
Abstract
The implementation of generic models for organizing information in complex institutions like those in healthcare creates a gap between standardization and the need for locally relevant knowledge. The present study addresses how this gap can be bridged by focusing on the practical work of healthcare staff in transforming information in EPRs into knowledge that is useful for everyday work. Video recording of shift handovers on a rehabilitation ward serves as the empirical case. The results show how extensive selections and reorganizations of information in EPRs are carried out in order to transform information into professionally relevant accounts. We argue that knowledge about the institutional obligations and professional ways of construing information are fundamental for these transitions. The findings point to the need to consider the role of professional knowledge inherent in unpacking information in efforts to develop information systems intended to bridge between institutional and professional boundaries in healthcare.
Keywords
Introduction
Electronic patient records (EPRs) have a central function in accumulating and coordinating the extensive flow of the various kinds of information that is needed for providing day-to-day patient care. 1 In comparison to paper-based records, the EPR functions as a hub for coordinating a wider range of professionals, specialities and stakeholders and in assembling information from different sources within a single system. 2,3 The objective is both to facilitate access to information and to achieve more effective ways of entering, organizing and sharing information. 2 Internationally, much effort is currently being channelled into the development of information systems that facilitate the flow of information between different healthcare providers, social welfare institutions and other agencies. 4 This vision of seamless information sharing places extensive demands on ‘writers’ and ‘readers’ within different institutional and professional domains to understand each other. 5 Entries formulated by one actor must be intelligible not only to colleagues but also to other professional groups with different knowledge domains, obligations, terminologies and information needs. Against this background, the standardization of information structures and terminologies has been put forward as the general solution for sharing information both within and between professions and institutions. 2 This presumes, however, that structured information could be treated as a self-sustaining entity that can convey a similar meaning in different contexts. 6 Assumptions about the standardization of information structures and terminologies are questioned in the current study by explicating the interpretive work inherent in selecting and organizing standardized information for the specific purposes at hand. In so doing, our aim is to contribute to the current discussions on the possibilities and constraints of facilitating knowledge sharing through standardization across professional and institutional boundaries.
In the light of what actually takes place in face-to-face reports between healthcare workers, it is invariably so that much more than a simple transmission of information takes place. 7 As claimed by Hartswood et al., such interactions have a constitutive role in ‘arriving at some shared sense of what the meaning of information actually is’ (reference 7, p. 244). Moreover, as Hartswood et al. have demonstrated, local needs cannot be anticipated for all practical purposes and all possible readers. Patient records have different audiences and the information provided is intended to serve a wide range of purposes additional to everyday patient care. As brought to the fore in Garfinkel’s groundbreaking work on documentary practices, 8 whilst medical records could perfectly well serve the purposes of staff members, the information contained therein can be inappropriate in another context (see also Heath and Luff 9 ). The reason, argues Garfinkel, is that the sense of expressions and remarks in records ‘cannot be decided by the reader without his knowing or assuming something about a typical biography and typical purposes of the user of the expressions’ (reference 8, p. 201). In a similar although more far-reaching manner, information in EPRs is meant to be an important information source for other care providers outside hospitals, such as primary and elderly care, as well as serving the function of providing data at an aggregated level to serve external stakeholders. Since records are intended to serve a multiplicity of information needs, demands are placed on the reader to make sense of data that are relevant for the specific purposes at hand. Consequently, there is a need for local interpretive work concerning the meaning of the text, signs and data and their consequences in particular contexts. 10
In line with a growing body of research claiming the necessity for a better understanding of the practices that information systems are designed to facilitate, 7,9,11 we argue that there is a need for a better understanding of the concrete conditions necessary for sharing information by means of EPRs. Although there are many studies elucidating the contextual nature of information in medical records, 12–14 few have addressed how healthcare staff actually make use of information in EPRs in situ. The purpose of the current study is therefore to contribute to our understanding of such activities by focusing on the practical work of selecting and organizing structured information in an EPR in a way that enables staff members to make sense of past and future care activities. Of particular interest is the knowledge inherent in this process of transforming vast amounts of information into brief presentations that are relevant for staff members in their care of patients. To address this issue we have carried out detailed investigations of how nurses in shift handovers search for, organize and present information provided by EPRs. As suggested by Wilson et al., this is an instance of collaborative work ‘that has not yet been subject to as much scrutiny’ (reference 15, p. 28).
Following one tradition of workplace studies, the interest is in understanding how participants organize their activities so that they become intelligible and actionable. 9 In doing this we combine ethnographic observations with analyses of video recordings of activities central to the setting. In this study, we scrutinize the use of EPRs in a series of shift handovers and address (a) the process of drawing different pieces of information together into coherent presentations, and (b) how specific forms of construing information are intertwined with specific professional ways of organizing and presenting information. By explicating the practical work inherent in making use of information at the local level, we aim to shed light on and discuss the additional possibilities for sharing information over professional and institutional boundaries.
Empirical setting and analysis
In order to examine how EPRs feature in everyday healthcare work, this study has examined the use of a Swedish information system (Melior) at a stroke rehabilitation ward. In this setting the EPR had been used on a regular basis for two years as the major source of information by the team starting each new shift. Every shift invariably included one registered nurse and two or three assisting nurses. When the registered nurses arrived at an evening shift they received a short briefing by the nurses on the day shift about urgent or ongoing matters. Thereafter the registered nurse on the new shift completed a cursory reading of the EPR before giving an oral report to the other assistant nurses.
Shift handovers were chosen for the empirical study since these provide highly relevant activities where structured information in the EPR is actualized and explicated. The handovers were held in a meeting room on the ward itself where the shift members all sat around a desk so they could all see the EPR on the computer screen. The EPRs provide access to extensive amounts of information about every patient’s health status and needs that are derived from all of the professional groups operating on the ward (nurses, physicians, physiotherapists, occupational therapists). Since the time scheduled for handovers is constrained, in order to make oral handovers both intelligible and sufficiently concise, the reporting nurses have to differentiate between those pieces of information that are relevant and those that are not. The focus of the analysis is directed towards the differences between how information was sequentially ordered in the EPR, and the ways in which it was selected and organized in oral presentations.
In all, 200 hours of observations were carried out by the first author and, on the basis of these, 10 shift handovers were subsequently video recorded in order to enable a closer analysis. Each shift was responsible for on average 10 patients and the handover was usually between 45 and 60 minutes. In order to be able to capture detailed aspects of the staff members’ interaction with one another and with the interface of the computer system, a camcorder was positioned in a way that enabled it to capture the way in which the team members oriented to each other and when the nurses wrote in their notepads. A second camcorder registered what happened on the screen. The reason for this arrangement was to make it possible to see both the interaction of the staff and the simultaneous view of the user interface.
All of the video recordings were transcribed and the principles of video analysis suggested by Heath et al. were adopted. 16 In line with these guidelines the whole data corpus was systematically reviewed. The aim was to find regularities in how nurses searched for and selected information in EPRs as well as what they said when doing this. In a subsequent step the analysis was narrowed down to a closer scrutiny of the differences between how information was sequentially ordered in the EPR and the ways in which it was selected and organized in oral presentations. The sequences presented are aimed to illustrate the regularities in these differences in order to demonstrate the type of transformations that take place in ordinary care work.
Results
Information in EPRs is retrieved in other ways and is differently structured in comparison to paper-based forms of documentation. 2,3 Although many classes and categories of information are reproduced in the digital format, it is not possible to simultaneously view information in different files in the EPR. Interweaving information from different classes or files thus demands scrolling through the EPR and sometimes moving between menus (Figure 1). This implies that the reporting nurses cannot simply reproduce the written text. Frequently, an extensive reorganization of the content is carried out. Certain parts are selected and emphasized, whilst others are not taken up at all. One could say that different transformations or readings of the EPR are at play.
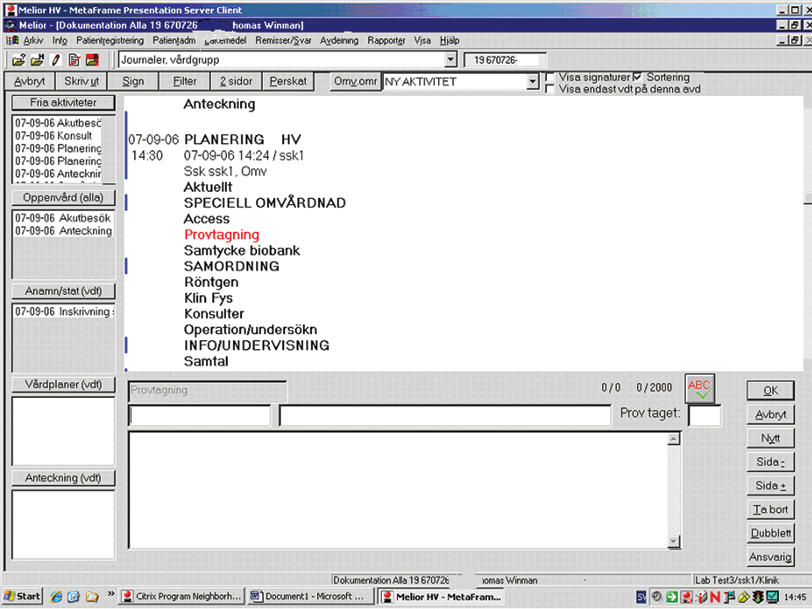
When the ‘Nursing record’ is chosen and a name from the list of patients is clicked on, a text is displayed that is structured by the main and subcategories shown
Reorganizing information into locally relevant knowledge
To illustrate how presentations of patients are sequentially structured, in Excerpt 1 we give a typical example from the onset of the report on one patient suffering from stroke. * When the registered nurse starts reporting to the assisting nurses about the patient, she initially focuses on the patient’s name, year of birth, date of arrival and the major medical disorders.
Excerpt 1
next we have Birgitta
(looks in her notepad)
in two one, Birgitta Svensson born thirty, who came in on
the ninth
(scrolls in the record and looks into her notepad)
look at this … weak right, aphasia
(looks interchangeably between the screen and her notepad)
I haven’t had a report on the CT … there is probably
nothing there either … we’ll see …
Fax one we could start with anyway …
When compared with the disposition in the EPR, the patient’s name, year of birth and date of arrival are provided in the first part, displayed when the record is opened up. The room and bed number, on the contrary, emanate from the nurse’s own notations. Up to lines 3–4, ‘who came in on the ninth’, the presentation of this piece of information seems rather straightforward, although not all information can be retrieved solely from the EPR. In line 5, however, the nurse scrolls between different parts of the record for a while. In line 6, she pays attention to two major symptoms, ‘look at this’, and reads from the screen: ‘weak right, aphasia’. In line 8, the nurse moves on, looking for the results of the CT scan (computerized tomography), which is a routine examination in cases where a haemorrhage or infarction in the brain is suspected. In the present situation the results are not found in the notes made during a prior report from the nurse on the previous shift: ‘I haven’t had a report on the CT’. Nor does she find the information sought for in the EPR under the main category Enrolment and its subcategory X-ray: ‘there is probably nothing there either … we‘ll see’. When the information sought for is not found immediately she scrolls up to the main category of Planning and to the first subcategory Fax I (line 10). †
The selection and order of data attended to by the nurse seem to be relevant for giving the other staff in the team basic information about who the person is, as well as her major disorders. It is important to note here that these data cannot be retrieved from a single section in the EPR. The analyses show that, although taken for granted and unnoticed in everyday practice, extensive work is expended in the ordinary retrieval and organization of data provided by the EPR. Due to the ordering of categories in the EPR and the order in which different topics are addressed in the handover, an extensive reorganization is carried out, which is further illustrated in Figure 2.
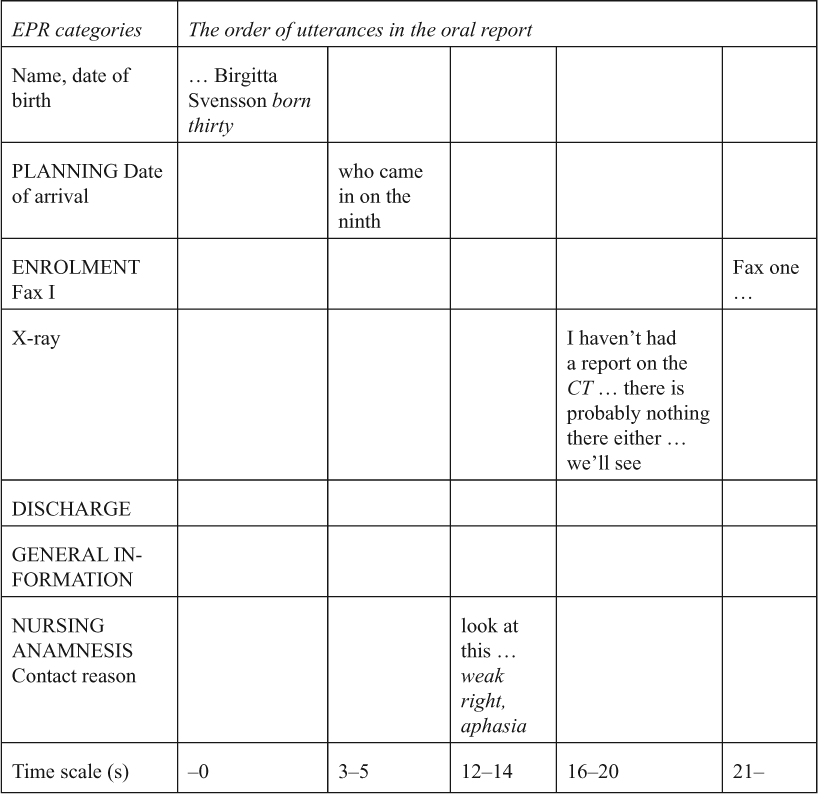
The first column shows the first five main categories of the record and the subcategories addressed. The other five columns show, from left to right, the order of utterances. The time scale in the final row starts with zero when the first utterance is finished and then indicates the onset and duration of the following utterances (in seconds) corresponding to each category
The steps needed for carrying out this reorganization are underlined by the difference between the structure of the EPR and the order of the nurses’ utterances. A typical feature of the reports is that the moves undertaken vertically are frequently associated with interruptions in the flow of talk. The sequential order follows a regular pattern in the nurses’ oral reports, but it is noteworthy that it deviates significantly from the structure of the classification in the EPR. The transformation needed for bridging these different structures puts demands on the reporting nurses in that they are required to reorganize the information in a way that is better adapted to the responsibilities of the team, i.e. to help patients in their daily living and rehabilitation. Since the structure of the EPR is supposed to serve information needs for different purposes, different professionals and different stakeholders, the structure of the oral report needs to be transformed to the specific tasks and obligations of the team. The selection and reorganization of particular elements into a coherent whole, as demonstrated here, are a necessary presumption in order to convey a meaning that is sufficiently specific and precise.
It is apparent that the patient’s story is referred to not in chronological order, or in the order of the EPR, but rather in a specific order that is structured by the conventions of oral briefings in healthcare. This is what Montgomery Hunter refers to as institutionalized narratives. 17 For nurses, this structure serves as a means not only for deciding what information is relevant, but also for reorganizing pieces of information emanating from different parts of the EPR into an intelligible and concise briefing. In contrast to the findings of Montgomery Hunter, the nurses’ briefings in our study seldom resulted in explicit suggestions for further interventions. Nevertheless, the shift handovers regularly seem to fulfil the staff’s prospective needs about how to continue with their work by providing highly specific pieces of information. The instance of ‘weak right, aphasia’ (Figure 2), addressed initially in the briefing, is a piece of information indicating both the nature of the patient’s problems (perceptual, motor, intellectual) and the need for assistance to manage her daily life (eating, walking, communicating). Both understandings are important for the staff members since the utterance implies a background both from which further information would be understood and for the specific care activities that have to be carried out with respect to their obligations as professionals on a rehabilitation ward. Even though the utterance is intelligible regardless of professional group, its consequences are bound to the context in which it is used. 8 In a similar vein, the results of the CT scan would have provided explanations of the current problem and indicated other potential problems and needs that could occur.
The sequencing of the presentation in Excerpt 1 follows the typical order of all reports on the ward and is recognized as a typical narrative structure for presenting medical cases used since the early days of medicine. 18 It is noteworthy that the EPR does not itself support a narrative structure. It is something that nurses have to be familiar with to be able to organize information so that it becomes intelligible in the context of their own and the other team members’ duties. The extensive reorganizing of the information provided also involves a way of constituting a new temporality that in turn provides possibilities for addressing causality. A typical way of doing this is exemplified in Figure 2, in which the cause of the patient’s initial request for care is addressed immediately after presenting personal data about the patient and her date of arrival. This parallels the results of other studies of professionals, such as for example how engineers need to break down complex issues in order to reorganize information into solvable problems. 19 If, instead, the structure of the EPR had been strictly followed it would have implied that the burden of the interpretive work would have been put on the individual team members in the sense of having to reorganize the information needed for the following shift.
Constituting figure ground through highlighting and selecting
In addition to the reorganization of the content of the EPR, as illustrated by Figure 2, specific topics are regularly put in focus by foregrounding some parts and backgrounding others. Figure ground is created by processes of highlighting and selecting. One way of doing this is to stress certain parts of phrases and merely mention others. In declaring, ‘look at this … weak right, aphasia’ (Excerpt 1), the first phrase is uttered in a low voice whilst the symptoms articulated in the second phrase are stressed, thereby indicating that the latter is to be regarded as something significant to be taken into consideration. Similarly the CT scan was focused on when the nurse says that ‘I haven’t had a report on the CT’. In contrast, the following utterance, ‘there is probably nothing there either … we’ll see’, is pronounced with neutral tone. The symptoms and the results of the CT scan are thus highlighted as being of significance for the team, whereas the subsequent utterance appears as less relevant and as a sort of meta-comment to the nurse herself in her attempts to find relevant data.
A similar pattern can be seen in Excerpt 2, in which ‘fax one’ is emphasized, whilst the tests and examinations are enumerated as mere reiterations of the text. What is shown in this excerpt, however, is that although the text in the EPR is not reorganized, the nurse’s oral presentation still includes extensive work in selecting relevant information.
Excerpt 2
… fax one was done on the fourteenth … eeh urine culture just
like on the fourteenth
(writes in her notepad)
eeh she’s been on a clinical UCG … doppler carotids …
referral to speech pathologist has been sent
(writes in her notepad)
the fourteenth that is … right hand lens should be changed it
says … says that right hand eye lens should be changed round
about the thirteenth of the first
(writes in her notepad)
As mentioned earlier, Fax I is the first subcategory under Enrolment. The tests attended to by the nurse – urinary culture, UCG, doppler of carotids – and the fact that a referral has been sent to the speech therapist, are reported in the same order in which the subcategories appear in the EPR. It is important in this respect to note that following the order set by the EPR does not mean that the content is simply reproduced. Similarly to the case in Excerpt 1, when data about the patient and her major medical disorders were in focus, parts of the text in the EPR are omitted and not referred to at all. In Excerpt 2, by focusing the tests carried out, only three out of a total of 21 tests entered in the EPR were mentioned, i.e. urinary culture, UCG and doppler of carotids. This means that a relatively limited part of all the information available in the EPR is in fact brought to the fore as relevant to the task at hand. Moreover, Excerpt 2 demonstrates how information is organized into a useful form by entering specific pieces of selected information in notepads. Various events such as Fax I, results of tests and the referral to the speech therapist are all facts that are entered in the notepad by the reporting nurse. This means that making notations has a prospective purpose, where the notepad can function as a tool in fulfilling essential professional obligations during the following shift. This parallels findings from other studies 20,21 which have suggested that handover sheets have the possibility to function prospectively as a personal waypoint, rather than merely as a repository of information.
Several studies have emphasized the centrality of shift handovers to support the planning of care, but have also criticized nurses’ handovers for lacking prospective perspectives or for giving mere summaries of past events. 18,22 Lamond argues in a review study of shift handovers that ‘all of this indicates that the information in the reports sometimes takes the form of a summary of the patients’ condition or progress’. 23 Our results, in addition, point to the practical and ordinary ways in which such retrospective accounts actually fulfil prospective purposes. On the one hand, our study indicates that the structure of the EPR poorly supports a prospective approach, since extensive reorganizations are often needed for relating interventions and their effects. On the other hand, nurses provide prospective perspectives on what has to be done by making use of the mainly retrospective content of the EPR. In Excerpt 2 this is done by the nurse in reading out a temporally ordered case that involves known details stored in the EPR. This bit-by-bit reading and entering of notations in notepads are important steps for highlighting instances that can be further checked and questioned during the following shift and which can function as a basis for future entries in the EPR. Reading information in its original form is thus the first step in ordering information and in constituting a problem that it is possible to act upon. All aspects relevant to the case are read out as they occur on the screen. This first step, however, does not say anything about the causes of the patient’s problems, or how these should be dealt with. In line with Suchman 24 a second step is necessary for constituting a temporality that provides opportunities for understanding the causal relations between the discrete aspects of the problem (cf. reference 25). This is achieved by the selective reading and reorganizing of information into a textured account, implying a focus on conjectures as to causes and effects that are anticipated to follow on from the work to be carried out. This constitution of causality does not only involve knowing how to select those events that are related to each other. 26,27 It is, additionally, also a matter of constituting a temporality that provides opportunities to understand the causality of the problematic aspects of the case, as well as the problematic aspects of working with the case. This is what Berg calls ‘bringing life to text’. 26
Discussion
The nature of the gap between formal information and the demands of locally interpretive work is demonstrated by the differences between the structure and content of information in the EPR and the nurses’ oral presentations during shift handovers. We maintain that the employment of this work displays essential aspects of professional achievements necessary for putting information into practical use. In a similar vein, as suggested by Duguid, 27 we propose that sharing information is not merely about the transmission of codified information, in that it also requires knowledge on how to codify this information. Knowing how is thus a prerequisite for knowing that. The explication of the practical work in selecting and reorganizing may also shed light on the possibilities for sharing standardized information over institutional boundaries. As claimed by Duguid, such efforts require a degree of shared knowing on how such information should be understood: ‘But when the practices of knowing how of two communities are different, epistemic barriers develop and productive sharing of knowing that becomes much more challenging’ (reference 27, p. 114). Our argument, that transformations of information needed within one single institution demand intrinsic knowledge of the situations in which it is produced and will be used, counteracts the idea that increased standardization by itself is a solution to the problems of sharing information between different kinds of institutions. This is in line with Færgemann and Schilder-Knudsen who argue that, in contrast to local or internal work, the inter-institutional is ‘much more complex. Actors do not in the same way have direct access to each other’s knowledge and capacity’ (reference 28, p. 178).
The movement towards standardization has been further accentuated by the introduction of EPRs, since the ability to enter free and unsorted text is further constrained in the electronic format. 29 The efforts to standardize information structures in EPRs imply a restriction to its openness. We suggest, however, that openness is essential for the utility of the EPR, something that is illustrated by the nurse’s moves between categories and which is indeed a prerequisite for constituting a coherent narrative (Figure 2). Moreover, the instance of ‘weak left, aphasia’ simultaneously refers both to the patient’s problems and to the possible needs for care, i.e. both a diagnosis and an intervention. This exemplifies how open category systems cause relevant information – which relates to both the patient’s present health problem and the staff’s work – to be loaded into the system. 7 Information entered under a given category in the EPR can refer to different phenomena, and similar aspects of a patient’s health problem can be classified under different categories. Since it is impossible to know in advance when, where and why specific pieces of information are relevant, the category system needs to be open to many possible demands for information. 30 An important conclusion is that the necessity for openness also points to the need for professional conduct to transform information into locally relevant knowledge. As a consequence a more constraining structure is unlikely to provide a solution for limiting diverse interpretations, since it may simultaneously constrain the possibilities for staff to transform information into practical use and, thus, weaken it as a clinical tool. 31
In the move towards a standardized information structure it is suggested that standardized terminologies are a prerequisite for sharing information, especially across professional and institutional boundaries. 32 We do not deny that there are needs for a shared conceptual apparatus in healthcare and social welfare that is sufficiently distinct for entering and retrieving information. We argue, however, that it would be a mistake to believe that a shared conceptual framework could by itself provide such a solution since the application of a given terminology also presupposes extensive skills for transforming the formal and conceptual into something that is relevant and intelligible for users in specific situations. As stated by Timmermans et al., 32 the use of categories and terminologies contributes not only to link professionals’ everyday language to education and research, but also to permeate ideas of what the profession is all about. Since the conceptual apparatus is at the core of the professional knowledge itself, the changes of terminologies interfere with the language already in use. The implementation of standardized terminologies thus has to take into consideration can be raised the extent to which writers and readers with different terminologies, professional knowledge, etc. are able to understand each other. The specific meaning of ‘weak left, aphasia’ for instance, is dependent on the staff members’ knowledge of what these terms imply in terms of their obligations for this particular shift on this particular rehabilitation ward. For administrators of care for the elderly, or for a speech therapist or a physiotherapist, these terms imply very different meanings of the nature of the problem and the institutional obligations they imply. As a consequence, one decisive condition for sharing standardized information is that it is open to different readings that can serve the information needs of different parties and stakeholders. Taking this into consideration is necessary for meeting the challenges of the computerization of healthcare, or as Færgemann and Schilder-Knudsen put it, ‘One of the main challenges for computer support in the health care area is to facilitate shared care to ensure coherence and continuity’ (reference 28, p. 165).
Conclusion
Our results demonstrate how processes of reorganizing, selecting, highlighting and constituting causality are decisive steps in putting information in EPRs into practical use. One central conclusion is that professional ways of codifying information are necessary resources in transforming text to talk in ways that are relevant for the purposes of shift handovers. This dependency of institutionally bound knowledge, in turn, indicates the necessity to acknowledge that knowing how is needed for information systems to serve the purpose of providing important information about patients and clients over institutional and professional boundaries. Our argument is that the extensive efforts currently put into developing standardized information systems for sharing information in and between healthcare and social welfare institutions, on national and international levels, ought to take into account the knowing how inherent in transforming information into professionally relevant knowledge. Most importantly, it seems necessary to consider the extent to which professionals within different institutions and authorities share the knowledge needed for transforming the same information into something that makes sense in relation to their different obligations and tasks. If this does not take place it is our belief that enormous efforts and financial resources will be wasted on an endeavour that may lead up a blind alley.
Footnotes
*
Emphasized parts of utterances are italicized. Short pauses are indicated with ‘…’ and non-verbal activities are indicated within single parentheses ( ). The names of patients are fictive.
†
To send ‘Fax one’ refers to a routine Fax I applied when the authorities caring for the elderly in the municipality have the responsibility for further care.