
Abstract
Objective
This study aimed to identify the risk factors for death in patients with sepsis-related myocardial injury.
Methods
A retrospective study was conducted in 158 patients with sepsis-related myocardial injury in a mixed medical intensive care unit from January 2009 to March 2020. The patients were divided into those who survived and those who died on the basis of whether they survived after 28 days. Demographic and clinical parameters were collected. Multivariate logistic regression was performed.
Results
Sixty-nine (43.7%) patients died within 28 days after admission to the intensive care unit. Multivariate logistic regression analysis showed that the oxygenation index (odds ratio [OR]: 0.979, 95% confidence interval [CI]: 0.970–0.989), acute kidney injury (OR: 4.787, 95% CI: 1.674–13.693), norepinephrine dose (OR: 1.706, 95% CI: 1.375–2.117), and abdominopelvic cavity infection (OR: 0.257, 95% CI: 0.076–0.866) were significantly associated with mortality within 28 days after admission in patients with sepsis-related myocardial injury.
Conclusions
Patients with sepsis-related myocardial injury have a high mortality rate. A high oxygenation index, occurrence of acute kidney injury, high norepinephrine dose, and occurrence of abdominopelvic cavity infection are independent risk factors for 28-day mortality in patients with sepsis-related myocardial injury.
Keywords
Introduction
Sepsis is a syndrome caused by various microorganisms and immunogenic substances. Sepsis leads to dysfunction of host immune regulation, including inflammatory factor cascade release, endothelial dysfunction, cell apoptosis, immunosuppression, and eventually, multiorgan dysfunction.1,2
Sepsis has gradually become the main cause of death in patients in the intensive care unit (ICU). An epidemiological investigation showed that approximately 40% of patients with sepsis also had different degrees of myocardial dysfunction; the mortality rate of sepsis accompanied by myocardial injury was as high as 70%. 3 Sepsis-related myocardial injury may be related to signaling pathway-mediated release of abundant inflammatory factors, pro-inflammatory/anti-inflammatory imbalance, and immune system disorders, rather than a single pathogenesis.4,5 However, the risk factors for death in patients with sepsis-related myocardial injury are not completely clear. Therefore, this study was performed to investigate the risk factors affecting the prognosis of patients with sepsis accompanied by myocardial injury.
Materials and methods
Clinical data
This retrospective analysis was performed using the clinical data of patients with sepsis-related myocardial injury who were admitted to Beijing Friendship Hospital Affiliated to Capital Medical University from January 2009 to March 2020. The study protocol was approved by the Beijing Friendship Hospital Affiliated to Capital Medical University (No. 2020-P2-068-01) and was performed in accordance with the Declaration of Helsinki. Individual informed consent was waived owing to the retrospective nature of this study.
Inclusion and exclusion criteria
The inclusion criteria were as follows: (1) diagnosis of sepsis according to the sepsis-3 definition 2 on admission to the ICU; (2) cardiac troponin I (cTnI) levels >0.04 ng/mL (detected by the PATHFAST chemiluminescence immunoassay; Beijing Friendship Hospital, Capital Medical University, Beijing, China) on admission to the ICU; 6 and (3) age ≥18 years. The exclusion criteria were as follows: patients with a history of myocardial disease, valvular heart disease, congenital heart, acute coronary syndrome, severe heart failure, cardiothoracic surgery, chest compression, defibrillation, direct current cardioversion, tumor, or autoimmune disease; and pregnant women.
Measures and grouping
Data on age, sex, medical history of basic illness, laboratory tests, and causes of sepsis infection were collected. Records on vital signs of the patients were obtained at the time of diagnosing sepsis, including mean arterial pressure, heart rate (HR), and central venous pressure. We also collected data on the oxygenation index and blood biochemical indices (leukocytes, platelets, and levels of creatinine, serum potassium ion, total cholesterol, blood glucose, N-terminal B-type natriuretic peptide, serum creatine kinase isoenzyme, procalcitonin, blood lactate, cTnI, and C-reactive protein). The oxygenation index was calculated as the partial pressure of arterial oxygen/the concentration of inspired oxygen. Blood lactate levels were measured upon ICU admission/diagnosis of sepsis (initial blood lactate value) and at 24 hours after ICU admission/diagnosis of sepsis (24-hour blood lactate value). The lactate clearance rate was calculated as follows: [(initial blood lactate value–24-hour blood lactate value)/initial blood lactate value] × 100%. The systemic infection-related sequential organ failure assessment (SOFA) score and Acute Physiology and Chronic Health Evaluation II (APACHE II) score were recorded for 24 hours after admission to the ICU. The use of mechanical ventilation, occurrence of acute kidney injury (AKI), use of continuous renal replacement therapy, and dose of norepinephrine during the ICU stay were recorded. The records of liquid intake and output volume for 7 consecutive days were obtained.
The patients were divided into the survival and nonsurvival groups on the basis of whether all-cause death occurred within 28 days after admission to the ICU.
Statistical analysis
Means and standard deviations are reported for variables that conformed to a normal distribution, and the independent-sample t test was used for comparison. Data that did not conform to a normal distribution are shown by the median (interquartile range, [25th percentile, 75th percentile). Comparison between groups was performed using the rank-sum test. Categorical data are presented as the percentage and the chi-square test was performed for comparisons. Univariate and multivariate logistic regression analyses were performed to analyze the independent risk factors associated with mortality. Variables with P < 0.1 in univariate analysis were involved in multivariate analysis, and the backward method was used to select the variables that remained in the multivariate analysis. All of the statistical tests were two sided. P values < 0.05 were considered statistically significant. IBM SPSS version 25.0 software (IBM Corp., Armonk, NY, USA) was used to perform statistical analysis.
Results
Clinical characteristics of the patients
Among the 158 patients included in the analysis, 89 were in the survival group and 69 were in the nonsurvival group. Clinical characteristics of the patients in relation to survival and nonsurvival are shown in Table 1. Overall, 57.6% of the patients were men and 42.4% were women. The age of the patients ranged from 57 to 79 years, with a mean age of 73 years. Infections in the lungs were the most common, followed by the abdominal cavity, urinary system, biliary tract, and others. Patients in the nonsurvival group had a significantly higher rate of pulmonary infection (P < 0.001), mechanical ventilation (P = 0.006), and continuous renal replacement therapy (P = 0.005), and a higher norepinephrine dose (P < 0.001) than those in the survival group. More than half of the patients had hypertension and AKI, followed by coronary atherosclerotic heart disease, diabetes, renal insufficiency, and hyperlipidemia. Notably, significantly more patients in the nonsurvival group had hypertension as the basic disease than those in the survival group (P = 0.038). The SOFA score was 7 (interquartile range [IQR]: 5–10) and 9 (IQR: 6–12) in the survival and nonsurvival groups, respectively, within 24 hours after admission to the ICU. The SOFA score was significantly higher in the nonsurvival group than in the survival group (P < 0.001) The median APACHE II score was also significantly higher in the nonsurvival group than in the survival group (30 [IQR: 22–35] vs 23 [IQR: 18–28]).
Comparison of clinical characteristics between the survival and nonsurvival groups.

Data are median (25th percentile, 75th percentile).
AKI, acute kidney injury; CRRT, continuous renal replacement therapy; CK-MB, serum creatine kinase isoenzyme; NT-proBNP, N-terminal B-type natriuretic peptide; SOFA, Sepsis-related Organ Failure Assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II.
Logistic regression analyses for identifying prognostic factors
Univariate logistic regression analyses showed that the following factors were associated with mortality within 28 days (P < 0.1): HR (P = 0.062), the oxygenation index (P = 0.016), mechanical ventilation rate (P = 0.006), continuous renal replacement therapy (P = 0.005), norepinephrine dose (P < 0.001), norepinephrine administration (P < 0.001), hypertension (P = 0.039), lung infection (P = 0.001), abdominopelvic cavity infection (P = 0.055), blood glucose levels (P = 0.028), creatinine levels (P = 0.008), serum potassium levels (P = 0.096), procalcitonin levels (P = 0.067), positive equilibrium of liquid accumulation on the third day from diagnosis as sepsis (P = 0.028), SOFA score (P = 0.003), and APACHE II score (P = 0.002) (Table 2). A multivariable regression model further showed that that the oxygenation index (odds ratio [OR]: 0.979, 95% confidence interval [CI]: 0.97–0.989; P < 0.001), AKI (OR: 4.787, 95% CI: 1.674–13.693; P = 0.003), norepinephrine dose (OR: 1.706, 95% CI: 1.375–2.117; P < 0.001), and abdominopelvic cavity infection (OR: 0.257, 95% CI: 0.076–0.866; P = 0.028) were independent factors for mortality within 28 days after admission in patients with sepsis-related myocardial injury.
Univariate and multivariate logistic regression analyses of prognostic risk factors in patients with sepsis-related myocardial injury.
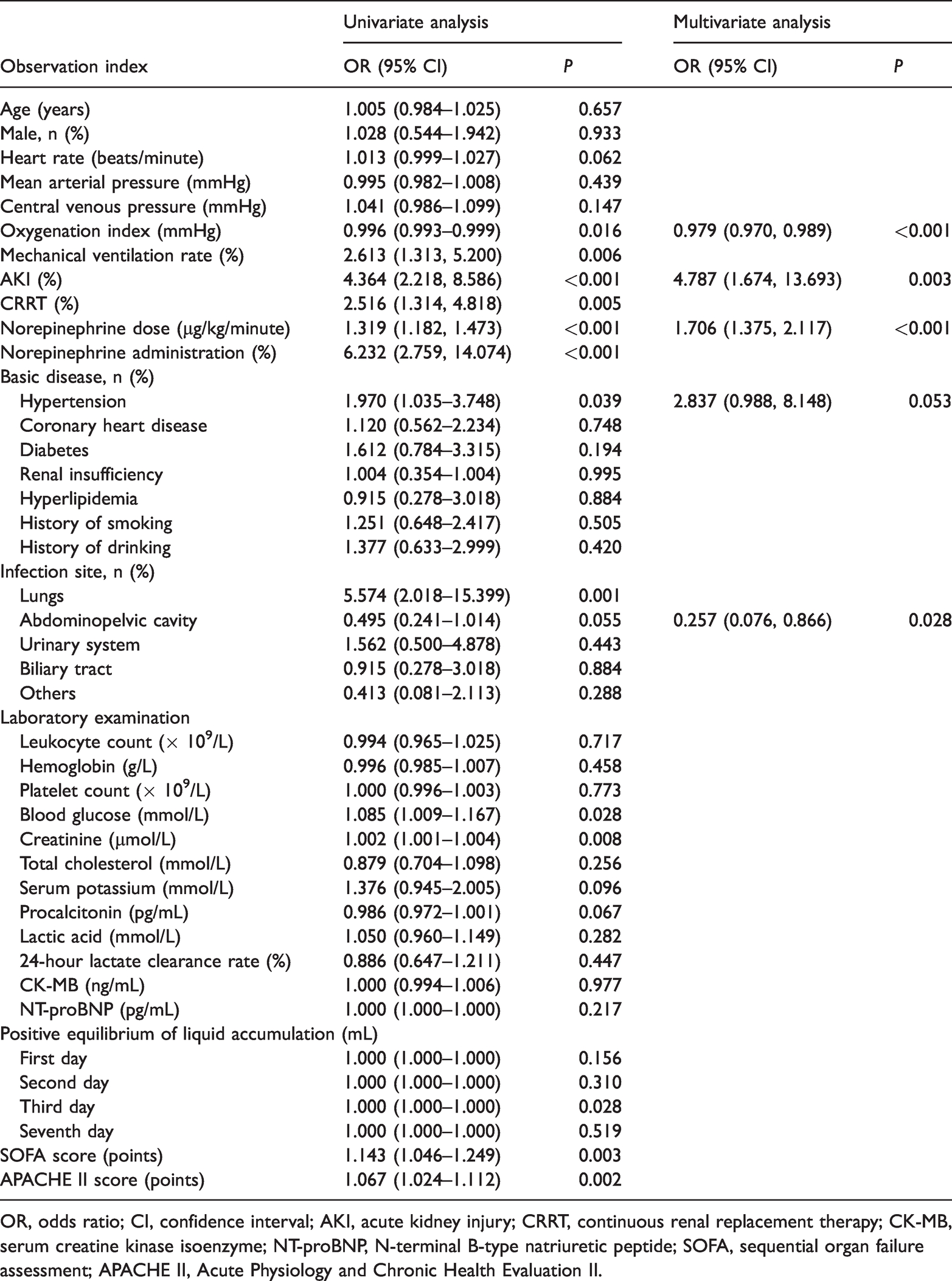
OR, odds ratio; CI, confidence interval; AKI, acute kidney injury; CRRT, continuous renal replacement therapy; CK-MB, serum creatine kinase isoenzyme; NT-proBNP, N-terminal B-type natriuretic peptide; SOFA, sequential organ failure assessment; APACHE II, Acute Physiology and Chronic Health Evaluation II.
Discussion
Sepsis can cause myocardial injury. Despite many studies on the detailed pathogenesis of sepsis, its mechanism is still not fully explained. Myocardial injury in sepsis may be related to hemodynamic changes, changes in myocardial cell metabolism, inflammatory pathway activation, myocardial cell apoptosis, and autonomic nervous dysfunction, 7 leading to myocardial dysfunction. In 1984, Parker and colleagues 8 were the first to find that myocardial dysfunction occurred in patients with sepsis, which was clinically called septic cardiomyopathy. Myocardial injury is sepsis can present as different types of cardiac dysfunction, such as left ventricular diastolic dysfunction, left ventricular systolic dysfunction, and right ventricular dysfunction. Different types of cardiac dysfunction coexist, which significantly increase the risk of death in patients with sepsis. 9 Among 158 patients with sepsis and myocardial injury included in this study, 69 patients died within 28 days after being admitted to the ICU, with a mortality rate of 43.67%. This finding is similar to that in a study by Frencken et al. 10 who showed a high mortality rate in patients with sepsis-related myocardial injury.
The APACHE II score reflects the severity of disease in critical patients. This score is used to evaluate the condition and predict the prognosis of the patients. The APACHE II score correlates with mortality in critical patients.11,12 In the present study, univariate and multivariate regression analyses showed that a higher APACHE II score was not a risk factor of death in patients with sepsis and myocardial injury. Sepsis-related myocardial injury is not only limited to heart tissue, but also affects systemic hemodynamics and has fluid resuscitation effects, 13 which significantly affect the short-term and long-term prognosis of patients. 10
Pulmonary infection, possibly due to a high rate of mechanical ventilation, 14 is the most common and major cause of sepsis in patients in the ICU. Caraballo et al. 15 showed a significant correlation between pulmonary infection and hospital mortality in patients with sepsis (OR: 3.4, 95% CI: 2.2–5.5). Similar results were also obtained in the present study, indicating that pulmonary infections might help predict survival of patients with sepsis. In patients with sepsis, the inflammatory response mediates myocardial inhibition, overactivation of nervous–humoral regulation, and changes in molecular and gene regulation, contributing to inhibition of myocardial function.6,7 Not only pulmonary hypertension, but also right heart failure due to overload of ventricular pressure caused by pulmonary hypertension, were found in the Staphylococcus aureus pneumonia rat model. 16 Cardoso et al. 17 reported that the mortality rate in patients with infection and cardiac insufficiency was higher than that in patients with infection alone (21.5% vs 17.6%, P < 0.05). Therefore, patients with sepsis and pulmonary infection may also have pulmonary hypertension, which increases the cardiac load and aggravates myocardial injury, thus leading to a higher risk of death.
Acute renal injury is a common clinical syndrome, which refers to a rapid decline in renal function in a short period owing to various reasons. Acute renal injury manifests as an increase in serum creatinine levels or oliguria. For patients with sepsis, the kidney is not only the organ involved, but may also be the cause of progression of disease. Studies have shown that acute renal injury significantly increases the risk of death in ICU patients, especially in those who require continuous bedside renal replacement therapy.18,19 Another study showed that patients with cardiogenic shock and AKI had a poorer prognosis, longer hospitalization time, and higher cost compared with patients with cardiogenic shock without AKI. 20 Some studies showed that acute renal injury was closely related to short-term and long-term all-cause mortality in patients with acute myocardial infarction.21,22 In our study, after adjusting for confounding factors, high levels of creatinine, which reflect kidney function, were a significant predictive factor for the prognosis of myocardial injury in patients with sepsis. Further studies should examine factors related to sepsis causing systemic organ injury and accelerated deterioration of organ function under an interaction of the heart and the kidney.
This study has some limitations. First, our study was a single-center, retrospective study with a small sample size, which might have resulted in selection bias. Second, 60-day or 90-day long-term follow-up data were missing in the study. Therefore, evaluating the long-term effect of occurrence of pulmonary infections, high creatinine levels, and a high APACHE II score for predicting mortality is important in the future. Furthermore, the results of this study need to be verified through multicenter, large-sample, randomized, controlled trials.
Sepsis with myocardial injury rapidly progresses with high mortality. The occurrence of pulmonary infections, high creatinine levels, and a high APACHE II score can predict high 28-day mortality. Clinicians in the ICU should pay great attention to these factors.