
Abstract
Background
The neutrophil-to-lymphocyte ratio has been proposed as a marker of systemic inflammation in major trauma patients that is associated with in-hospital mortality. However, the initial neutrophil-to-lymphocyte ratio does not appear to be predictive of in-hospital mortality. The aim of this study is to determine the discriminative ability of the neutrophil-to-lymphocyte ratio profile over 48 h as a predictor of in-hospital mortality following major trauma.
Methods
This was a case-control study involving all major trauma patients meeting the criteria for inclusion into the Alfred Health Trauma Registry who presented directly from the scene of injury over a 24-month period. Patients were then divided into two groups, cases being major trauma patients who died at hospital discharge and controls being patients who survived. We extracted data for Day 0, Day 1 and Day 2 neutrophil-to-lymphocyte ratio values for each patient. The primary outcome was mortality at hospital discharge.
Results
Data were extracted for 1689 major trauma patients, of which 72% were male, the median age was 49 years (IQR 31–68) and most (90%) patients presented after a blunt mechanism of injury. There were 165 cases that were compared to 1524 controls. Patients who died were older (p < 0.001), and had higher injury severity scores (p < 0.001) and lower revised trauma scores (p < 0.001). Analysis of response profiles demonstrated a significant difference between the trajectories of the neutrophil-to-lymphocyte ratio over time (p < 0.001).
Conclusions
The profile of neutrophil-to-lymphocyte ratio over 48 h after injury shows promise as a prognostic tool in trauma and warrants further investigation.
Background
Multiple trauma scoring systems and tools to predict outcomes are available. 1 Modern predictive tools require the potential to change clinical decisions. Furthermore, it is important that predictive tools are objective and produce reproducible observations in different settings. While trauma scoring tools are used frequently for bench-marking and quality assurance, few tools are used in clinical practice.
The neutrophil-to-lymphocyte ratio (NLR) is a marker of systemic inflammation and has recently been proposed as an outcome prediction tool in trauma.2,3 By combining both the changes in neutrophil and lymphocyte counts, NLR is elevated following trauma. In a systematic review, an association between NLR and mortality for trauma patients was observed. However, many limitations of the existing literature were highlighted within the systematic review including heterogeneity among studies, differences in trauma management between centres and varied time-points for measurement of outcomes. 4
When assessing the initial NLR (on arrival to the trauma centre) as a predictor of in-hospital mortality and intensive care unit (ICU) admission following major trauma, there was no significant correlation between initial NLR and in-hospital mortality or ICU admission. 5 Consistent with other authors, it was postulated that the inflammatory response was highly variable between patients and utilising the neutrophil and lymphocyte counts as markers of inflammation did not correlate with outcomes. 2
The resulting direction for further research was an assessment of NLR at different timepoints. It was hypothesized that NLR as a trend over 48 h from admission may be able to better predict outcomes in the major trauma cohort. Therefore, the aim of this study was to assess whether the NLR trend over 48 h from admission is an accurate predictor of outcomes following major trauma.
Methods
Setting
The Alfred Hospital is the busiest adult trauma service in Australia and admits over 1600 major trauma patients per year. Within the Victorian State Trauma Service, it is one of two adult major trauma services which provide trauma services to a state-wide population of about 6.3 million people.
Data extraction
Data were extracted from the Alfred Trauma Registry (AHTR). Missing data from the trauma registry were manually extracted from medical records by a single investigator (YQ) and incorporated into the final data set.
Population
All major trauma presentations who presented directly from the scene of injury to The Alfred between January 2018 and December 2019 were eligible for inclusion in this study. The inclusion criteria for the AHTR have been previously described and include patients with an Injury Severity Score (ISS) > 12, death after injury, admission to the ICU for more than 24 h with mechanical ventilation, partial and full thickness burns ≥ 20% total body surface area, urgent surgery within 48 h from arrivals such as craniotomy, thoracotomy, laparotomy, pelvic or spine surgery or interventional radiology. 6 The Revised Trauma Score (RTS) and shock index (SI) provided measures of baseline differences in injury severity. The RTS is a physiologic scoring system based on the initial vital signs of a patient and is made up of three categories: Glasgow Coma Scale, systolic blood pressure, and respiratory rate. 7 The SI was obtained from the ratio between heart rate and systolic blood pressure (HR/SBP). 8
Design
This was a case-control study with the population divided into two groups, with the cases being major trauma patients who died in hospital and the control group being patients who survived. The study was approved by The Alfred Hospital Human Research and Ethics Committee (Project ID 226/20).
Exposure and outcome variables
The primary exposure variable was the NLR trend over 48 h. The NLR was calculated as the neutrophil count divided by the lymphocyte count. The NLR measures were collected as discrete variables at 0, 1 and 2 days of presentation. For each time-point, the blood test results closest to 0, 24 and 48 h were extracted. The primary outcome variable was mortality at hospital discharge.
Statistical analysis
Baseline continuous variables were reported using medians and interquartile ranges (IQR). Categorical variables were represented as frequencies and percentages. The differences between the case and control groups were examined using the Mann-Whitney U-test to assess continuous variables, while the chi-square test was used to assess categorical variables. We conducted an analysis of response profiles using a mixed effects linear model. In order to test if there is a difference in the pattern of change between alive and dead patients, we were interested in if there is a difference in the change over time in patients between the two groups. More specifically, the core research question was whether the difference between groups of interest changes from one occasion to the next. 9 This corresponds to an interaction. The model used included an effect for the patient sub-group (death) and an effect of time with initial NLR being the reference group. The interaction between death and time created three interaction terms since we allowed a difference between the two groups of patients at each time point.
Since we had repeated measures data, we used patient I.D. to index independent patients. We did not include any random effects. We assumed that the residuals within a patient are related and that the covariance matrix for the residuals within a person was unstructured. We used restricted maximum likelihood for estimation. Missing data were handled by pairwise analysis. We used this method as the primary goal of this longitudinal study was to characterise the change in response over time. This statistical technique was required as the repeated measures on the same individual are usually positively correlated, and variability is often heterogeneous across measurement occasions. As such, the assumptions of linear regression are not met. 10 All statistical analysis was performed by Stata v 15.0 (College Station, TX, USA). Statistical significance was defined as p < 0.05.
Results
There were 1689 major trauma patients that presented to The Alfred Emergency and Trauma Centre and met AHTR inclusion criteria. There were 1218 (72.11%) male patients. The median age was 49, with 458 (27.12%) patients older than 65 years of age. The mechanism of injury was blunt injury in 1516 (89.76%) patients, 89 (5.27%) penetrating trauma and 59 (3.49%) burns. The median ISS was 17 with 510 (30.20%) patients having an ISS of ≥ 25.
Baseline demographic and injury characteristics for the two groups are listed in Table 1. In-hospital mortality occurred in 165 (9.77%) patients. Time to death for patients is illustrated in Supplemental Online Material 1. Patients who died were older, and had a higher ISS and lower RTS. The median NLR was different for patients that died at all three timepoints. On admission, the dead cohort had a lower median NLR when compared with the control, but by 24 and 48 h, they had significantly higher median NLR.
Baseline characteristics of major trauma patients.
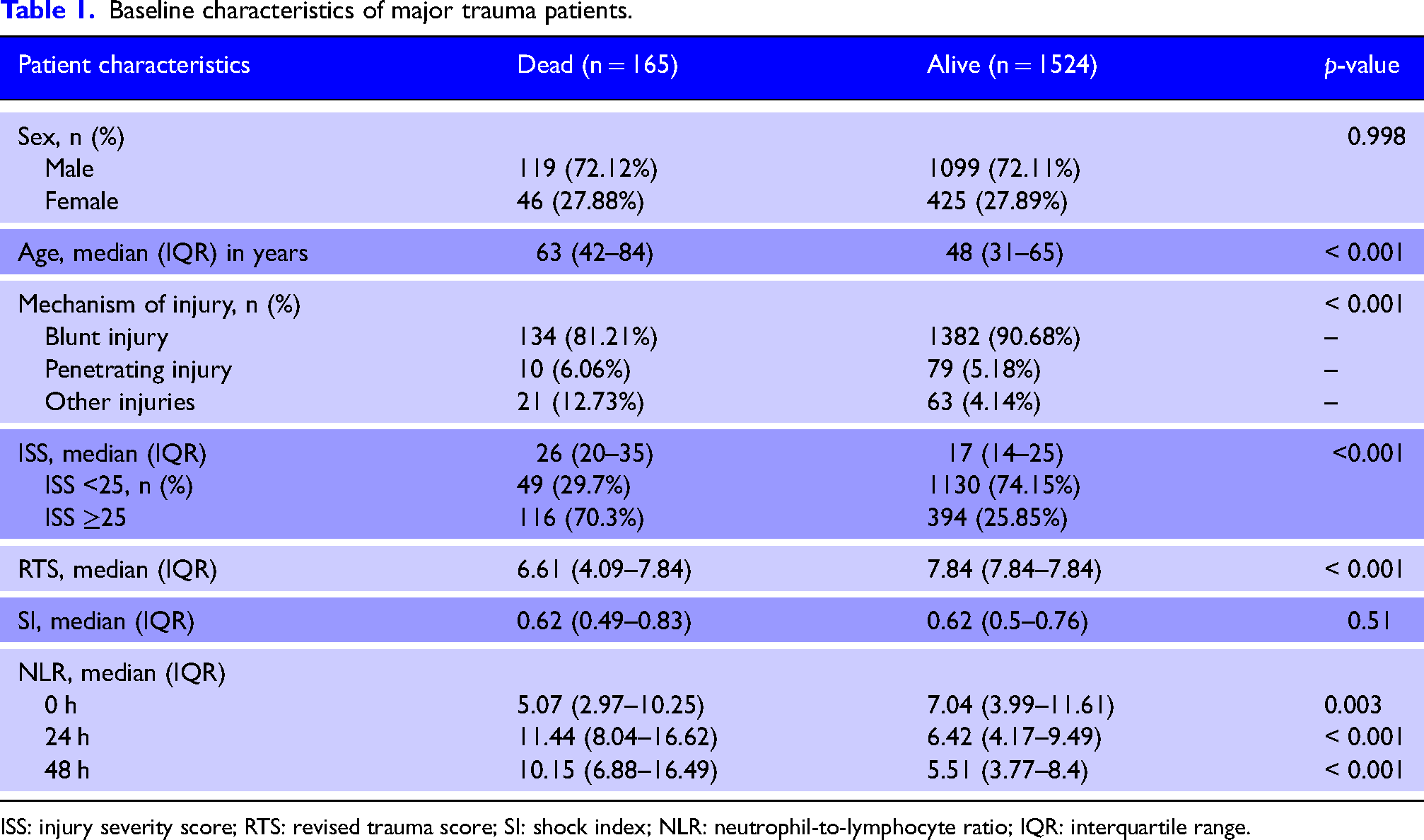
ISS: injury severity score; RTS: revised trauma score; SI: shock index; NLR: neutrophil-to-lymphocyte ratio; IQR: interquartile range.
The distribution of initial NLR is depicted in the figures below (Figures 1 to 3). Analysis of response profiles (Figure 4) demonstrated a significant difference between the trajectory of NLR over 48 h from admission between the dead and alive groups. At 24 h after injury, the regression coefficient for the interaction of death and NLR was 7.32 (95% CI: 5.64–9.01; p < 0.001). At 48 h, the regression coefficient for the interaction was 7.08 (95% CI: 5.40–8.77; p < 0.001). There was a significant difference in the NLR slope over the 48 h period. The chi2 (2-degrees of freedom) test characteristic for parallelism was 89.9 (p < 0.001).
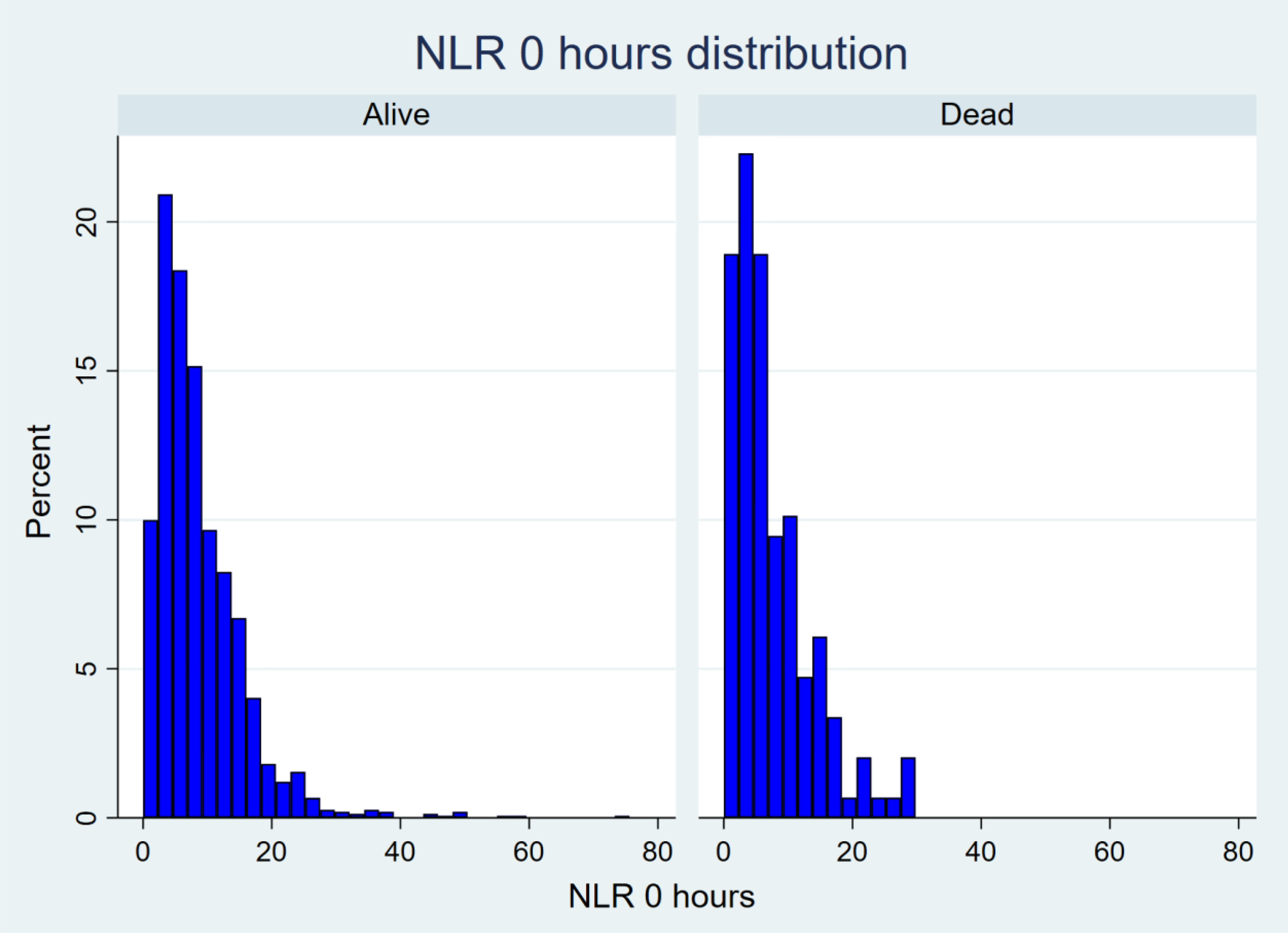
Histogram of neutrophil-to-lymphocyte ratio (NLR) distribution at 0 h.
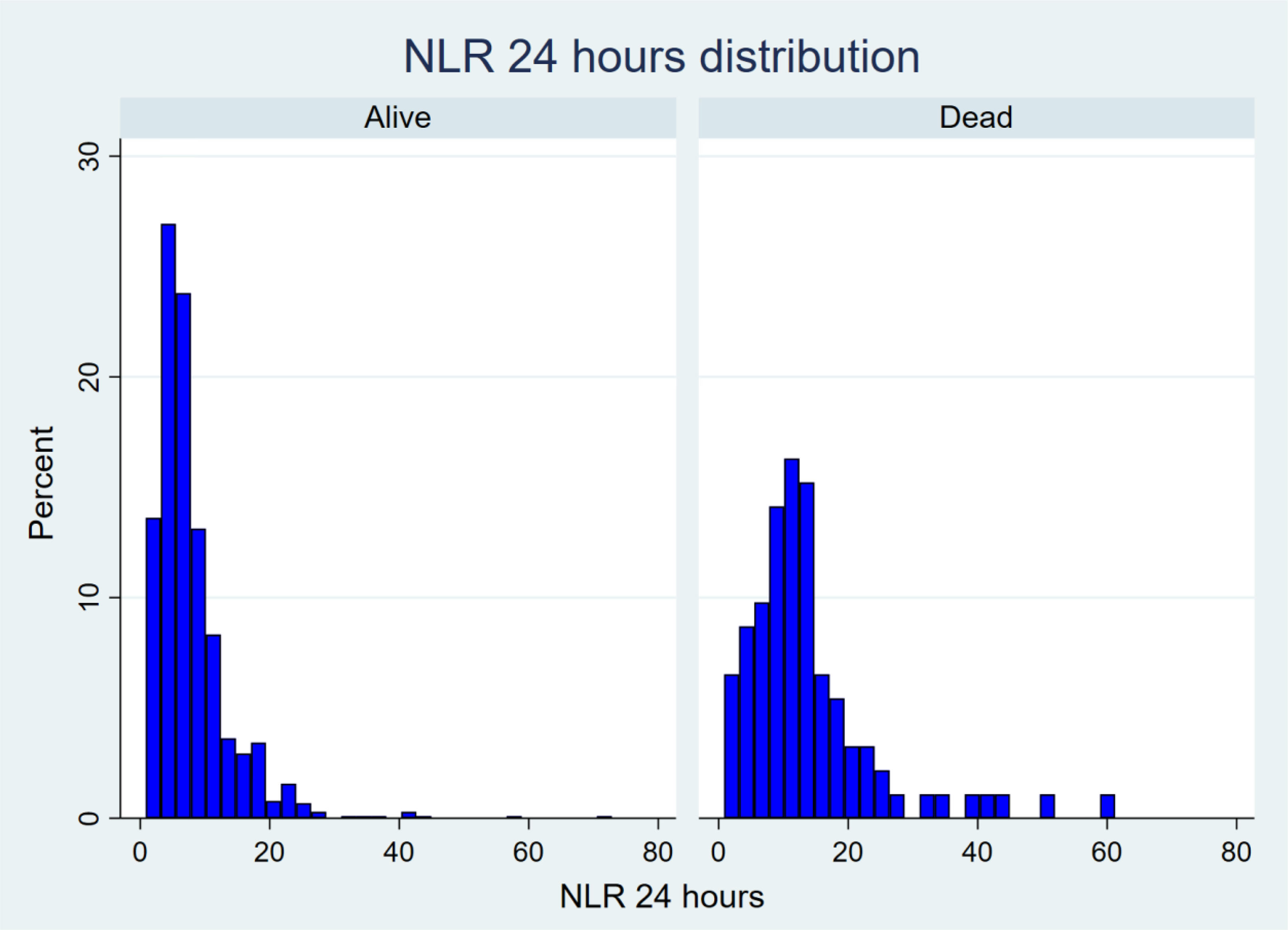
Histogram of neutrophil-to-lymphocyte ratio (NLR) distribution at 24 h.
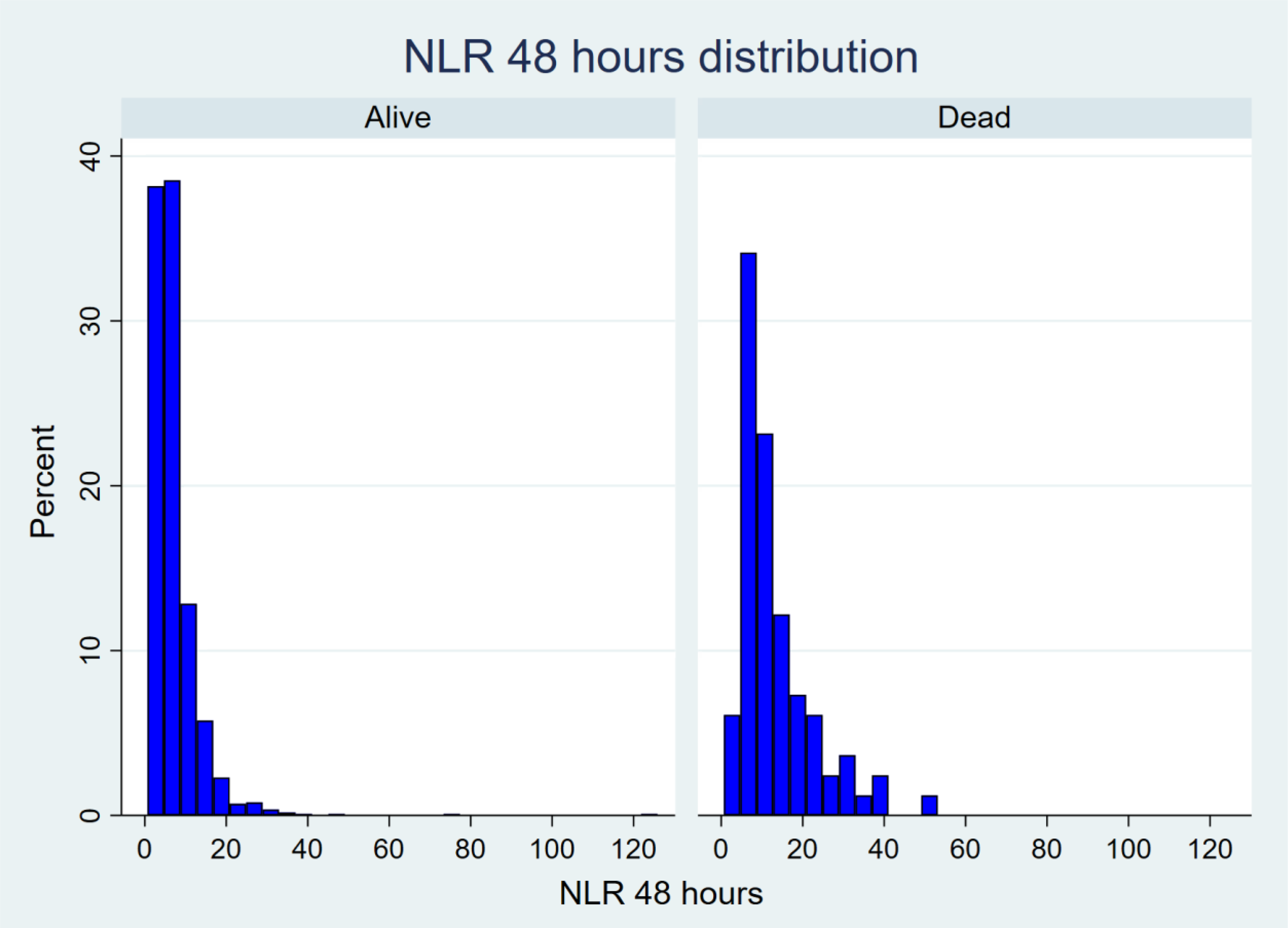
Histogram of neutrophil-to-lymphocyte ratio (NLR) distribution at 48 h.
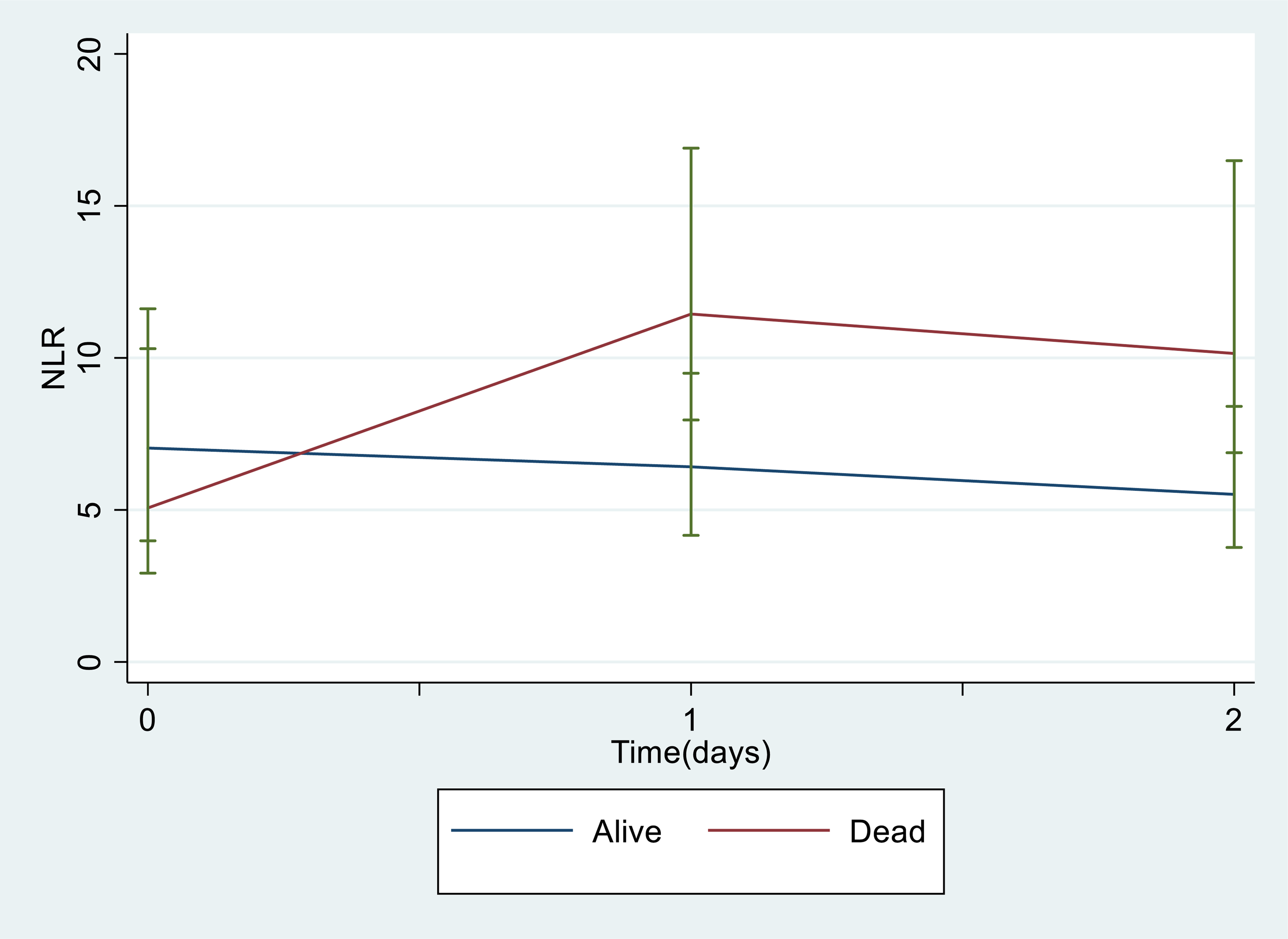
Comparison of neutrophil-to-lymphocyte ratio (NLR) trajectories over 48 h. NLR with standard errors is displayed at each time-point, sub-grouped by the patient outcome.
Discussion
In this case-control study, a difference in NLR trajectory over 48 h was observed between patients who eventually died compared with those who survived. This suggests that patients at higher risk of mortality induce a different, potentially more aggravated inflammatory response, as measured by the neutrophil and lymphocyte counts. Thus, monitoring NLR over the first 48 h from admission may be a useful tool to identify patients at high risk for in-hospital mortality.
Cases and controls were of similar sex and had similar baseline SI, but there were significant differences in all the other baseline characteristics. In-hospital mortality was associated with increased age and injury severity, summarised using the ISS and RTS. These findings are consistent with other publications reporting increased mortality in geriatric trauma and in those patients with higher injury severity.11,12 While the association of age and injury severity with hospital mortality is well known, the NLR can therefore provide a further objective measure when tracked over the first 48 h.
The findings are consistent with previous reports on the topic. Younan et al. 13 observed an increased risk of organ failure in critically ill male trauma patients with an increasing NLR trajectory over 48 h. However, Younan et al. had specifically looked at comparing an increasing versus a decreasing NLR trend and so did not account for non-linear NLR trends. The authors failed to identify a relationship between increasing NLR trend and mortality, but this was likely due to the small sample size of patients who died.
The trend of NLR may provide the prognostic ability that was not observed with the initial value and is consistent with other studies that have concluded value in NLR in the subsequent days after major trauma. Dilektasli et al. 2 observed an elevated NLR on days two and five to be associated with increased risk of mortality whereas Duchesne et al. 3 demonstrated a high NLR on days 10 to be associated with an increased risk of mortality and increased transfusion requirements. Similarly, Chae et al. 14 reported day seven NLR significantly predicted mortality, suggesting that blood-based markers can more accurately predict mortality at later stages. NLR within the first 24 h of admission, therefore, appears to be an unreliable marker but, consistent with previous literature and demonstrated in this study, as the inflammatory response progresses, the NLR becomes a more accurate marker of the body's inflammatory status. Additionally, observing the NLR trend accounts for baseline variations in white cell counts, focusing our observations on changes in NLR due to injury.
This study was limited by its retrospective study design and intrinsic selection bias by only including patients with major trauma. Our study was performed at a single centre and may not be generalisable to centres receiving lower volume or lower acuity trauma. Additionally, the large proportion of blunt trauma in our population limits generalisability to other trauma centres where there may be greater amounts of penetrating trauma. Finally, this study did not compare the NLR trends with that of other scoring systems, such as the TRISS, RTS or the ISS and could be a focus of future research. It is possible that the addition of NLR to other tools may provide more robust outcome predictions that are dynamic and responsive to management. 15 As full blood examinations are routinely performed regularly on critically injured patients, the NLR provides an objective measure of injury severity that can be easily determined. Addition of the NLR to more complex prediction tools may result in robust outcome predictions after trauma and initial resuscitation. 16
Conclusion
Major trauma patients who experienced in-hospital mortality had a different NLR trajectory over the first 48 h when compared with patients who survived. After major trauma, NLR over time may be utilised as a prognostic tool or combined with other tools for more accurate outcome prediction.
Declaration
Supplemental Material
sj-docx-1-tra-10.1177_14604086221131106 - Supplemental material for Longitudinal analysis of neutrophil-to-lymphocyte ratio over time after major trauma
Supplemental material, sj-docx-1-tra-10.1177_14604086221131106 for Longitudinal analysis of neutrophil-to-lymphocyte ratio over time after major trauma by Yunfei Qiu, Mark Fitzgerald and Biswadev Mitra in Trauma
Footnotes
Conflicting of interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article. Provenance and peer review Not commissioned, externally peer-reviewed.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
This study was approved by The Alfred Hospital Human Research and Ethics Committee (Project ID: 226/20).
Informed consent
Not applicable.
Trial registration
Not applicable.
Guarantor
BM
Contributorship
BM initiated the research question. All authors participated in ethics approval and design. YQ extracted the data. BM and YQ analysed the data. All authors participated in writing of manuscript and edits.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.