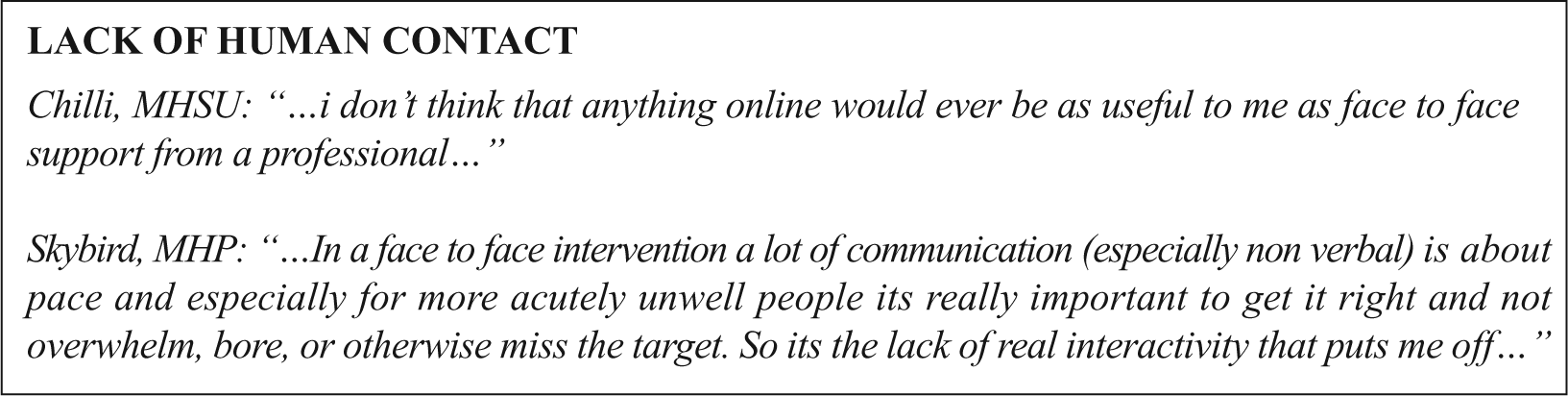
Stakeholders’ views on lack of human contact in lifestyle change websites.
Research supports some, but not all, of the following stakeholders’ views: (1) Those already motivated to change are more likely to use lifestyle change intervention websites than those who may have greater need of change. 55 (2) The need for some motivational support or human contact has been recognised for CCBT, and some have piloted ways of dealing with this online. 56 (3) In an Australian general practice, more than half the doctors recommended websites to their patients in the consultation, 50 whereas in Spain it was only 28 per cent. 49 (4) Most literature does not support the stakeholders’ views on truthfulness. For example, a meta-analysis found less social desirability distortion in computerised self-reporting of personal information such as illegal drug use than in face-to-face interviews, 57 suggesting computerised self-assessment may increase truthfulness in the absence of possible evaluation apprehension with face-to-face interviewing. (5) Finally, stakeholders’ concerns about ‘poorer services’ and cost cutting need to be carefully handled in any e-health implementation.
Webcast group therapy
We are not aware of prior research into webcast group therapy but as the technology we were using, it seemed appropriate to discuss its possible use. Unsurprisingly, no participant had prior experience of group therapy via webcast, and this was reflected in the uncertainty of whether it would work. The following four themes arose from the discussion: (1) Dislike of group therapy: Some would be willing to try webcasts but some MHSUs did not like group therapy, whether face-to-face or online; (2) Online skills: MHPs had concerns about their ability to manage a group online (Figure 4), dealing with the multiple tasks of presenting, reading comments, and replying, or the possibility of ‘structure’ including rules and turn taking; (3) Relationships: There were contrasting views on relationships with some MHPs concerned that online ‘distance’ between professional and patient and the loss of non-verbal communication would hinder relationship development. Another was concerned that anonymity would restrict any follow-up of distressed service users, whereas two MHSUs viewed the anonymity as reducing face-to-face anxieties; and (4) Therapy or education?: Rather than presenting the discussion topic as ‘therapy’, it may have been more appropriate to focus the idea on education or follow-up. Some MHPs suggested preference for delivering mental health education topics such as lifestyle change and condition education, rather than therapy. Others suggested group webcast therapy for additional care rather than in place of face-to-face care.
Stakeholders’ views on online skills and webcast group therapy.
The role of online anonymity has been discussed extensively 48 and is something that needs careful explanation when proposing new online services. We typically need to specify who is aware of identities rather than referring to anonymity as an overall state. For example, in these discussions, MHPs were not anonymous to us (the organisers) but were anonymous to each other. On the other hand, MHSUs were anonymous both to other participants and to us.
Videophone
We discussed videophone using the example of Skype (www.Skype.com) but did not present the research literature prior to discussion. Few MHSUs and some MHPs indicated prior Skype experience with friends and family; only one MHP had used Skype with patients. Some MHPs and MHSUs expressed an interest in using Skype for health care, and the other MHSUs did not. The following seven themes arose from the discussion: (1) Robustness of technology: Although some MHPs thought there was potential, there were concerns that the technology was not yet sufficiently reliable, suffering bandwidth, and connection disruptions, with restrictions particularly in some health-care settings. User adaptation to the technology was also an issue. A new technology known as Giraff, a mobile device that gives health professionals a videophone connection into a patient’s home was viewed by a few MHSUs as potentially beneficial but considered by a few MHPs as potentially difficult to adapt to using (Figure 5); (2) More choice for MHSUs: Video consultations were seen by some, both MHSUs and MHPs as offering an additional choice of contact; (3) Comparison with telephone: MHPs mostly preferred ordinary telephone to Skype for ease of use, and some viewed the addition of a picture as useful, but some disagreed; (4) Need for prior contact: Some thought Skype should not be used without prior face-to-face communication and felt that Skype lost some face-to-face information; (5) Benefit of the event: One MHSU reported greater benefits from the whole experience of attending an appointment rather than convenience of communication from home; (6) Cost and practical benefits: MHPs and a MHSU saw potential of using Skype in geographically remote areas, for immobile patients, and to save time and money; and (7) Patient state: Concern that if patients were ill at ease, they would be able to just walk away from the computer screen if uncomfortable during the session.
Stakeholders’ views on videophones.
Webcam appointments for people with diabetes are currently being trialled in Newham in London. 59 They are seen as a likely future development in mental health. 60 A study of working alliance between professional and patient found no significant differences between face-to-face and online therapy, 37 and a randomised clinical trial found that psychiatric treatment via videoconference was equally effective for patient clinical improvements as face-to-face treatments and suggested potential benefits for rural and remote patients. 61 Although not raised by our participants, patients and health-care professionals have expressed concerns about privacy and security. 62 These are being addressed by Skype, 63 and recommendations have been made to reduce risk. 64
We did not present any literature prior to discussion as all participants were familiar with email. Two MHSUs reported email experience with nurse and key worker, and none of our MHPs reported email experience with patients, but there was interest among both MHPs and MHSUs in using email for health care. Six themes arose from the discussion (Figure 6): (1) Convenience: Some MHSUs, including two from experience, viewed email as convenient for anytime access for non-intrusive communications. One MHP viewed emails as more likely to be replied to than missed calls; (2) Timing: Concern that email is not a fast response method for patients in crisis and should not be used as such. However, one MHP suggested email had potential for reflective group communications, that is, where the delayed response was useful; (3) Disinhibition: Two MHSUs viewed email as more effective for emotional expression and revelation than face-to-face; (4) Trust: Some thought email was helpful in conjunction with face-to-face care, and that prior face-to-face contact was needed to develop trust before email can be effective; (5) Printed record: Some MHPs reported potential benefits of recorded information for reflection, but they expressed concern for misinterpretation and effects of written text; and (6) Security: Two MHPs reported that they were personally prohibited from email communication with patients by health-care trust rules, and one MHSU viewed email as not secure and would not personally correspond by email even for appointments.
Stakeholders’ views on the use of email between patient and professional.
Considering that email has been available and used routinely for many years, and that Eysenbach reported on unsolicited emails in 2000, 65 it was surprising that there appears to be relatively little research published on routine use of email between patients and their providers. A US article 66 suggested that in 2005, few actually used email for this purpose having concerns such as the potential for increased workload for clinicians and privacy issues for patients.
Computer–patient interviews
Computer–patient interviewing (CPI) has been used for history taking in mental health since 1966. 67 Branching series of questions are developed to assist medical history taking by clinicians. Standard questions are used, with systems having hundreds of questions but patients only answering those relevant. Over 200 studies of CPI 20 have demonstrated benefits for patients including the following: (1) giving patients time to think about questions; (2) allowing patients to more easily disclose embarrassing information; and (3) ensuring lines of investigation are not forgotten, leading to more complete data and fewer diagnostic errors and better agreement between patient and doctor. An early US example was CPI for suicide risk prediction. 68 None of our participants had prior experience of CPI but some tried Instant Medical History (IMH) 69 available via a US practice website.
The following four themes arose from the discussion (Figure 7): (1) Quantity of questions: Some thought patients might lose motivation or feel overwhelmed by the number of questions; (2) Impersonal method: Concerns that the method of questioning may be impersonal, exacerbated by use of clinical language and restricted possible responses; (3) Support: Benefits of allowing patients to answer questions in their own time was recognised, but also concern that MHSUs would dislike completing questions without support and opportunity to discuss potentially upsetting questions with professionals; and (4) Screening and outcome measures: Participants thought that CPI could provide information for population screening.
Stakeholders’ views on computer-patient interviews.
Although it seems a legitimate concern that even though CPI is tailored to individuals, some patients feel overwhelmed by the number of questions, we found no articles with evidence of this happening. There is evidence that CPI can be therapeutic rather than impersonal, 70 and if the CPI design allows patients the opportunity to find out why questions are being asked, this might turn any sense of frustration with the number of questions to an opportunity for patient education. 71 Although some patients may view a computer as impersonal, studies have shown they may change that view after use;72,73 this will depend on the careful choice of questions. 74 CPI is usually used prior to consultations with clinicians so that they are able to discuss upsetting questions after use. 20 We are not aware of studies where it is used unsupported. CPI has, as stakeholders suggested, been used for population screening. 75
Map of medicine
Map of Medicine is an evidence-based online clinical knowledge resource, using a pathway approach to provide visual representations of evidence-based practice. 21 Only two MHPs had prior experience, commenting briefly on its helpfulness as a diagnostic tool, and two other comments from a MHP and MHSU indicated minimal knowledge of this tool; therefore, we were unable to establish themes from the stakeholder discussion.
Patient access to their online medical records
Patients in the United Kingdom can apply to access their records for a possible fee, 76 but some clinicians give their patients routine access, with examples in general practices, 77 diabetes, 78 and renal disease. 79 No participants had experience with online medical records. The following six themes arose from the discussion: (1) Security/privacy: MHSUs thought security and privacy were critical, particularly concerns about patients’ capability to implement the Internet security measures (Figure 8); (2) Reflection: Some MHPs suggested that online notes could be beneficial for patients to reflect on their treatment but some MHSUs thought personal reflection would lead to rumination and possible distress; (3) Support: Some thought that records should only be viewed with professional support to avoid upset, disappointment, and potential mistrust; (4) Empowerment: If access to records improved patient–professional communication, then it was welcomed. Some MHPs believed that shared medical record contributions between professional and patient would encourage patients to become active partners in their care; (5) Accessibility: There was some agreement that online records would improve patient accessibility to their notes, but one MHSU was concerned she or he would read too much into them; and (6) Unnecessary: Some MHSUs preferred face-to-face methods or the copying of letters so did not see the need for online methods. Some MHPs argued that it should not be at the expense of face-to-face methods.
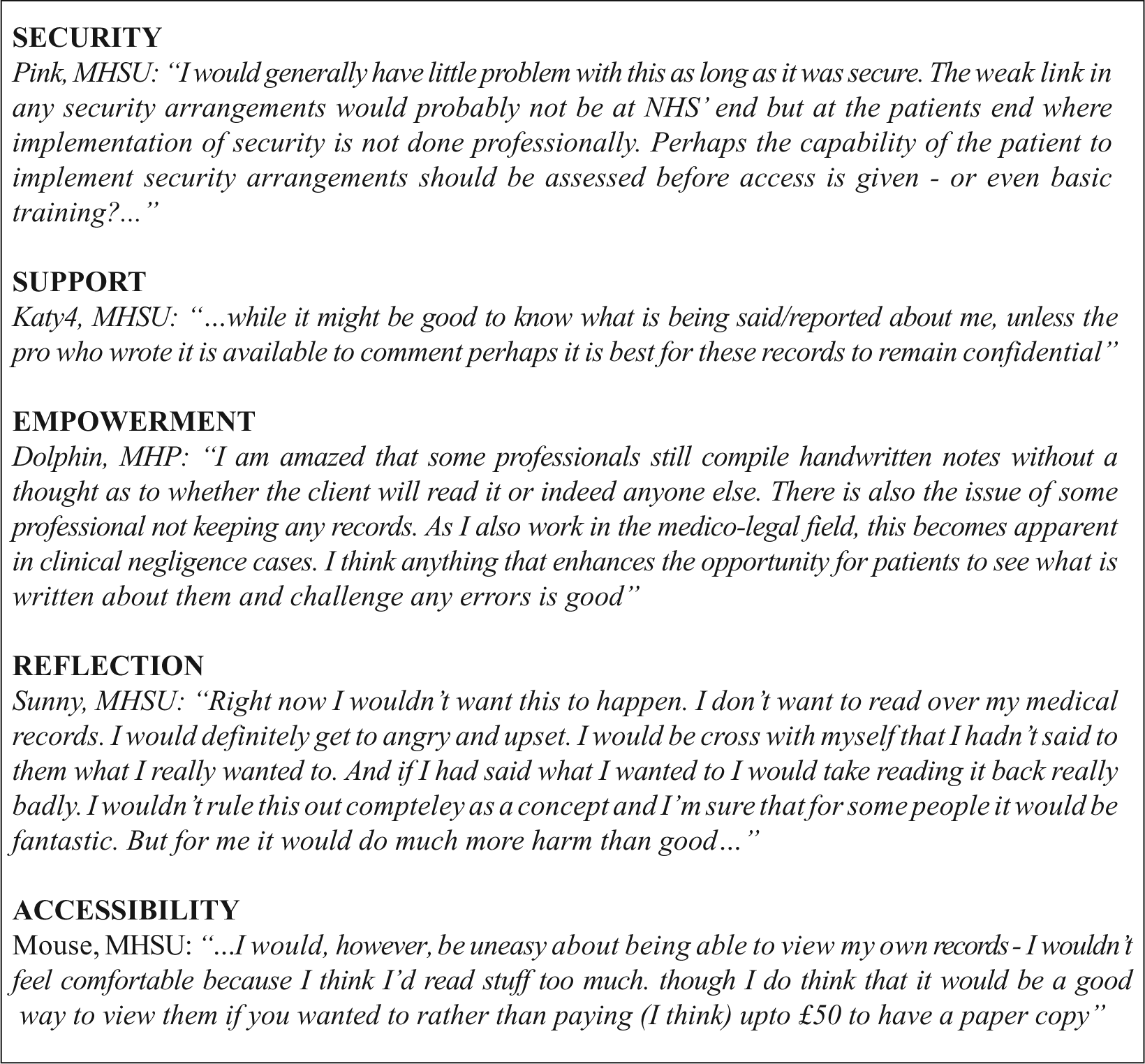
Stakeholders’ views on patient online access to their records.
Stakeholders’ wariness about patient online access to their records was at odds with the positive research evidence. Reviews have noted benefits including improved patient understanding, empowerment of patients, better clinical care, improved accuracy and completeness of records, better professional patient communication, patient satisfaction and outcomes, and improved adherence to lifestyle recommendations.22,80–82 However, stakeholders’ wariness was in accordance with concerns expressed in newspapers. 83 Compared to the banking sector where ‘scammers’ have major incentives, 84 most would argue that the rewards of medical data theft are fewer. We are unaware of studies or routine use of online records resulting in security issues. Those surveyed about the national summary care record thought that with security measures in place, personal health details were a low security risk compared to personal bank details. 85 Most professionals think that patients discovering a diagnosis for the first time on reading a record would be damaging and care is needed to ensure that doctor and patient have had a chance to discuss record content before release.86,87
Barriers to greater use of the Internet in mental health
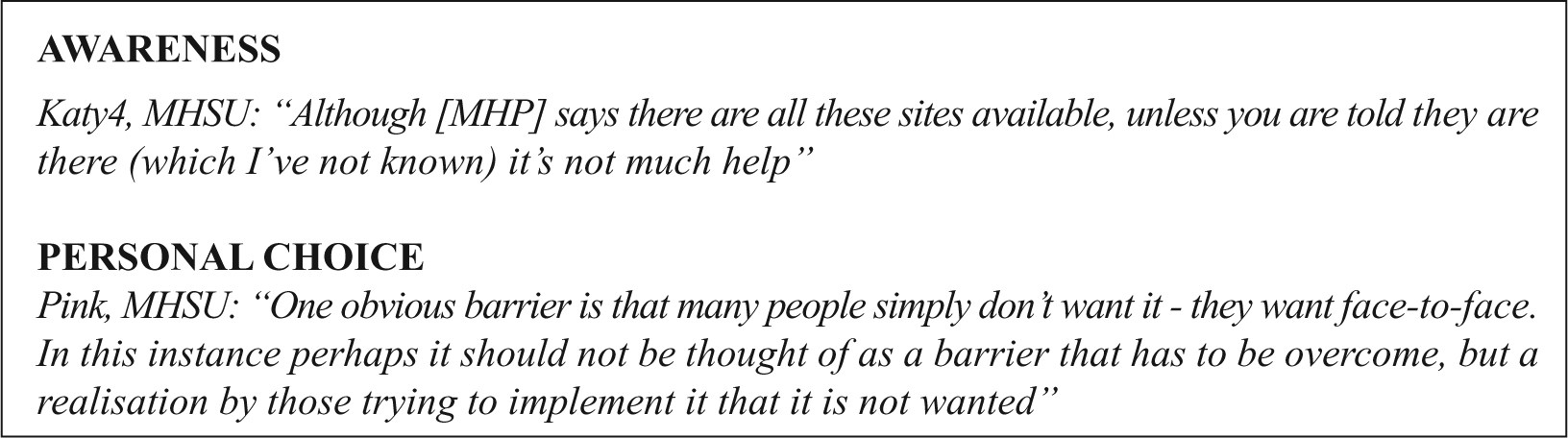
We did not present research data to introduce this topic as participants had already identified many. The following five themes arose from the discussion specifically on barriers and from earlier discussion: (1) Access: Concern about patients who were not confident computer users or who had no Internet connection was frequently raised. Patients with no personal Internet connection may find public access (e.g. libraries) unsuitable for mental health use; (2) Organisational support: MHPs said there was a need for the NHS to support the Internet use in practice, and that professionals’ ability to use technology varied greatly. Many commented on the frustrations of technical glitches; (3) Security: Concern for security was seen as a barrier to the Internet use, including NHS trust restrictions; (4) Awareness: MHSUs viewed lack of awareness of the Internet resources and lack of such provision as barriers (Figure 8); and (5) Personal choice and ability: Some may prefer face-to-face methods and will resist using the Internet. Older patients may not have the ability or confidence to use new technology.
These barriers have been identified in the literature and policy including access issues, 88 the need for organisational support and the need for training, 89 security concerns, lack of awareness of Internet resources, 90 and personal preference. 91
Groups who would benefit from the Internet
We did not present research data but asked if certain groups would benefit from the use of the Internet. The following five themes arose from the discussion: (1) Generalisation: Some thought there were too many individual factors to be able to generalise; (2) Physical restrictions to health care: It was thought that those with physical and psychological restrictions to health-care access, including those in rural communities, the disabled and those working anti-social hours may benefit; (3) Professionals: Two reasons were given why professionals may benefit, namely, (a) reduced costs and (b) being able to seek personal help anonymously (e.g. those suffering ‘burnout’ without risking their jobs); (4) Computer users: Groups who naturally turn to online resources for help were viewed as benefitting from the Internet but there were concerns that some may ‘need’ face-to-face contact; and (5) Initial stages: Different Internet uses at different stages were recognised, and it was thought that those in the initial stages of seeking help might benefit most.
There is research to support participants’ ideas. For example, those living in rural areas could benefit from reduced travel 87 but there may be problems with Internet connectivity. 92 The Internet can support people with disabilities 93 but disabilities may also present barriers to use. 94 Professionals have appreciated the anonymity afforded by the Internet use for mental health issues. 48 ‘Internet natives’ 95 are an obvious first group with which to explore e-health methods but some suggest that young people can become socially isolated by overuse. 46 Finally, there is evidence that information can be tailored to different stages in patients’ journeys, for example, for lifestyle change 96 or in uptake of screening. 97
Implementation and requirements for supporting Internet uses
Stakeholders discussed how they would like to see the Internet used in mental health services and what would be needed to support these uses. The following six themes arose from the discussion (Figure 9): (1) Supplement: Some wanted e-health services as additional resources, to complement and not replace face-to-face therapy; (2) Individual differences: The need to tailor services to individuals was stressed and concern that e-health methods might not be suitable for all MHSUs, but that, for example, younger people expected up-to-date use of technology; (3) Ideas for particular implementations: Participants had specific ideas including NHS-run discussion forums, peer support emails, computerised therapies other than CBT, and use of text reminders; (4) Research evidence: Participants recognised the need for evidence of comparisons between the effectiveness of the Internet and face-to-face methods; (5) Training and guidelines: Training and guidelines were needed for implementing e-health methods; and (6) Rationale: The way that uses of e-health were presented, that is, its underlying rationale, was important and might lead to opposition if presented as cost cutting rather than quality improvement.
Stakeholders’ views on the barriers to implementing e-health.
Conclusion
This study demonstrated that anonymous online discussion among MHSUs and MHPs can identify perceived barriers and benefits in implementing e-health services. These stakeholders identified some ‘easier wins’, areas where they were sceptical of the applicability of research, and areas where the benefits of e-health methods are not proven and more research is needed.
Easier wins
Stakeholder discussions identified areas where the benefits of e-health methods are fairly well accepted and where MHSUs might expect practitioners to be offering such services. Policymakers developing implementation plans should address these topics first. For example, giving both patients and professionals more choice in methods of communication was considered important, both between different online methods, and whether to use online or not. These methods will depend on the type and stage of treatment process. For example, discussion forums were considered by some users as good for initial exploration, email or Skype was considered useful when in an existing familiar relationship with professionals, and CCBT and lifestyle change websites were considered useful for aftercare beyond treatment plan. Implementation of these methods in agreed situations would likely get a programme of e-health methods started with support from stakeholders.
Education
There are areas where, despite research evidence showing benefit, stakeholders had continuing concerns. Implementing e-health methods in these situations would require a careful approach addressing stakeholder concerns. For example, the need for professional support was raised in topics such as CCBT, CPI, and online medical records. Although research shows benefits of, for example, open and unsupported access to records, these stakeholders were not convinced. Researchers need to find more effective arguments, or methods of dissemination to make the evidence from their studies more persuasive. Policymakers considering implementation would probably require further local evaluation before adopting these e-health services.
Research
This study identified areas where further research is needed. These included exploration of online alternatives to the CCBT approach such as transactional analysis, rational emotive behaviour therapy, and solution-focused brief therapy; better assessment of the impact of bad online experiences; when, in the course of someone’s condition, forum membership would be most useful; comparison of the effects of unmoderated and moderated forums; outcomes of routine use of email between patients and professionals, examining the effects of asynchronous communication on disinhibition and relationships; and exploration of webcast in comparison to face-to-face group therapy. Practitioners and service users need to be made aware that research evidence is not yet clear, and researchers could identify studies that could add to the evidence in these topics.
Ongoing education
E-health is a rapidly evolving area, and practitioners and policymakers will find it difficult to keep up-to-date. There is a role for methods such as this, using syntheses of the research literature in continuing professional development and providing a dialogue between the concerns of MHSUs and MHPs and researchers.
Limitations
One advantage of using online structured discussion was that it enabled discussion between MHSUs and MHPs that would have been difficult using other methods. The disadvantage is that participants were self-selected and may be more e-literate than average. However, most professionals were attending to find out about e-health. Other MHSUs and MHPs may be more apprehensive about using e-health. We pre-specified 12 discussion topics based on our literature review, and this may have limited the range of discussion. It meant that participants may not have directly experienced the e-health methods discussed, but as such, they will represent other ‘novices’ being asked to implement e-health methods.
Footnotes
Acknowledgements
The authors acknowledge Tobit Emmens, Research and Development Manager, Devon Partnership Trust, co-grant holder for the project; Dr Graham R. Williamson, Lecturer in Adult Nursing, co-grant holder for the project; and Jon Perry, Lecturer in Mental Health Nursing, who helped with some of the webcasts.
Declaration of conflicting interest
None.
Funding
This study was supported by the Devon Partnership Trust and the Technology Strategy Board via a shorter Knowledge Transfer Partnership.