
Abstract
The development of modern technology brings convenience to our lives but removes physical activity from our daily routines, thereby putting our lives at risk. Extended computer use may contribute to symptoms such as visual impairment and musculoskeletal disorders. To help reduce the risk of physical inactivity and promote healthier computer use, this study developed a time-scheduled delivery of health-related animations for users sitting in front of computers for prolonged periods. In addition, we examined the effects that the program had on the computer-related health behavior intentions and actions of participants. Two waves of questionnaires were implemented for data collection before and after intervention. The results showed that the animation program indeed had a positive effect on participants’ healthy computer use actions in terms of breathtaking, body massages, and body stretches. It also helped to bridge the intention–action gap of the health behaviors. The development and evaluation were documented, and users’ experiences/suggestions were discussed at the end.
Introduction
Computer and Internet use is becoming increasingly commonplace at home, in school, and at work nowadays. According to the European Working Conditions Observatory (EWCO), 53 percent of the active population in the EU15 used a computer for professional purposes. 1 The Eurostat also showed that in 2010, 64 percent of individuals surveyed across the EU27 had Internet access at home and 28 percent at work. 2 Incidentally, the Workplace Employee Relations Survey (WERS) reported that 75 percent of all workers in the United States used computers at work in 2004; the US Census Bureau reported that 68.7 percent of the households (78.2% of the population) had access to the Internet at home, and on average, the Internet users spent more than 3 h a day online. 3
The benefits of increased convenience, connectivity, and flexibility that the computer and Internet have brought to us are tremendous. However, these new technologies also add more stress and new demands to our lives. A population-based prevalence study showed that on average, children and adults in the United States spent 54.9 percent of their waking time, or 7 h and 42 min per day, in sedentary behaviors, or leading a sedentary lifestyle. 4 Moreover, along with advances in technology such as the Internet, home computing systems, and other telecommunication devices, telework (working with a personal computer away from the employer’s premises at least a quarter of the time) is becoming a new pattern of work in many countries. The Eurofound reported that in 2000, the overall average proportion of employees involved in telework was about 5.3 percent in the 15 EU Member States (EU15), and it had increased to 7 percent for the entire EU27 in 2005. 5 Teleworkers (mainly home-based workers) generally spent longer in sedentary work than their office-based colleagues. 6 For example, in the Netherlands, 44.7 percent of teleworkers or homeworkers perform sedentary work for between 6 and 8 h a day, compared with 30.4 percent among their nonhome-working counterparts. Moreover, 25 percent of these workers spent between 6 and 8 h a day working in the same posture, compared with 19 percent of their counterparts.
Extended computer use does not happen merely at the workplace. The adoption of computers in schools is proceeding apace. 7 Stanford University annual Student Computing Survey (2010–2011) reported that almost 100 percent of undergraduate students have their own computers, and most of them use their computers between 4 and 8 h a day, with 32 percent using them between 4 and 6 h a day, 32 percent between 6 and 8 h a day, and 18 percent more than 8 h a day. 8 The new generation of students entering college is most tech-savvy and have high levels of skill in areas of information technology. However, the health risks of prolonged sitting have gained researchers’ attention in recent years. It has been shown that extended computer use may contribute to symptoms of visual impairment (commonly dry eyes), musculoskeletal injuries (e.g. neck, shoulder, and low back pain), skin problems, and even emotional disorders. 9 Among the many possible causes of injuries, not taking regular breaks from computer work has been acknowledged as an important factor. 6
The numbers of users experiencing eye fatigue, pain or dryness, shoulder stiffness, and back and low back pain sharply increase due to different optical and physical characteristics between “computer displays and keyboards” and “paper and pencil.” 7 Compared to writing with pencil and paper, posture at the computer tends to be more tightly restrained and eye movement is busier. Sotoyama et al. 10 claimed that during upward gaze when working at computer, the ocular surface area, the surface area of the eyeball exposed to the air, increases and tears decrease. Therefore, as the use of computer technology becomes more pervasive, knowledge about the safety and comfort of computer use and regular ergonomic exercise deserves more attention, especially for the habitual computer users in the hope of decreasing the risk of computer-related injuries.11,12
Health promotion
For many years, there has been growing interest in promoting healthy behavior. Various interventions have been provided to help with different targets, such as stop smoking, eating healthily, exercising regularly, and reducing alcohol intake. Research efforts have been devoted to develop different types of programs promoting health, such as personal consulting and evaluation, monthly delivered information, group class, and incentive rewards. 13 Meanwhile, the rapid growth of information technologies (especially the Internet) has also created opportunities for innovative health promotion. Research shows that computer-mediated communication has potential in disseminating interventions to increase physical activity.14–17 Whether the relevant interventions are person to person or Internet based, most of the systems are aimed mainly at passively providing health information or exercise instruction, in which participants need to actively access the information or aggressively participate in the programs in order to achieve behavior changes.
For people who must sit in front of computers for prolonged periods, they might understand the importance of regular breaks and ergonomic behaviors but have a hard time reminding or encouraging themselves to engage in the healthy computer use behaviors. Therefore, in this “computer” era, greater efforts on promoting healthy computer use behavior are necessary.
Ergonomics training
Despite the fact that computer-related health issues are critical, surprisingly little effort has been made regarding the design and development of relevant interventions. Several ergonomics training methods have been developed with regard to setting up effective computer workstations to increase the comfort, safety, and productivity for prolonged sitting computer users at work.18,19 However, printed materials, seminars, and lectures are the most common approaches for the delivery of information, with which computer users need to actively access or participate in the programs. Meanwhile, some ergonomics software packages have been designed to prompt computer users to take a break and guide them toward regular exercise. However, most of the software packages either contain only limited information or are not very user friendly. Furthermore, to date, there is little research on evaluating the effectiveness of these software packages.
Recently, with increasing interest in how to help prolonged sitting computer users avoid computer-related syndromes, there are still few studies investigating the effects of computer break programs. Marangoni 20 proposed an intermittent stretching exercise program and found that the interventions contributed to a significant reduction in musculoskeletal pain associated with working at a computer workstation. Van den Heuvel et al. 21 reported a positive effect on recovery from complaints of work-related disorders through the use of software programs stimulating regular breaks and exercise. Nevertheless, these studies targeted office workers as the research participants, and so far, little is known about the effects of the programs on both the intention and action of healthy computer use behaviors.
Health behavior change
Most cognitive theories claim that people’s intention to change is one of the best predictors of their actual change.22–24 However, in reality, people usually do not just follow their intentions to conduct certain behaviors, such as physical exercise, problem drinking, or eating patterns. An intention does not necessarily by itself lead to action. We need to build the knowledge and skills to act on their intentions and then to create a supportive environment for the behavior change. 25 This study tries to carry out an intervention to help with the creation of a supportive environment for healthy computer use behaviors and to investigate the effects on both the intention and action of healthy computer use. Following the theory of planned behavior, intention refers to the degree to which people are willing to try or how much of an effort they are planning to exert to perform the behavior; action refers to the degree they enact their desire to actually conduct the tasks. 26 In this study, the intention and action of healthy computer use behavior mean to what degree the participants desired to perform the behaviors and the frequency with which they actually performed the behaviors, respectively.
If the rapid computer technology adoption continues without due consideration of users’ healthy computer use behavior, there is a possibility that students will suffer from computer-related syndromes in the very near future, just as office workers. 7 Therefore, we must acknowledge that as computer use becomes more and more prevalent, so will computer-related syndromes. This gives us the opportunity to reconsider the design and development of ergonomic software and to investigate its effects on healthy computer use behavior for extended computer users, particularly in school.
Purpose of this study
The purposes of this study were to delineate the design and development of the proposed program, to answer the questions of how the program would influence the participants’ intention and action of healthy computer use behaviors, and to investigate how the proposed program was accepted and experienced. In this study, we developed a time-scheduled computer health animation program prompting computer users to carry out healthy computer use behaviors (e.g. break, breathing, brief stretching, and massaging), for the people who sit in front of computers for extended periods.
The process and necessary tasks of development and the effects of this intervention on computer health intention and action changes are the focus of this study. A series of relevant health information and exercise animation clips (both in the form of text and figures) was designed and integrated into the program. Without too much instructional purpose, the goal of the program was to motivate and induce healthy computer use behaviors.
Methods and process
Development of the animations
The program focused on messages dedicated to increasing awareness and behaviors with regard to healthy computer use among people using computers for extended periods. Through a collection of relevant materials and a process of classification with the aid of physicians, four categories of healthy behaviors of computer use were identified and defined as break, breath adjustment, body massage, and body stretch. In total, 90 animation clips were designed and stored in the database for time-scheduled delivery. Each of the clips lasted about 25 s. Furthermore, five subcategories of body parts (eyes, head/neck/shoulder, hand/wrist, waist/back, and leg/foot), based on the common symptoms of extended computer use, were selected and included in the design of body massage and stretch. One thing that should be noted here is that no animation clips were created directly for prompting users to take a break. However, the “break” behavior was expected to happen indirectly because of the other three categories of animation prompt. That is, users were expected to follow the animations prompting actions, or to simply stop their work that was in progress for a while, or even both.
For the purpose of helping to increase flexibility and reduce tension and stress, several units of office stretches and exercises were created for the content development, such as neck, shoulder, chest, torso, back, waist, forearm, wrist, hip, thigh, stretches/shrugs/twists, and eyeball movement and rotation. Please refer to Figure (1-1), (1-4), and (1-7) of Figure 1 for visual presentations of the screen prints. Some office acupressure massages (see Figure (1-3), (1-6), (1-8), and (1-9) of Figure 1) were embedded as well to help relieve muscular tension and ease the discomfort of the body (head, eyes, neck, shoulders, hand, leg, foot, and so on). Figure (1-2) and (1-3) of Figure 1 were for breath adjustment.

Screen prints of examples of the developed animations.
Two-dimensional (2D) and three-dimensional (3D) computer animations in both textual and graphic formats were the media for the delivery of health messages. With the help from experts in the fields of health and physical activity, multimedia and animation creators, and the animation-making tool Flash, 90 animation clips were developed for this study (for some visual examples, see Figure 1).
Sampling and participants
Through a convenience sampling approach, the freshmen enrolled in the program of Educational Technology (ET) at National Chiayi University, who normally worked more than 5 h a day in front of a computer, were the targeted population for this study. In the beginning, 41 participants were recruited. Most of the participants were aged 18–20 years. Two participants withdrew from this study during the posttest stage. Data of the 39 valid samples (25 females and 14 males) were retained for further analysis.
Implementation process
After recruiting participants, the researchers installed the animation program on the participants’ computers in the laboratory (or at work). The entire execution time for the research was 10 days. The animation program was initiated and remained active every time the participants turned their computers on, which had been configured to randomly play one animation clip every 40 min (see Figure 2 for snap shots of the implementation scenario). In other words, every 40 min, one animation clip would pop up on the screen with background sound and music. Each animation clip was designed to play the embedded content for 20–30 s. The pop-up window would last for another 5 min to repeatedly play the content unless called off manually. Therefore, ideally, participants were expected to follow and repeat the proposed movements for about 5 min after 30–35 min computer use. As research suggested, either 5-min break every 30 min or 10-min break per hour resulted in worker comfort and increased performance. 27 Each participant was contacted briefly to check whether there were any problems with the implementation program after the first day of use.

Video snap shots of implementation scenario.
Data collection
Before and after surveys were conducted to collect participants’ intention and action of healthy computer use behaviors before and after the intervention. The surveys used self-reported questionnaires, which have been found to be an effective and common way to evaluate health and exercise behaviors.28,29 A pretest survey was distributed at the beginning of the study to collect the participants’ demographic information, and their self-reported intention and action of healthy computer use behavior for the past 10 days. A posttest survey was conducted right after the 10-day experiment to gather data about the effects of the program on health behavior changes and how the designed program had been accepted and experienced.
The questionnaire comprised 34 items including three open-ended questions. The first part of the questionnaire asked about participants’ demographic information including gender, age, level, and average length of time for using computers every day. The second part asked participants about their intention and action of healthy computer use behavior: frequency of breaks, breath adjustment, body stretch and massage (for eyes, head/neck/shoulder, hand/wrist, back/waist, and leg/foot), and so on. All the statements were measured using a 5-point Likert scale that ranged from “never” (scored 1) to “very often” (scored 5). Sample statements would be “For the past 10 days, how often did you intend to stretch your hand or wrist?” (for the intention) and “For the past 10 days, how often did you actually stretch your hand or wrist?” (for the action). The questions about computer-related health issues were designed parallel to the categories of the developed health animation contents. The third part of the questionnaire contained three open-ended questions, which asked participants’ likes/dislikes about the intervention and their suggestions for the design of the program. The content validity of the survey was assessed by a panel of experts in the fields of technology and health services. The internal consistency was verified and guaranteed with Cronbach’s alpha coefficients equal to or greater than 0.75.
Results and discussion
Intentions and actions of healthy computer use behaviors
The participants’ healthy behavior scores in terms of “intention” and “action” were examined respectively. Overall, the difference in means for behavior “intention” between before (3.52 ± 0.874) and after (3.62 ± 0.625) intervention did not reach statistical significance (p = 0.510), indicating that the implementation of the time-scheduled health animation delivery program did not exert a meaningful impact on the participants’ behavior intention (Table 1).
Healthy behaviors of computer use before and after intervention (N = 39).
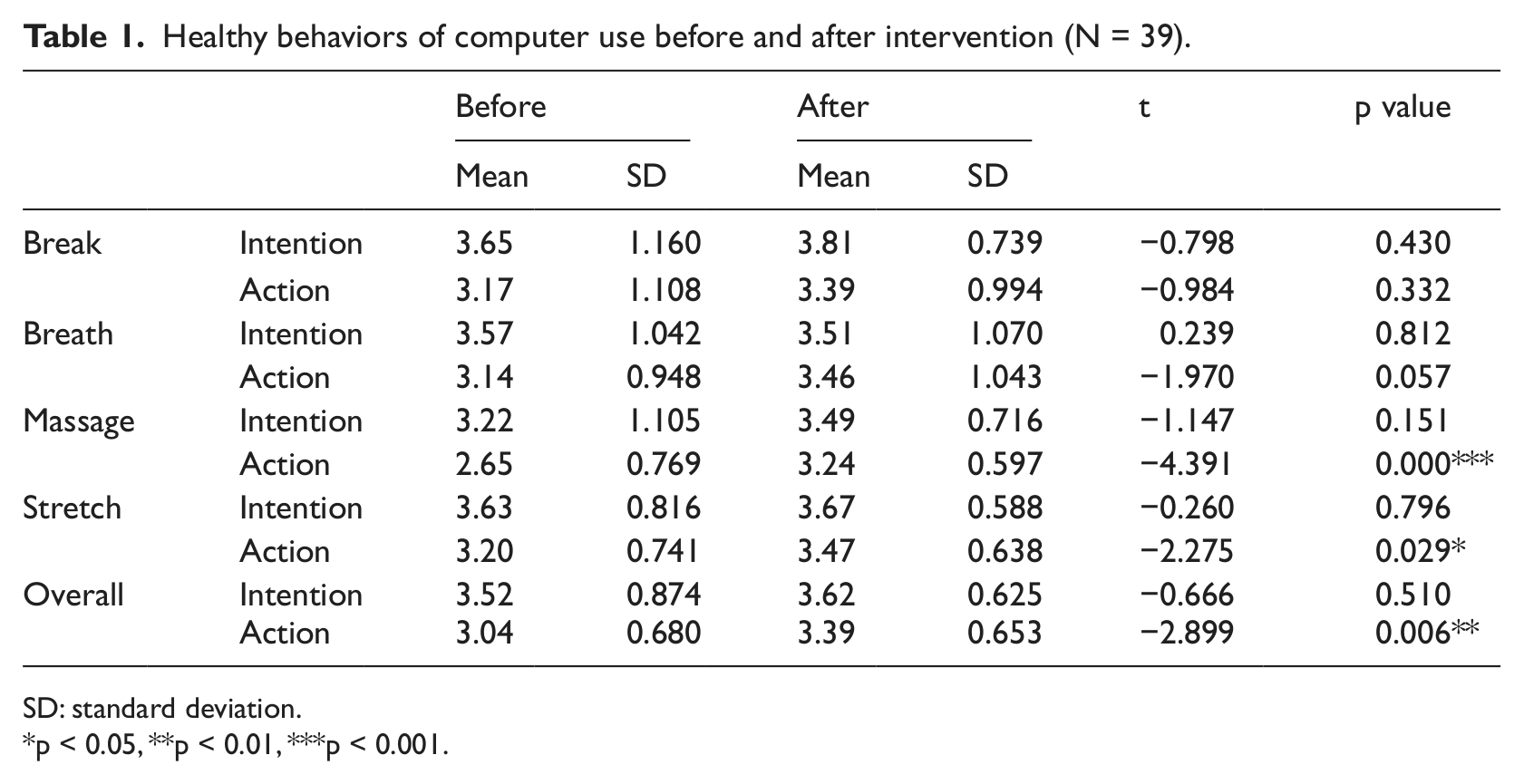
SD: standard deviation.
p < 0.05, **p < 0.01, ***p < 0.001.
Overall, the difference in means for behavior “action” between before (3.04 ± 0.680) and after (3.39 ± 0.653) reached significance (p = 0.006). Furthermore, among the four categories (break, breath, massage, and stretch) of healthy behaviors of computer use, “massage” and “stretch” revealed significant improvement in “action” (Table 1). The action of breath adjustment showed improvement (3.14 ± 0.948 vs 3.46 ± 1.043) as well, but did not reach statistical significance (t = −1.970, p = 0.057). Surprisingly, the action of taking regular breaks showed no significant improvement (p = 0.332) after the intervention. One explanation for the insignificant improvement in taking regular breaks might be because no animation clips were created specifically for prompting users to take a break. That is, unlike the other three categories of healthy behavior, “break” was the one which was not delivered to the computer users as a reminder of healthy behavior at the scheduled time. Another reason may be that the increased actions of other behaviors (breath/massage/stretch) weakened the impulse of taking breaks, since “taking a break” in nature means actually walking away from the work in progress. On the contrary, massage is the one with far lower preintervention score but with the highest range of improvement (from 2.65 ± 0.769 to 3.24 ± 0.597). This indicates that prolonged sitting computer users do not think of doing massage as often as stretch/break/breath, but it is easier for them to be prompted to do so.
Intentions and actions for body massage/stretch
The difference in the overall average scores for the intention of body massage/stretch between before (3.47 ± 0.235) and after (3.61 ± 0.141) intervention did not reach a level of significance (p = 0.056). As demonstrated in Table 2, among the five different body parts, before the intervention, the highest intention score for massage/stretch was head/neck/shoulder, which also remained the highest after the intervention. The relatively high scores might suggest that head/neck/shoulder-related symptoms were the relatively severe health problems that the participants experienced most for extended computer use. Therefore, they did not need to be reminded of the discomfort related to head/neck/shoulder, as indicated by the already high score before the intervention (Table 2).
Intention and action scores for body massage and stretch before and after intervention (N = 39).
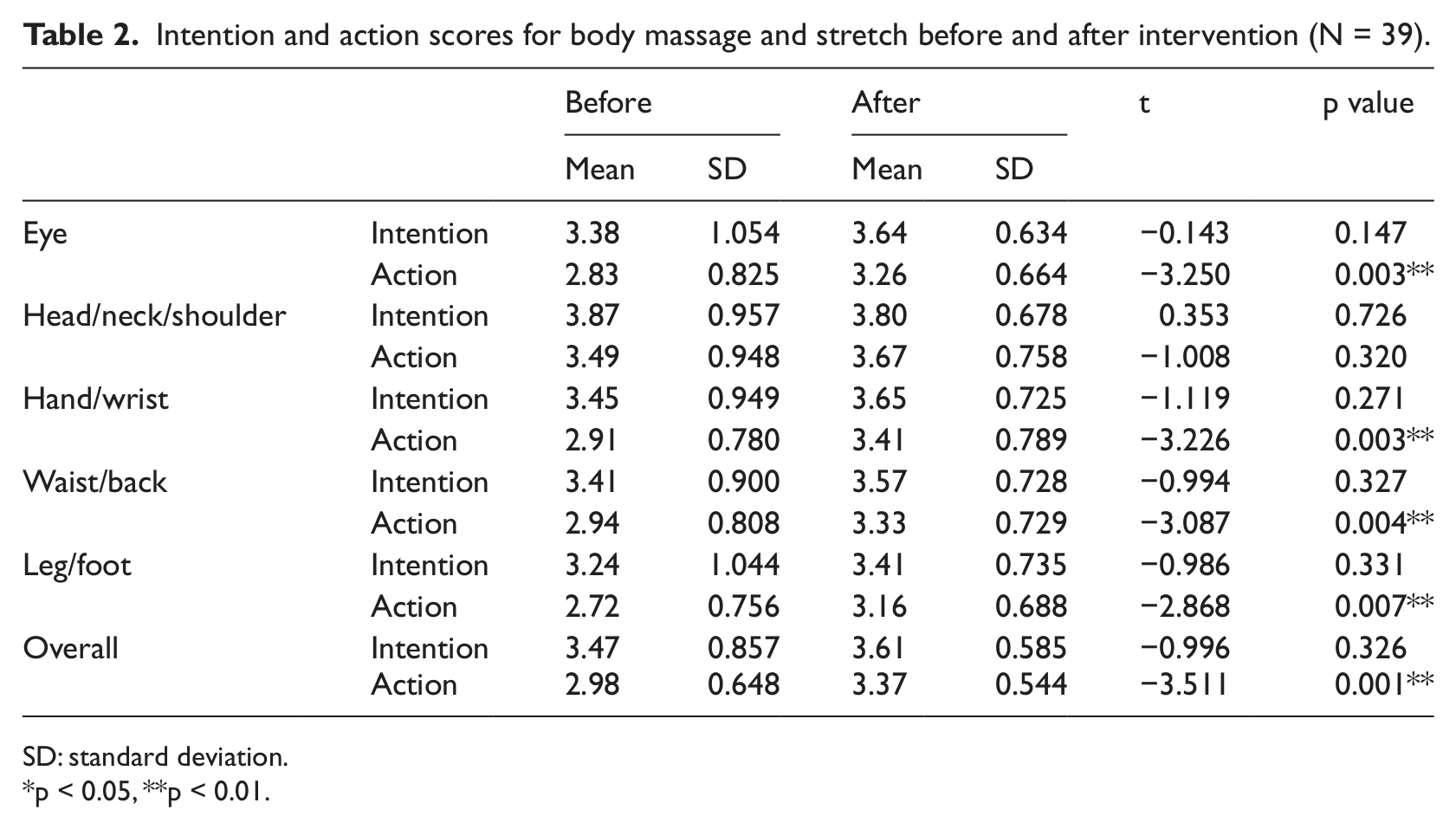
SD: standard deviation.
p < 0.05, **p < 0.01.
The difference in the overall average scores for the action of body massage/stretch between before (2.98 ± 0.297) and after (3.37 ± 0.191) the intervention reached a level of significance (p = 0.002). With the animation promotion of healthy computer use, four out of five (except the head/neck/shoulder) categories (body parts) demonstrated statistically significant improvement in the action of body massage and stretch after the intervention (Table 2). More importantly, the average scores increased from between “slightly disagree” and “agree” to between “slightly agree” and “agree.” The nonsignificant improvement in the action of head/neck/shoulder health behavior could be attributed to the fact of already high score on the action before intervention (3.49) when compared with the other four categories (2.83, 2.91, 2.94, and 2.72). This implies that participants were not just more aware (see Table 2, highest intention score, 3.87) of the potential harm of extended computer use to their head/neck/shoulder than other parts of the body, but also already acted on it before the intervention.
Acceptance/experience of the program
The feedback from the open-ended questions surfaced many interesting suggestions toward the possible further development of the research direction. Those worth mentioning were the popularity of “massage” content-related animation clips. Most of the participants stated that they liked the massage animations best and fully followed the instruction of massage animations, much more frequently than other kinds of animation contents. The possible reasons for the popularity may be ascribed to the relatively mild form and easy-to-perform characteristics of activities. Besides, the healing function of acupressure massage therapy has been proven effective.30–33 However, two more things regarding the massage animations were raised. First, they wanted to know the theoretical functions and possible impact of the particular acupoint massage. Second, they wanted to make sure that they worked on the right spots for acupressure since the animation clips did not give any help locating the acupoints.
Some participants expressed that they liked the program and knew that they needed it for the sake of their health. However, they did not like the feeling of being disturbed, especially when they were playing video games. Others stated that they enjoyed the program and recommended it to their friends already. Some claimed that they followed the instructions of the animation exactly when the clips prompted them to. Still others expressed that they sometimes did not feel like following the instructions but did stretch/massage on their own or even took a break as or right after the animation clips prompted; for example, they might feel that their eyes burned but the animation clip was showing on leg stretch. Besides, several improvements were suggested, such as stopping the program automatically if the computer had been idle for a certain period of time; each pop-up clip should fade out if there is no further operation (e.g. canceling or replaying) after a while; and the background sound should use fade-in mode to avoid startles by sudden sound, which are considered useful for the future development of the program.
Different from other studies of computer break software, this study experimented with university students instead of occupational workers. First and foremost, we would like to bring this to the attention of younger generations for their healthy computer use behavior and to see how much effect designed break software has. We tried to propose the concept that “just like that you need to brush your teeth after meals, you have to do something after the use of computers awhile.” We also are aware that workers, compared to students, have more demands on not being disturbed. Therefore, using a top-down approach, the animation software may be built into the server system of the company to unify the animation prompting schedule for workers located in the same sitting area. It is assumed that workers would then be more willing to follow the animation presentation without feeling guilty of “staying” away from work for a while.
Conclusion and suggestion
The participants considered the program to be a useful reminder for healthy computer use. The results showed that the program significantly affected the participants’ computer-related health behaviors throughout the 10 days of the experiment, as demonstrated by decreased discrepancies between intention and action. These findings provide encouragement for further development of the program.
The relatively mild effect on the intention seems to suggest that for the future development, the program should not merely focus on the function of “reminding” extended computer users of healthy behavior to bridge the gap between intention and action. More importantly, sufficient knowledge and skills regarding how and why to live healthier with computer and technology should be embedded to increase the intention level as well.
The average scores (3.52 vs 3.62) of intention for healthy behaviors of computer use did not imply a high demand for participants on the solutions of computer-related syndromes. However, given that the participants in this study were relatively young, they may not sense any severe problem associated with extended computer use yet. However, as is well known, “prevention” is far better than “cure.” Therefore, we need to figure out a way to “install” a set of healthy habits of computer use for the young generation on computers.
As Rogers 34 declared, prevention innovation has its difficulty in diffusion due to the lack of immediate consequences. This study calls attention to the negative effects of extended computer use and suggests that increased efforts be made regarding the immediate needs of promoting healthy habits among people who spend extended periods in front of computers. For example, computer-related industries should consider including (providing) solutions (such as the programs) with their highly valued computer application packages, to help with the increasingly severe health problems associated with extended computer use. Furthermore, the skills and techniques of massage/breath have the potential to be included as part of the break software content design, in addition to traditional body stretch clips. Computer break/stretch software is also worthy of further definition and development for advanced functions to achieve learning and practicing purposes instead of merely as a reminder for breaks/stretches.
This study developed an animation prompting program for extended computer users and reports the effects of the program on users’ relevant computer health behavior changes. Further research designs such as using a control group, blinded research, and an assessment method along with the self-report are suggested for the future studies. More rigorous evaluation with focus on different dimensions, such as Kirkpatrick’s model, from reaction, learning, and behavior to result, should be also noted in the future. 35 A longitudinal approach of study design would also be necessary for following up to examine the influence of the program on health outcomes.
Footnotes
Acknowledgements
The authors would also like to thank Prof. Rob Procter and the two anonymous reviewers for their thoughtful and valuable comments and suggestions.
Funding
This study was supported by a grant from the National Science Council (grant number NSC 98-2511-S-415-009-MY2).