
Abstract
This article examines the health information literacy of elderly Finns. The results are based on a survey conducted in January 2011. The questionnaire was distributed to 1000 persons that were randomly drawn from the Finnish Population Register. The respondents were aged 65–79 years (mean age 70 years) and lived in the Turku region in Finland. A total of 281 questionnaires (28%) were returned. χ2 analyses were used to find possible relationships between demographic factors, as well as interest, seeking activity, current self-rated health and different dimensions of health information literacy, including needs, seeking and use of health-related information. Significant relationships were found between education level, interest in health information, seeking activity, self-rated current health and dimensions of health information literacy. Some categories of elderly people are more vulnerable regarding obtaining and use of health information: those with lower levels of education, those with poor health, and those who are not interested in and active at seeking information. For people who are found in any of these categories, it is important that available health-related information is understandable and can be accessed without too much effort—something that information providers should take into account.
Introduction
People’s ability to obtain health-related information is considered important for how well they can take care of themselves. The concept of health literacy, typically used within health sciences and health communication, is often defined as ‘the degree to which individuals have the capacity to obtain, process, and understand basic health information and services needed to make appropriate health decisions’ 1 ; the focus is on the individual’s abilities to make decisions. However, there is also a definition where the cognitive and social abilities, and the aim to promote and maintain an individual’s health, are emphasised. The Health Promotion Glossary of the World Health Organization defines the concept in the following way: ‘health literacy represents the cognitive and social skills which determine the motivation and ability of individuals to gain access to, understand and use information in ways which promote and maintain good health’.2, 3
A related concept that describes health-related information behaviour, including needs, seeking and use of information related to health or medicine is health information literacy (HIL). The Medical Library Association 4 defines HIL as the ability to recognise a need for health information, to know how and where to find information about health, and how to evaluate and use this information in everyday life to make good health decisions. The concept is a combination of health literacy and information literacy. An information-literate person has, according to a widely used definition, the ability to determine the extent of information needed; access the needed information effectively and efficiently; evaluate information and its sources critically; incorporate selected information into one’s knowledge base; use information effectively to accomplish a specific purpose; and, understand the economic, legal and social issues surrounding the use of information, and to access and use information ethically and legally. 5 As with health literacy, within the concept of health information literacy the ability of a person to make decisions are emphasised, whereas information literacy, furthermore, includes the ability to use the information in a proper way, both ethically and legally. As a concept, information literacy was introduced in the early 1970s and has since spread from being used within information management in organisational contexts to also being common in other information environments. The approach is increasingly moving away from being focussed on individual skills towards including a social perspective, too. 6 Research on information literacy has mainly concentrated on information-seeking skills in educational or library settings.7–10 However, some studies have looked at work environments and people’s own perceptions of information literacy.11, 12 Information literacy in everyday life has, so far, been little studied. 13
Health information literacy is a fairly new concept that has been sparsely studied. Some studies have used the concept in order to describe information-seeking by students of medicine or health sciences.14, 15 The concept is also referred to in the literature without being based on empirical research. Cullen 16 presented the concept as a new approach to information literacy instruction for both health librarians and other information professionals. Burnham and Peterson 17 also used the concept in a library environment. Health-related information is, however, not encountered only in certain settings, which means that it is not unusual to have to cope with this kind of information from many different sources and angles. In these complex, and perhaps confusing, situations, we just have to do our best to master it. 18 It has, however, been shown that not everyone can master health information and be health-literate. A study from the USA found four performance levels of health literacy, ranging from proficient to below basic levels. Of those tested, 53% had intermediate, 22% had basic and 14% had below basic levels. Inadequate health literacy seemed to be more common in older age, while those aged 65 years and older had lower average health literacy, whereas those in the group aged 25–29 years had higher average health literacy. 19 An adequate health literacy might be crucial in older age, as it has been reported that inadequate levels of health literacy are related to worse self-reported physical function and mental health among seniors. 20
This study aims at measuring health information literacy in everyday life within a group of people that is growing, i.e., seniors. How do seniors perceive their ability to identify needs for health-related information and how confident are they that they are able to find and use such information? Are there differences in the perceived abilities and, if so, what lies behind them? Are demographic factors important or are there other factors that can affect the abilities to obtain and use health information?
Measuring literacies
Health literacy is often measured through standardised formulae, mainly concentrating on reading comprehension or the ability to read out words correctly. The Test of Functional Health Literacy in Adults (TOFHLA),21–23 or its short-form, s-TOFHLA, is the most commonly used test.24–29 Another test used for this purpose is the Rapid Estimate of Adult Literacy in Medicine (REALM). 24 Standardised tools, such as readability formulae, have been mainly tested in English, French or Spanish, and the tests are available only in English and Spanish. 30 Before health literacy can be tested in a non-English environment, a valid test has to be developed. For this purpose Baron-Epel et al. 25 validated a questionnaire measuring health literacy in Hebrew based on the s-TOFHLA. Chew et al. 31 developed another type of test, Health Literacy Screening Questions, which contained 16 questions that asked how often different kinds of patient materials are easy to understand, how often the respondents have problems in learning and understanding, and how confident they are to act on it. Peerson and Saunders 32 do, however, mention that these tests have been criticised by several researchers, and Zanchetta et al. 33 actually assessed health literacy in a simpler way by asking the respondents to assess their own level, after explaining what the concept means.
Although health information literacy has been measured in different ways, there are, so far, no standardised tests to evaluate health information literacy. Ivanitskaya et al. 15 used the Information Literacy Competency Standards for Higher Education 4 as a base when they developed the Research Readiness Self-Assesment (RRSA) in order to measure university students’ information-seeking skills on the Web, their ability to evaluate the obtained health-related information, their knowledge about plagiarism and their perceptions of their own seeking skills. Eriksson-Backa34, 35 has assessed everyday HIL by using questionnaires asking about people’s needs for health-related information, their use of information sources, perceptions of information quality, understanding of information, and knowledge and behaviour in health matters. An Australian study adopted a qualitative approach and studied how ageing Australians experienced HIL by asking them how they use information to learn about, and maintain, their health. 36 Niemelä et al. 37 have designed a 10-item tool for measuring everyday health information literacy by applying the Medical Library Association’s 4 definition of HIL. Respondents are asked to assess their needs for health information and perceived importance of it. Other statements cover the authority, reliability and use of both printed and Web-based health information. The topic in one statement is the degree of independence in health decision-making. 38 An addition to these tools is a question related to a diagnosis of dyslexia.
eHealth literacy is a concept that combines health literacy and also information literacy, along with an addition of traditional literacy, media literacy, computer literacy and scientific literacy.39, 40 eHealth literacy can be measured through the eHealth Literacy Scale (eHEALS) that consists of eight statements to be answered on a five-grade Likert-type scale ranging from strongly disagree to strongly agree. eHEALS measures how knowledgeable and comfortable people are at finding, evaluating and applying electronic health information to health problems, and how they perceive their skills in that context. 40
Current study
This article presents results from a survey conducted by self-administered questionnaires in January 2011 on a sample of 1000 Finnish seniors aged 65–79 years, who live in the Turku region in southwestern Finland. The respondents were a random sample drawn from the Finnish Population Register. The article explores the self-rated health information literacy of the studied population, i.e. how the respondents themselves perceive their ability to recognise health information needs and to find suitable information sources and use them, as well as to obtain, evaluate, understand and use health information. Health information literacy was measured in a way inspired by the eHEALS scale 40 and was determined by eight statements to be answered on a five-grade scale ranging from totally agree to totally disagree. The statements were as follows:
It is easy for me to decide in which kinds of situations I need health-related information
I know which sources to turn to in order to obtain health-related information
It is easy for me to find the health information I need from the information sources I use
I obtain too much health-related information
It is easy for me to determine whether health information is trustworthy or not
I learn many new things from the health-related information I obtain
I know how to use the health information I obtain to take care of my health
I often have difficulties to understand words or sentences used in health-related information
A total of 281 completed questionnaires were returned, leaving the response rate at 28%. The data was coded for PASW Statistics 18 for Windows (Microsoft, Redmond, WA, USA). The statistical analysis consists of χ2 analyses where p values of ≤0.05 were considered statistically significant.
Various factors, including demographics and health status, have been shown to be related to differing levels of health literacy.25–29 The current study examined how demographics (gender, age and education level), as well as motivation factors, i.e. interest in health information, seeking activity and current self-rated health, were related to the different dimensions of health information literacy. Seeking activity is considered to be a trigged motivation factor as it was strongly related to interest (χ2 = 185.233, p = 0.000). Previous research has also shown a strong correlation between interest in health information and seeking activity. 41 Current health is often considered a factor that is related to needs for, and seeking of, health information. It has been shown that changes in one's own health situation have given rise to increased needs for information.34, 42–44 Because the extremes (totally agree/totally disagree), in particular, in several of the HIL statements attracted only a limited number of responses, the alternatives ‘agree’ and ‘totally agree’, as well as ‘disagree’ and ‘totally disagree’, were grouped together for the analysis. For the same reason, the same was done with the extreme values for the motivation factors (e.g. ‘fairly’ and ‘very interested’ were grouped into one category).
Results
Demographics and motivation factors
Of the respondents, 43% (n = 122) were men and 57% (n = 159) women. The mean age was 70 years. For the analysis, age was categorised in three groups: 65–69 years (49%, n = 137), 70–74 years (32%, n = 90) and 75–79 years (19%, n = 54). The education levels varied, as 34% (n = 95) had a basic, primary education, 44% (n = 124) had a medium-level (secondary) education and 22% (n = 60) were educated to university level or similar. When the respondents were asked to rate their current health, 16% (n = 45) rated their health as poor, 36% (n = 98) as mediocre and 48% (n = 132) as good or excellent. Seven percent (n = 20) were only a little or not at all interested in health-related information, whereas 20% (n = 56) were moderately and 73% (n = 204) were fairly or very interested. Fifteen percent (n = 42) were a little/not at all active at seeking health information, while 23% (n = 63) were moderately active, and 62% (n = 173) were fairly or very active. When demographics and motivation factors were cross-tabulated, a significant relationship was found between education level and interest in health information (χ2 = 13.952, p = 0.007). More than 80% (n = 49) of those with the highest level of education were fairly or very interested compared with only 60% (n = 57) of those with a basic education. Gender was significantly related to both interest in health information (χ2 = 7.308, p = 0.026) and seeking activity (χ2 = 12.664, p = 0.002). Female respondents were both more interested (80%, n = 125, vs. 65%, n = 79, were fairly or very interested) and active (71%, n = 113, vs. 50%, n = 60, were fairly or very active). Those who rated their health as good or excellent (82%, n = 108) were also more interested in information about health (χ2 = 12.616, p = 0.013) than were those who rated their health as poor (58%, n = 26) or mediocre (69%, n = 67).
Demographics and health information literacy
When men and women were compared with regard to their perceptions of the different dimensions of HIL, hardly any differences between the two genders could be found. As can be seen in Table 1, it is only concerning confidence in their own ability to use the obtained information to take care of one’s own health (statement 7), that a significant relationship was found between gender and HIL dimensions. Women showed stronger confidence, as 54% (n = 86) of them, compared with 42% (n = 51) of the male respondents, agreed with this statement. The age groups showed no significant relationships at all with any of the HIL dimensions.
Demographics and dimensions of health information literacy
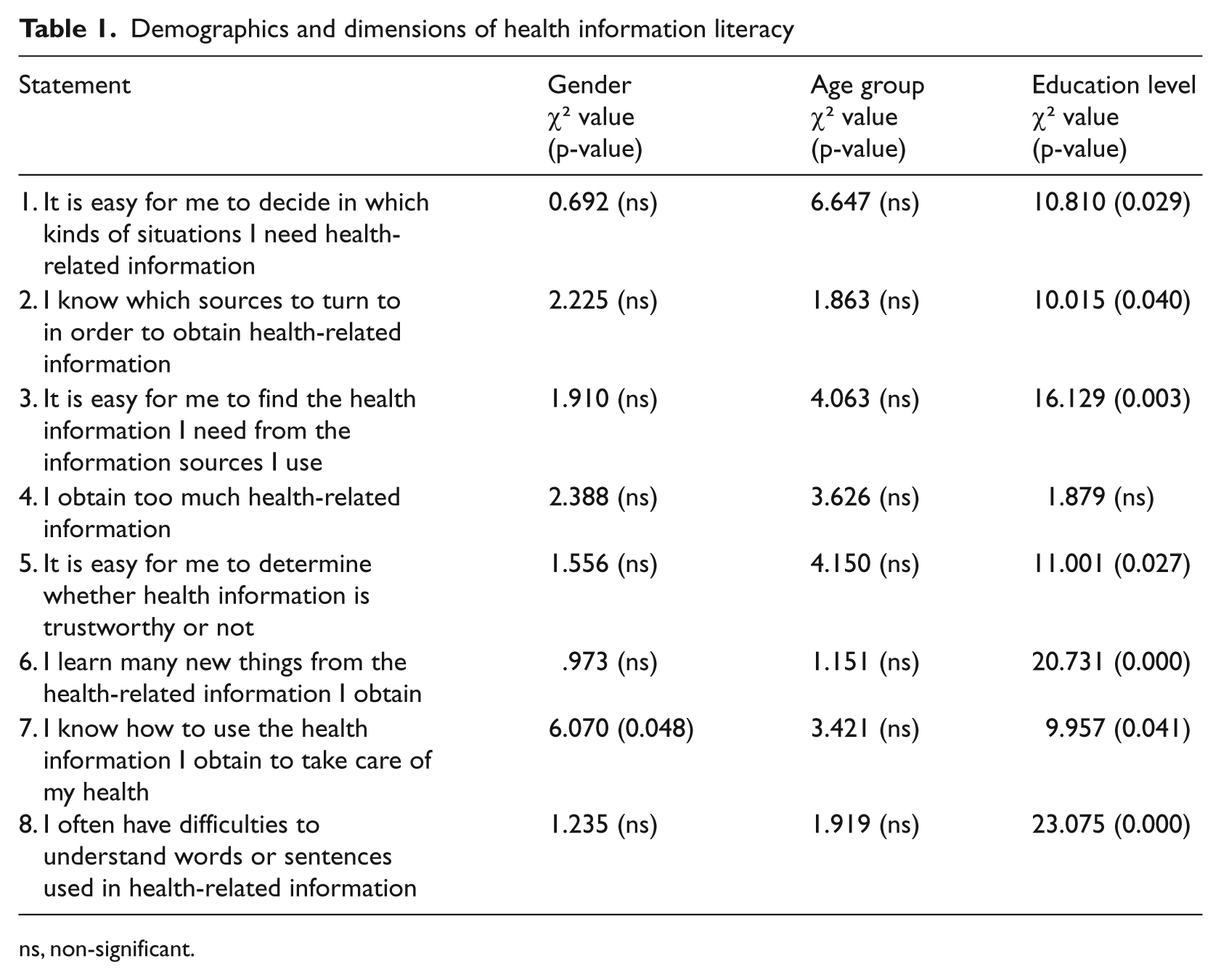
ns, non-significant.
Education level was, however, significantly related to most of the HIL dimensions (Table 1). Nearly 8 out of 10 (78%, n = 46) respondents with a high level of education agreed with statement 1: that it was easy to decide in which situations they needed health information, while this was the case among only 54% (n = 50) of those who had a basic education. Another 78% (n = 47) compared with 67% (n = 83) of those with a medium level education and 57% (n = 54) of those with only a basic education agreed that they knew which information sources to turn to (statement 2). Furthermore, 60% (n = 36) of the respondents with the highest level of education thought that it was easy to find the needed information (statement 3) compared with 43% (n = 53) of those with a medium-level education and 39% (n = 37) of those with a basic education. Those with only a basic level of education seemed to have the most trouble in determining whether an information source was trustworthy or not (statement 5), as more than a half (n = 49) disagreed with the statement saying that this is easy. In comparison, only 25% (n = 15) of respondents with the highest education level disagreed on this. A higher level of education also seemed to make it easier to learn from the obtained information (statement 6). More than half (53%, n = 32) in the highest education level group compared with less than 40% (n = 46) in the medium-level education group and only a third (n = 31) in the basic-level education group agreed with this statement. In the basic-level education group nearly 40% (n = 36) instead disagreed with the statement. Those who had the highest education level also seemed to be more confident in their ability to use the obtained information (statement 7); two-thirds (63%, n = 38) of the respondents in the highest education level group compared with only 38% (n = 36) of those in the basic-level education group agreed with this. Furthermore, education seems to be related to the ability to understand health-related information (statement 8); 60% (n = 36) of the respondents who were educated to a university level disagreed with the statement that it is difficult to understand terminology, whereas almost half (47%, n = 45) of the ones who had only a basic education instead agreed with this statement. Only statement 4, concerning information overload, was not significantly related to any demographic factor.
Motivation factors and health information literacy
Interest in health information was significantly related to some dimensions of HIL (Table 2). Slightly more than half (n = 104) of the respondents who were fairly or very interested in health information compared with a third (n = 7) of those who showed only little, or no, interest at all, thought that it was easy to find the needed information from the information sources they use (statement 3). Interest was also strongly associated with perceptions of abilities to learn from obtained information (statement 6), as well as of abilities to use this information for the benefit of one’s own health (statement 7). Half (n = 100) of the most interested respondents thought that they learn a lot from the information, while nearly 60% (n = 11) of the least interested ones disagreed with this statement. More than half (54%, n = 110) of the most interested respondents compared with a third of both the moderately (n = 19) and the least interested ones (n = 7) were, furthermore, confident that they knew how to use the obtained information.
Motivation factors and dimensions of health information literacy
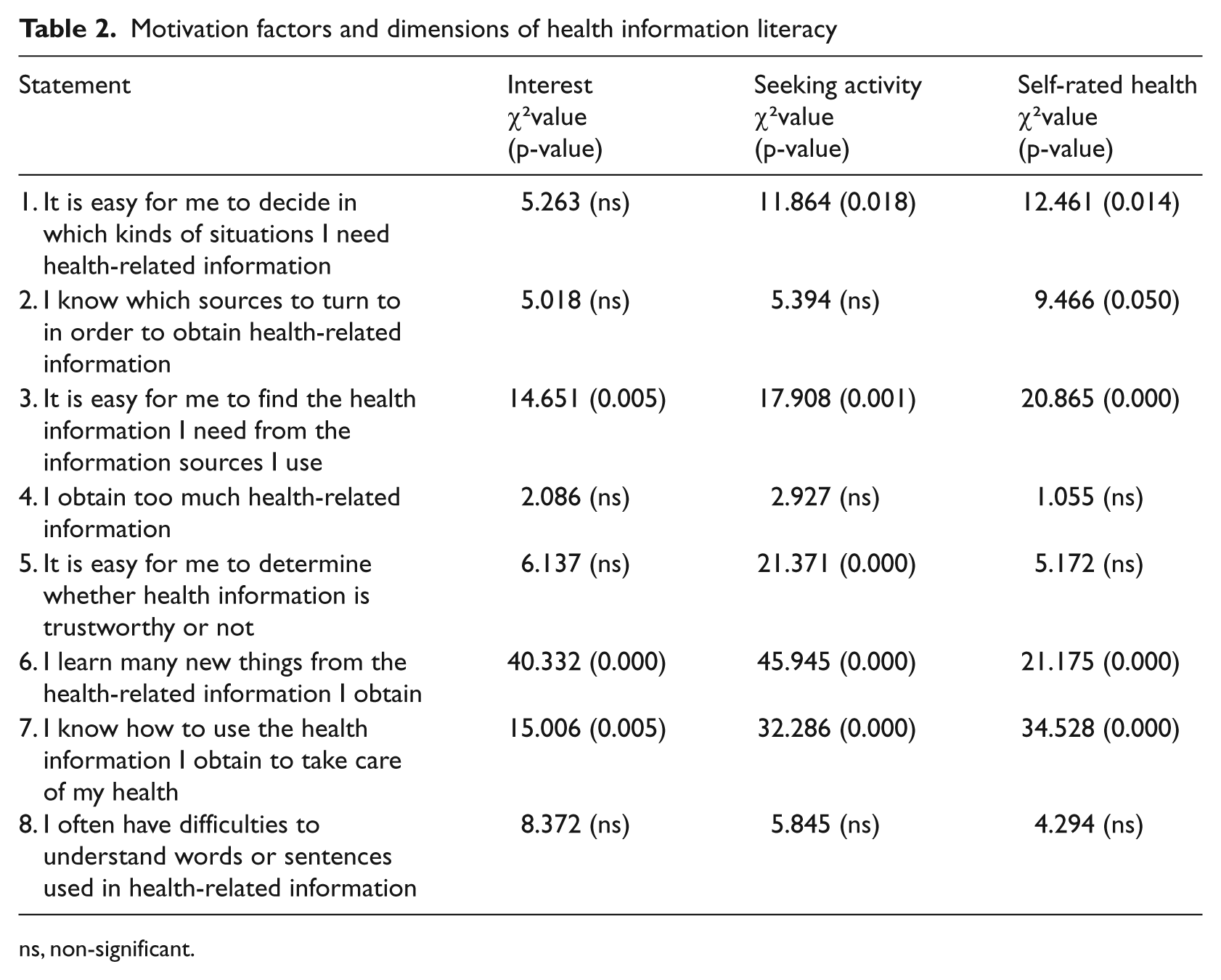
ns, non-significant.
Seeking activity was also significantly related to several dimensions of HIL. Nearly 70% (n = 115) of the most active seekers compared with about 60% (n = 25) of the least active ones and half (n = 32) of the moderately active ones agreed with the statement that it is easy to decide in which situations they need health information (statement 1). The least active ones were, however, most inclined to disagree with this statement (22%, n = 9). The most active seekers also agreed with the statement that they find the required information easily (statement 3) more often than did those in the other two groups (53%, n = 92, agreed, vs. 32%, n = 20, and 33%, n = 14 in the moderately and little active groups respectively). The least active information seekers seemed to have more difficulty than the other seekers in determining whether health information is trustworthy or not (statement 5); as many as 60% (n = 25) of the respondents in the least active group compared with only 31% (n = 54) of those in the most active group disagreed with the statement that it is easy to determine the trustworthiness. The ability to learn from obtained information (statement 6) is significantly related to seeking activity, as well; half (n = 88) of the most active seekers but only 22% (n = 14) of the moderately active ones, and 17% (n = 7) of the least active ones agreed with the statement saying that they learn many new things from the obtained information. In fact, as many as 56% (n = 23) of the least active respondents disagreed with that statement. Furthermore, the most active seekers were more confident in their ability to use the obtained information for their own health (statement 7). Whereas 60% (n = 103) of the active seekers agreed with this statement, only 29% (n = 18) in the moderately active group and 33% (n = 14) in the least active group did alike.
Current self-rated health was significantly related to several of the HIL dimensions, as well, as Table 2 shows. More than 70% (n = 94) of the respondents, who rated their health as good or excellent, compared with slightly more than 40% (n = 18) of the ones who thought that their health was poor, agreed that they knew how to decide in which situations they needed health information (statement 1). Nearly 75% (n = 97) of those who rate their health as good/excellent, but only half (n = 23) of the those with poor health thought that they could find information sources to turn to (statement 2). Those with good/excellent health (58%, n = 77, agreed, vs. 34%, n = 33 of those with mediocre health, and 36%, n = 16 of those rating their health as poor) also thought that they find the needed information more easily (statement 3). Furthermore, 52% (n = 68) of those with good or excellent health agreed with the statement that they learn a lot from the obtained information (statement 6), while only 31% (n = 30) of the respondents rating their health as mediocre and 25% (n = 11) of those with poor health agreed with this. Instead, as many as 41% (n = 18) of the respondents rating their health as poor disagreed with this statement. Poor health was also connected with difficulties in using the obtained information. While nearly 61% (n = 80) of those who rated their health as good or excellent agreed with the statement that they know how to use the obtained information (statement 7), this was the case with 45% (n = 44) of those with mediocre health and only 22% (n = 10) of those with poor health. In the latter group, 44% (n = 20) instead disagreed with this statement. As with the demographic factors, only one HIL statement was not significantly related to any motivation factor at all, and that was, again, the one about obtaining too much information (statement 4).
Discussion
This article presents results that show how seniors aged 65–79 years perceive their ability to identify needs for health-related information, and how confident they are regarding their abilities to obtain and use needed information for the benefit of their own health. Demographics and motivation factors, including interest in, and activities to, seek health information, as well as current self-rated health, were compared with different dimensions of health information literacy to find factors that are possibly lying behind differences in HIL. Education level was almost the only demographic factor that was related to the different dimensions of HIL, as seven out of eight statements were significantly related to this factor. Age group had no significant relationships with any HIL dimension at all and gender was also only connected to confidence in the ability to use obtained information in order to take care of one’s own health.
The so-called motivation factors (interest, seeking activity and self-rated health) were found to be related to several HIL dimensions each. The actual seeking skills of the respondents were not tested in this study, but self-confidence regarding seeking and use of health information was assessed. Motivation is an important factor and it may not be surprising that those who are more motivated, i.e. interested in health information and more active at obtaining it, are also more confident in their ability to do so. Lack of knowledge or confidence to seek health information has been shown to be a barrier to obtaining such information. 45 Being more active at seeking information means that a person is more used to seeking information and hence he or she can be expected to be more confident in the own skills. One interesting finding is that those who rated their health as being good or excellent were also more confident in their abilities to find and use information. Deteriorating health is often mentioned as a reason for increased needs for information and seeking of it,34, 42–44 but in this study those who had poor health seemed to be more discouraged to even seek and use information. Other studies have, however, found that it is not uncommon that people seek information about health matters not only because they feel unwell, but because they have a general interest in the matter.34, 46, 47
To our knowledge, no previous studies have assessed health information literacy in the same way as this one. Hence, the results cannot be directly compared with those of previous studies. Some small-scale studies have, however, used similar questionnaires and have been applied to the same age group. A small-scale study of retired Finns showed that the female respondents were more confident that they knew how to take their medication after having read the patient information leaflet or the prescription. Men were more likely than women to think that some information is often, or fairly often, contradictory and confusing. Those who had the lowest level of education found it more difficult to evaluate information and they more often thought that health-related information was confusing and contradictory. 35 Also, in the current study, the female respondents were more inclined to think that they knew how to use the obtained information for the benefit of their health and a higher level of education was connected to several of the HIL dimensions. The other dimensions of HIL were not significantly related to gender, although it was found that women, like in other studies, 41 were more interested in, and active seekers of, health information than men. In a study describing health information literacy among young adults in differing health situations, it seemed that those who were more active at seeking information were also more health information literate and showed better knowledge levels and health behaviour. 34 In the current study, seeking activity was significantly related to the ability to decide when information is needed, to find information easily, to evaluate the obtained information, and to both learn from and use information.
Research on the understanding of health information, i.e. health literacy assessed by tests measuring especially reading comprehension, show that various demographic factors affect understanding. In a population of Israeli patients, those who had lower levels of education, women and older respondents had significantly lower levels of health literacy. 25 Baker et al. 48 found dramatic differences in functional health literacy across age groups while testing elderly people with s-TOFHLA. The scores for those aged 65–69 years were much higher than for those who were aged 85 years or older. Furthermore, the number of school years correlated highly with health literacy. Gazmararian et al. 26 found a strong relationship between age and years of school, respectively, and inadequate health literacy. In the current study, mainly education level was significantly connected to abilities to seek and use health information, whereas age showed no significant associations. Because health literacy and HIL are measured in different ways, one should be cautious in comparing the results. It is, however, both interesting and alarming that education is so important, not only when it comes to understanding health-related information, but also when seeking and using it. Some of the available information can actually be directed towards people with higher education. Studies do, for example, show that in order to understand patient information or to profit from medical information on the Internet, a fairly high level of education is required. 49,50 It seems that a higher level of education is important, as people who had a better education were more confident in their ability to master available health-related information. This could, however, mean that those with lower levels of education are not only experiencing more difficulties in obtaining and using health information, they could also be discouraged from even trying to obtain such information.
Studies examining health literacy among people with different kinds of health problems have found that poor health literacy is common among patients with chronic medical conditions, such as type 2 diabetes, asthma, AIDS and hypertension.26, 28, 29, 48 In the current study, HIL was also more advanced among those who rated their health as better. The fact that those with poor health experienced more difficulties in seeking and obtaining health information is a matter of concern, as those with poor health might need health-related information more than others. In conclusion, there seem to be some categories of elderly people who are more vulnerable when it comes to obtaining and using health information: those with lower levels of education, those with poor health and those who are not interested to seek out information actively. To seniors who are found in any of these categories, it is important that available health-related information is understandable and can be accessed without too much effort, and providers of health and medical information, both within the healthcare context and information services, should take this into account.
There are limitations to this study. Firstly, the response rate was moderate, and those who responded tended to be quite interested in health information and active at seeking it, as well as rating their health as mostly good or excellent. There were also some inequalities in the gender ratio, with women being more eager to return the questionnaires. Secondly, it could be discussed whether you can actually assess people’s health information literacy by using a tool that contains only a few statements and that does not concern any specific situation but refers to any health-related information at any time. However, the aim was to assess HIL in everyday life, not in any specific context. The null hypothesis might, furthermore, be true (Type 1 error) for some testing results, hence the statistical significance was set at 0.05 and the number of tests conducted was relatively high (48). Even so, the findings of this study shed light on a number of statistically significant connections, and they give rise to questions on whether similar associations can be found among larger populations and people in other age groups as well.
Footnotes
Acknowledgements
The advice given by Dr Peter Bath at the University of Sheffield during the planning of the study and the design of the questionnaire are greatly acknowledged.
Funding
The Research Institute of Åbo Akademi Foundation granted financing for part of the data gathering. The study is conducted as a part of the research project Health Information Practice and Its Impact (HeIP), financed by the Academy of Finland during 2008–2011.