
Abstract
Introduction
In recent years, injury insurers in Australia have introduced compensation cover for services delivered via telehealth. The aim of this study was to investigate the uptake of telehealth services by people recovering from road trauma in Victoria, Australia, and the characteristics of participants accessing these services.
Methods
All Victorian State Trauma Registry and Victorian Orthopaedic Trauma Outcomes Registry cases, aged ≥16 years, who sustained transport-related injury from March to August 2020, and were linked with the Transport Accident Commission claims dataset, were included in this registry-based cohort study. The primary outcome was the uptake of services accessed in-person and via telehealth.
Results
Within 12 months of injury, 413 participants accessed 93,035 services, with 1432 of these via telehealth (1.5%). Seventy-five percent of family counselling, 26% of psychology and 7% of medical consultations were accessed via telehealth. For telehealth users, a greater proportion had worked/studied prior to injury, met major trauma criteria, and were discharged to inpatient rehabilitation, compared to non-users. For participants with no telehealth use, a greater proportion were discharged home, and were classified as ‘rapid recovery’ clients.
Conclusions
While telehealth uptake was low during the study period, it was accessed by people with more severe injuries. There was also greater telehealth uptake during some of Victoria's strictest COVID-19 lockdowns. Telehealth may continue to be an appealing option for medical and psychological services into the future, and may assist with return to work following transport injury.
Keywords
Introduction
The COVID-19 pandemic led to a rapid policy shift regarding the provision of services via telehealth for many health insurers and injury compensation schemes. To ensure continuity of care for their clients, these organisations were compelled to quickly introduce and/or extend telehealth billing codes. 7 Research on telehealth also rapidly expanded during and after the pandemic.7–9 However, to date, there has been little research on telehealth access and uptake specifically conducted with people recovering from road trauma. 6
In Victoria, Australia's second most populous state, the Transport Accident Commission (TAC), Victoria's ‘no-fault’ insurance scheme for people with transport injuries, 10 introduced telehealth billing codes at the start of the COVID-19 pandemic. This policy change enabled the current research, which aimed to investigate (i) the uptake of telehealth services by people recovering from road trauma in Victoria, Australia and (ii) the characteristics of participants accessing services via telehealth.
Methods
Data sources
The registry-based cohort study used linked data from the Victorian State Trauma Registry (VSTR), the Victorian Orthopaedic Trauma Outcomes Registry (VOTOR) and the TAC claims dataset. The study was approved by the Monash University Human Research Ethics Committee (project ID 30416) and is reported according to the STrengthening the Reporting of OBservational studies in Epidemiology checklist. 11
The VSTR is a population-based registry that includes all major trauma patients from all trauma-receiving hospitals in the state of Victoria, Australia. 12 Major trauma is defined as any of the following criteria being met: (i) death after injury; (ii) an Injury Severity Score (ISS) > 12; (iii) admission to an intensive care unit (ICU) > 24 h and requiring mechanical ventilation for at least part of the ICU stay; or (iv) urgent surgery (within 24 h of injury).
The VOTOR is a sentinel site registry collecting data from four hospitals in Victoria; two adult major trauma services, one metropolitan trauma service, and one regional trauma service. 13 The VOTOR captures data on all adult (≥16 years) patients with an emergency admission (>24 h) to the participating hospital for an orthopaedic injury.
The TAC provides people with transport-related injury in Victoria access to statutory benefits for a variety of services, including healthcare and income replacement, regardless of fault. 14 TAC claims data are collected to support claims management processes and improve understanding of healthcare utilisation, costs and outcomes of transport related injury cases. TAC claims data are routinely provided to VSTR and VOTOR for the purposes of research.
Participants and recruitment
All VSTR and VOTOR cases, aged ≥16 years, who sustained their injury via a transport-related event between 1 March 2020 and 31 August 2020, were included. This timeframe was chosen to capture the period after the introduction of TAC telehealth billing codes (March 2020). Transport-related events included motor vehicle, motorcycle, bicycle, pedestrian and other transport incidents. Any VSTR or VOTOR cases unable to be definitively linked within the TAC claims database were excluded. The VSTR and VOTOR use an opt-out process for inclusion. Any individual who opts out of the registry is completely removed, with no details retained, and therefore cannot be included in any analysis or research. Clients of the TAC agree to the TAC collecting data related to their claim, and this includes acknowledgement that the data will be used for research purposes.
Data collection
Data linkage of VSTR/VOTOR data with TAC claims data was performed by the TAC. Demographics, injury event details, diagnoses, in-hospital outcomes and 12-month survival rates were extracted from the VSTR and VOTOR for this study. Claims data were made available up to 12 months following the date of initial injury; that is, claims data were extracted up to 31 August 2021. Claims data included all services paid for by the TAC for all included clients, described according to the service date, type and cost of service, and whether the service was delivered via telehealth. The TAC division for each client was also provided (Rapid Recovery, Supported Recovery, and Independence). Rapid recovery is a division for clients with low healthcare and support needs who usually recover within six months. Supported recovery is a division for clients with more complex needs, such as persistent pain or mental health conditions. Independence is a division for clients who have sustained significant life-altering injuries, such as severe traumatic brain injury or spinal cord injury, who require multiple supports and long-term compensation.
Data analysis
To determine the uptake of telehealth services, the total number of services (i.e., telehealth and in-person consultations) per month, from the period of March 2020 to August 2021, were summarised as frequencies and percentages, and plotted, relative to the month of service access. The utilisation of telehealth across a variety of service types, including allied health or medical services, up to 12 months post-injury, was presented as frequencies and percentages.
Participants were categorised according to whether they had any telehealth use, defined as using at least one telehealth service within 12 months of injury, or no-use of telehealth within 12-months of injury. To compare differences in baseline characteristics between groups, continuous variables were expressed as means (standard deviation) or medians (interquartile range (IQR)) where relevant, while categorical variables were expressed as frequencies (percentages). Chi-square tests for categorical variables, and univariable linear regression modelling for continuous variables, were used to explore differences in participant characteristics between telehealth users and non-users. Where appropriate, generalised linear regression modelling with a gamma distribution and log link was used to overcome skewness associated with variables. 15 Statistical significance was indicated with a two-sided p-value <.05. All statistical analyses were completed in STATA version 17 (StataCorp, College Station, Texas).
Results
Participants
Of the 426 VSTR/VOTOR cases with a date of injury between 1 March 2020 and 31 August 2020, 414 survived to hospital discharge and 413 accessed at least one service (i.e. one consultation) within 12 months of injury (Figure 1). The 12-month survival of participants was 99% for telehealth users, and 97% for the telehealth non-users (Figure 1).
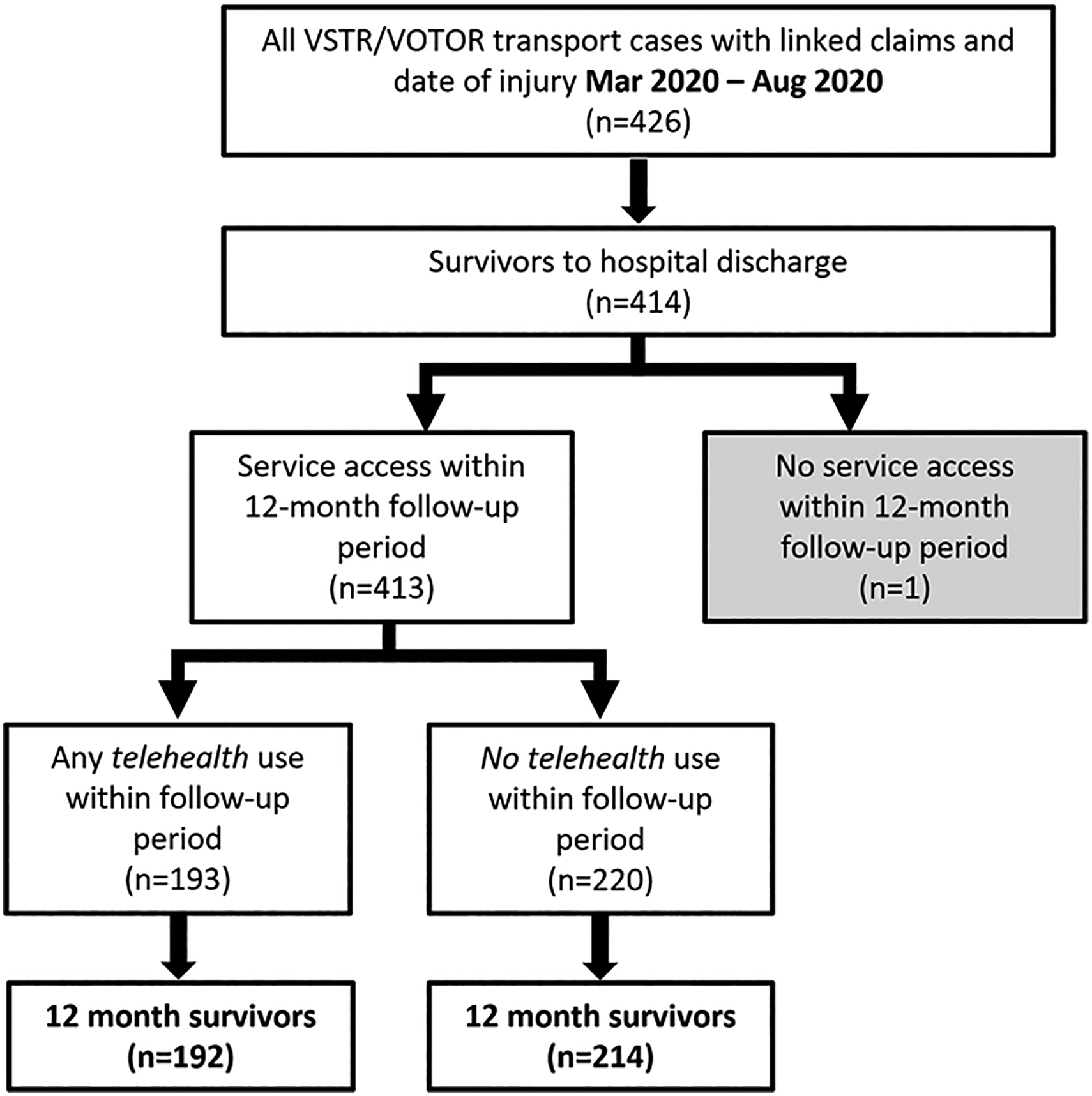
Participant flow chart. VSTR, Victorian State Trauma Registry; VOTOR, Victorian Orthopaedic Trauma Outcomes Registry.
Telehealth uptake
Within 12 months of injury, 413 participants accessed a total of 93,035 services, with 1432 of these accessed via telehealth (1.5%). Figure 2 presents the percentage of in-person and telehealth services, according to the month of service access. The highest proportion of service access via telehealth was in September 2020 (5.2% of all services).
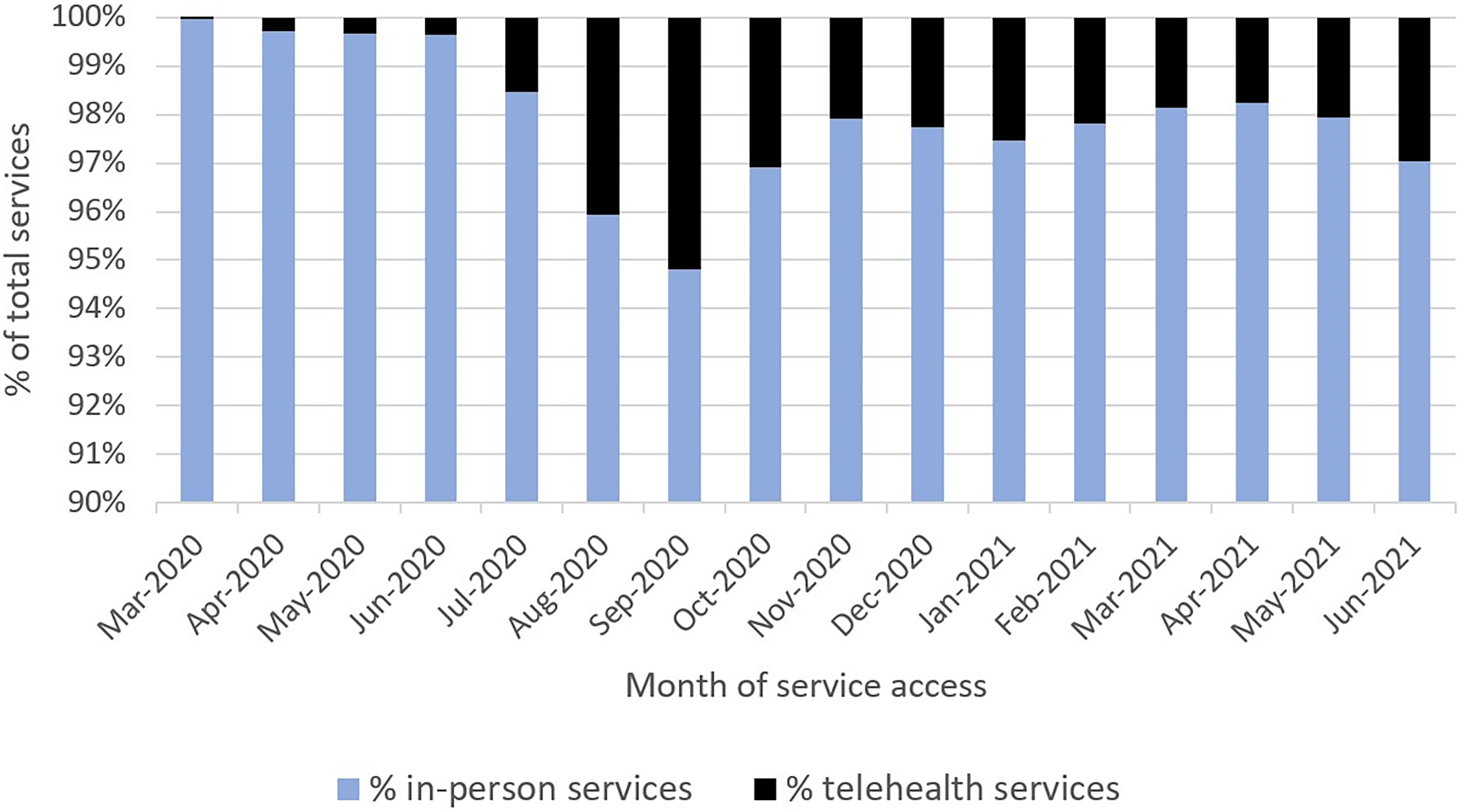
Percentage of in-person and telehealth services accessed by month.
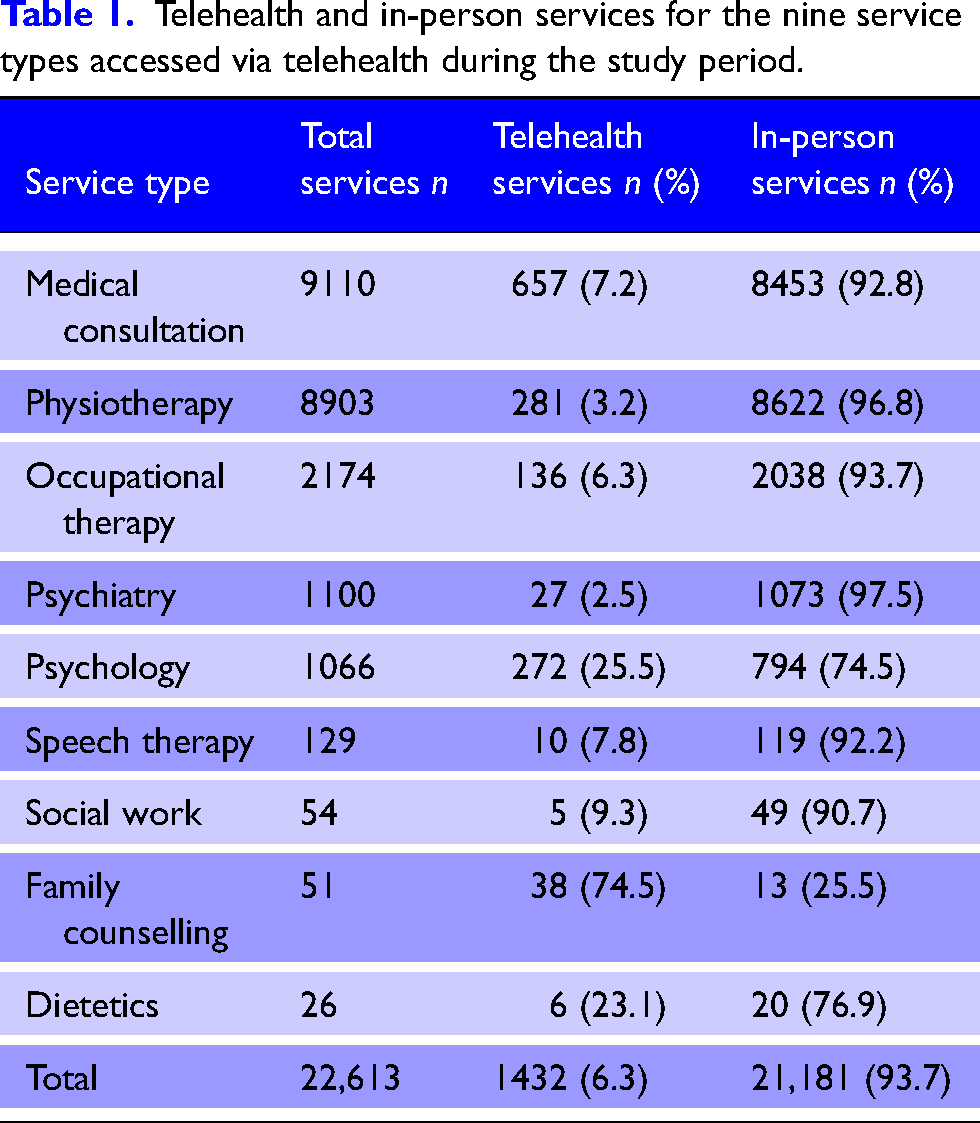
Overall, participants accessed nine service types via telehealth within the first 12 months of injury (Table 1). For these nine service types, 6.3% of all consultations were via telehealth. In total, 75% of family counselling, 26% of psychology and 7% of medical consultations were accessed via telehealth.
Telehealth and in-person services for the nine service types accessed via telehealth during the study period.
Participants with any telehealth use within 12 months of injury (n = 192) used a median (IQR) of 4 (1 to 10) telehealth and 248 (117 to 446) non-telehealth services, and those with no telehealth use within 12 months of injury (n = 214) used a median of 69 (40 to 135) non-telehealth services (Table 2).
Distribution of telehealth and in-person service access for telehealth users and non-users (n = 406).
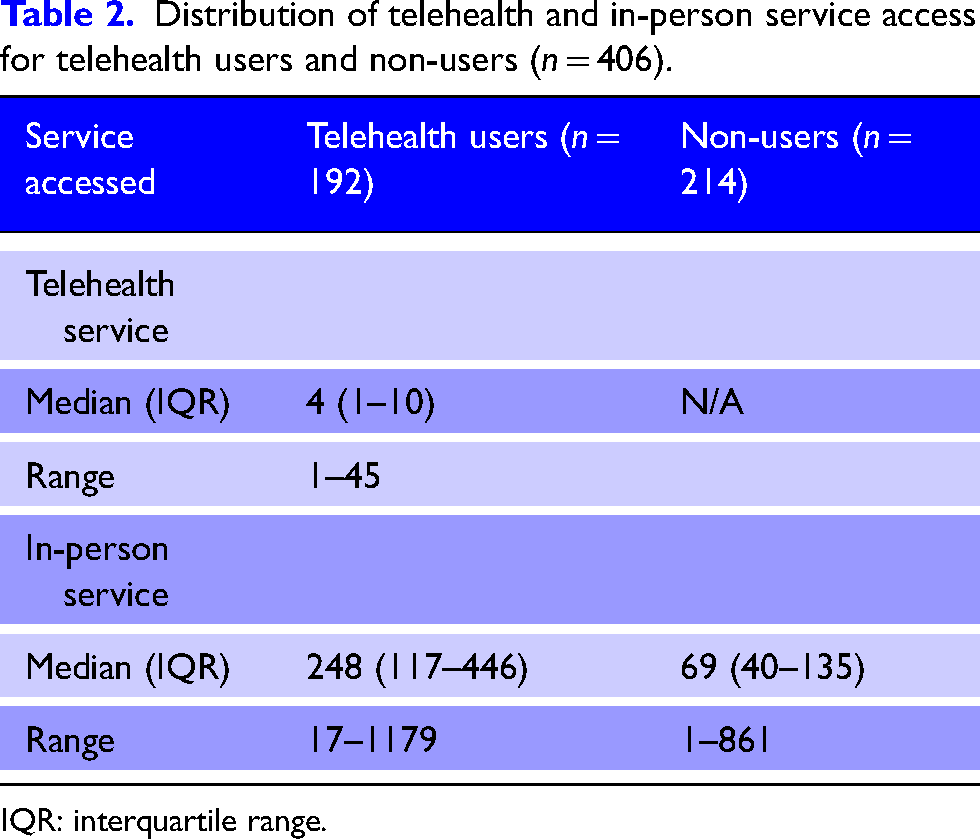
IQR: interquartile range.
Participant characteristics according to telehealth access
The characteristics of participants, according to telehealth use, are presented in Table 3. There were notable associations between telehealth use and certain characteristics. For clients with any telehealth use, a higher proportion had worked/studied prior to injury (p < .05), met VSTR (major trauma) criteria (p < .05), had head/other injuries and chest/abdominal/other injuries (p < .01), were discharged to inpatient rehabilitation (p < .001) and were classified as supported recovery or independence (p < .001), compared to clients with no telehealth use. Clients who used telehealth also had a higher average ISS (p < .001), ICU length of stay (p < .01) and hospital length of stay (p < .01), than clients with no telehealth use. For participants with no telehealth use, a higher proportion experienced multitrauma/other injury, were discharged home, and were classified as ‘rapid recovery’ compared to participants who used telehealth. There was no association between telehealth use and age group, sex, speaking a language other than English, living in regional or remote areas, or level of socio-economic (dis)advantage.
Characteristics of telehealth users and non-users (who survived to 12 months post-injury, n = 406).
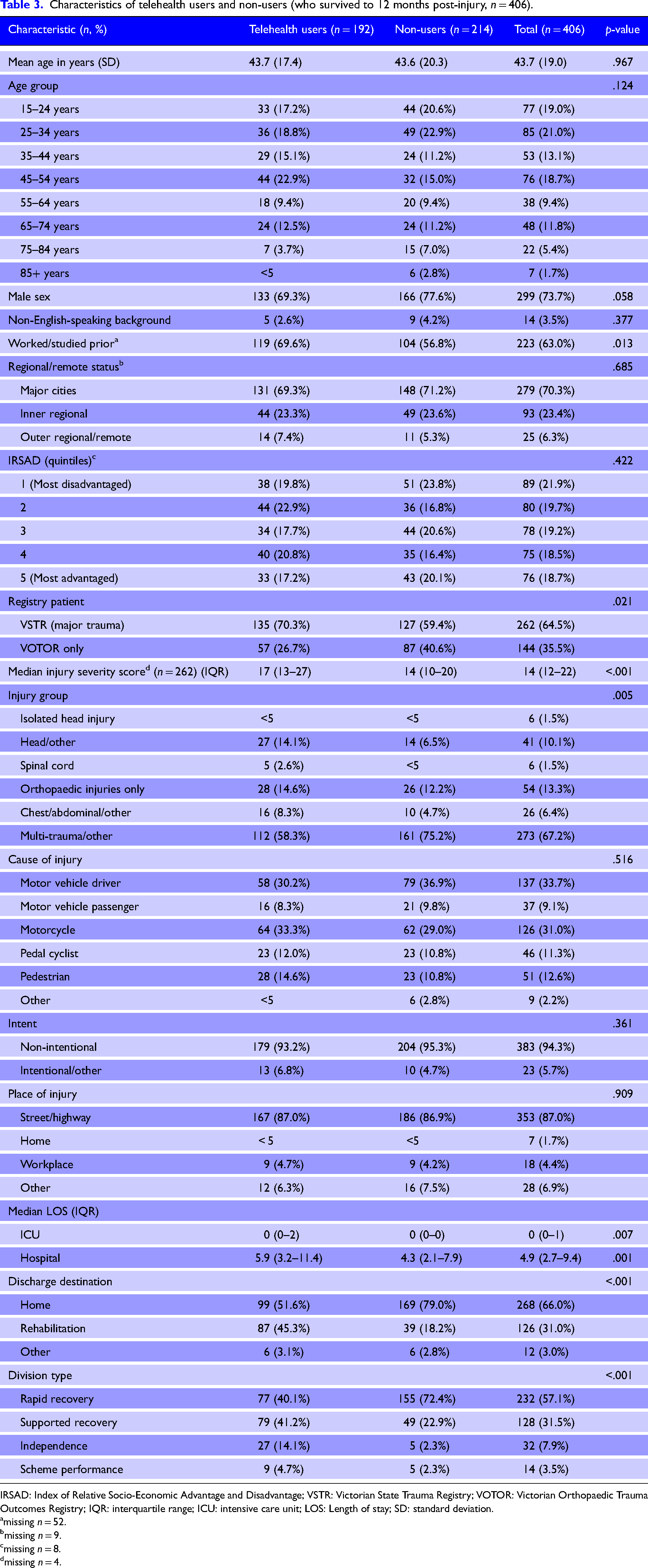
IRSAD: Index of Relative Socio-Economic Advantage and Disadvantage; VSTR: Victorian State Trauma Registry; VOTOR: Victorian Orthopaedic Trauma Outcomes Registry; IQR: interquartile range; ICU: intensive care unit; LOS: Length of stay; SD: standard deviation.
missing n = 52.
missing n = 9.
missing n = 8.
missing n = 4.
Discussion
Telehealth billing codes were introduced by Victoria's TAC in March 2020, in response to the COVID-19 pandemic. 10 This new mode of service delivery within the TAC enabled an evaluation of the uptake of telehealth services by people recovering from road trauma and the characteristics of participants according to whether or not they accessed services via telehealth. Key findings were that, while telehealth uptake was low during the study period, it was accessed by people with more severe injuries. There was also greater telehealth uptake during some of Victoria's strictest COVID-19 lockdown periods (i.e. September 2020).
The low uptake of service use via telehealth during the study period suggests that participants continued to mainly access health care services in-person. This was an unexpected finding, given the restrictions in place in Victoria at the time which stipulated that health care providers could only see patients in-person if they assessed the patient to be at risk of significant change or deterioration in functional independence, necessitating escalation of care. 16 It is possible that, because of the severity of injuries in this cohort, in-person services were still deemed necessary to avoid functional deterioration throughout the pandemic.
Previous research has also indicated that individuals with greater physical and cognitive impairments, such as those included in this study, can be hard to assess and treat via telehealth, owing to reduced communication capacity, lower digital literacy, the need for support to set up and use telehealth, and safety concerns.17,18 Therefore, telehealth uptake may have been higher in a less seriously injured cohort. The minimal uptake of telehealth in this cohort may have also resulted from restricting the study period to the first 12 months of injury. In previous research, new patients were reported to be harder to assess and treat via telehealth compared to long-standing patients where there was already established rapport with the treating clinician. 9
There were some notable differences in the types of services delivered in-person compared to via telehealth. Out of all psychology consultations during the study period, over a quarter were accessed via telehealth, compared to only 3% of physiotherapy services. These findings are supported by previous research, which reported that telehealth was feasible and effective for ‘talking therapies’, including psychology, whereas this mode of service delivery was more challenging for conducting comprehensive equipment, and other physical, assessments and treatments.8,19 There were also a high number of medical consultations accessed via telehealth which is also supported by previous qualitative research with this cohort, where telehealth was reported to work well for medical appointments, especially quick reviews, referrals, and prescription renewals. 19
In comparing the characteristics of telehealth users and non-users, there were some notable differences. Telehealth users were the most severely injured group and also accessed a higher median number of services overall during the study period, compared to telehealth non-users. Therefore, rather than preferring telehealth to in-person services, telehealth users may have had a greater need for healthcare services, in general, than clients who did not use telehealth.
Telehealth users had also more commonly worked or studied prior to injury than non-users. Given these factors, and consistent with qualitative findings, telehealth users may have had additional work responsibilities, making telehealth a more convenient option than in-person appointments.6,19 Thus, provision of services via telehealth may assist with return to work following transport injury as patients may need less time off work to attend medical appointments. In addition, given their work/study status, it is possible that telehealth users were more digitally or health literate and therefore, more willing and able to engage with services via telehealth. Despite telehealth access reportedly being influenced by language proficiency, geographic factors and digital literacy,2,18,20 we found no differences between groups based on having a non-English-speaking background, living in regional or remote areas or level of socio-economic (dis)advantage. However, case numbers were small across groups and, with a larger cohort, differences in these characteristics may have been observed.
To our knowledge, this is the largest study of telehealth uptake in a sample of people recovering from road trauma, and includes a population-level, representative sample of this cohort. However, there are a number of limitations in the current study that are important to consider when interpreting the findings. Firstly, while the follow-up period was standardised across participants by restricting analysis to the first 12 months post-injury, it was not possible to determine participants’ date of discharge from inpatient care (including rehabilitation). Therefore, some participants may have been inpatients during part of their 12-month follow-up period, and not receiving services in the community during this time, thus limiting the number of telehealth services accessed. In addition, the primary analysis cohort was restricted to people with a date of injury from March to August 2020, during a period of COVID-19 lockdown. Therefore, findings are not necessarily generalisable to periods beyond this timeframe. However, there is recent evidence to suggest that post-pandemic, telehealth continues to be widely used, particularly in primary care settings.21,22 Patients have reported continued benefit of using telehealth since the pandemic for certain types of services, such as reviews and referrals. 19 Furthermore, in many countries, including Australia, changes to compensation and public healthcare funding schemes for telehealth services have been maintained. 23 It can therefore be surmised that the COVID-19 pandemic acted as the catalyst for a permanent shift towards improved provision and uptake of telehealth worldwide, a change which has long been called-for. 24
Conclusion
Telehealth has previously been identified as a possible solution for addressing health care access issues for people recovering from serious transport injury. Telehealth uptake was relatively low for people recovering from road trauma during the COVID-19 pandemic. However, telehealth was mainly used for medical and psychological services, by people with more severe injuries, and by those who had worked/studied prior to injury. This suggests that telehealth may continue to be an appealing option for certain services into the future, and may assist with return to work following road trauma.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors disclosed receipt of the following financial support for the research, authorship, and/or publication of this article: This work was supported by the Transport Accident Commission (Grant No. T047). BG was supported by a National Health and Medical Research Council Investigator Grant (APP 2009998). The Victorian State Trauma Registry is funded by the Victorian Department of Health and the TAC. The Victorian Orthopaedic Trauma Outcomes Registry is funded by the TAC.