
Abstract
Home telemonitoring has been used as a solution to support the care of individuals living with chronic disease. While effectiveness of telemonitoring have been widely studied, more research is needed to understand the perceptions among patients and clinicians in incorporating telemonitoring into their daily routine and practices. This paper presents an investigation of patients’ and clinicians’ experiences in a care augmenting telemonitoring service, their perceived impact delivered through the service, and clinicians’ perceptions on how the service was introduced in their organizations. This work was embedded in a large multi-site trial of home telemonitoring using a mixed method approach for evaluation. Interviews with clinicians involved in the study were conducted at multiple time points during the trial. Questionnaires were administered to clinicians and patients at the end of the trial. Results showed that both patients and clinicians recognized the benefits of patient empowerment through telemonitoring, and patient-clinician interactions. Results identified the needs of a dedicated telemonitoring clinical care coordinator role, guidelines that translate telemonitoring services into clinical pathways and engagement of different healthcare providers, especially general practitioners, to support the integration of telemonitoring into chronic disease management programs and long-term organizational strategic plans.
Introduction
Chronic disease is a leading health concern worldwide with the population aging at an unprecedented rate. There is an increasing trend to enhance home health care services to meet the demand for the care of individuals living with chronic diseases. Telehealth has played a crucial role in responding to the needs of home health care. More precisely, home telemonitoring, a sub-category of telehealth and defined as an automated process for the transmission of data on a patient’s health status from home to the respective health care setting, 1 is increasingly implemented to capture patients’ clinical parameters easily in a continuous or intermittent pace to support patient care. Various studies have reported the effectiveness of telemonitoring in reducing mortality,2–4 hospitalizations and emergency department visits,4,5 as well as improving patient perceived quality of life, 6 evidence-based prescribing and overall management of disease.7,8
While the effectiveness of home telemonitoring on clinical outcomes and health care costs have been widely explored, the evaluation of home telemonitoring has been expanded to include user experience,9,10 perceived impact and organizational analysis.2,11 Telemonitoring does not just “work” or “not work” 12 as the success of telemonitoring depends on many factors, including organization of the telemonitoring program, technology complexity, patients’ compliance, and how clinicians and patients are engaged.11,13–15 Positive user experience of telemonitoring systems and experience of patient-clinician interaction and communication are essential to ensure the adoption of this new care modality.14,15 Clinicians’ acceptance is pivotal for the implementation of a telemonitoring program in their practice. Without effective adoption and implementation, telemonitoring will not be sustainable as a successful care model for chronic disease management.
To evaluate the benefit of home telemonitoring, researchers have indicated the need to understand patients’ perceptions of the impact services have on their choronic disesase knowledge and their ability to self-care of their chronic diseases.2,10,15,16 It is also important to explore patients’ experience in interacting with clinicians in the telemonitoring journey, as developing a shared understanding of self-management between patients and clinicians can help to facilitate telemonitoring.15,17 Researchers have called for trials and studies with improved evaluation designs that investigate the effect on patients’ self-care and their acceptance of telemonitoring, in particular adoption factors.10,15,18
Improving clinicians’ acceptance has been cited as one of the challenges for telehealth implementation and a key factor for sustainability of these models of care.19–21 Reviews of telehealth programs have explored the barriers to implementation and mapped them to the attributes identified in acceptance theories, such as the Diffusion of Innovations.22,23 By looking at the degree to which an innovation is perceived, these attributes assess whether the innovation is better than the idea it supersedes (advantage), consistent with the existing values and needs of potential adopters (compatibility), relatively difficult to understand and use (complexity), experimented on a limited basis (trialability), and the results of an innovation are visible to others (observability). Recent organizational analysis of home telehealth implementation has indicated the need of a renegotiation of clinicians’ roles and responsibilities.17,23 Although clinicians found monitoring patient’s conditions useful, they also voiced concerns about workload, liability, incentives, and technical support.24,25
The investigation of the patients’ and clinicians’ experience and their perceived challenges for introducing telemonitoring is an active field of research.16,26 Appropriate approaches are required to better understand their experience from technological, organizational and individual perspectives.22,27 In addition to the use of questionnaire measures, longitudinal qualitative research has been increasingly used to provide insights about telemonitoring adoption barriers and facilitators.15,17,23 Lessons learned from telemonitoring trials can provide valuable insights for wider scale integration of telemonitoring as a new model of care. 11
In this paper, we present the results of our investigation of patients’ and clinicians’ experiences and perceptions on the effect of in-home telemonitoring service. This work was embedded in a large-scale home telemonitoring for chronic conditions trial that we carried out at multiple states of Australia.5,28 The trial investigated the effectiveness of home telemonitoring has demonstrated positive health service untilization and economic outcomes. 28 In addition, the trial addressed an important gap in the overall evalution of home telmonitoring by incorporating a research component of investigating patients and clinicians’ perceptions on the impact of telemonitoring on patient empowerment, their interaction experience, and factors clinicians perceived to influence the introduction and sustainability of telemonitoring service. Our work presented in this paper describes this particular component which contributes to the research in understanding the users’ acceptance of home telemonitoring, their perceived impact, and the implementation challenges in different healthcare organizations. In this paper, we first provide an overview of the intervention trial and research settings. We then describe the methods of the study presented in this paper. We present the results related to perceptions of patients and clinicians and discuss factors influencing the implementation and adoption of telemonitoring.
Settings
Chronic disease management in Australia usually involve multiple service providers, including general practitioners (GPs), allied health clinicians, disease specific specialists and other healthcare professionals. An integral part of the services is the coordinated care program which covers a care plan dedicated to individual patients. Based on their disease severities, patients are assigned to different levels of care programs, ranging from hospital-based to community-based and from federal funded to state funded programs. A central worker (normally a nurse) coordinates with service providers on the delivery of an individualized care plan and provides ongoing follow-up to patients.
A multi-site trial was conducted across five Australian states to investigate the effects of introducing at home telemonitoring of vital signs for the management of a heterogeneous group of chronically ill patients.5,28 A detailed description of the trial methods have been reported previously. 28 A home-based telemonitoring service was introduced to assist in the management of these patients over a period of 12 months. To compare with the existing homecare model, a Before-After Control-Intervention (BACI) design was developed with a matched control group who received normal care. Inclusion criterial for intervention patients included: aged 50 years old and over, who had unplanned acute admission for one or more chronic conditions (chronic obstructive pulmonary disease, coronary artery disease, hypertensive diseases, congestive heart failure, diabetes), and were under the care of community nurses and/or GP.
A commercially available home-telemonitoring unit (TeleMedCare) 29 was used by intervention patients for the scheduled monitoring of measures required by their care plans such as non-invasive blood pressure, pulse oximetry, single channel ECG, Spirometry, body temperature, body weight, and blood glucose levels. The system also had a web-based clinical portal where clinicians could log in and monitor their patients’ uploaded data. The device was also able to deliver questionnaires to patients at regular intervals as required.
The trial was carried out in collaboration with local healthcare organizations at six sites. Of these, two sites were hospital based with access to specialist nurses and medical doctors. The remaining were community based sites with existing normal care being delivered primarily by GPs and/or community nurses and coordinated by Medicare Locals (now called Primary Health Networks) which were the local coordination body for GP service. Despite the complexity of conducting a clinical trial across different organizational contexts and the decommission of one site, a total of 114 intervention patients and 173 control patients were recruited.5,28
Through our engagement with the trial site local organizations, a new role of Clinical Care Coordinator (CCC) was introduced as part of the intervention at each site. CCCs were funded by their local organizations. Their role was to monitor intervention patients’ vital signs and liaise with patients’ GPs, specialists, hospital-based nurses and community nurses. At sites where chronic care programs already existed, an resident nurse coordinator or specialist nurse was used as the frontline CCC to manage the daily monitoring and phone calls with patients. In sites where nurse coordinator or nurse specialists were not as readily available, a registered nurse was employed to lead the telemonitoring service. Site CCCs generally reviewed patient data daily (only on weekdays) via the web-based clinical portal.
A project officer (PO) was also allocated to each site to manage operational activities of the trial. The POs predominantly had a nursing background and facilitated the installation and configuration of the telemonitoring units according to clinical best practices. At each site, one or two managers who led their existing chronic disease programs or supervised the care team took charge of rolling out the telemonitoring, staff recruitment and progress review.
GPs provided consents for the patients to be telemonitored at home. The trial protocol was presented to GPs by the trial researchers and trial support to GPs was provided by CCCs and POs. All GPs were offered access to patient monitoring data either through the clinical portal or paper reports.
The trial examined different effects of telemonitoring services. 28 Besides the evaluation focusing on clinical outcome and health resource utilization, 5 in order to better understand the impact and provide broader evidence, the design of the evaluation also incorporated a component to investigate how telemonitoring was introduced in each site and how the effect was perceived by clinicians and intervention patients who have used the telemonitoring. This paper presents our work related to this component.
Ethics approvals for the trial including the study reported in this paper were granted by the CSIRO CAFHS Human Research Ethics Committee (#13/04) and health authorities at each of the test sites.
Methods
A multi-method approach was adopted for this research component. The study of clinicians’ perceptions was undertaken by using semi-structured interviews at multiple time points during the trial and a questionnaire answered by all CCCs and POs at the end of the trial. Patients’ perceptions and telemontoring experiences were evaluated by using questionnaire administered to intervention patients at the end of the trial. Three researchers were involved in the design, data collection and data analysis process.
Questionnaires to patients and clinicians
Patients’ and clinicians’ experiences and perceptions of telemonitoring were assessed in three dimensions: (i) perceived benefits to patients, (ii) interaction and communication experience, and (iii) acceptance. We developed two sets of satisfaction questionnaires, a questionnaire for patients and a questionnaire for CCCs and POs involved in the trial, to cover the three dimensions:
The questions of the first dimension were adapted from a validated scale 16 used in telemonitoring study to measure the perceived empowerment benefits of telemonitoring on patients. It is worth mentioning that we had similar questions of this dimension for the clinician questionnaire and patient questionnaire for consistency.
The second dimension, the interaction and communication experience measures, included questions related to experience with technology (complexity, usability) based on Diffusion of Innovations acceptance theory 22 and experience with clinician-patient interaction and communication based on similar evaluation in other telehealth studies (e.g. Asua et al., 27 Chau and Hu 30 ). The clinician questionnaire also included questions about nurse-doctor communication.
The third dimension included the questions of compatibility of the technology with patients’ needs and clinicians’ existing practices, observability and satisfaction of using the technology, drawing on the Diffusion of Innovations acceptance theories 22 and telehealth related work (e.g. Asua et al. 27 ).
The clinician questionnaire consisted of 20 questions in total using a five-point Likert scale (strongly disagree to strongly agree). The clinician questionnaire also incorporated three open-ended questions asking about their perceived success factors and barriers for implementation.
The patient questionnaire comprised 32 five-points scale questions in total. Twelve of these related to technology complexity and compatibility, and were grouped into a subset titled “technology satisfaction” and the other 20 questions addressed perceived impact, experience and satisfaction and were grouped into a subset called “service satisfaction.”
The patient satisfaction questionnaire was administered through the telemonitoring device and scheduled by the PO. The “service satisfaction” subset was added to the list of exit questionnaires at a later stage of the trial due to arrangement issue and some patients did not receive this subset before the device was returned. For these patients, the paper-based satisfaction questionnaire was subsequently posted to them by POs. Among the 96 intervention patients who finished the trial, we collected responses from 56 patients.
CCCs and POs from the five active trial sites received the questionnaire by email and altogether nine returned the completed questionnaire by post. One of the three researchers coordinated the questionnaire data collection process at each site.
Clinician interviews
Semi-structured interviews were conducted at multiple time points, during the first 3 months and during the implementation (from 3 months onwards), to understand how the telemonitoring service was introduced at each site, their processes and issues. Researchers were introduced to site CCCs, POs and managers at a discussion workshop held face-to-face when the trial commenced. Interviews during the first 3 months and 3–6 months implementation phase were conducted via telephone. Field visits were carried out to all trial sites during the 6–12 months implementation phase and face-to-face interviews were conducted in combination with the visits.
Interview questions focused on (1) How the home telemonitoring impacted on their care delivery; (2) What impact it had on their patients; (3) How the care coordination practices evolved as a result of telemonitoring; and (4) What was learnt from the implementation approaches. We also explored what the clinicians believed an ideal home telemonitoring service would look like, based on their experiences. Interviews lasted 30–60 min and were audio recorded.
CCCs and POs at the six sites were invited to participate in the interviews and all accepted the invitation. One or two managers at each site were interviewed during site visits. A small number of GPs who had patients using telemonitoring in the trial were interviewed during site visits to understand their expectations and perceived potential issues. Most GPs were not intricately involved in trial monitoring.
Details of each time points, participants and data collection are summarized in Table 1.
Interview data collection time points and participants.
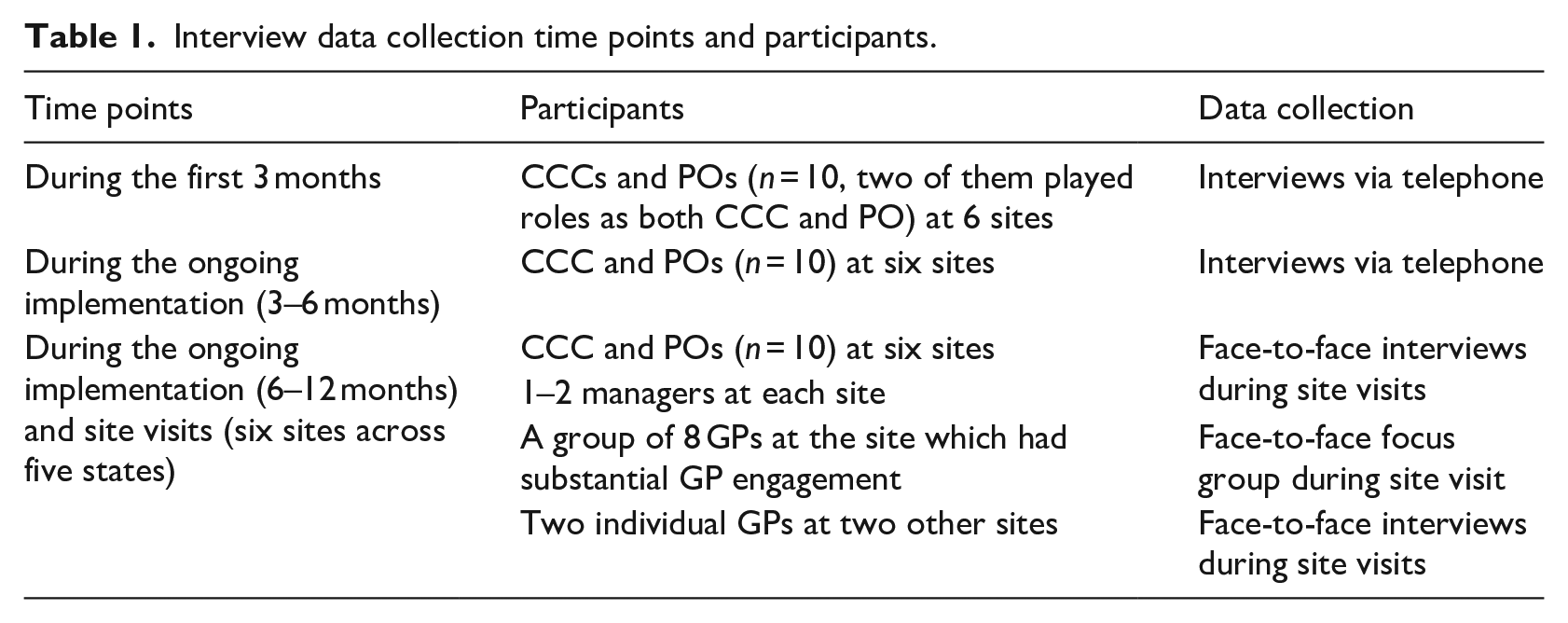
While interviews with intervention patients were desirable and we did conduct a small number of home visits during the trial through the help of local sites, due to the challenge of local coordination required, and the constraint of trial timeframe, we were unable to include interviews with patients before the completion of the trial.
Data analysis
Questionnaire responses were analyzed by one of the researchers using Excel data analysis software. Interviews were professionally transcribed. Transcriptions were analyzed by two of the three researchers using thematic coding 31 in NVivo software. Initial data codings and categories were reviewed by and discussed between the three researchers involved in the interview process. Key themes and sub-themes were identified and closely examined based on the frequency of mentions and relationship to the questions asked. Iterative analysis identified major themes related to perceived impact, interactions, specific organizational and operational challenges and how clinicians dealt with these challenges. Results and themes emerged across different sites and at different stages were summarized and discussed at each time point as part of the data analysis process.
Results
We present questionnaire and interview results related to perceived patients’ empowerment experience, communications, technology satisfaction and usability, compatibility, telemonitoring experience, and clinicians’ views on implementation challenges and adoption factors.
Patients’ perceived benefits, experiences, and acceptance
The results in this section are based on a total of 56 intervention patients’ responses to the satisfaction questionnaire (49 of them responded to both Service Satisfaction and Technology Satisfaction subsets, seven of them did not return the Service Satisfaction component due to the arrangement issue described in section 3.1.). The 56 patients were located in five states. Their average age was 71.75 years old and 34% were female.
Empowerment experience
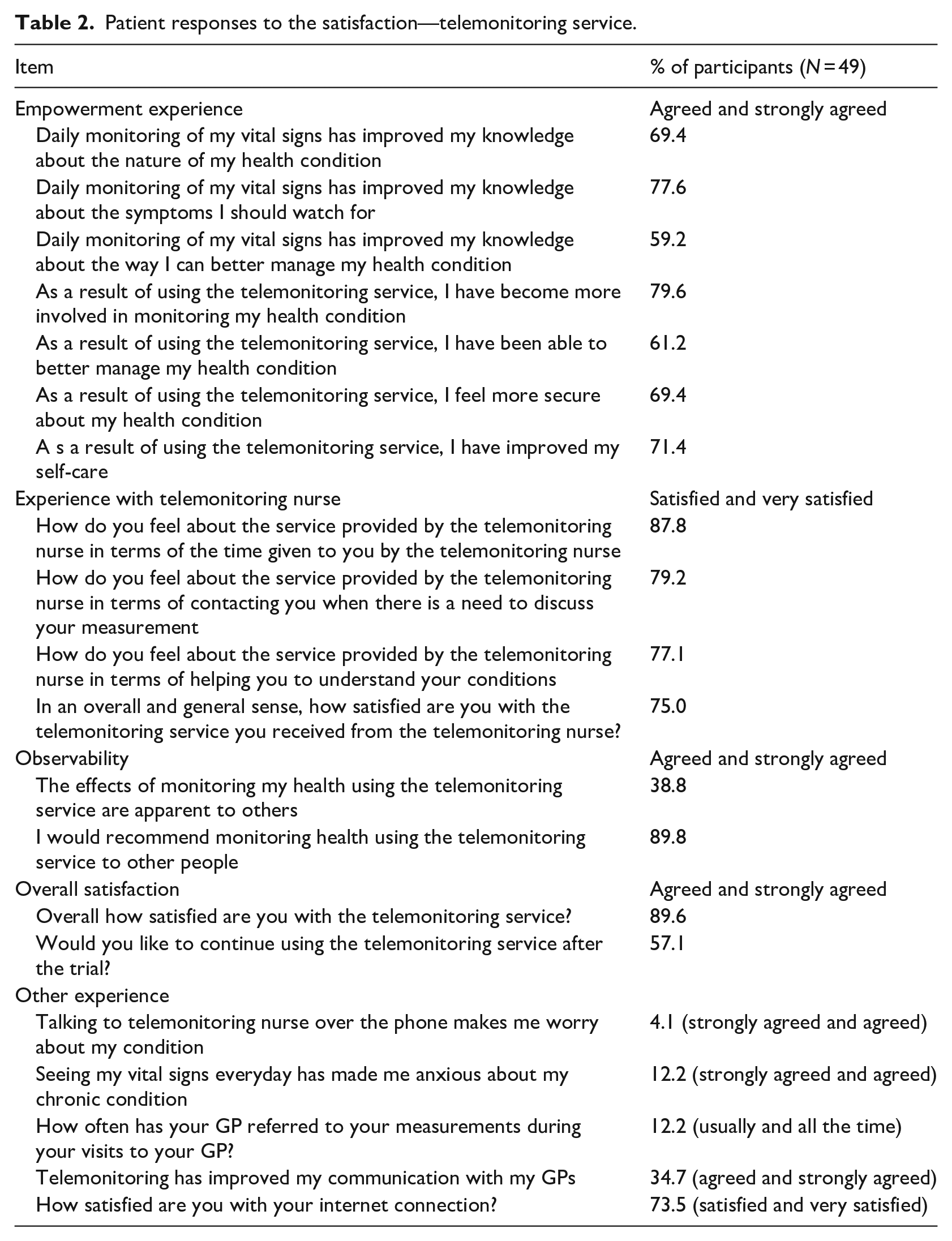
As shown in Table 2, 69.4% of patients found that telemonitoring had improved their knowledge about their conditions and 77.6% of them found it improved their knowledge about symptoms to watch for. 79.6% of them felt were more involved in monitoring of their health conditions. A sense of security and assurance was reported by 69.4% of patients. 61.2% of them also felt that they were able to better manage their health condition and 71.4% reported improvement in their self-care as a result of telemonitoring.
Patient responses to the satisfaction—telemonitoring service.
Clinician-patient communication
Patients’ overall experience of interacting with telemonitoring nurses was positive (Table 2). Majority of them reported that they were satisfied the communication with telemonitoring nurses in terms of the time they received from the nurses (87.8%), the discussions about their measurements (79.2%) and assistance in understanding their conditions (77.1%). However only 12.2% of patients reported that their GPs reviewed the telemonitoring results during their visits to GP clinics and only 34.7% patients agreed that telemonitoring improved their communications with their GPs.
Technology satisfaction, usability, and compatibility
All 56 patients were overall satisfied with using the telemonitoring device (TMD) (Table 3). Majority of participants found the TMD easy to use (87.5%) and felt confident in using it (85.7%) despite 32.1% of them reported that there were occasions of frustration. Responses indicate that only a few patients found the device cumbersome, unnecessarily complex, or thought that they would need a technical person’s support in using the device.
Patient responses to Satisfaction—telemonitoring technology.
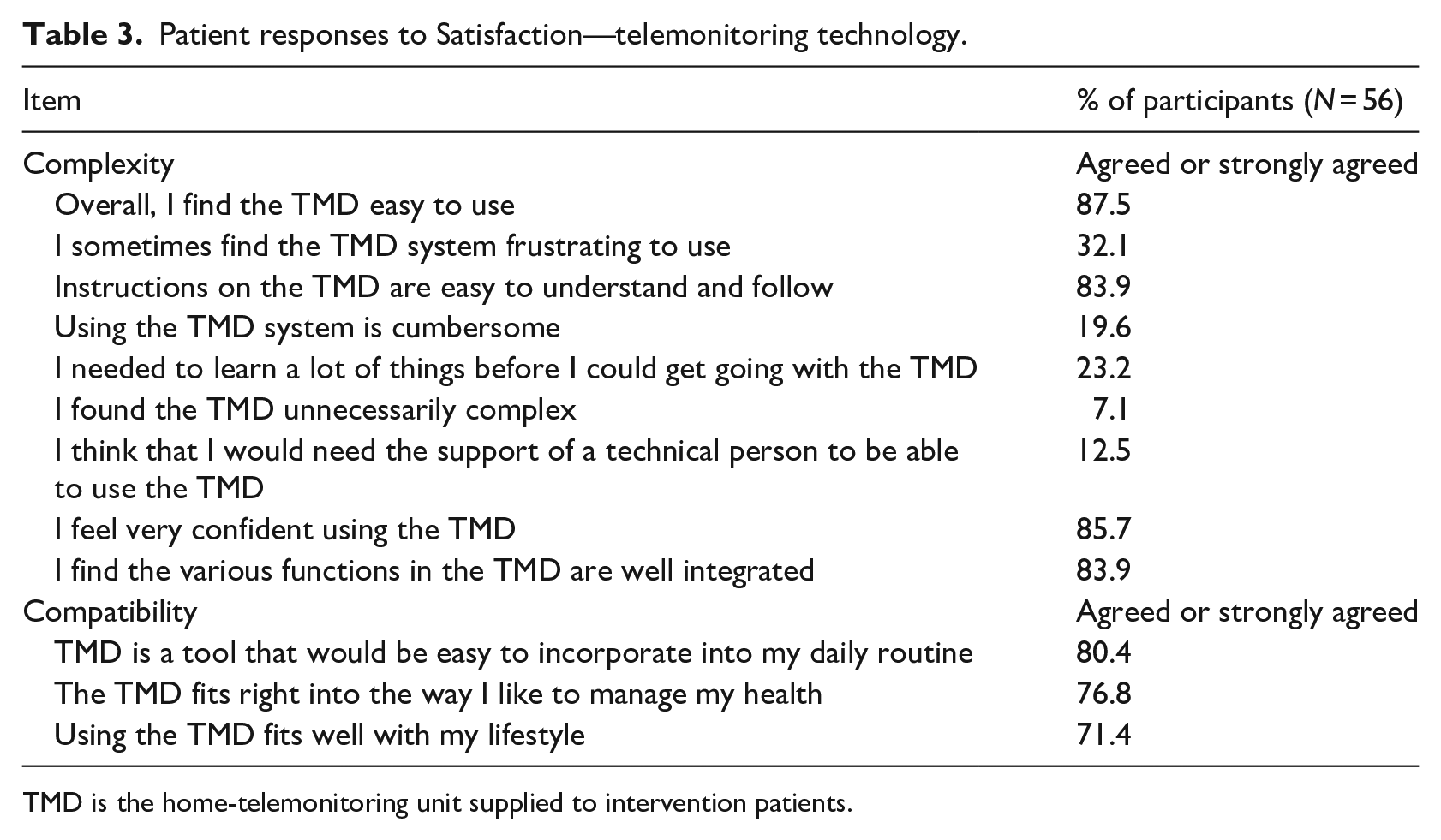
TMD is the home-telemonitoring unit supplied to intervention patients.
In terms of compatibility, majority of participants found that using the monitoring device could be incorporated in their daily routine (80.4%), fitted in with their daily life (71.4%), and the way they would like to manage their health (76.8%) (Table 3).
Telemonitoring service experience
Majority of patients (89.6%) reported that they were satisfied with the telemonitoring service (Table 2). Some of them (57.1%) answered that they wanted to continue using the service after the trial and through our interviews with clinicians we learned that some patients concerned that they would need to pay for the service after the trial. Few of them (12.2%) felt that seeing their vital signs every day and talking to telemonitoring nurses made them anxious or worried. 89.8% responded that they would recommend telemonitoring service to other people.
Clinicians’ perceived benefits on patient care, experience, and challenges
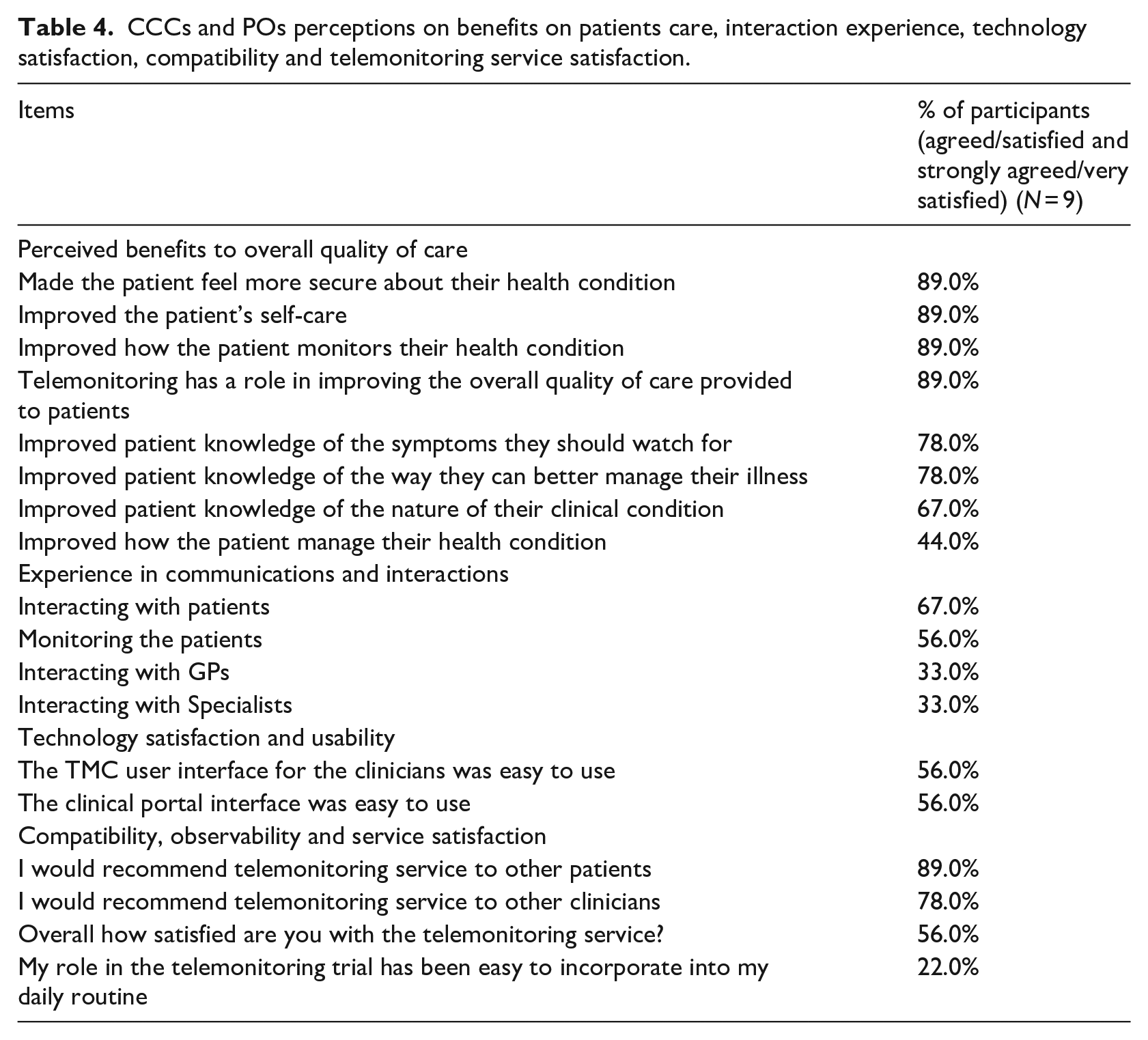
The results in this section are based on CCCs and POs questionnaire responses and the interviews analysis. Questionnaire responses are summarized in Table 4.
CCCs and POs perceptions on benefits on patients care, interaction experience, technology satisfaction, compatibility and telemonitoring service satisfaction.
Perceived benefits on patient care
Positive responses were received from CCCs and POs in the questionnaire in terms of improving patient knowledge about the nature of their chronic conditions and symptoms. Eighty-nine percent of them responded that telemonitoring had improved the patients’ self-care and made patients’ feel more secure about their health conditions. A similar percentage (89%) believed that telemonitoring would have a role in improving the overall quality of care provided to patients.
In the interviews, all CCCs, POs, and GPs participants believed that home telemonitoring could have potential positive impact on the care of chronic disease patients. Some CCCs and POs found that their patients were able to understand the meaning of their measurements and to discuss these with their clinicians. CCCs and POs pointed out that telemonitoring helped to identify adverse trends in their patients’ measurements and assisted them in providing intervention in a timely manner for patients. One of the POs described the benefits this way:
“By talking to patients, for example, during the visits to home for software updates, I have learned that people are being more and more empowered by telemonitoring information and being able to go to GPs to talk about measurements, learn more about their health. They can see things going up and down every day. One of the biggest opportunities for reducing hospitalization is by telehealth nurses picking up clinical deterioration and sometimes patients are picking up these.”
The GPs we interviewed also pointed out that telemonitoring could be particularly useful in rural settings. One of the GPs who also worked in a rural hospital believed that it could help early discharge of patients from hospitals.
Some CCCs and POs put in effort to educate their patients about their diseases and self-care during regular contact with the patients. Although many positive stories about patients’ attitudes and improved knowledge were recorded, they felt that the impact on patient self-management of their health conditions needed to be explored in a longer period of time as the trial had a limited timeframe and recruitment challenge.
The following are examples of perceived benefits that CCCs and POs listed in the comment section of the questionnaire:
Offering support to each individual patient to meet their needs, not just when their readings are outside their parameters
Enabling patients make informed choices since they can see their measurement readings
Empowering self-management through awareness and education
Giving patients confidence in taking care of their own health and peace of mind that there is someone to assist them if necessary
Reinforcing their interest in their own health through the visual effect of seeing data, especially male patients
Identifying deterioration or new issues
Reducing or avoiding hospital admissions since patient can see their readings and seek care early.
Communications
Majority of the CCCs and POs reported positively about interaction with patients (67%) in the questionnaire. However, the communications between CCCs/POs and GPs/specialists were not very efficient at some sites, with only 33% of CCCs and POs rating this interaction as satisfactory.
We explored the inter-professional communications in the interviews. CCCs and POs felt that the inefficiency was partly due to the way that patients were recruited in the context of research trial and most of GPs were not intricately involved in trial monitoring. GP consent for their patients’ participation was required in the trial protocol and it could take a long time for POs to get it. Quite often communication with GPs was via patients when patients visited their GPs. There were also issues of educating GPs about the process of telemonitoring and the access to monitoring data. A manager at one site made the following comment:
“We need patient history and summary to have a little bit background about patients. . . GPs are the major healthcare provider in our program at the moment. There was not established connection to provide feedback to clinicians which are patients’ usual healthcare providers and involve clinicians.”
However, CCCs noticed that the communications improved as the trial progressed and GPs and their clinics became aware that they could contact CCCs to discuss patient problems.
In terms of improving their collaboration with CCCs, GP participants at the focus group expressed their preference for receiving a summary (e.g. a pdf file) about patient measures from CCCs on a regular basis. They pointed out that ideally the construction of the report should include interpretation of monitored data.
Technology satisfaction and usability
In the questionnaire, we asked CCCs and POs about the usability of the TMD user interface in the clinical portal for them to schedule patient measures and monitor the data, 56% of them answered that the interface was easy to use.
In the interviews, TMD installation issues at the beginning stage were mentioned by POs. POs were supported by the TMD company technical staff and most of the technical problems were usually resolved quickly. However, they felt that the communication would be much more efficient if the support was provided by a local IT support staff. Drawing on their experience of using telemonitoring, CCCs and POs made several suggestions for the clinical portal, such as creating a field in the patient diary, an analysis tools to help identify changes in patient status.
Telemonitoring satisfaction and compatibility
Majority of the CCCs and POs (78%) responded in the questionnaire that they would recommend the telemonitoring service to other patients and clinicians. However, there was a mixed feeling in terms of the implementation process. The questionnaire results showed that 56% CCCs and POs were satisfied with telemonitoring services in the trial context. Results also indicated that CCCs and POs observed problems in terms of incorporating telemonitoring work into their daily routine, and only 22% of them felt the integration was easy. Interview results provided insights on the challenges they experienced, as presented in the next section.
Implementation challenges and adoption factors
In-depth insights related to implementation challenges during the journey of integrating the telemonitoring services into their existing work practices were captured. These factors included: adapting to local organizational context, the need for a dedicated telemonitoring nurse role, clinicians’ liability concerns, the need to engage with GPs, and the need to integrate with clinical pathway and practices.
Adapting to local organizational context
This trial involved different sites with different local settings where the delivery of telemonitoring was based on. These differences of local context included organizational structure, existing chronic disease programs and experiences in telemonitoring and other telehealth work, and the collaborations between different healthcare professionals.
The sites organization structures ranged from hospital-based, Medicare Local, community-based to non-for-profit private aged-care, and homecare organization. Most of the sites had existing programs for chronic disease management. One of the sites had worked on a home telemonitoring program for 2 years before this trial. Three other sites had experience in other telehealth applications. Two sites’ CCCs were physically based at hospitals and worked closely with multidisciplinary teams consisting of specialists and other nurses. Some of the local health organizations undertook innitiatives of supporting community care after patient hospital discharge and the design of telemonitoring service were explored within this context.
According to most of the interviewed participants, it was an opportunity (albeit with accompanying challenges) for them to fit telemonitoring into their existing models and practices. At the sites where telemonitoring was introduced and integrated in existing chronic disease management programs, their conclusion was that the trial only added a layer of monitoring to the existing chronic diseases services that continued as usual. It was more challenging for trial sites which did not previously directly provide chronic disease management programs as they had to develop it as a new model of service which required the design of appropriate workflows and accountability.
A dedicated role of telemonitoring care coordinator
We found that although the configuration of the role and practice of a CCC depended on the existing resources and capabilities at each site, a dedicated role would be required to better manage the monitoring of a larger number of patients.
Some sites assigned the CCCs role to existing nurse coordinators or nurse specialists were already in place in order to incorporate the new roles to their existing work. The rationale was that in this way the sustainability of this capability could be maintained even after the conclusion of the trial. One PO pointed out that:
“We prefer to use people who are already working in chronic disease management type roles so that the knowledge and use of this type of healthcare, I suppose, is sustainable beyond this trial and a specific funded position.”
There was a concern about the workload for CCCs as pointed out by our interview participants. They had to accommodate telemonitoring into their existing work schedules. CCCs worked hard to meet the requirements of the telemonitoring in their daily work, making phone calls and following up. At some sites POs helped the site CCC by acting as a part-time CCC and taking over some of the telemonitoring tasks.
Despite the workload concern, CCCs overall attitude were positive. For most of the CCCs, the management of chronic care patients was their normal practices. The added burden of reviewing patient data was in line with their key responsibilities and duties. They believed that high quality telemonitoring in addition to existing chronic care service can be achieved with a full-time telemonitoring nurse with support from a multidisciplinary team.
Developing guidelines for telemonitoring
Majority of the participants pointed out that telemonitoring was not just simply making phone calls to patients and GPs. It required coordinated actions and proper documentations of their activities. They highlighted the issue of duty-of-care and clinical responsibility related to telemonitoring service which was a particular form of digital health services, and had its challenge in the context of trial investigation. There was a need to define and describe the responsibility and scope for the telemonitoring practice. At some sites, patients were recruited from existing chronic disease programs and adding telemonitoring on these programs created additional activities to the existing workflow for nurse coordinators, such as recording their contacts with patients, communicating with GPs and follow-ups. For sites where there was no existing coordinated care program, it was even more challenging as nurses lacked clinical support from other clinicians and the engagement with GPs was more difficult.
A protocol for the CCCs’ telemonitoring task was initiated by the trial researchers at the early stage of the trial. Each site further developed their guidelines for integrating telemonitoring into chronic care services. Some of the participants we spoke to stated that the experience from this trial and other telehealth projects provided a rich foundation for long-term planning and would guide development of future telehealth services.
Getting GPs motivated and involved
One of the challenges the CCCs and POs observed at the beginning of the trial was getting GPs motivated and engaged. They expressed concerns that GPs’ motivation for participation in research trials is usually not high. GPs were offered access to patient monitoring data through the web portal or paper-based report but only few of them opted for these options. CCCs and POs also felt that a factor inhibiting GP participation in a telemonitoring service could be the funding model. Australian Medicare only funds services delivered by clinicians face-to-face with patients. Although funding for some forms of telehealth services involving teleconferencing have been introduced in recent years, there was a question as to whether GPs could get healthcare funding for their involvement in home telemonitoring.
CCCs and POs worked actively to engage with GPs. They regularly sent reports regarding patients’ monitoring results to their GPs. They also advertised the trial information in their regular newsletters sent to GPs.
The GPs we interviewed, especially the focus group participants, were positive about the potential value of telemonitoring service. CCCs and POs also observed improved GP involvement after a few months of the trial when some GPs began to recognize the benefits for their patients. One PO reported a story that their Chronic Care Unit sent trial updates in the newsletters and a GP practice nurse contacted the Unit for the referral of candidate patients. A similar story was reported by another site that a GP contacted them to help the recruitment of patients to the trial. One PO mentioned two cases that GPs used the patients’ monitoring data in their practices:
“When visiting a patient today, he told me his GP has his telemonitoring measurements up on the screen when he walks into the consulting room, and uses them during his consultation.”
“When visiting a patient earlier this week, they informed me that their GP looks at her measurements every day and commented that they find it very useful.”
Moving forward and integration
We found in the interviews that there were ongoing processes to adjust and integrate home telemonitoring into existing services. Managers of chronic care programs at some of the trial sites had strategic thinking about how to apply the learnings from the trial into future redesign of services. One of the managers commented that running the telemonitoring trial could be considered as a journey of creating a new service with an innovative approach. One way to move forward as suggested by some managers was identifying patients suitable for telemonitoring service at hospital discharge and incorporating telemonitoring service into their clinical pathways or existing chronic care coordination programs. Participants also suggested ways of better alignment with the process of re-evaluating the integration of primary and secondary care at their Local Health Districts. They felt that the design of the telemonitoring service could be explored within this context. For example, in addition to the involvement of specialists nurses at hospitals, nurse educators who work closely with primary care services can be trained and employed in telemonitoring services. They pointed out that these approaches could potentially assist Medicare Locals and community services to play a role in the future implementation of telemonitoring services.
Discussion
The work presented focused on the experience of intervention patients and clinicians in using home telemonitoring for management of chronic conditions. The contributions can be summarized as follows. Firstly, while clinical outcome and cost benefits of telemonitoring have been extensively studied in prior work,7,8,25 very few clinical trials have examined intervention patients and clinicians’ perceptions and adoption factors.10,15,18 In addition to the component of clinical outcome and cost benefit evaluation in the large trial we carried out, we have incorporated an important investigation of both intervention patients and clinicians’ acceptance, their interactions and factors affecting their telemonitoring experiences. Secondly, there is a need to better understand clinicians’ roles and responsibilities and their experience from individual and organizational perspectives.17,22,23,27 Our work synthesized questionnaire and qualitative inquiry of clinicians’ experience and explored how telemonitoring can be better integrated into existing organization programs and primary health care service. Our findings related to factors affecting patients and healthcare professionals’ experiences and challenges for implementation are discussed below.
Factors affecting patients’ telemonitoring experience
Our results showed that patients had a positive attitude toward home telemonitoring. Several factors could affect their overall perception, including patients’ empowerment experience, clinicians’ support, technology complexity, and compatibility.
Empowerment experience: This represents one of the key factors for fostering self-management behaviors and the management of chronic diseases for patients living in the community.10,16 Improved knowledge about their conditions and the ability of managing their conditions were reported by the patients in our study. The clinicians’ perceptions on patient empowerment were consistent with findings from patients’ responses. They believed that telemonitoring has a role in improving the overall quality of care provided to patients.
Clinicians’ support: Besides improved knowledge, peace of mind and in-person communication with telemonitoring, care coordinators can also contribute to patients’ acceptance. Patients’ increased sense of security from being monitored and sense of reassurance with improved access to telemonitoring care coordinators have been reported as the perceived benefits of telemonitoring. 2 Our study patients reported a positive experience in terms of the support and contacts they received from CCCs and POs. They appreciated the connection with CCCs and POs and did not feel telemonitoring made them worry or anxious. This positive interaction perception was also evidenced in the CCCs and POs responses.
Technology satisfaction: We also measured technology satisfaction drawing on complexity and compatibility measures. 22 Device usability and suitability play important roles in patients’ acceptance and compliance as the target population for telemonitoring programs typically consists of older patients with chronic diseases. Monitoring technologies must be specifically tailored to the cognitive and physical capabilities of older patients and their home living environment.
Factors affecting healthcare professional’s experience and telemonitoring implementation
Although the clinicians in our study believed that telemonitoring had a positive effect on the patients, they also experienced challenges which impacted on their overall satisfaction. Understanding the implementation processes has been increasingly incorporated into telehealth studies, emphasizing the growing appreciation that organizational and sustainability factors are key to implementation.15,20 Issues that clinicians and organizations faced during the implementation journey have been identified through our interviews and field visits. In addition, factors to help overcome the challenges have been highlighted in our study.
Workload: Telemonitoring technology alone cannot achieve the desired results. Effort must be made by the organizations and staff to shape the telemonitoring service on the top of their existing work. An increase workload for telemonitoring care coordinator (e.g. monitoring and telephone calls, follow-ups) represents a challenge of trying to design an efficient home telemonitoring service that can attain a balance between resources and ensuring patient security. Supporting clinicians to manage the changes to workload and patient cases could improve clinicians’ acceptance of home telehealth.20,32 Future work can also incorporate advances in computing, such as intelligent alert management systems, to enhance the visualization and interpretation of vital sign data to assist with decision making.15,33
Guideline: Similarly, establishing guidelines supporting telemonitoring care coordinators to manage changes in work routines is also important.15,34 Liability related to patient safety can be a concern among clinicians involved, as the measurement data can be indicative of patient deterioration and the need for timely intervention. 35 Clinical guidelines outlining responsibilities for responding to abnormal data and documentation of communications with patients and other clinicians will provide confidence for them to cope with the changes to care delivery practices which are mediated by technology and to some extent alter the model of service delivery.34,36
Collaboration: The need for collaboration and engagement of various clinicians for telemonitoring has also been observed in our results. CCCs and POs felt that the interactions with GPs and specialists involved in the care delivery for telemonitoring were not easy, especially at the beginning of the trial. Although trial protocol was presented to GPs and support from CCCs and POs was available, engaging with GPs and their practices was challenging. Lack of financial reimbursements for their time in telemonitoring services could also impact on their motivation and involvement. 21 However, we found that once GPs noticed improvements in patient outcomes, their attitudes toward telemonitoring significantly changed. This indicates that a shared vision of telemonitoring patient management and potential impact needs to be built among all stakeholders to sustain their engagement. In addition, while GPs could access the monitoring data, sending them regular reports and short summaries of patients’ measurements can help to improve the efficiency of their data reviewing and patient consultation process. To facilitate interprofessional collaboration, telemonitoring services need to recognize, and support the reorganization of work between the telemonitoring staffs, hospital, primary care, and home health service providers. 15
Integration: Telemonitoring needs to be tailored to allow for integration within existing programs for different patient needs, resources, and organizational contexts. Our study revealed that effort must be made to fit the telemonitoring service into existing chronic care program structures. Sites with available resources and organizational structure may be able to more readily incorporate telemonitoring into their existing service. An efficient model was developed in some of our study sites by using existing nurse coordinators as the frontline nurse for telemonitoring. A site serving patients with a lower disease severity may not require the same intense monitoring schedule as the sites with higher disease severity. Employing a trained nurse educator working closely with GPs might be considered efficient from a resource optimization perspective. The adaptable nature of the implementation may also represent opportunities for current and future organizational strategic plans.
The findings of our investigation have some limitations. The work was embedded in a clinical trial which had the scope of BACI design and with a relatively short timeline. The perceived impact and acceptance can be better understood after a longer period of implementation and when the service is more closely integrated into clinical practices. Due to the trial completion constraint, we were not able to conduct interviews with patients to explore further their experience and adoption factors as explained in Method section. Such observations, as well as the expectations of control patients who did not have the opportunity to use the telemonitoring, when possible will be part of future analytic activities.
Conclusion
This paper presents the investigation of patients and clinicians perceived impact of telemonitoring on chronic care patients and their experience in the implementation of a telemonitoring service intervention. Increased patient empowerment and satisfaction with the patient-nurse communication were perceived by both intervention patients and clinicians. Qualitative analysis of clinicians’ perceptions on the implementation process provided insights of how the new model could be introduced in different organizational settings. An adaptive approach is required for telemonitoring programs to become fully incorporated into routine home health service delivery and part of long-term strategic planning. It is essential to address telemonitoring clinical care coordinator’s challenges regarding increased workload, communication and guideline requirements. The collaboration of different clinicians from hospital, primary care and community services is required to realize the potential of telemonitoring becoming a core part of care pathways for management of various chronic conditions.
Footnotes
Declaration of conflicting interests
The author declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This project was funded by the Australian Commonwealth Government National Broadband Network Telehealth Pilot Program with additional financial support from the CSIRO and in-kind contributions from health service providers at the trial sites.