
Abstract
Background
Trauma is the third largest contributor to the global burden of disease with 90% of the trauma-related mortality occurring in low to middle income countries (LMICs) such as South Africa. The Acute Physiology and Chronic Health Evaluation (APACHE) II is widely used, but was developed in a first-world setting. This study sought to evaluate the APACHE II's ability to predict intensive care unit (ICU) mortality among trauma patients in a LMIC and to identify predictors of mortality within this population.
Methods
This retrospective study was conducted by analysing data records of 284 ICU patients over 2 years. Performance of the APACHE II was assessed with calibration and receiver operator characteristic curves. Survivors and non-survivors were compared using descriptive statistics, and logistic regression identified independent risk factors.
Results
An overall mortality rate of 18.8% was observed. Sensitivity of the APACHE II was 0.74, and specificity 0.68. The model showed good discrimination (area under receiver operating curve (AUROC) 0.82, 95% confidence interval) and calibration (Hosmer–Lemeshow p > 0.3). The cut-off value for APACHE II was 20.2. Community assault and intubation were more common in the demised cohort (p < 0.01, odds ratio (OR) 4) although the APACHE II remained the strongest predictor of mortality when adjusting for confounders (p < 0.001).
Conclusion
APACHE II is a valid mortality prediction tool in polytrauma patients. Patients with scores above 20 were at highest risk of mortality. Intubation and community assault were significant risk factors of mortality, however, they aren’t included in the APACHE II score, highlighting the need to consider additional risk factors in the trauma population.
Introduction
Trauma, as classified by the World Health Organization, ranks as the third largest contributor to the global burden of disease, yet its management often lacks the same level of priority afforded to communicable and chronic diseases.1,2 This oversight is particularly pronounced in resource-limited countries like South Africa (SA), where the multifaceted toll of trauma is staggering. 3 SA has an unparalleled high trauma burden when compared with first-world countries and experiences over 30,000 trauma-related deaths annually. 3 The financial burden of trauma on the healthcare sector is high, with interpersonal violence (IPV) contributing towards a large proportion of trauma-related costs.4,5
In SA, approximately 50% of all intensive care unit (ICU) admissions are trauma-related admissions. 6 ICU services are expensive and are a scarce commodity especially in the public healthcare system. 7 Albeit the overall ICU bed-to-population ratios in SA are in the mid-range by international comparison, most of these beds are found in the private health sector, accessible to only a minority of the population. 8 The ICU bed to hospital-bed ratios are 2.2% in the public sector, compared to 14.3% in the private sector. 8 Careful selection of these patients into an ICU needs to be considered and objective scoring systems are thus a useful tool in triage and resource allocation. The Acute Physiology and Chronic Health Evaluation (APACHE) is an example of one such tool. 9
The APACHE II scoring system has emerged as a widely used tool for predicting mortality in critically ill patients. Developed in the early 1980s in a first-world setting, APACHE II incorporates the worst physiological parameters within 24 hours of patient admission to an ICU, age, and chronic health conditions to generate a numerical score indicative of disease severity and prognosis. 9 The computer-generated numerical score translates to a percentage mortality risk which is used to estimate ICU mortality. Whilst extensively validated in various critical care settings, its performance in predicting mortality among polytrauma patients in low middle income settings such as SA is limited.10,11 In addition, SA has a different disease burden with disproportionately high trauma rates when compared to the setting in which the APACHE II was developed. 3 Despite APACHE II being widely used, there is a paucity of local data evaluating its utility, specifically in trauma patients.
The intention of our study was to evaluate the APACHE II's ability to predict in-ICU mortality among trauma patients and to identify the strongest predictors of mortality within this population. Secondary objectives were to assess the inter-rater agreement between the APACHE II scores documented by clinicians and those independently calculated by the primary investigator (PI).
Methodology
Study design
This retrospective observational descriptive study was conducted at a tertiary hospital in the Western Cape, SA, from 1 March 2022–30 June 2024. Overall, 284 patient records met criteria for retrieval and analysis. For this study, the definitions in Table 1 were used. A sufficiently predated period was chosen to prevent missing data due to frequent delays in uploading patient information onto electronic systems. Only complete patient records were retrieved, thus there were no missing data. Level 3 multi-disciplinary ICUs served as the study site, accepting admissions from within the hospital and peripheral referral hospitals. Sample size was calculated based on an estimated receiver operating curve (ROC). Minimum Area under the ROC (AUROC) of 0.8 was used as a good estimate. Width of the confidence interval (CI) was defined as 0.125 and overall confidence defined to be 95%. Estimated mortality rate of polytrauma ICU patients for this study was calculated as a post-hoc combined analysis using known data from the study site resulting in an aggregated 28.44% mortality rate. In conjunction with the described AUROC, a sample size of 284 participants was recommended. Convenience sampling was employed. Eligible participants encompassed all polytrauma patients admitted to these ICUs during the specified timeframe whilst patients under 18 years of age and trauma admissions with single organ involvement were excluded from the study.
Definitions used in this study.
ICU: intensive care unit.
Data collection was conducted utilizing data from an online patient database. The ICU electronic database was used to document the actual mortality. Each deidentified case's data were captured on the secure online application ‘REDCap’ and later exported to Microsoft Excel.
Ethical approval for this study was obtained from the Health Research Ethics Committee [S24/04/092]. Approval was also obtained from the Institutional Review Board. [WC_202409_018].
Data analysis plan
Descriptive statistics were obtained using Python 3.11 software, in consultation with a biostatistician. For all statistical analysis, the alpha level of statistical significance was set at 0.05.
PI APACHE II calculation
The APACHE II score (Figure 1) was calculated (worst variables within 24 h of admission to ICU) 9 and then recorded on the spread sheet. The actual mortality was obtained from the ICU electronic database.
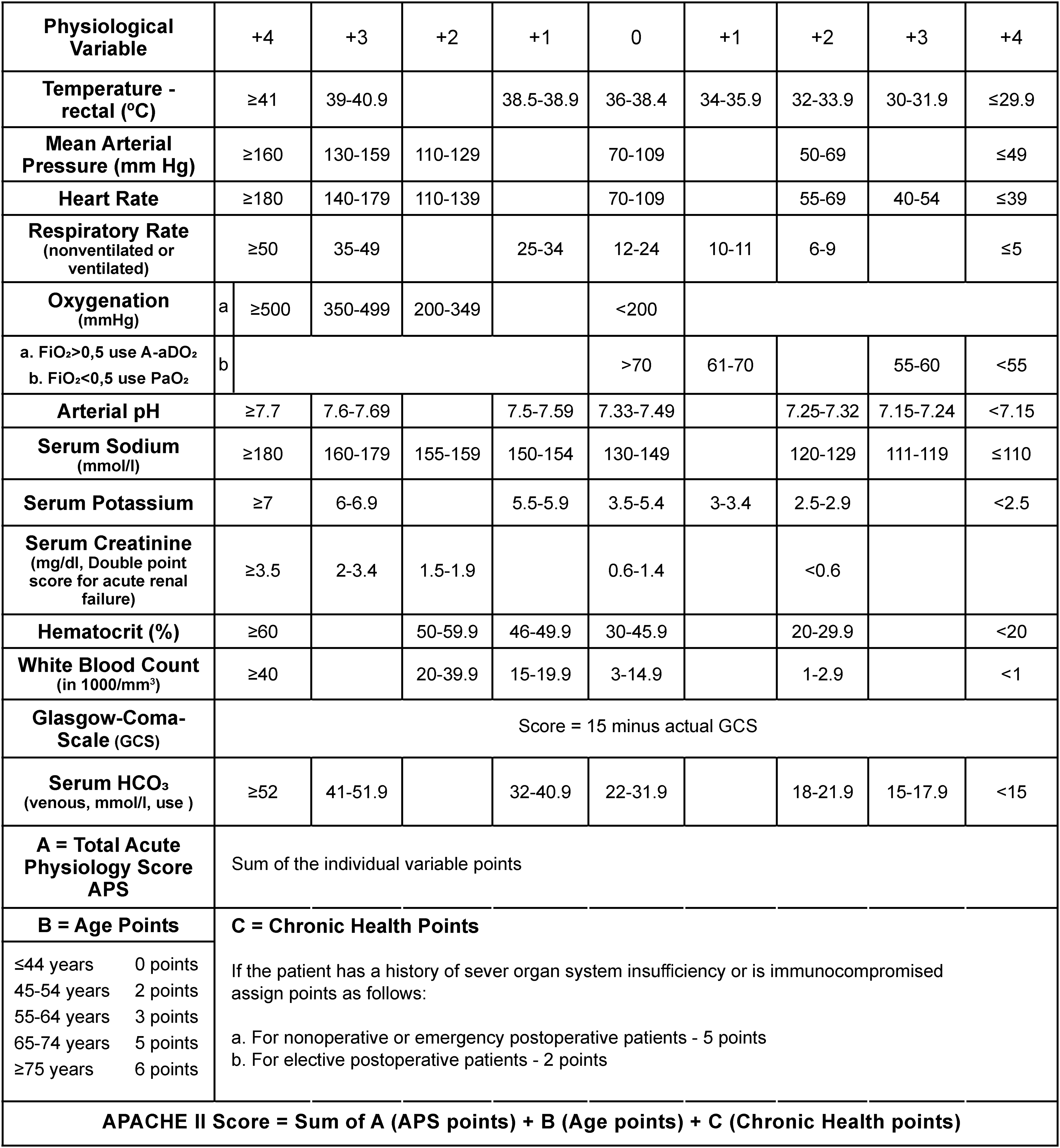
APACHE II scoring system parameters and interpretation.
Descriptive analysis
Frequency and percentage were calculated for categorical data, and means and standard deviation or median and interquartile range (IQR) were calculated for normal or non-normally distributed continuous data. Mann–Whitney-U test was used for basic comparison of means between continuous data, and Chi-squared test and odds ratios (ORs) with 95% CIs were used for comparison between categorical groups.
Evaluation of APACHE II
Discrimination is the ability of the model to accurately distinguish between survivors and non-survivors which was obtained by a ROC. Specificity and sensitivity was used in this study, and thus the AUROC calculated. An AUROC of 0.5 equates to random chance and 1 is considered perfect discrimination. 12 An AUROC of greater than 0.8 is preferred for a good prediction model. 12 In line with calculation of the sample size, the width of the CI was set at 0.125 with an overall confidence level of 95%.
“Calibration refers to the ability of a model to describe a group of patients accurately. If the number of deaths in the actual population is close to that which was predicted, then the model is well calibrated.” 13 For calibration, the Hosmer–Lemeshow statistic was used. Calibration is displayed by means of a calibration curve (expected vs actual mortality) with 95% CIs calculated for actual mortality.
Inter-rater reliability
Intraclass correlation (ICC) was calculated to determine inter-rater reliability. Significant level of discrimination between raters was set at ICC of 0.2. Specifically an ICC (3,1) model, which indicated a consistency ICC in the presence of bias, with comparison of only two raters, was used. 14
Risk factors
OR was used as a basic overview of univariate risk factors. A multivariate logistic regression analysis was run to identify risk factors of mortality, adjusting for co-variates. Variables with total counts less than 10 were excluded. The multivariate logistic regression model was built with variables backward-selected from univariate logistic regression model with p > 0.25. OR and p-values were calculated and reported for each variable in the model.
The clean dataset for the study has been made available online through https://figshare.com/s/7133848947e6d235e6be. This study was reported according to the strengthening the reporting of observational studies in epidemiology statement.
Results
Baseline characteristics
In total, 284 patient records met criteria for analysis. The study population was largely male (n = 242, 85.2%) with a low rate of female admissions (n = 42, 14.8%). The median admission age was 35 [IQR 27–44]. The human immunodeficiency virus (HIV) positive status rate was low (n = 22, 7.5%) with a large amount of unknown HIV statuses (n = 178, 62.7%). The majority (78.9%) of the study population had minimal comorbidities. Of those that had comorbidities hypertension was the most prevalent (n = 37, 13.7%) followed by diabetes (n = 15, 5.3%).
Injury types were diverse. When looking at the mechanism of injury (MOI), IPV (assault, stab, gunshot wounds (GSWs), community assault) was the biggest contributor towards admissions (n = 135, 47.5%), this was closely followed by road traffic accidents, i.e. motorcycle accidents, pedestrian vehicle accidents and motor vehicle accidents (MVAs) (n = 119, 42.5%). High rates of MVA (21.5%) and GSWs (29.9%) were observed (Figure 2).
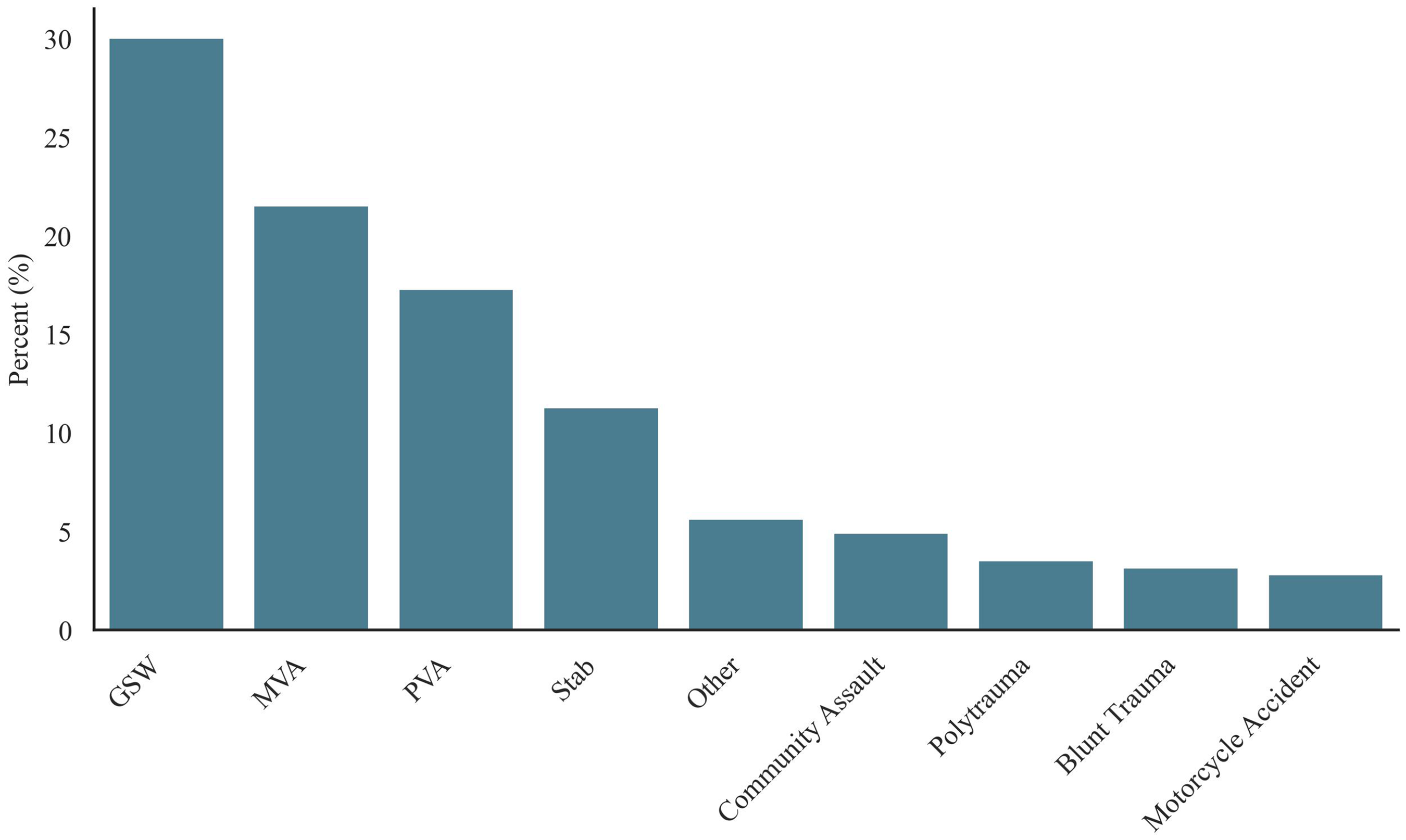
Bar graph of admission diagnosis.
The median length of stay (LOS) in hospital before ICU admission was 1 day, whereas the median LOS in ICU was 5.5 days; 81% patients received emergency surgery, and the majority were emergency admissions. Our study found an overall mortality rate of 18.8%.
The majority didn’t have any severe organ failure (n = 283, 99.6%). We found a 44% (n = 125) incidence of acute kidney injury (AKI). There was a 19% incidence of FiO2 > 50% (n = 54) which lends itself to the high number of intubated patients (n = 214, 75.4%)
Evaluation of APACHE II
The sensitivity of the APACHE II model was 0.74, and specificity 0.68. Calculated AUROC score was 0.82 (Figure 3). Calculated Hosmer–Lemeshow p-value was >0.3 and the calibration curve also followed a generally linear path (Figure 4). Median APACHE II score was 18.
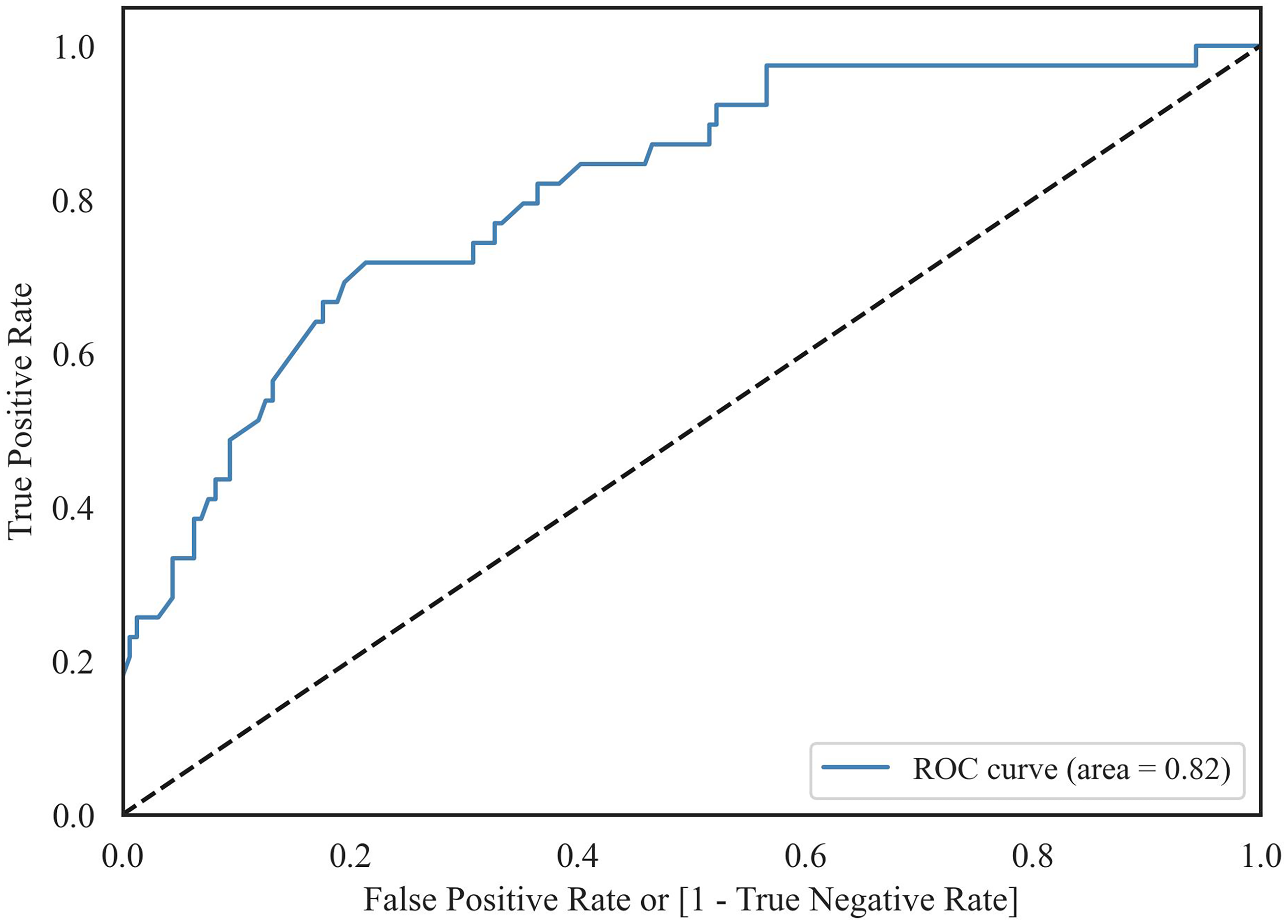
Receiver operator curve.
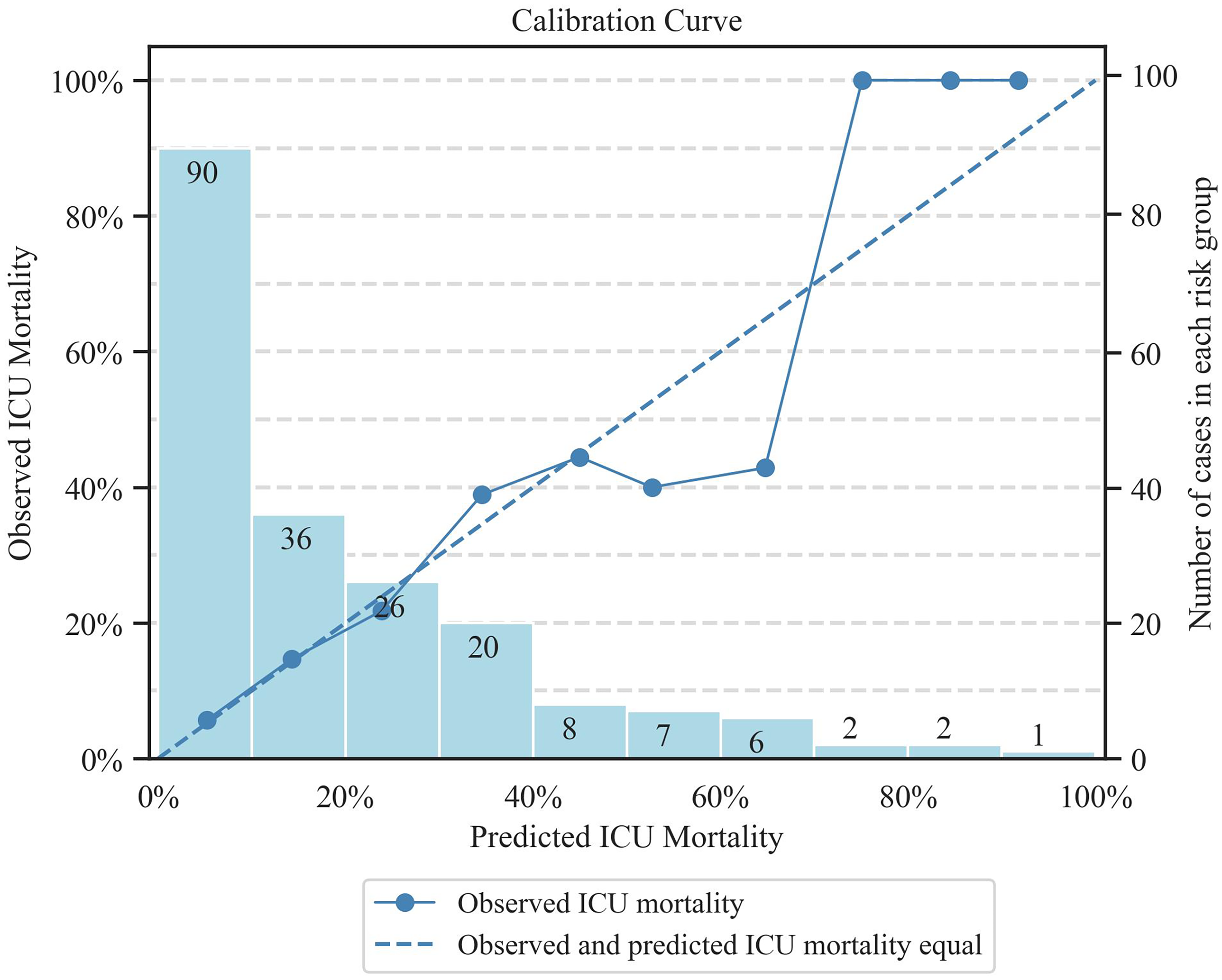
Calibration curve.
Logistic regression analysis of calculated APACHE II score (Figure 5) against demise in the ICU demonstrated a correlation coefficient of 0.19 [0.12, 0.26], with a p-value ≪0.001 [OR 1.21.] The cut-off APACHE II score in predicting mortality was found to be 20.2, indicating that patients with scores above 20.2 are at highest risk of mortality according to the model.
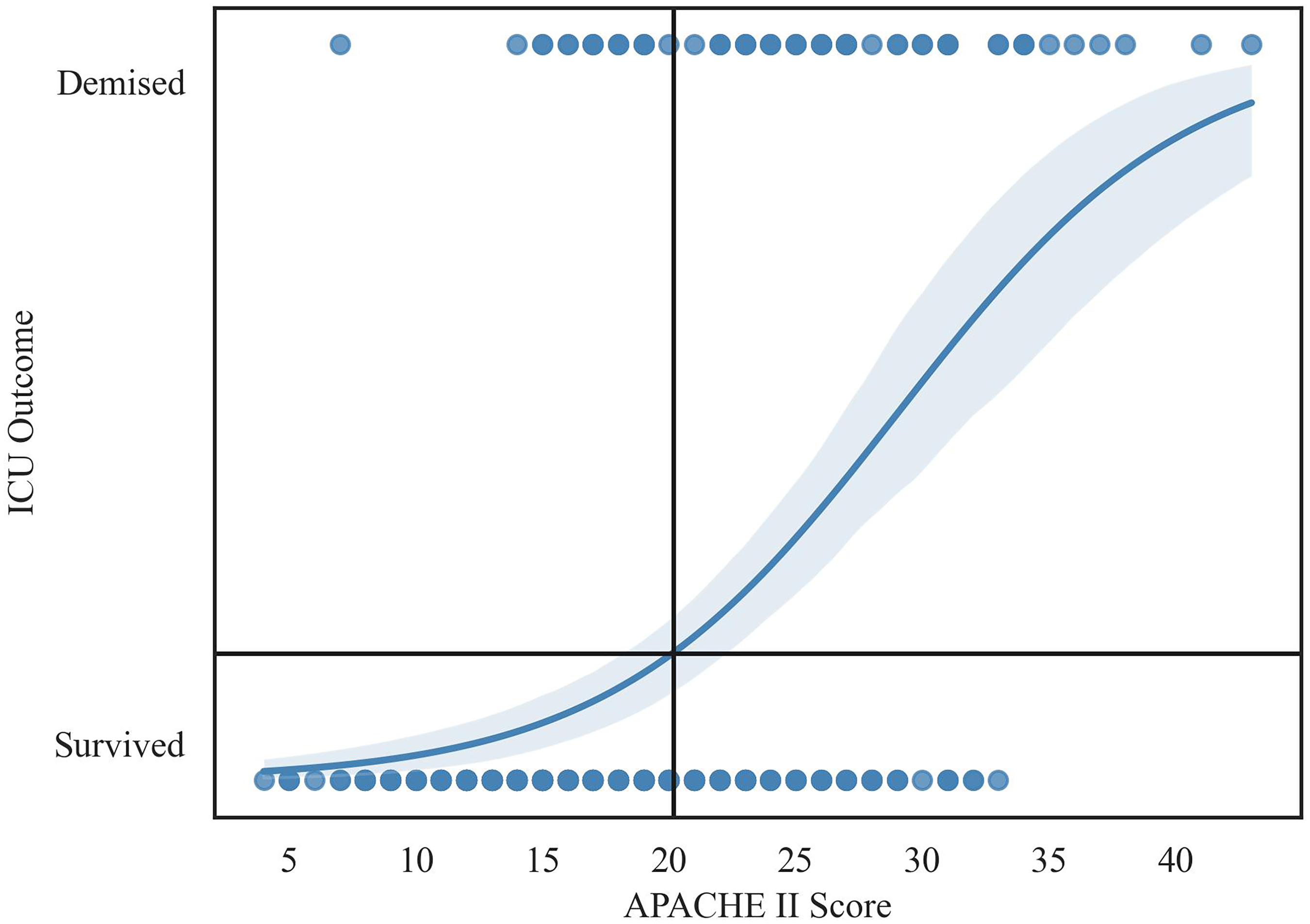
Graph of logistic regression curve with shaded 95% CI.
Risk factors
There was a statistically significant relationship between admission diagnosis of community assault and demise (p = 0.003), (n = 14), OR 4.47 [1.28, 15.72]. There was also a statistically significant relationship between a patient being intubated and demise (p = 0.002).The incidence of intubation in the demised cohort was 91.1%, compared to 71.5% in the survivor cohort, OR 4.05 [1.52, 13.59].
There was a statistically significant difference in the distribution of APACHE II scores between the survivor and demised cohorts (p < 0.001), OR 1.21. Median APACHE II score in the survivor cohort was 16.5 [13.0, 21.0], whereas the median APACHE II score for the demised cohort was the significantly higher 25.0 [19.0, 31.0].
Of the risk factors described, the APACHE II score was the most statistically significant factor in determining mortality when adjusting for confounders (using multivariate logistic modelling) with a sensitivity of 0.72 and specificity of 0.69.
Inter-rater reliability
Inter-rater reliability, ICC was found to be 0.604 with a 95% CI of [0.5–0.69], and p-value <0.001 (Figure 6). This indicates only a moderate agreement between calculated and recorded APACHE II scores.
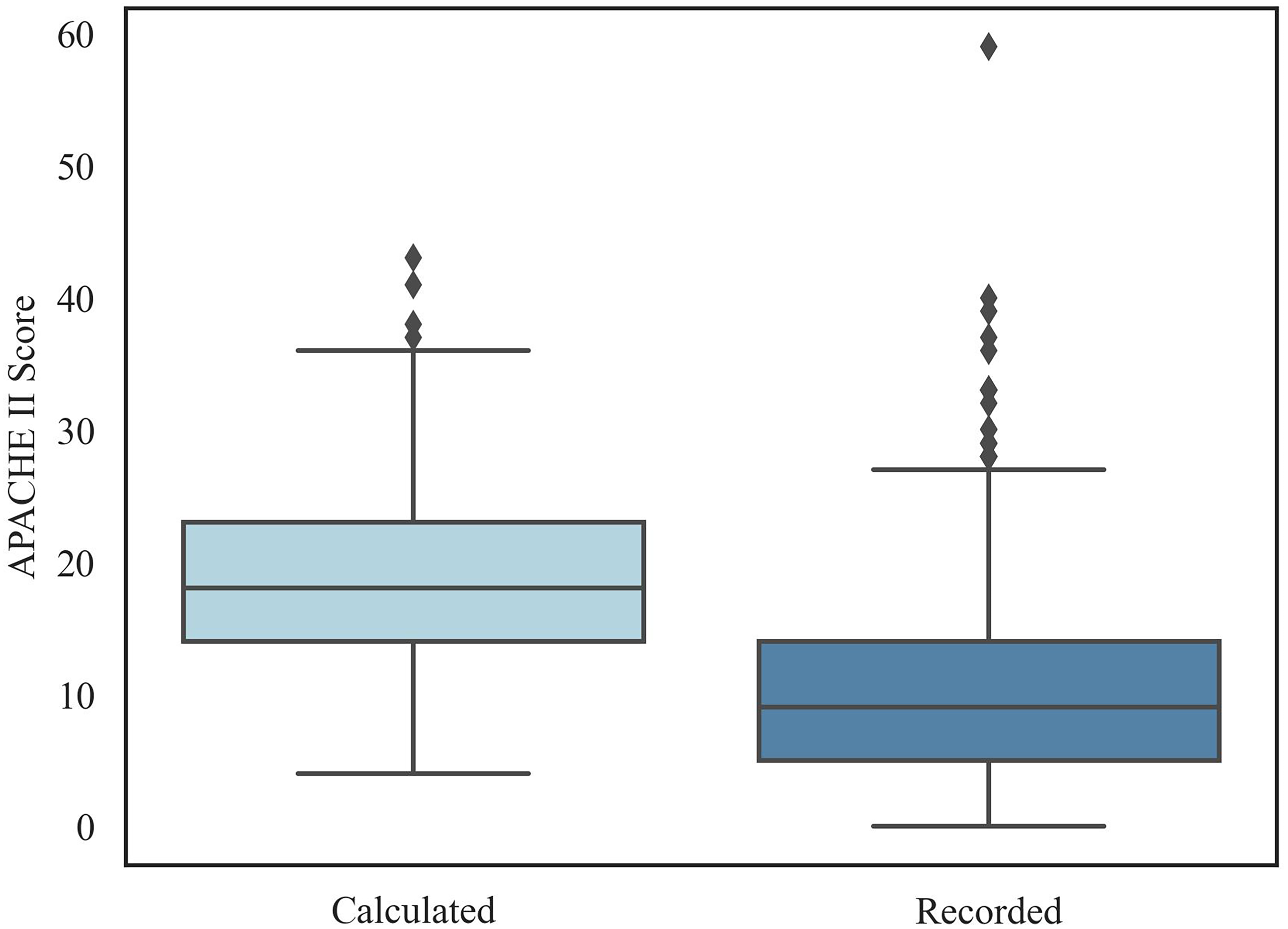
Box and whisker plot of calculated vs recorded APACHE II scores.
Discussion
Our study found a median APACHE score of 18 which closely aligns with local data in which the average APACHE score was 17.4. 13
Despite data from a 1992 American-based study stating that the APACHE II was inferior to alternate trauma scoring systems as it lacked an anatomical component, 15 we found that the APACHE II demonstrated good discrimination and calibration in our setting. Importantly, APACHE scores above 20 were at highest risk of mortality (Figure 5) suggesting that the score may be valuable not only for prognostication but also as a selective triage tool. In resource-limited settings such as ours, early identification of high-risk patients could facilitate more judicious allocation of resources.
When comparing our findings to a study done at the same institution 10 years prior, Van Der Merwe et al. found an AUROC of 0.83, and the model was within a 95% CI of the hospital mortality, albeit the ICU in question cared for predominantly medical patients. 13 This reinforces the APACHE II as a valid and reliable model to use in our context, as both studies demonstrated consistent discrimination and calibration of the model spanning 10 years. 16
This study found an overall mortality rate of 18.8% which is comparable to local data which typically describe a mortality range from 10–32%.17–20 Our study found a lower mortality rate when compared to previous years which could potentially reflect changes in trauma practice. 1 We hypothesize additional reasons for the lower observed mortality; the quoted range is a combination of 30 day hospital mortality and ICU mortality, and this study looked exclusively at ICU mortality, thereby potentially under estimating mortality. Secondly, polytrauma patients in alternative ICU settings such as the resuscitation room in the emergency department were excluded. Lastly there are other determinants of mortality which could have influenced the discrepancy, such as case severity, delayed presentation, geographical location, and limited resources which is a common issue in low to middle income settings.2,3,5
As noted in Table 2, admission diagnosis of community assault, being intubated in the ICU, and calculated APACHE II score were the only risk factors to impact demise in the ICU.
Comparison of demographic data for survived vs demised cohort.
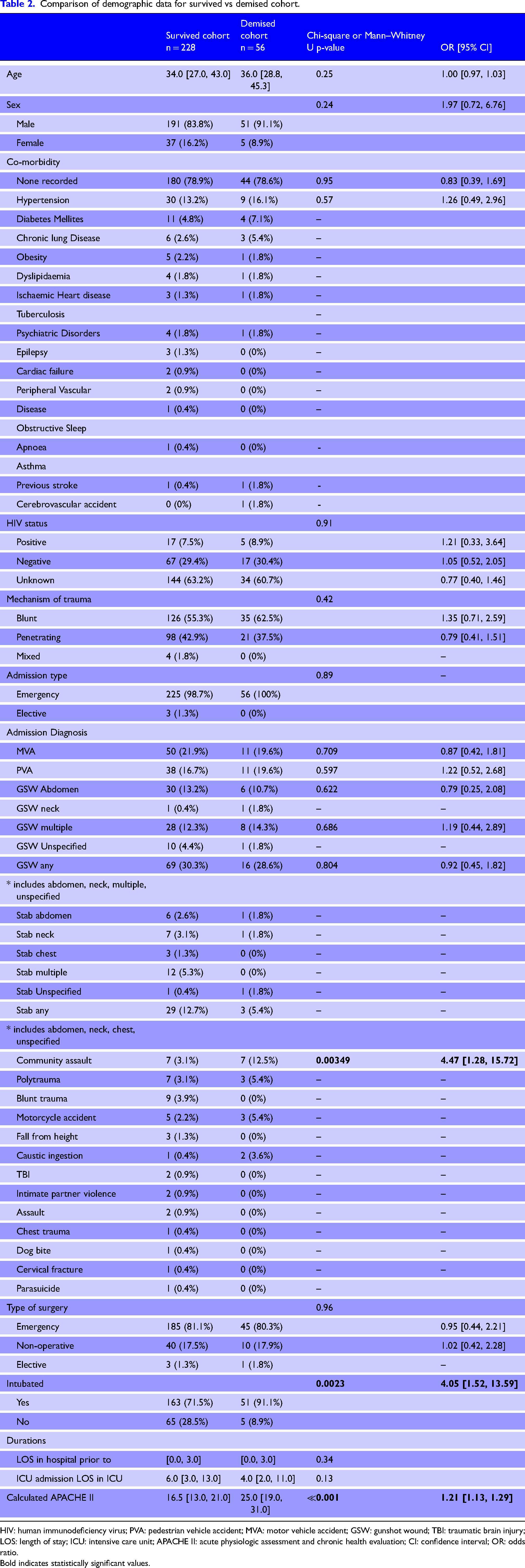
HIV: human immunodeficiency virus; PVA: pedestrian vehicle accident; MVA: motor vehicle accident; GSW: gunshot wound; TBI: traumatic brain injury; LOS: length of stay; ICU: intensive care unit; APACHE II: acute physiologic assessment and chronic health evaluation; CI: confidence interval; OR: odds ratio. Bold indicates statistically significant values.
Whilst there was a statistically significant relationship between community assault and demise, these data were severely limited (n = 14) and warrants further investigation instead of offering conclusive evidence of a relationship. Whilst further studies are recommended to elucidate this link, this finding (in accordance with literature) suggests that certain MOI'S are important contributors towards mortality in the trauma population and physiological variables cannot be looked at parochially. This is an important finding as MOI is not incorporated in the APACHE II. Scoring systems which incorporate MOI such as the ‘TRISS’ remain valuable, and there is benefit in comparing these systems against the APACHE II in low to middle income settings.10,11
The APACHE II score does not include intubation as a variable; however, the subsequent APACHE IV (which has superseded the APACHE II in accuracy) incorporates mechanical ventilation as a covariate. 21 Prehospital intubation has been described as a risk factor of mortality in trauma patients. 22 Because our study didn’t delineate where tracheal intubation took place, a subgroup analysis on location of intubation, mechanical ventilation days, and ventilator-free days would be beneficial to understand this finding better.
Intubation, and especially prolonged intubation, is associated with complications such as peri-intubation events (cardiovascular instability, hypoxaemia, and cardiac arrest), aspiration, and ventilator-associated pneumonia. 23 Our study found a high incidence of blunt trauma of 56.7% (which is usually associated with chest trauma5,6) and underlying injuries such as pulmonary contusions, which could place these patients at a higher risk of intubation-related events. In addition, many patients were intubated as a baseline in the ICU. Since ICU's offer organ support with more critically ill patients requiring more support, it's not clear whether the increased risk of mortality is related to intubation per se or to the extent of case severity.
As mentioned, the APACHE II doesn’t include intubation as a variable; however, the association is implied with the FiO2, as many patients requiring higher FiO2 are usually intubated. Our study found (n = 54, 19%) requiring FiO2 > 50%. Hyperoxia is potentially harmful, with sequelae such as absorption atelectasis, lung injury and oxidative stress. It remains unclear what the optimal oxygenation target should be that balances the risks of hypoxia and hyperoxia.24,25
Identified risk factors of mortality were compared against each other with multivariate modelling (in order to adjust for confounders). Of these risk factors, the APACHE II score was found to be the most statistically significant predictor of mortality.
Inter-rater reliability was found to be 0.604, highlighting the inaccuracy in clinicians’ recording of APACHE II scores. 26 For reference, an ICC of >0.75 is good, whilst >0.95 is excellent. 26 If using a mortality scoring system, accuracy is imperative to avoid overestimating mortality risk. The APACHE score is used to guide critical clinical decisions, so accuracy is important and a ‘good’ agreement should be a minimum standard.
We propose two major reasons for the low level of agreement; clinicians aren’t aware that APACHE II requires the worst variables within 24 hours of admission to be recorded, (and suggest further education should be done in this regard) and that its subject to human error. We suggest implementation of an electronic record system to mitigate against this – with a built in formula to calculate the APACHE II. As the APACHE II plays a critical role in guiding ICU admission decisions, especially under conditions of increased demand, inaccurate or inconsistent documentation could result in the exclusion of eligible patients, by erroneously overestimating mortality. Likewise, mortality could also be under estimated resulting in inappropriate admission of patients. Given the complexity of the APACHE II score and its reliance on multiple variables, a simplified, context-specific tool that incorporates key predictors such as intubation status and MOI (e.g. community assault) may improve usability and accuracy. Reducing cognitive load and time required for calculation could enhance clinician adherence and support more reliable risk stratification.
There were also a few unexpected findings. The HIV positive rate was seemingly low at 7.5% (n = 22). Due to the large cohort of unknown HIV statuses (n = 178, 62.7%), we were unable to define the actual rate. In our institution, HIV status is routinely tested as part of the admission protocol, and the large amount of unknown statuses reflects poor adherence to hospital protocol. Length of hospital stay before ICU admission was not found to be a significant risk factor albeit there is evidence that delayed admission to ICU impacts mortality in critically ill patients. 27 Certain MOI's have been associated with higher mortality, such as GSWs to the chest and torso and blunt trauma.5,23,28 Our study couldn’t corroborate this, which could be due to the study's retrospective nature and sample size.
We found a high incidence of AKI, consistent with international and local data.29,30 However, the majority of the population didn’t have any preceding organ failure (n = 283, 99.6%). The reasons for this may be multifactorial. The majority were young patients (median age 35 years) in which one would not expect a high incidence of preceding organ failure and comorbidities. Current evidence suggests that a variety of co-morbidities contribute towards mortality in the trauma population; 31 however, we were unable to establish any relationship due to the low number of events limiting statistical power.
Strengths and limitations
Strengths
Our study provides a comprehensive dataset including demographics, physiological parameters and detailed trauma patterns and may aid in hypothesis generation. It also provides useful baseline characteristics which can be used for later comparison against future studies and can serve as a quality benchmark for care across different ICUs. It also represents the only study of its kind examining the use of the APACHE II in polytrauma patients in the South African ICU setting.
Limitations
Data collection was dependent on the quality and accuracy of hospital records and preexisting data may be subject to multiple biases. We also acknowledge general limitations of retrospective studies, i.e. selection bias due to convenience method of sampling, and inability to determine causation – only association. Other possible limitations include study sample size and data set. As this is a contextual descriptive study in a single centre, the results may not be generalizable to similar ICU's.
Conclusion
The APACHE II is an appropriate prognostication tool to use in polytrauma patients to accurately describe the risk of death in ICU. Patients with scores above 20 were at highest risk of mortality. Although the presence of intubation and community assault were significant risk factors of mortality, they are not included in the APACHE II score, highlighting the need to consider additional risk factors in the trauma population. Finally, clinician-recorded scores aren’t accurate and cannot be relied on.
Supplemental Material
sj-docx-1-tra-10.1177_14604086261435148 - Supplemental material for Evaluation of the APACHE II as a mortality scoring system among intensive care unit polytrauma patients at a tertiary hospital in South Africa
Supplemental material, sj-docx-1-tra-10.1177_14604086261435148 for Evaluation of the APACHE II as a mortality scoring system among intensive care unit polytrauma patients at a tertiary hospital in South Africa by Nina Zea Carelse, Simone Piovesan and Ryan Davids in Trauma
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval and informed consent
The study obtained ethics approval from Stellenbosch Health Research Ethics Committee [S24/04/092]. Approval was also obtained from the Institutional Review Board. [WC_202409_018].
Contributorship
NC researched literature, conceived the study and conducted the data collection. NC, SP, RD was involved in protocol development, gaining ethical approval and data analysis. NC wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.
Acknowledgments
Abigail Titus, biostatistician.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.