
Abstract
This study had two aims: to measure patient preferences for medical appointment reminder systems and to assess the predictive value of patient usage and familiarity with other service providers contacting them on responsiveness to appointment reminder systems. We used a cross-sectional design wherein patients’ at an urban, primary-care clinic ranked various reminder systems and indicated their usage of technology and familiarity with other service providers contacting them over text messages and e-mails. We assessed the impact of patient usage of text messages and e-mails and patient familiarity with other service providers contacting them over text messages and e-mails on effectiveness of and responsiveness to appointment reminder systems. We found that patient usage of text messages or e-mails and familiarity with other service providers contacting them are the best predictors of perceived effectiveness and responsiveness to text message and e-mail reminders. When these variables are accounted for, age and other demographic variables do not predict responsiveness to reminder systems.
Keywords
Introduction
Patient nonattendance (commonly known as “no-shows”) at scheduled medical appointments represents a serious problem for many health-care providers. An earlier national study in the United States revealed that over one-third of the surveyed practices had a no-show rate of over 21%. 1 More recently, multiple studies have reported high no-show rates ranging from 23% to 34% in outpatient clinics.2–4 Patient no-shows represent a significant problem that follows from unreliable schedules: the administration is inconvenienced and clinicians’ time, which could have been used to serve other patients, is wasted. Both of these problems reduce the efficiency of care delivery.5–7
Although some of the no-show appointment slots can be compensated by walk-in patients, complete financial recovery from a high no-show rate is most likely impossible. For instance, in one of the few national-level studies, nonattendance at outpatient clinics costs the UK National Health Service an estimated ₤790 million per year. 8 Furthermore, missed appointments are particularly problematic for patients with chronic conditions who can more effectively manage their health if they keep their medical appointments. For example, patients with frequent missed appointments were less likely to utilize preventive health services and thus had poorer control of their blood pressure and diabetes.6,9,10
To reduce the patient no-show rate and alleviate the concomitant negative impact, health-care organizations have tried a variety of strategies. One particularly useful intervention seems to be adopting an appointment reminder system, that is, remind patients a few days prior to their appointments via a phone call, an e-mail, a short message service (SMS), or a letter.11,12 Many studies have focused on the effectiveness of reminder systems, and most of them compared one or two modalities of reminder systems (e.g. phone call and SMS) to nonintervention control.2,4,13–15,i A recent systematic review of this literature concludes that, although no-shows cannot be eliminated completely, nearly all these reminder systems reduced patient no-show rates. 16 Specifically, this review finds that the weighted mean relative reduction in no-show rate was 34% of the baseline no-show rate.
Many of the above intervention studies assume a “one-size-fits-all” approach. That is, by implementing phone or SMS reminder systems, all patients receive their reminders in the same fashion. However, research suggests that the effectiveness of a reminder system is dependent on the patient population, the modality of reminder, and service type. 11 Even within a single modality of reminder system—SMS reminders—Guy et al. 12 report a significant variation in effectiveness: the odds ratio of the attendance rate in the SMS group compared with controls ranges from 0.91 to 3.03. Such a variation in the effectiveness of the reminder systems implies that there is no “one-size-fits-all” reminder system and that reminders need to be tailored to individual patients or at least to specific patient groups to make them more effective.
One strategy for constructing more nuanced reminder systems is to assess patients’ preferences. Indeed, research in psychology suggests that people’s preferences and attitudes impact their behavior.17–19 Accordingly, once patients have expressed a preference for text message or phone call reminder systems, they will be more likely to respond to text message or phone call reminders, respectively. Thus, by reminding patients in the way they prefer, they are more likely to attend the scheduled appointment, or at least cancel the appointment. However, research measuring patient preferences for reminder systems is very limited. What little research there is has found that preferences for different reminder systems depend on patient populations, 20 younger patients prefer to have voicemails sent to their cell phone as opposed to work and home phone, 21 and younger patients exhibit more favorable attitudes towards SMS reminders. 22
In practice, this previous research has yielded perhaps an overly simplistic understanding of how patient demographics impact preferences for different reminder systems. For instance, this research suggests that younger patients tend to be more technology “savvy” and hence are more likely to prefer SMS reminders. This also seems to agree with our common wisdom. However, one important effect that has been overlooked when studying patient preferences for reminder systems is the role of expertise, specifically, how patients’ usage of text messages or e-mails in their everyday lives impacts their willingness to use and respond to text messages or e-mail reminders in the context of health care. This is especially puzzling as research in marketing suggests that consumer learning and expertise are important topics in understanding choice and behavior.19,23,24 This research would suggest that the more people become adept at interacting with a product feature (e.g. SMS), the more favorable their attitudes are toward using that product feature and the more likely they are to alter their behaviors so that they can use the product feature.
One way in which consumers can gain familiarity with product features, such as SMS, is for other service providers to contact them over that medium of communication. Many service providers, such as banks and credit card companies, send consumers reminder messages about their accounts. For example, many banks allow consumers to enroll in a text message reminder system where people are reminded of their account balances and notified of any account shortfalls. Similarly, many phone companies allow consumers to customize their account so that they receive e-mail and text message reminders when their bill is due or paid. 25 Conceivably, then, consumers who use these reminders from other service providers will be more likely to utilize text or e-mail reminders from health-care providers. Thus, consumers’ preferences for reminder systems in health-care settings might be impacted by their preferences for reminder systems from other service providers. Despite the fact that other service providers send messages and reminders almost every day via a variety of channels, no research to date has explored how individuals’ familiarity with other service providers contacting them can affect patient preference for medical appointment scheduling reminders. In particular, lack of such information may lead to use of less-effective reminder systems due to limited understanding of patients’ “true” preferences and usage of SMS or e-mail product features.
The purpose of this study was to investigate patient preferences for different modalities of reminder systems, including home phone call, cell phone call, SMS, e-mail, and direct mail systems. We examined the impact of patient experience with other service providers on their preferred choice of medical appointment reminder systems. The study was conducted in a primary-care setting, where appointment scheduling is most widely used and patient no-shows are most commonly observed, and more importantly, where patient preferences for appointment reminders have seldom been explored and remain largely unknown.
Method
Design
We used a cross-sectional survey design to assess patient preferences for five different reminder systems, to measure patients’ usage of—and familiarity with other service providers contacting them over—text messages and e-mails, and to assess reported responsiveness to different reminders systems.
Settings and participants
Data were collected on 161 adult patients from a primary-care clinic in New York City. The clinic serves a diverse patient population in a low-income area. Forty-one providers operate at the clinic to serve about 26,000 patients per year. A convenience sample of patients from this clinic was recruited for this study. Patients were eligible to participate if they spoke English or Spanish languages and if they were over the age of 18 years. Overall, 240 patients were eligible to participate, and 161 of them agreed to participate, yielding a response rate of 67%.
Survey instrument
A self-report survey instrument was created in English, which later was translated into Spanish to be used with the Spanish-speaking patient population at the clinic. A native Spanish speaker conducted the translation and a second native speaker verified the accuracy of the translation. The instrument was designed to collect data about patients’ preferences for different reminder systems, patients’ usage of text messages and e-mails, and patients’ familiarity with other service providers.
Patients first ranked their preference for five different reminder systems from “most preferred” to “least preferred.” The reminder systems included the following: (a) home telephone call, (b) cell phone call, (c) text message, (d) written reminder, and (e) e-mail reminder. Next, patients indicated whether they have active home phone lines, cell phone lines, and e-mail accounts (yes/no responses); what charge they incurred from receiving text messages (monthly data plan or per text fee); how many text messages and e-mails they send and receive a day; and how effective they think phone call, text, and e-mail reminders are (7-point scales from “not at all effective” to “very effective”).
In the second portion of the instrument, patients indicated their familiarity with other service providers (e.g. banks, credit card companies, and airlines). ii Specifically, patients indicated (7-point scales from “not at all likely/familiar/typical” to “very likely/familiar/typical”) (a) how likely they are to read messages sent by other service providers over text messages, (b) how familiar they are with responding to text messages from other service providers, and (c) how typical it is for other service providers to contact them over e-mail.
The third portion of the survey mainly assessed patients’ responsiveness to different appointment reminder systems. On a 7-point scale (from “not at all likely/important/typical” to “very likely/important/typical”) patients indicated (a) how likely they would be to reschedule their appointment over text messages or e-mails, (b) how important it would be for them to reschedule their appointment, and (c) how typical it is for other health-care providers to use text messages or e-mails to reach them.
The demographic characteristics of the patients including their age, sex, and race/ethnicity were collected. In addition, information about the language spoken at home, whether they are a first-time patient at the clinic, length of time as a patient at the clinic, and their health insurance were collected.
Data collection
Data collection took place from December 2011 to February 2012. We obtained approval to conduct the survey from the Medical Director of the clinic. Two research assistants approached patients in the waiting room and informed them of the study. Specifically, patients were told that a study was being conducted to improve the clinic’s appointment reminder system, no personally identifying information (e.g. names, social security numbers) would be obtained from them, all responses would be reported in aggregate form, and they could discontinue at any time if they felt uncomfortable completing the survey and their responses would be discarded. To ensure that patients had enough time to complete the survey, the research assistant asked patients roughly how much time they had until their scheduled appointment and only recruited patients who expected a 10-min wait time or longer at the clinic. Surveys were only passed out to patients who agreed to participate. Once patients agreed to complete the survey, the research assistant moved to a separate area to avoid disturbing the participants as the survey was self-directed. If the patients had any questions, they were asked to raise their hand so the research assistant would know they needed assistance. All surveys were completed in full, and no patients volunteered to remove their responses.
Ethical considerations
The study was approved by the Institutional Review Board at Columbia University Medical Center. Patients were thanked for their participation and given a small token gift (a pen) for their participation. Verbal consent was obtained.
Data analysis
The data were entered into SPSS Version 17 software (IBM Corporation, Armonk, NY) for analysis. We computed descriptive statistics including means and frequencies for the demographic characteristics as well as for the patients’ usage of technology.
We employed a Friedman Nonparametric Test to assess patients’ ranked preferences and a Wilcoxon Signed Ranks test to assess significant differences between ranks. Models were built to assess the impact of patient usage of text messages and e-mails and patient familiarity with other service providers contacting them over text messages and e-mails on the effectiveness of and responsiveness to appointment reminder systems. We constructed a dummy variable for whether patients sent text messages or e-mails on a daily basis. We employed a series of analyses of covariance (ANCOVAs) where patient familiarity with other service providers and patient usage of text messages or e-mails were fixed factors. We had two key dependent variables: perceived effectiveness of reminder systems and responsiveness to reminder systems. Since we had multiple scale items measuring responsiveness to reminder systems that were highly related (α = 0.90 for text message, α = 0.83 for e-mail reminders), we collapsed these items into two indices of responsiveness to text message and e-mail reminders.
Based on previous research indicating that age impacted patients’ responsiveness to reminder systems,21,22 we included age as a covariate. When analyses yielded significant interactions, we categorized patients into those who are very familiar versus those who are less familiar with other service providers contacting them over text messages or e-mails (based on a median split as familiarity with other service providers is a continuous variable) to further explore key differences in perceived effectiveness of and responsiveness to reminder systems as a function of familiarity with other service providers. In all of our analyses, p < 0.05 was considered statistically significant and 0.10 < p < 0.05 was considered marginally significant.
Results
Demographics
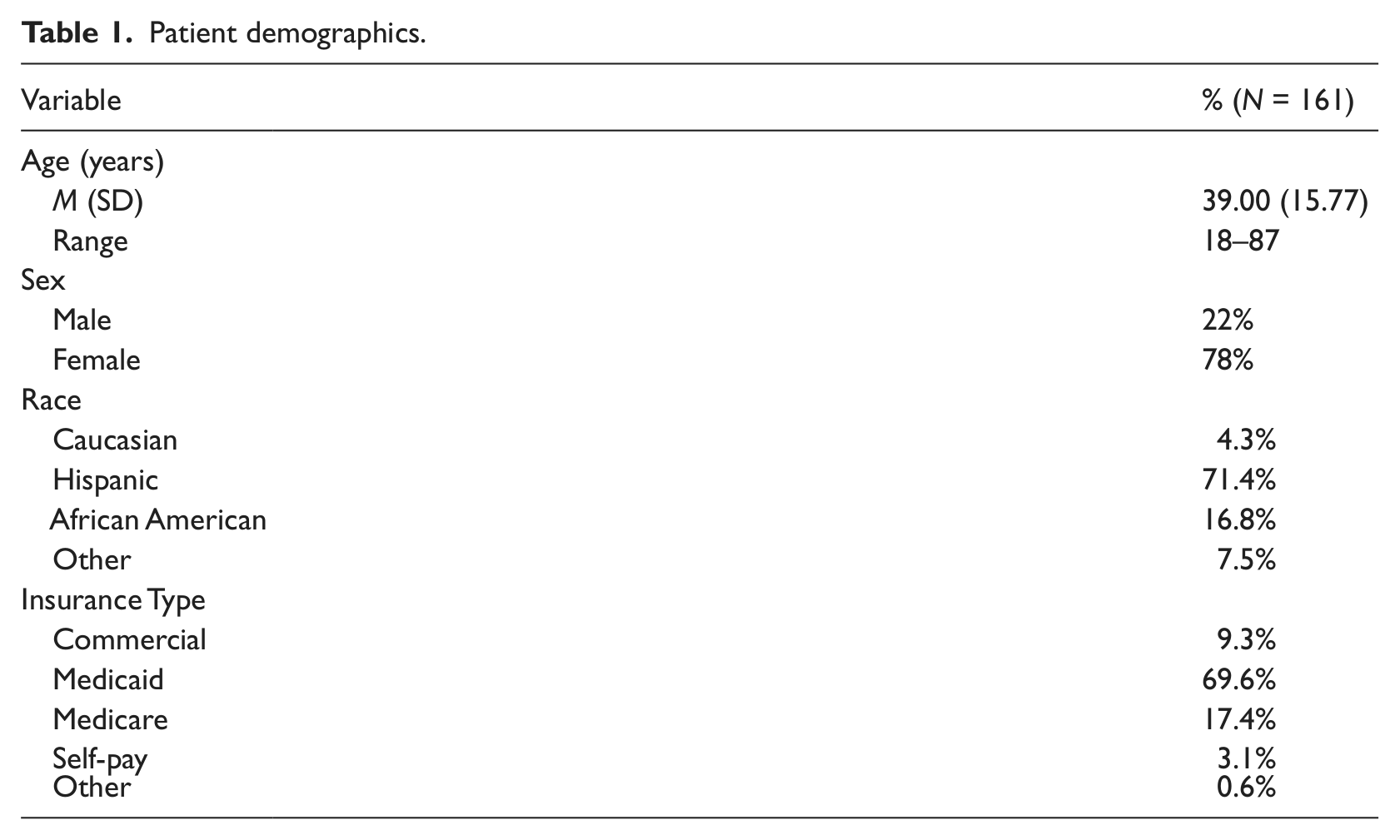
Table 1 provides information on patient demographics. The average age of patients was 39 years, and 78% of the sample was female. The patient population was predominantly Hispanic (71.4%) and a majority utilized Medicaid (69.6%) or Medicare (17.4%) to pay for their health-care services.
Patient demographics.
“Technological Savvyness”
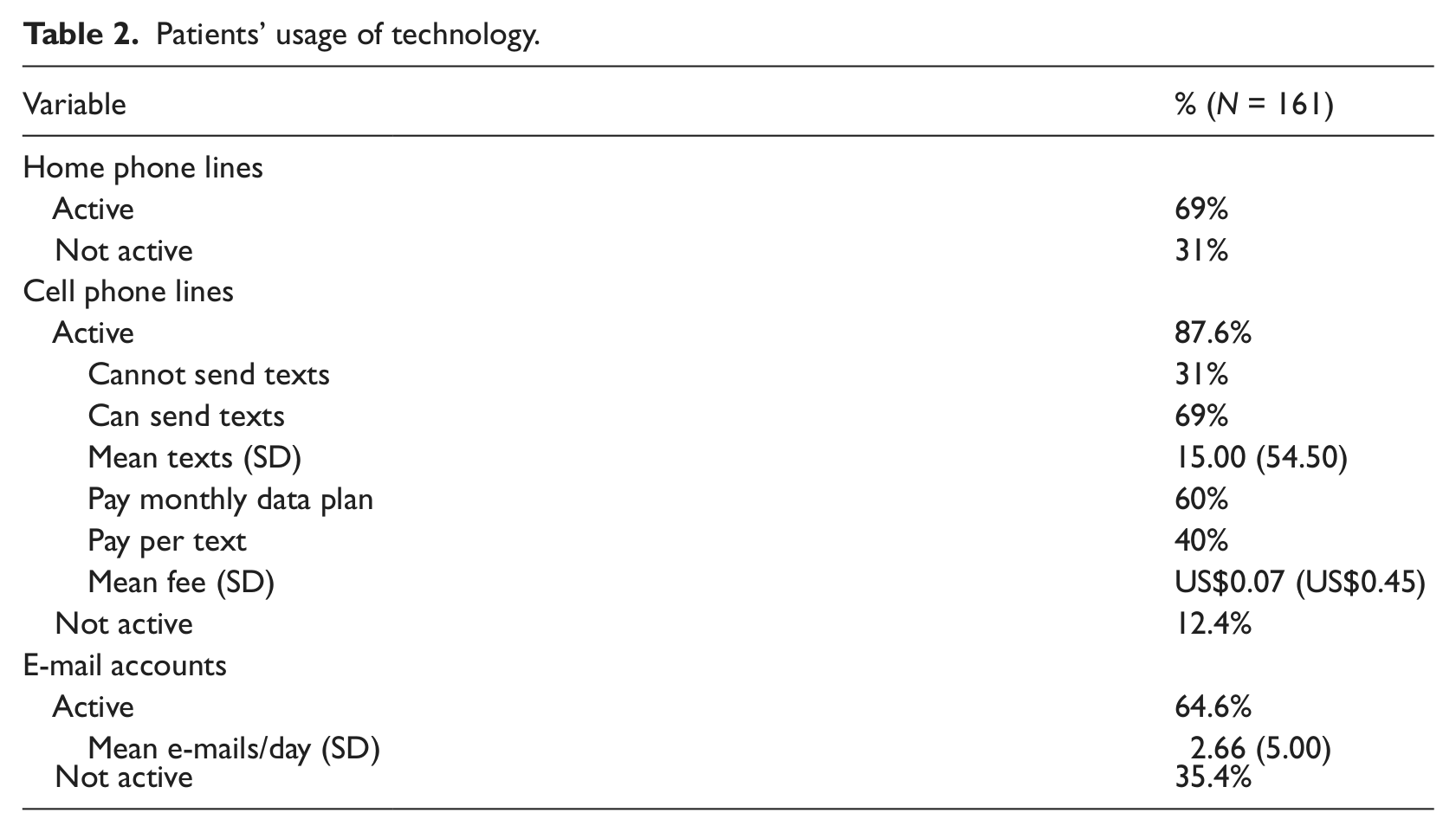
Table 2 summarizes the descriptive data on patients’ usage of technology. There was large variation in the technology patients currently used. About 31% of the patients did not have an active home telephone line, 12.4% did not have an active cell phone line, and 35.4% did not have an active e-mail account. Of the patients who did have active cell phone lines, there was large variation in the number of text messages patients sent as well as in how patients paid for their text messaging service. Specifically, 69% of the patients with active cell phone lines could send text messages and, of this population, 60% paid monthly data plan fees and 40% paid fees per text (Mean fee = US$0.07). Patients, on average, sent 15 texts per day. Of the patients who did have active e-mail accounts, 88% were likely to check their e-mail every day. Patients, on average, sent 2.66 e-mails a day.
Patients’ usage of technology.
Ranking of preferences for reminder systems
Our analysis revealed the following rank order for reminder systems (in the order of most preferred to least preferred): (a) cell phone, (b) home phone, (c) text message, and (d) direct mail and e-mail (tie). Although many patients indicated they would like to be contacted over their home telephone, a significant number of patients (31%) did not have an active home telephone line.
Our analysis further revealed significant differences in ranked preferences for the following relationships (preferred choice–least preferred): home phone–text message (Z = 4.48, p < 0.001), home phone–direct mail/e-mail (Z = 6.48, p < 0.001), cell phone–text message (Z = 6.07, p < 0.001), cell phone–direct mail/e-mail (Z = 6.95, p < 0.001), and text message–direct mail/e-mail (Z = 3.99, p < 0.001). There was no significant difference in ranked preference for cell phone and home phone reminders (Z = 0.94, p = 0.34) nor was there a significant difference in ranked preference for e-mail and direct mail (Z = 0.72, NS).
The impact of other service providers contacting patients via text on attitudes to text message reminders
The ANCOVA yielded a significant main effect for participants’ usage of text messages, F(1,115) = 9.11, p < 0.01, a main effect for patients’ familiarity with other service providers contacting them over text messages, F(12,115) = 3.51, p < 0.001, and the predicted familiarity × usage interaction, F(8,115) = 2.95, p < 0.01. For ease of depicting this interaction, we conducted a median split to separate patients who are more or less familiar with other service providers contacting them via text (see Figure 1). This analysis revealed that among patients who were more familiar with other service providers contacting them, patients who sent text messages on a daily basis viewed text message reminders to be more effective than patients who did not send text messages on a daily basis, t(64) = 6.36, p < 0.001. Among patients who were less familiar with other service providers contacting them, patients who sent text messages on a daily basis also viewed text message reminders to be more effective than those who did not send text messages on a daily basis, t(95) = 8.23, p < 0.001. Notably, once we accounted for patients’ usage of text messages and familiarity with other service providers contacting them via text messages, age was no longer a significant predictor of perceived effectiveness of reminder systems, F(1,115) = 0.66, p = 0.42.
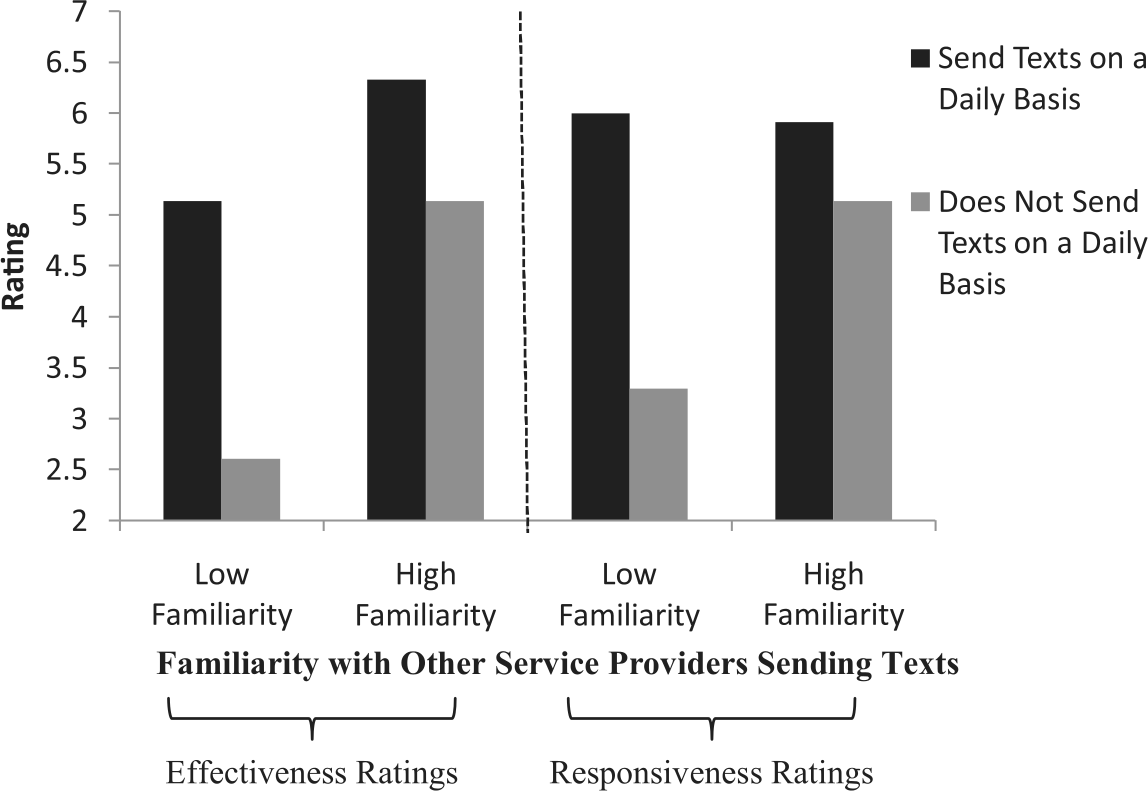
Effectiveness and responsiveness ratings of text message reminder systems as a function of familiarity with other service providers sending text messages (median split) and whether patients send text messages on a daily basis.
The impact of other service providers contacting patients via text on responsiveness to text message reminders
The ANCOVA of responsiveness to text message reminder systems revealed a marginal main effect for patients’ usage of text messages, F(1,129) = 2.80, p < 0.10, a main effect for patients’ familiarity with other service providers contacting them over text message, F(1,129) = 20.47, p < 0.001, and the predicted familiarity × usage interaction, F(1,129) = 2.66, p < 0.10. To explore the nature of this interaction, we divided patients into those who were more versus less familiar with other service providers contacting them over text messages, based on a median split (see Figure 1). Among patients who were less familiar with other service providers contacting them over text messages, those who sent text messages every day indicated higher levels of responsiveness to text message reminders than those who do not send text messages every day, t(78) = 2.55, p < 0.01. Among patients who were more familiar with other service providers contacting them over text messages, those who sent text messages every day indicated higher levels of responsiveness to text message reminders than those who did not send text messages every day, t(63) = 5.65, p < 0.001. As before, age was not a significant predictor of responsiveness to text message reminders, F(1,129) = 0.01, p = 0.92.
The impact of other service providers contacting patients via e-mail on attitudes to e-mail reminders
The ANCOVA yielded a marginal main effect for patients usage of e-mails, F(1,138) = 3.46, p < 0.07, a significant main effect for patients’ familiarity with other service providers contacting them over e-mail, F(6,138) = 5.95, p < 0.001, and the predicted familiarity × usage interaction, F(6,138) = 2.99, p < 0.01. For ease of depicting this interaction, we conducted a median split to separate patients who were more versus less familiar with being contacted from other service providers over text messages (see Figure 2). Among patients who were more familiar with other service providers contacting them over e-mails, those who sent e-mail messages on a daily basis viewed e-mail reminders from their health-care provider as more effective than patients who did not send e-mails on a daily basis, t(90) = 3.70, p < 0.001. Notably, age was no longer a significant predictor of perceived effectiveness of reminder systems, F(1,138) = 0.21, p = 0.65.
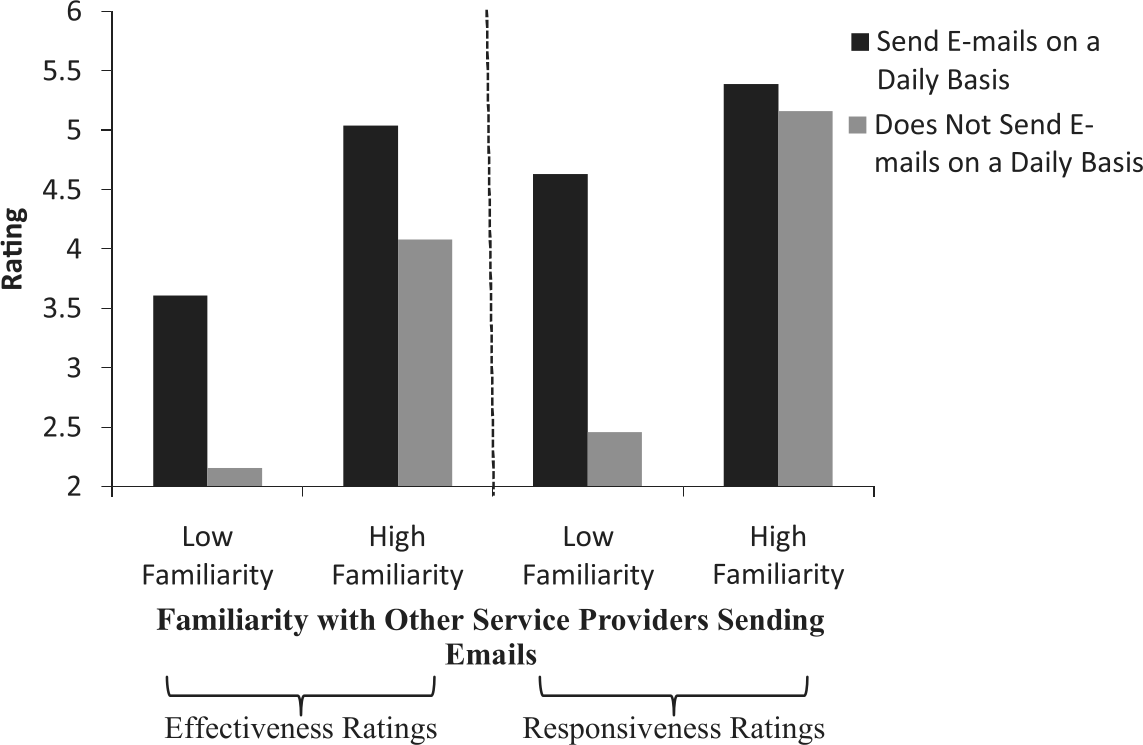
Effectiveness and responsiveness ratings of e-mail reminders as a function of familiarity with other service providers sending e-mails (median split) and whether patients send e-mails on a daily basis.
The impact of other service providers contacting patients via e-mail on responsiveness to e-mail reminders
The ANCOVA of responsiveness to e-mail reminder systems revealed a main effect for patients’ usage of e-mail, F(1,145) = 10.01, p < 0.01, and a main effect for patients’ familiarity with other service providers contacting them over e-mail, F(1,145) = 31.69, p < 0.001 (see Figure 2). To further explore the nature of these effects, we divided patients into those who were more familiar versus less familiar with other service providers contacting them over e-mails, based on a median split. Among patients who were less familiar with other service providers contacting them over e-mail, those who sent e-mail messages every day indicated higher levels of responsiveness to e-mail reminders than those who did not send e-mails every day, t(76) = 2.73, p < 0.02. Among patients who were more familiar with other service providers contacting them over e-mails, those who sent e-mails every day indicated higher levels of responsiveness to e-mail reminders than those who did not send e-mails every day, t(79) = 4.40, p < 0.001 (see Figure 2). Notably, age was not a significant predictor of responsiveness to e-mail reminders, F(1,145) = 0.01, p = 0.95. iii
Discussion
This cross-sectional study is among the first to explore patients’ relative preference for different appointment reminder systems in primary-care settings. Our results suggest that appointment reminder systems can be improved if patient preferences are taken into account. For instance, we find that a direct mail reminder, though still used by many clinics including the one where we conducted the survey, is the least preferred communication medium by the patients. This is not unexpected in the current era of technology and is also consistent with recent findings in other developed countries. 22 Cell phones and home phones, in contrast, are the most preferred choices of reminders; however, one-third of the surveyed patients did not have an active phone line and one-eighth did not have cell phones. This might be typical for other clinics that also serve low-income patient populations. To make reminder systems more effective, health-care providers need to identify what technology patients have access to. 26 Clinics in low-income areas face another challenge to reach their patients, and this inability to reach patients affects continuity of care and may increase the gap in health disparities.
One important finding in our study is that patient usage of technology and familiarity with other service providers are the best predictors of their perceived effectiveness and responsiveness to the appointment reminders via the same technology. This finding is consistent across two different communication mediums, text messages and e-mails. Interestingly, usage and familiarity seem to amplify the effect of each other. That is, the more frequently a patient uses a certain communication medium and the more familiar this patient is with other business providers approaching him or her via the same medium, the more effective and responsive this patient would be if he or she is reminded via this medium.
Previous research finds that age is a significant predictor of attitudes toward text message reminder systems. Indeed, separate analyses analyzing the raw effects of age do find that age, among other demographic variables, impacts responsiveness to reminder systems (F(1,82) = 0.008, p = 0.001, collapsing across communication mediums). However, our research suggests that caution should be taken when relying on age as the sole predictor of attitudes and responsiveness to reminder systems as this perspective may lead to misconceptions that elderly patient populations will not be responsive to more technologically grounded reminder systems. Consequently, health-care organizations may design appointment reminder systems that are less technologically grounded for their elderly patients (i.e. they might send direct mail reminders to elderly patients). We find no such effect of age after controlling for patient usage and familiarity with other service providers contacting them over a certain communication medium. Thus, our study suggests that if a health-care organization does not account for patients’ usage of technology and familiarity with other service providers in designing their appointment reminder system, they may not be effective and can lose opportunities to maintain continuity of care, particularly for elderly patients.
This study has some limitations. We only collected data from one clinic serving low-income populations located in a large urban metropolitan area; our findings might not be applicable to other settings. We recruited a convenience sample of patients waiting in the clinic. However, we intentionally conducted surveys across different times of the day and different days of the week to avoid time effects. Thus, it seems unlikely that our sample would significantly deviate from a random sample. Our survey data are self-reported, which might contain bias. However, since none of the survey questions solicits answers against social desirability, 27 we believe the self-reported bias, if any, will be small.
Conclusion
In conclusion, this study investigated patient preferences over different appointment reminder systems in primary-care settings. We found that patient preferences are diversified. Their perceived effectiveness and responsiveness to high-tech reminders, such as SMS or e-mails, cannot be predicted by age, a conventional predictor commonly associated with individual’s technological savvyness; patient experience and expertise of using such technologies with other service providers are the best predictors.
The rise of patient-centered care and personalized medicine calls for “no-one-fits-all” approach for treating patients28–31; the same mantra should apply for “reaching” patients. Marketers are sophisticated at reaching clients through a variety of communication mediums, including text messages and e-mails. Such strategies are certainly possible in health-care organizations too, especially in those clinics using advanced electronic scheduling systems, with which it would be fairly easy and inexpensive to add a text message component to their reminder systems. To ensure effective use of high-tech reminder systems, health-care organizations need to have policies in place to collect data and verify processes to ensure that patients’ contact information is correct, thus allowing them to receive reminders.4,26 Future research is required to address how to “personalize” reminder systems to maximize effectiveness as well as the cost-effectiveness of such a personalized reminder strategy.
Footnotes
Funding
This research received no specific grant from any funding agency in the public, commercial, or not-for-profit sectors.