
Abstract
Patients with chronic disease may suffer frequent acute deteriorations and associated increased risk of hospitalisation. Earlier detection of these could enable successful intervention, improving patients’ well-being and reducing costs; however, current telemonitoring systems do not achieve this effectively. We conducted a qualitative study using stakeholder interviews to define current standards of care and user requirements for improved early detection telemonitoring.
We determined that early detection is not a concept that has informed technology or service design and that telemonitoring is driven by the available technology rather than by users’ needs. We have described a set of requirements questions to inform the design and implementation of telemonitoring systems and suggested the research needed to develop successful early detection telemonitoring. User-centred design and genuine interdisciplinary approaches are needed to create solutions that are fit for purpose, sustainable and address the real needs of patients, clinicians and healthcare organisations.
Introduction
Chronic disease accounts for a significant and increasing proportion of morbidity and healthcare resource use around the world. 1 Some conditions e.g. heart failure and chronic obstructive pulmonary disease (COPD) are punctuated by instances of sudden deterioration which may require hospital admission and result in an overall worsening of the patient’s enduring health. These exacerbations account for a large part of the burden of certain diseases2,3 and are considered to be partly preventable, or at least reducible, if deterioration could be detected sufficiently early and appropriate treatment provided.
Detecting deterioration in a patient’s health status requires monitoring which, for most patients, consists of the patient or their carer assessing the point at which symptoms become troublesome enough to warrant medical attention. However, patients may be in denial of their condition or unable to recognise an impending deterioration. 4 In order to provide more reliable and early-as-possible detection, patients’ self-awareness could be replaced or supplemented by a more objective method using technology to collect patient data and facilitate assessment. This has variously been labelled telemonitoring, home monitoring, telehealth, remote monitoring or telecare. 5
There have been many trials of telemonitoring for patients with chronic diseases. Whilst there are indications of clinical benefit in some conditions, high quality evidence of consistently improved outcomes6–8 or cost-effectiveness9–11 is lacking and telemonitoring is in general still failing to make the transition from pilot studies into mainstream practice.12,13 Such trials have also not addressed the core issues of early detection: what are the characteristic indicators and how should these be collected and analysed?
As part of a larger project, this study aimed to use stakeholder engagement to identify: (a) the current state of the art of chronic disease management; and (b) to define the requirements for an ideal early detection monitoring system and then suggest some further research needed to achieve this. In other work, we have combined this information with literature reviews, patient focus groups and roadmapping exercises to create a research programme to guide further work.
Method
Qualitative fieldwork methods were used to gather information about current front-line chronic disease healthcare. We used semi-structured interviews with key informants to explore the issues around early detection using three common chronic diseases as exemplars: heart failure, COPD and diabetes. These conditions affect large patient populations and consume significant healthcare resources, so improved detection and prevention of deterioration in these could result in significant benefits.
Proposed sample
We selected participants using a purposive approach. Informatics and telehealth conferences, professional networks and snowball sampling were used to identify key opinion leaders in the following fields: health informatics and technology; policy leads in this field; health service researchers; and clinicians familiar with the exemplar conditions.
Data collection
The interview schedule addressed the following issues: which are the best indicators (signs or symptoms) for early detection of deterioration; when to initiate monitoring; how to collect data, analyse and store it; how to act on detected events (alerts); what are the patient or clinical issues with the use of such technologies; which research questions remain unanswered? The interviews were audio recorded, transcribed and summaries provided to interviewees for endorsement.
Analysis
Thematic analysis was conducted on the transcripts: inductive coding and categorisation were undertaken before the development of identifiable themes, using a constant comparison method. 14 A collaborative approach was taken: discussion amongst the research team was facilitated by outlining themes using concept maps 15 until consensus was reached regarding synthesising and summarising the data.
The requirements for early detection telemonitoring were identified by approaching the results of the thematic analysis with the following questions:
What are the shortcomings of existing care for patients with chronic conditions?
What are the characteristics of a successful early detection monitoring system?
We then outlined a set of research questions by asking:
C. What research is required to overcome A, and achieve B?
Results
Participants
Twenty-six key informants from across the UK were interviewed (Table 1). Eighteen had a clinical background, seven of these in nursing, of which four worked as community-based nurses providing care for patients with chronic diseases. Eight informants had experience in health informatics, four were policy leads in the National Health Service (NHS) and nine had experience with recent telehealth programmes. Two informants were academics involved in medical technology development. The interviews took place between June and November 2008 and lasted approximately 90 minutes each.
Informant characteristics.
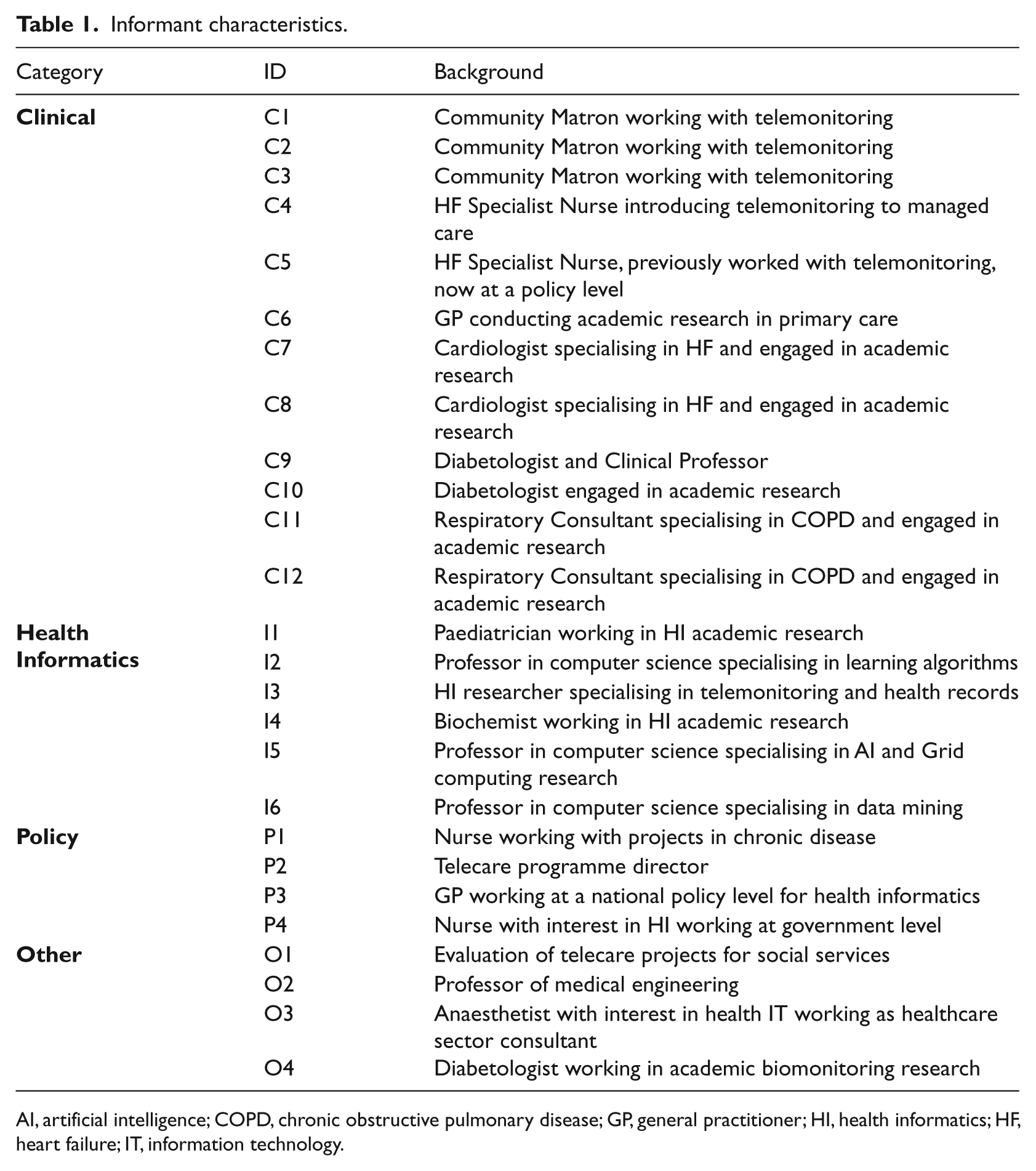
AI, artificial intelligence; COPD, chronic obstructive pulmonary disease; GP, general practitioner; HI, health informatics; HF, heart failure; IT, information technology.
Thematic Analysis: structure
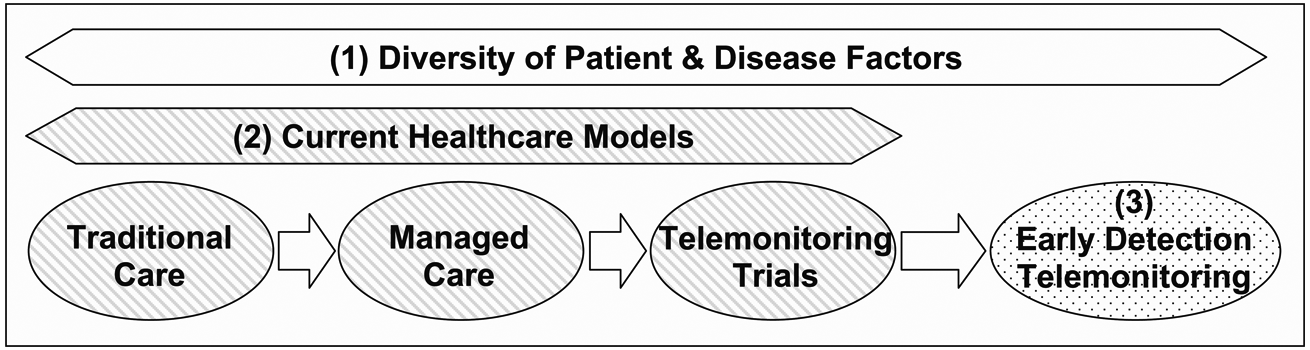
Interviewees emphasised the complexity and diversity that characterised patients suffering from chronic conditions. It became apparent that a successful technological solution must take account of these factors in order to be clinically effective and widely adopted. Also, there were wide variations in current care practices; the analysis identified three existing models of care—traditional, managed and telemonitoring— which can be considered as evolving towards early detection monitoring.
The results of the analysis were therefore categorised as three broad themes (Figure 1): ‘Theme 1 - The Diversity of Patient and Disease Factors’, describes the characteristics of chronic diseases and the patients who suffer from them; ‘Theme 2 - Current Healthcare Models’, describes existing healthcare models and their drawbacks; and ‘Theme 3 - Early Detection Telemonitoring’, describes participants’ ideas for the characteristics of an ideal future system.
Thematic analysis results
Theme 1 - Diversity of Patient and Disease Factors
The informants emphasised that patients with chronic disease have complex needs and often suffer multiple-morbidity. Many patients are elderly, and physical and cognitive health problems may pose significant challenges to the tasks of self-management. A patient’s psychological status and level of social support also affects their ability to manage or monitor their health. For example, many patients with chronic disease suffer from anxiety or depression:
“[they] become dependent very quickly because they’re frightened. They’re frightened by what’s happening to them…it’s not what they planned.” [Informant C3]
In contrast to this are those expert patients who have high levels of self-awareness and prolonged experience of effective self-management. Variability such as this, is characteristic of the patient population (e.g. wealth, health literacy, language, location) and can impact an individual’s access to healthcare and their ability to make use of it.
Patients may alternatively deny their condition, resulting in poor compliance and delay in seeking advice. Informants noted how changes in symptoms that herald deterioration can be missed, ignored or misinterpreted and that it can be difficult for patients who are constantly unwell to distinguish a gradual decline from their usual day-to-day variability.
“Top of the list of things to sort is communication…people not understanding what they were meant to do, not understanding the early warning symptoms…” [P1]
Theme 2 - Current Healthcare Models
There is a spectrum of care models currently in use for patients with chronic disease (Figure 1). ‘Traditional Care’ operates in a fragmented way and the majority of patients are managed by general practitioners (GPs). ‘Managed Care’ describes the use of case-management, typically where community nurses provide co-ordinated care to small numbers of high risk patients. ‘Telemonitoring Trials’ are implemented (in the experience of our informants) primarily as additions to managed care and often include very small numbers of selected patients.
Traditional Care
Typically, when patients move between healthcare sectors and specialities there is limited, if any, access to existing clinical information in other organisations, for example the GP medical record. The lack of information creates uncertainty and can lead to risk-averse decisions, especially out-of-hours.
“Nobody knows really what’s wrong with that patient… they just end up getting hospitalised because nobody wants to make a decision, because the communication pathway’s not there…” [C5]
It also leads to duplication of effort and information; where information is maintained within clinically-defined silos and patients follow single-disease pathways.
“…many professionals came to interview her…each one of them asked very similar questions but…they only took a certain view…and not one of those professionals have the complete picture…she only told them what they asked her…” [P4]
Although GPs and community nurses are in a good position to have a holistic view of the patient, including their social and behavioural context, this information is seldom available to other professionals. The informants painted a picture of fragmented care where information sharing was virtually non-existent; there are significant barriers owing to concerns about data security and confidentiality, and to a lack of trust in information collected by others or difficulty in interpreting it.
Informants also described a paternalistic attitude in some health professionals which can encourage patient dependency. Such professionals may also be dismissive of information collected by patients, impacting on their motivation for self-care.
“…for weeks and days people have been filling up their [records]. They go along and sometimes it’s not even looked at. Other times, ‘Mmm, that looks quite good. You’re doing fine’, and handed them back. These are the sort of people that say ‘I’m not going to bother doing that any more’.” [P1]
Managed Care
Case managers attempt to span the boundaries described in Traditional Care and provide a single point of contact for the patient. Informants described how obtaining clinical information from other NHS providers and implementing integrated patient management across fragmented services and information sources was difficult.
“You’ve got the acute NHS Trust, you’ve got the Primary Care Trust, you’ve got Social Services, you’ve got, you know, whoever else, maybe the private agencies, all of whom will have issues about sharing information...But I think the people on the ground couldn’t care less and would just like it to happen.” [C3]
There was consensus that better communication of patient information between professionals was a key factor in providing improved care, as was communication of information to the patient. Case management includes elements of patient education and mentoring whereby the patient is encouraged to take increased responsibility for their health. Improved motivation and self-management can ensue from this:
“The patient themselves is an untapped resource…” [P4]
Familiarity with individual patients and their circumstances was noted several times as being an important factor in successful case management. Having a holistic and personalised approach to each patient provided contextual knowledge that can have diagnostic value in detecting clinical deterioration, for example by identifying changes in a patient’s appearance or behaviour.
Telemonitoring Trials
Telemonitoring was seen as an example of technological push, whereby developments are driven by commercial interests rather than a careful analysis of patient and clinical needs.
“People started introducing the technologies. Then they go and look for a group of patients to use it on, and finally they talk to the people trying to provide the day-to-day services to those patients and shoehorn it into their process…” [P3]
This can result in clinicians feeling the systems are not relevant to them.
“…it is rubbish though, because it doesn’t help anything…” [O4]
There was a clear desire amongst informants for clinicians to be involved in the early stages of development and for forward planning of its implementation.
In the experience of our informants, telemonitoring comprised patients measuring their physiological variables, such as pulse rate and oxygen saturation and answering questions about symptoms. This information was then transmitted to a central database where it was inspected daily, usually by a nurse. In such systems automation is limited to highlighting measurements that cross individually set thresholds. When this is observed, patients are contacted by telephone. Most of these were run by Primary Care Trusts. Telemonitoring projects were often seen as small-scale, theory-poor and not rigorously planned or evaluated. Trials were criticised for being conducted with a finite mindset, so that telemonitoring was isolated from usual care, had no protocols for managing emergency care and lacked planning for the project end.
Current systems are limited in their ability to accommodate the variability and complexity of patients. The available technology dictates the use of generic physiological indicators (vital signs) that can only provide limited information about the health of the patient, although clinicians have some choice about which indicators to apply and set thresholds relevant to an individual patient’s ‘normal’ status.
Symptom monitoring was felt to be very valuable.
“… a gentleman recently whose vital signs were absolutely spot on…but his answers to the questions were dreadful. When I went to see him he was having more angina…but when he was actually doing his readings he wasn’t having chest pains” [C2]
However, it was also noted that symptoms are unlikely to provide optimal early detection.
“…if you could detect something in someone’s voice [e.g. difficulty in breathing] you wouldn’t be detecting it early. At that stage it’s progressed…” [C1, C2]
The stated aims for the use of telemonitoring included reducing hospital admissions, titrating medication and improving staff efficiency. Early detection of deterioration was not identified as an explicit aim although it is clearly implied in the hope that monitoring would lead to reduced admissions. Nevertheless, there was clear enthusiasm for telemonitoring amongst existing clinical users and this support was based on the benefits for patients’ quality of life and case-managers’ work processes.
“We don’t want it taken away. It helps us do our job more effectively.” [C1] “…the more information you have, the more empowered you are to actually respond effectively and appropriately…” [C3]
In general, informants indicated that patients were accepting of the technology, although patient selection could have biased these findings. Informants reported that telemonitoring:
“Gives them [patients] confidence and empowers them to be…have more of an understanding.” “They get to know what’s normal for them.” “Reduces their anxiety…and also it really, really supports education around their disease.” [C1, C2]
Theme 3: Early Detection Telemonitoring
All the telemonitoring systems discussed in the interviews comprise a common set of components and relationships (Figure 2). Participants’ requirements for future systems that could effectively achieve early detection of deterioration are reported according to these.

Telemonitoring model components
Patient and purpose: appropriate targeting according to the aim
Informants emphasised the need for telemonitoring to have improved clarity of purpose and better criteria for the type of patients for which it is suitable. Telemonitoring will not be suitable or available for all patients with chronic diseases, therefore matching of the aim of the implementation (health promotion, staff efficiency, clinical outcomes) with the target patient population is important.
“We have to be very clear about who we select, why we’re monitoring them, what questions we want answering and what action we would take with that question?” [O4]
Monitoring for early detection of deterioration should target patients at high risk of admission. As this is only partially related to disease severity, multiple risk factors need to be assessed to determine the most appropriate patients.
The patients suitable for monitoring could change over time as a result of improvement or progression in a patient’s clinical condition, changes in their social circumstances, or as technology advances. Participants were also convinced that certain groups of people should not be monitored, e.g. the ‘worried well’, end-stage patients and long-term stable patients.
“The whole point of technology is to empower people, not to tell people they’re sick when they actually feel quite well.” [C2]
Sensor: usability and novel modalities
Many existing commercial physiological sensors are cumbersome and their use poses a burden to patients. Usability of telemonitoring for patients was considered to be important. Informants envisaged a future where sensors would be less visible, capable of measuring multiple parameters simultaneously, would require low power or be self-powering, be capable of on-board data storage and analysis and be able to transmit data wirelessly and securely. Such sensors would not restrict freedom of movement (‘free-living’), whereas current equipment often ties the patient to the home.
“For some of those telecare things we are talking about fixing you to your own house…in a world where people are increasingly mobile, or indeed mobility is a sign of wellbeing and independence.” [P2]
Free-living sensors are in development, including those incorporated into garments, but are currently a long way from robust, reliable and commercial application.
Given the emphasis placed on contextual knowledge by case managers, future systems should also be capable of capturing ‘soft’ parameters more effectively (symptoms, behaviour, mood, appearance) and may include detection of events that can lead to deteriorations (medication errors, infections, environmental changes).
Signals: intelligently selected indicators in reusable formats
Clinical participants had clear ideas about parameters that may provide useful early detection information in future for specific conditions: inflammatory biomarkers in COPD, B-type natriuretic peptide (BNP) or electrocardiography (ECG) analysis for heart failure, and blood glucose surrogates or lipid measurements in diabetes. Although given the complexity and variability of many patients with chronic disease there was little confidence that telemonitoring could achieve “distant diagnostics” [C8].
“There’s probably only about 10 vital signs that might be useful, might just give me a bit more clue as to how bad somebody was.” [P3]
Appropriate deterioration indicators may also vary between patients with similar conditions.
Chosen indicators appeared to be monitored because they could, rather than because they should. A consistent view was that data was often collected without a clear aim or consideration of relevance and that the questions that are important to clinicians are not sufficiently addressed.
“What we really want is a very good way that lets clinicians articulate the questions they want answered.” [I5]
Data should also be fit for its defined purpose: authenticated, of appropriate quality (e.g. signal-to-noise ratio), and with context (metadata that allows interpretation of the data). Data collected for one purpose can be reused (e.g. for audit or research) and shared with others if it conforms to a common standard (e.g. HL7 CDA, IHE XDS, EN 13606), permitting interoperability across different devices/databases and facilitating semantic interpretation.
Analysis: automation, personalisation and diagnostic signatures
Informants stressed the importance of establishing individual baselines, as patients who are chronically ill are unlikely to conform to population norms. Establishing these in complex patients would require clinicians to identify ‘wellness templates’ of data patterns.
“…at the early stages [of learning] it’s not possible to do the automation. You have to have the clinician’s judgement.” [I6]
The parameter changes (signatures) that would reliably indicate an incipient deterioration in conditions such as heart failure and COPD have not been characterised and analysis methods capable of learning individual data signatures for each patient may be required. Algorithms that use multiple parameters, statistical or pattern-matching methods are under development, but such automation is lacking in commercial systems. This is partially because of the difficulty of encoding clinical expertise. Informants sometimes referred to being ‘familiar’ with a patient, to expertise that can’t be taught and to ‘intuition’ telling them that the patient’s condition has worsened. In addition, the difficulty of achieving true interdisciplinarity and cooperation between informatics scientists, system engineers and clinicians is a significant challenge to developments in this field.
“…there’s still a disparity in, sort of, beliefs between physicians and engineers..[engineers] think they can make the round peg go through the round hole and that’s….that’s the problem solved.” [O4]
Alerts and information representation: accuracy, patient involvement and usability
Accurate analysis is insufficient by itself. Trust must be established that the analysis leads to reliable alerts and that health professionals can use it to provide appropriate responses. This is more difficult to achieve in automated systems than for human-controlled systems.
“To trust it you have to understand it. Or do the trials....and see if it works.” [I2]
The accuracy of alerts is a critically important issue for automated monitoring systems. False positives can result in increased clinical workload, unnecessary treatments and reduced trust in the telemonitoring system and should be minimised. However, there will always be situations which have not been anticipated and allowed for, but which are not clinically significant. False negatives are potentially more hazardous, whereby patients remain untreated for a real health crisis. These are handled in current systems by attempting to ensure that patients do not become dependent on the technology. Patients should understand that they are not under continuous observation and that they must not rely on the monitoring to detect and notify health problems in lieu of self-reporting.
In current telemonitoring technology, the patients are relatively passive and do not often have access to their own monitoring information. Informants suggested an alternative to this in which the data and alerts can be delivered direct to the patient, either with or without a health professional being informed. This has the advantage that it can increase patient responsibility and potentially their motivation for self-care.
Usability of hardware, analysis and outputs is key if a telemonitoring system is to find widespread use. Clinicians and patients are more likely to use a system if it is robust and intuitive to use.
“The idea is to make the system complex, but make it simple to use…” [I6]
Information should be presented in a way that is comprehensible and meaningful and does not increase workload or anxiety. Multiple levels of complexity and detail in a single system could be employed to meet the needs of multiple users. More sophisticated analysis methods would also enable hierarchies of alerts to be delivered to different actors depending on the severity or urgency of the situation.
Response: planned and integrated into care structures
Several informants believed that the first response to an alert should always be telephone contact with the patient to rule out poor measurement technique, forgetting to monitor or lifestyle factors that don’t require clinical action. Responses to alerts should be planned in advance, but clinical judgement should be able to override protocols. However, the telemonitoring model does not fit comfortably with the current structure of UK care organisations where the role of responder is not defined. Most previous and current evaluations of telemonitoring are small-scale and exist in isolation from the normal service model.
“Generally they were quite poorly integrated, unfortunately. Just within that unit where they were happening, or just within that hospital. There were no links to primary care or to social services or to anywhere else.” [I3]
However, large-scale implementation into existing services would require detailed specification of who should be responsible for receiving an alert and how to take and document the most appropriate action. Some informants indicated that it could be necessary to re-organise care systems to allow implementation of the telemonitoring model.
“I can’t emphasise enough this business about getting the service model right first…” [P3]
Some informants had concerns about the medico-legal unknowns of clinical governance and accountability for the detection pathway and patients’ welfare.
“…If I request that one of my patients has a continuous monitor the onus should be on me to ensure that that data is handled responsibly. That doesn’t necessarily mean that I should be looking at it….I don’t know how it’ll work.” [O4]
These issues will become more challenging as increased mobility of patients and sensors results in telemonitoring crossing more organisational and geographical boundaries and being distributed over many providers.
Data storage: volume, control and interoperability
Telemonitoring has the potential to create large volumes of data, particularly if continuous free-living monitoring is used. The storage requirements will additionally depend on the data quality and format – whether it is kept in its original format or aggregated. There was no consensus amongst informants whether advances in storage capacity and data compression would keep pace with increasing volume demand.
Informants with informatics backgrounds did not favour centralised records, but distributed systems are not currently effective. Many envisaged a future with linked and virtualised multiple health records with easy access and the details of implementation hidden from the user.
“I don’t care how it happens, I just want it to happen. Because it’s very frustrating and time consuming at the moment trying to ferret out all the information.” [C3]
Interoperability of stored data allows for information-sharing and re-analysis, but also raises the issue of consent for secondary purposes. Several informants voiced the opinion that patients should have control or ownership of their telemonitoring data and that there should be processes for clinicians to access it when needed. Increasing information-sharing and integration of care across organisations will require details of control, access, privacy and security of health data to be resolved.
“You don’t want to share everything… sometimes the challenge of what you think the other professional needs and what they actually want is quite difficult to identify.” [P4]
Summary and synthesis
The description of Current Healthcare Models indicates that most of the drawbacks of existing systems are not technological but social, organisational and political. Fragmented care leads to information silos, to a lack of trust between organisations, specialities and roles, and to simplistic and unrigorous local pilots of telemonitoring. Clinical engagement is absent in the design of these, resulting in telemonitoring systems that are inflexible, provide limited information and are relevant only to niche patient groups and clinical applications. The use of current telemonitoring systems appears to be mostly opportunistic rather than a deliberate effort to inform clinical decision-making and the complex and diverse needs of patients and multiple clinical roles are not accounted for. However, this technology is still capable of providing benefits to some users.
The concept of early detection was not explicitly included in managed care or telemonitoring trials although such systems should initiate clinical intervention before a patient requires hospital admission. Telemonitoring was generally implemented as a test of usability and involved basic vital signs and symptom monitoring combined with manual data inspection and interpretation. Symptom changes and other ‘soft’ parameters associated with close familiarity with the patient appear to have high diagnostic sensitivity, but these are also late indicators of deterioration.
We present a generic model of a telemonitoring system (Figure 2). By questioning each component of this in depth we can define the specifications for an improved telemonitoring system capable of accurate early detection, wide applicability and successful adoption (Table 2). However, the process of answering these questions should take into account the nature and needs of the users (patients, clinicians and organisations), which so far appears to have been perfunctory at best:
Patients: the complexity and diversity of people suffering with chronic disease; personalisation of provision must replace the one-size-fits-all approach;
Clinicians: what clinicians actually want/need; ‘clinical pull’ must replace ‘technology push’;
Organisations: match systems with organisational structures and established roles to become integrated into standard care.
Requirement questions and research outline.
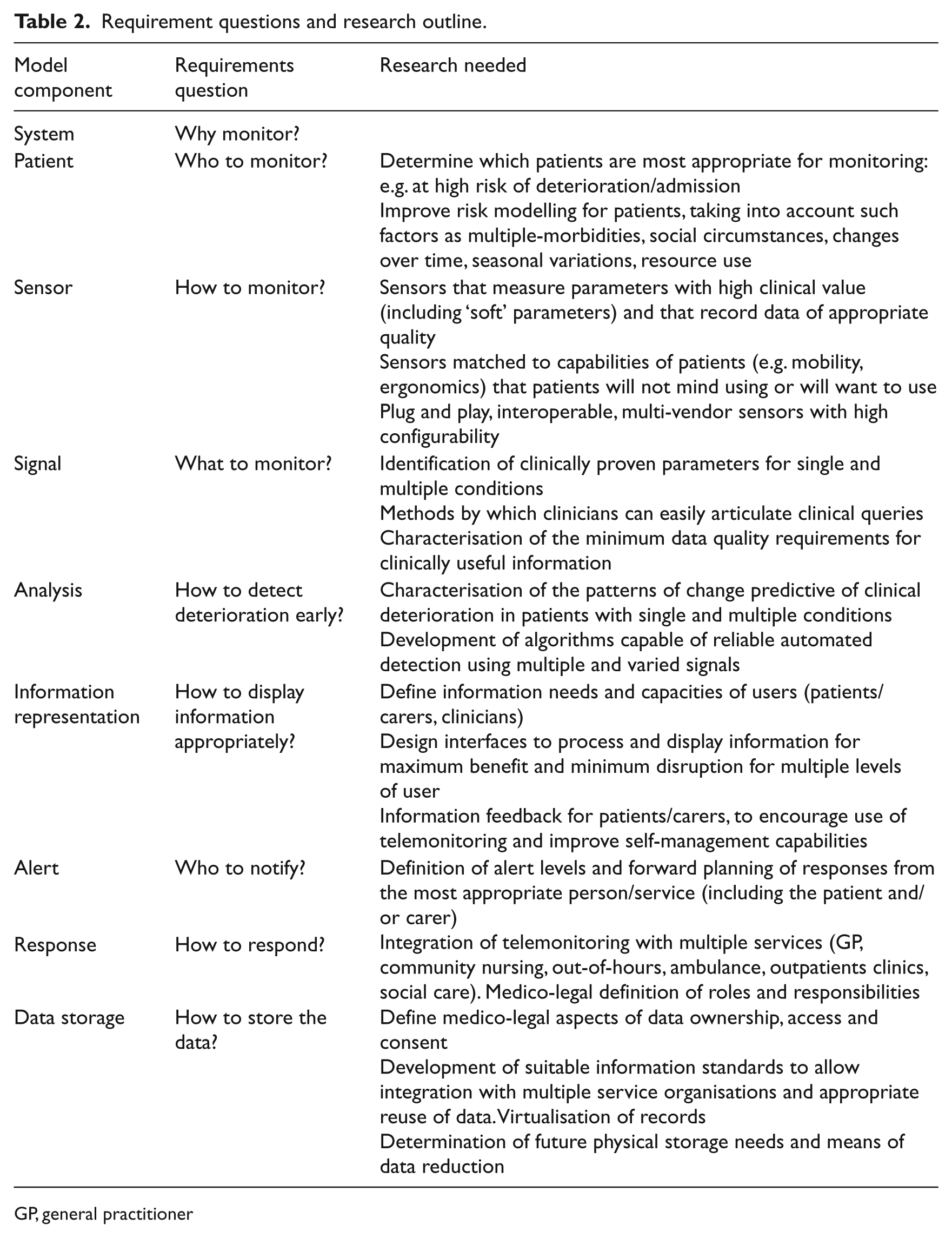
GP, general practitioner
Table 2 also shows how these questions can be used to define the research needed to achieve such a system. To accomplish effective design, genuine interdisciplinary working between engineers, informaticians and users must become an essential part of the process and may also involve professionals from other specialties (e.g. sociologists and psychologists). Making assumptions about what users want or need, or employing cursory requirements analysis, is unlikely to produce systems with high usability and has created technologies that can be perceived as disruptive and unhelpful.
Discussion
Principal findings
Early detection as a driver for introducing telemonitoring was not a concept our participants recognised. Small scale telemonitoring trials had resulted in improved staff efficiency and patient empowerment but there were concerns that these services were driven and constrained by technological developments and commercial availability rather than by clinical need. Telemonitoring systems had not overcome the drawbacks of traditional care because they existed as an off-the-shelf ‘bolt-on’ and could not be connected with many of the different care services that these patients engage with. A future early detection telemonitoring system should be designed with high levels of user input and therefore be characterised by high usability and integration with multiple services. The technical requirements include more versatility of monitoring capabilities and proven automated methods of pattern detection.
We have defined the components of a generic telemonitoring system and a set of questions that should be considered when designing or implementing such technologies. We also proposed a series of research topics which will address these questions for an early detection telemonitoring system. Suggestions for further research have been outlined, but not prescribed. For example, the analysis to automatically detect changes in patient status could use knowledge-based algorithms or machine learning methods. The important aspect is that the questions are addressed with scientific rigour where appropriate (e.g. in determining the most suitable clinical indicators) and with users’ needs as a major design factor.
Strengths and weaknesses of the study method
One strength of our study was the wide range of participants that were interviewed. Front-line clinicians, including community-based nurses and specialist consultants, were able to describe the daily challenges faced by those providing care for patients with chronic disease. Our sample also included professionals from a variety of backgrounds with current and past experience of telemonitoring projects. However, our study is necessarily limited by the experience of our participants and the nature of the interviewing methodology, i.e. the questions asked and the ideas that participants chose to express. Therefore, although the requirements and research questions appear to be comprehensive, we do not claim that they are exhaustive. In particular, we did not interview any patients, although further work has involved consultations on this topic with patient focus groups.
Our informants were based around the UK and our information is UK-specific, but this does not mean that the questions we have identified are only relevant to the UK. Most countries have fragmentation in their care systems (state- or privately-run)16–18 and face similar demographical changes. Also, economics and migration require telemedicine solutions that cross geographical boundaries. None of the items in Table 2 are UK-specific and each can be interpreted in consideration of local or national circumstances.
The informants who had direct involvement with telemonitoring were all based in primary care and so the architectures of the telemonitoring systems they described were quite similar. Other participants had indirect experience of trials based in secondary care or university departments. Those reported in the peer-reviewed literature are more often of this type.
Results in context – published work
Other researchers have conducted work seeking to inform future research in the general area of telehealth or health informatics/e-health and there is inevitable overlap between these and our findings. Many authors have identified the organisational and social challenges to successfully implementing such technologies.19–25 As telemonitoring does not match up with current organisational structures and has not been designed with sufficient clinical input, it is seen as a disruptive technology that forces users to change their established work practices and roles and imposes inflexible protocols, thus impeding its wider acceptance.19–25
Clinical usefulness is one of the most important requirements for users of telemonitoring. 23 Calls for improved usability, ease of use, fitness for purpose, etc. are relatively common in the e-health literature, 20,21 and it is felt that these issues can be addressed by increased user involvement in the design process.21,24,25 Our participants were consistently in favour of this approach and the gap between engineers and informaticians on the one side and clinicians on the other was blamed for many of the perceived problems with current systems. The wider literature on the design and implementation of information systems proposes the use of such paradigms as co-design, co-realisation, participatory design and computer supported co-operative work (CSCW) to bridge these gaps.25–27 We do not propose which method should be adopted, but agree that improved definition and communication of requirements is essential for telemonitoring systems to improve their effectiveness and efficiency. In the experience of our participants many systems were effectively bought ‘off-the-shelf’ with little attempt to adapt them to local needs. In depth consideration of the questions suggested here when planning to introduce telemonitoring would be a significant improvement on such practice.
Previous work on telehealth interventions has not specifically addressed the concept of early detection of deterioration. Our findings are that the requirements for this are related to the technical issues of clinical indicators and pattern detection. There was no consensus amongst our clinical informants regarding the natural history of physiological indicators preceding symptomatic deterioration. Clinical professionals could not describe what changes in the monitoring data they expected to see, only that changes from baseline should be identified and acted upon. It appears that very little research has been conducted to demonstrate whether there are suitable physiological markers for early detection. Wolfel 28 has listed several indicators that can be predictive of incipient heart failure deterioration, only one of which (weight) is currently used in commercial telemonitoring interventions. The specificity and selectivity of these in typical primary care patients is unknown. From the technical perspective we cannot predict at this point, for example, whether statistical pattern matching or machine-learning techniques will prove most effective at detecting deterioration; this is yet to be determined. Personalisation of indicators and analysis methods may well be the most effective means to improve telemonitoring outcomes. 21
The local primary care pilots or feasibility studies described by some informants were small-scale and lacked scientific rigour and effective evaluation There have been many published trials of different forms of telemonitoring for chronic disease management,6,10 but there are limitations in using these as an evidence base for the design and adoption of telehealth; not least that the technology changes faster than controlled studies can be conducted and published. Published trials are often of relatively short duration and lack high quality cost-effectiveness evidence.29,30 They also tend to conduct complex interventions, 31 but assess only simplistic health or resource use outcomes and lack qualitative evaluation. 20 There have been calls for more theory-based interventions 32 and for improved study designs and evaluation methods for telehealth trials.22,30,33 However, the majority of published data is from systems based in secondary care, whereas the majority of patients are managed in primary care and have complex and variable conditions.
Results in context – current situation
The need for improved communication and closer working between UK care organisations and patient-centred approaches has been accepted for some time 34–36 and the latest five-year plan for the NHS is especially apposite:
“We will make more use of information-based technologies to design new models of care as well as improving the performance of existing services. We will integrate information around the patient, deliver relevant information at the right time to clinicians and use technology to drive efficiency for both patients and clinicians.”
37
However this was published before the coalition government described its intention to reform the NHS, and the shape and effects of the Health and Social Care Bill 38 on the use of such information technologies are still to be determined.
The Department of Health is currently evaluating a large-scale trial of telecare and telehealth for chronic disease management13,39 which is due to report in 2011 and has also commissioned 16 Integrated Care Pilot projects 40 that will address some of the organisational and informatics questions we have identified. We eagerly await the publication of these results and hope that the evaluation will be more effective and informative than most.
Organisations currently contemplating introducing a telemonitoring service can use the questions we have defined here to ensure that their requirements are well considered, explicitly defined and communicated to system providers. Although apparently simplistic, the concept of such forward planning appears to be absent from some interventions. These questions are brief, but comprehensive, and could improve the effective use of currently available technology. We call for a move away from ‘What can we do with this technology?’ approaches towards ‘What technology can help us do this?’.
Conclusion
Telemonitoring has had some success in the management of patients with chronic diseases but previous implementations have not had an emphasis on early detection of deterioration. There are many organisational, social and political factors which impede the ability to effect optimal care for such patients, but there is also a need for technical and clinical research to inform the development of the next generation of systems.
We call for greater interaction between engineers, informaticians, clinicians, other relevant professionals and patients in the research and design of future healthcare information and communication technology (ICT) systems, including the adoption of more advanced user-design methods. 27 True interdisciplinarity will require much closer working between disparate specialists than has previously occurred, involving translocating people to other departments and learning the language of other fields or finding individuals with cross-disciplinary expertise.
“I (fairly uniquely) work with clinicians and engineers equally and we have dialogue every day…and we come to speak more of a sort of a common language about how to…do biomedical engineering…” [O4]
Despite the expanding availability of remote team-working technologies our own research team has found that collaboration is still easiest and most effective when sharing a physical location.
We have not set out to produce a sociological analysis of telemonitoring use in the UK or to compare the efficacy of different interventions. This piece of work was designed to collate information about current working practices and expert opinion regarding the requirements for early detection telemonitoring. These outcomes formed one of several inputs to a higher level analysis which has produced a roadmap for future research programme. 41
Footnotes
Acknowledgements
The Grand Challenge Team at Cardiff University was composed of: Dr Omnia Allam, Dr Charlotte Bolton, Dr Ed Conley, Professor Glyn Elwyn (PI), Professor W. Alex Gray, Mr Alex Hardisty, Dr Alex Hillman, Professor Tim Maughan, Professor David Owens, Dr Susan Peirce, Professor Alun Preece, Professor Omer Rana, and Dr Zaheer Yousef. We acknowledge the valuable contributions of each team member and the assistance they have given leading to the present paper.
This work was supported by the Engineering and Physical Sciences Research Council [grant number EP/F058640/1]