
Abstract
Introduction
Computerized tomography is an essential element of the early diagnostic stages of trauma care for hemodynamically stable patients. However, there are inherent challenges and risks associated with the intra-hospital transport of critically injured trauma patients to the radiology suite and during the scanning process itself. We examined the frequency and nature of adverse events during computerized tomography among critically injured patients.
Methods
This is a retrospective cohort study of adverse event in critically injured adult (>18 years old) trauma patients who underwent emergent computerized tomographic scan following evaluation in the trauma bay over a 22-month period who were either admitted to the intensive care unit or the operating room post computerized tomography. Data was abstracted from the hospital's trauma registry and chart review of electronic medical records. The frequency of adverse events during computerized tomography and the associated patient transport phases was recorded. Multivariable logistic regression was performed to assess the impact of adverse event on 7-day in-hospital mortality.
Results
Of the 526 critically injured trauma patients who underwent computerized tomographic scan during the study period, 17.3% (91/526) experienced one or more adverse event. The most common adverse events were hypotension n = 50 (9.5%), hypertension n = 18 (3.4%), initiation of vasopressors n = 11 (2.1%) and vomiting n = 8 (1.5%). One patient required re-intubation following endotracheal tube dislodgement and one patient required intubation following hypoxia post-sedation for agitation. Patient factors independently associated with adverse event were mechanical ventilation and blood product administration. When adjusted for injury severity score and age, patients who experienced adverse event were at increased odds of death (odds ratio: 2.2, 95% confidence interval: 1.11–4.36) compared to those who did not experience adverse event.
Conclusion
Adverse events occur frequently in critically injured patients undergoing emergent trauma computerized tomography and may significantly impact clinical outcomes. This study provides important information to guide system and process-level improvements including optimized designs of the built environment and safety-informed protocols for high-risk patients undergoing emergent trauma computerized tomography.
Introduction
Computerized tomography (CT) imaging of the hemodynamically stable trauma patient is a standard diagnostic procedure in early trauma evaluation that provides critical information to inform treatment decisions.1,2 CT is generally not recommended for hemodynamically unstable trauma patients by most guidelines, however, a patient who is hemodynamically stable initially in the trauma bay may not remain so throughout their clinical course.3,4 Fluctuations in patient condition during transport to the radiology suite and during CT scanning are potentially life-threatening and require a cautious balance of the risks of transport and benefits of CT. 5
Even in the absence of hemodynamic instability, there are inherent challenges associated with the transport and imaging of trauma patients. Many centers in North America require transport of patients to the radiology department remote from the trauma bay. 6 In transit to and within the radiology department access to resuscitation equipment is often limited. Once in the CT scanner, difficulty in escalation of care and lack of direct bedside trauma team presence increases the potential for patient deterioration and complications.
The incidence of adverse events (AE) during intrahospital transport of critically ill patients undergoing diagnostic testing or therapeutic procedures ranges from 1.7% to 79.8%.7–13 However, this range of AE captures all critically ill patients including adult medical, surgical and trauma patients. Little is known regarding the rates of AE exclusively among trauma patients during intrahospital transport for CT despite the significant risk posed during this phase of care.
The primary objective of this study was to assess the incidence and nature of AE in critically injured trauma patients being transported to radiology to undergo a CT scan. Secondary objectives included the identification of specific patient factors associated with AE and a comparison of 7 day in-hospital mortality between trauma patients who did and did not experience an AE during CT.
Methods
Study design and setting
This is a retrospective cohort study of all injured patients included in our trauma registry who underwent CT scan following evaluation in the trauma bay at St. Michael's Hospital, Toronto, Ontario Canada between 1 January 2019 to 1 November 2020. Trauma team activation occurs for patients who meet triage standards based on anatomic, physiologic, mechanism of injury (MOI) or special considerations criteria. 14 At our institution, the CT suite is located three floors above the trauma bay requiring transport via one of three service elevators. Data were abstracted from the hospital's trauma registry with supplemental information obtained from manual chart review of electronic medical records.
Participants and data collection
Using our trauma registry, critically ill patients (aged 18 years or older) who underwent CT scan following evaluation in the trauma bay were included if their post-CT destination was the intensive care unit (ICU) or the operating room (OR). Patients who were transferred to the ward, transferred to another facility (i.e. Police custody), or discharged home were excluded.
We collected patient demographics, injury severity score (ISS), MOI, initial trauma bay vitals, Glasgow Coma Scale (GCS), outcome of FAST exam (positive abdominal free fluid), and in-hospital characteristics including length of stay, disposition, and mortality from the trauma registry. In addition, we collected variables including risk factors potentially associated with AE including serum lactate, base deficit, transfusion requirement, activation of massive hemorrhage protocol or mechanical ventilation. Given the lack of studies that focus exclusively on transport for diagnostic procedures we defined AE using published literature of critically ill patients undergoing interfacility transport.7,8,10–12,13 Physiological AEs included acute deterioration in Level of Consciousness (LOC) (GCS ≤ 8 or fall ≥3 or new onset of seizure activity), vomiting/aspiration, a new arrhythmia, cardiac arrest, hypotension (SBP ≤ 90 or fall by ≥20 mmHg), hypertension (SBP ≥ 190 mmHg), bradycardia (HR < 50) or tachycardia (HR > 150) or hypoxia (SpO2 < 90%). Equipment AE included loss of parenteral or central access, dislodgement of endotracheal tube (ETT), chest tube or other significant equipment failures. Interventions included the need for intubation, initiation of blood product administration, initiation of vasopressors or any invasive or surgical procedures (i.e., chest tube insertion, needle decompression).
Data were abstracted from the hospital's trauma registry with supplemental information obtained from manual chart review of electronic medical records including trauma bay nursing records and trauma team leader transcription. The occurrence of AE was screened from the manual chart review defined by when the patient departed the trauma bay for the CT suite to when the patient was handed over to the ICU or OR staff. Overall, 98% (526/537) had complete trauma bay records and laboratory results. We excluded 11 patients (2%) with missing data and completed a comprehensive case analysis. 15
Two study authors reviewed a random sample of 20 patient charts and the inter-rater reliability resulted in 100% agreement for AE assignment. There was no formal sample size calculation obtained as the study is predominately descriptive; we selected a 22-month study period to account for annual and seasonal variations in trauma volumes. This time frame allowed us to achieve a sample size similar to other published reports10,16
Outcomes
The primary outcome is the incidence of AE during transport and/or during CT among critically injured trauma patients. The secondary outcome included the risk factors associated with AE and the risk of 7-day in-hospital mortality between patients who did and did not experience AE.
Statistical analysis
We used descriptive statistics for all variables of interest. We performed a univariate analysis for continuous variables using t-tests, parametric or non-parametric as appropriate. We analyzed categorical variables using Chi-Square tests.
We developed a logistic regression model to study the association between AE and in-hospital mortality at day 7. Age and ISS were determined a priori to be included in the model as confounders to mortality. A similar logistic regression model was also used to explore specific patient characteristics and probability of having AE. To obtain information as to when the event occurred, a time-to-event analysis was used to investigate the relationship between AE and in-hospital death after adjusting for age and ISS. Schoenfeld residuals were used to assess the proportional hazards assumption. Residual analysis was used to examine the model fit. All models were internally validated using the bootstrap method and calibration of the logistic regression model was also performed using the bootstrap method. 15 The number of variables included in each of the above models was limited using the rule of thumb of 10 events per predictor
Results
Frequency and nature of AEs in patients undergoing trauma CT
A total of 526 critically injured trauma patients underwent CT scan during the study period (Figure 1). The incidence of AE was 17.3% (91/526), and occurred during CT image acquisition. There were no significant differences in age, gender, mechanisms of injury or ISS between AE and no-AE patients (Table 1).
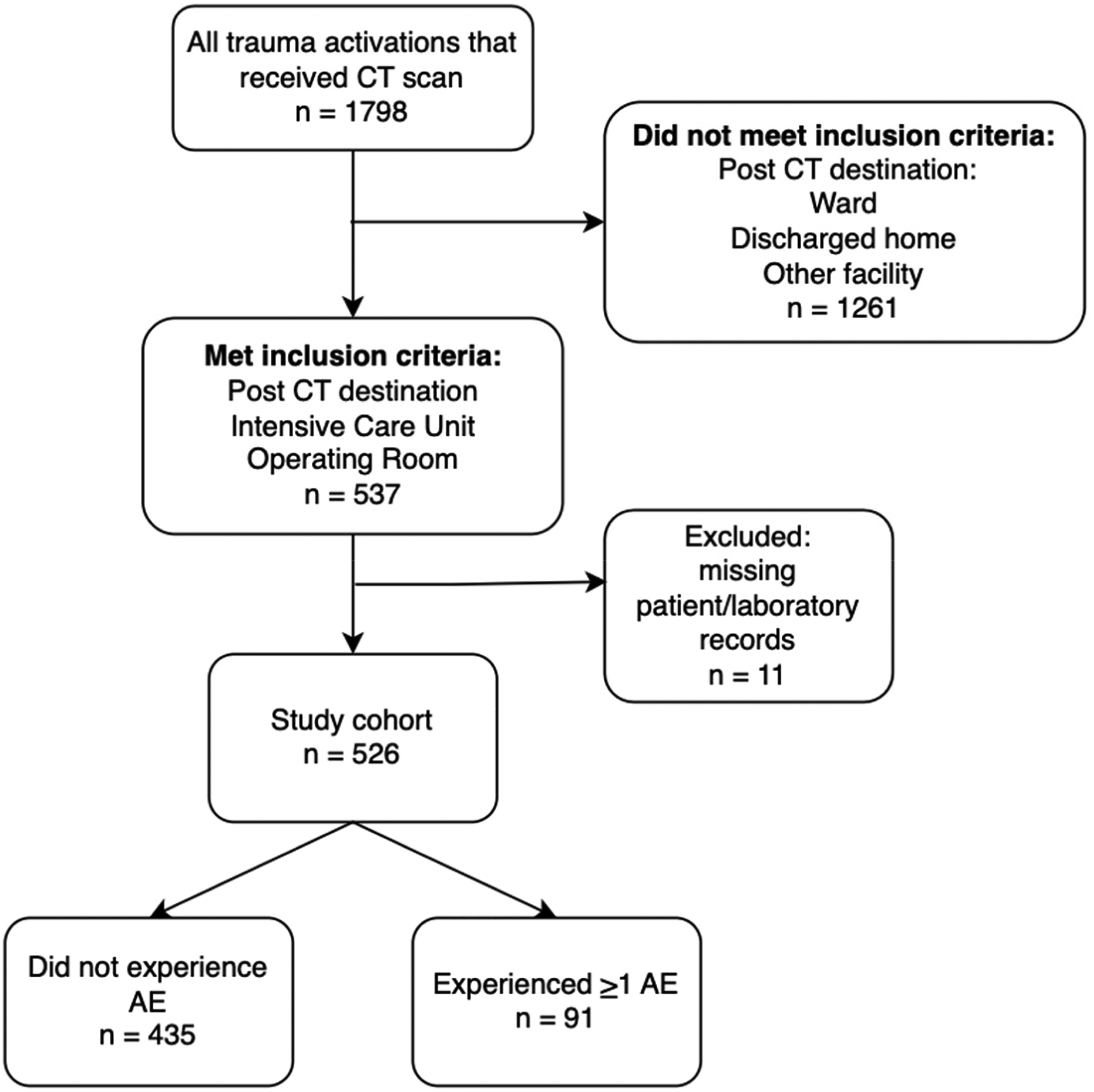
Study flow diagram of critically injured patients who underwent emergent trauma CT and experienced AE between 1 January 2019 to 1 November 2020. CT: computerized tomography; AE: adverse event.
Baseline characteristics of patients who underwent trauma CT who had and did not have an adverse event.
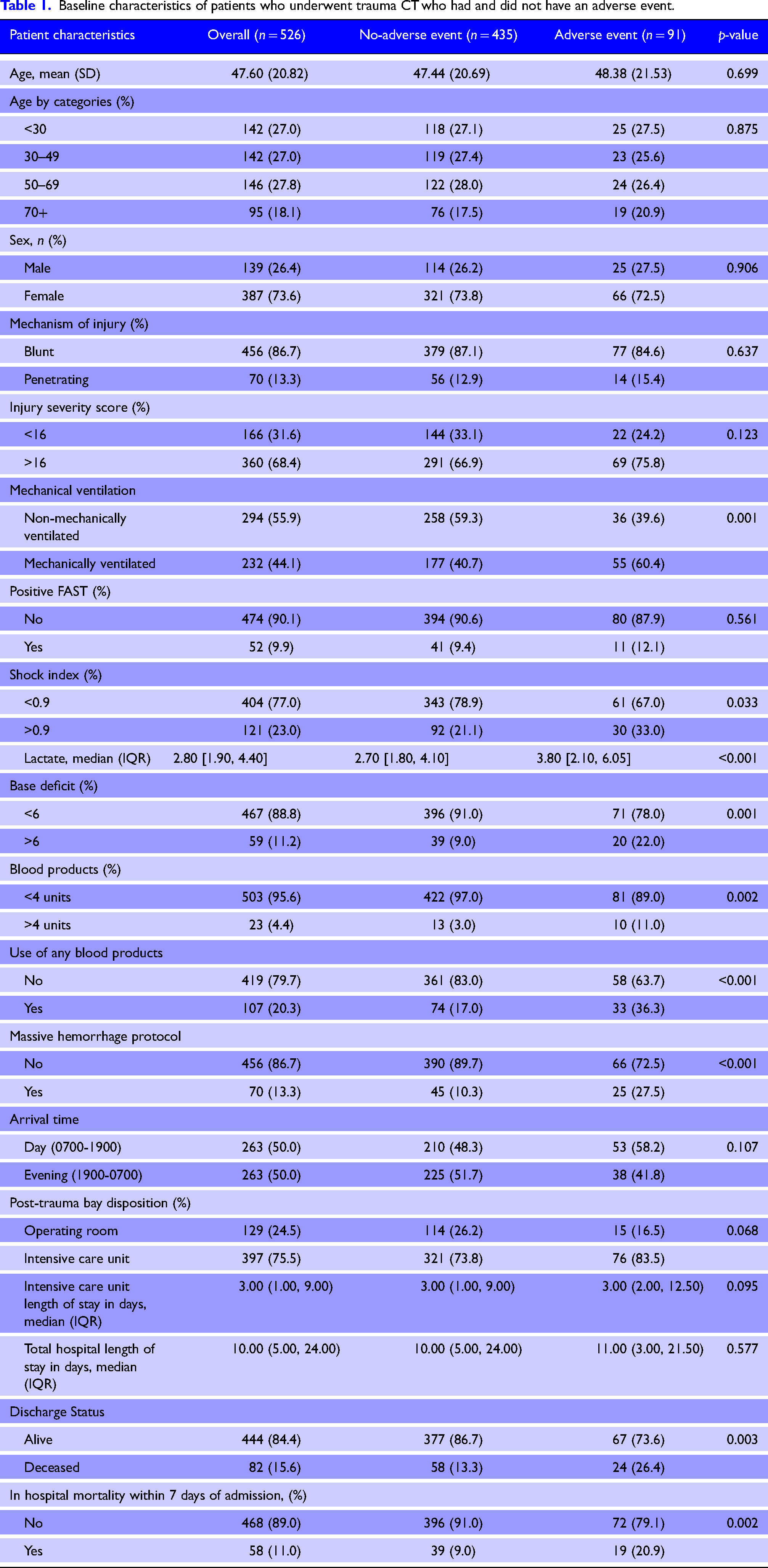
Patients in the AE group were more likely to be mechanically ventilated (60.4% vs. 39.6%), have a positive shock index >0.9, higher lactate (3.8 vs 2.7), or greater base deficit >6 (22% vs. 9%) than those in the no-AE group. Patients in the AE group were also more likely to require the use of any blood products (36.3% vs 17%), require >4 units of blood products (11% vs. 3%) or require massive hemorrhage protocol activation (27.5% vs 10.3%).
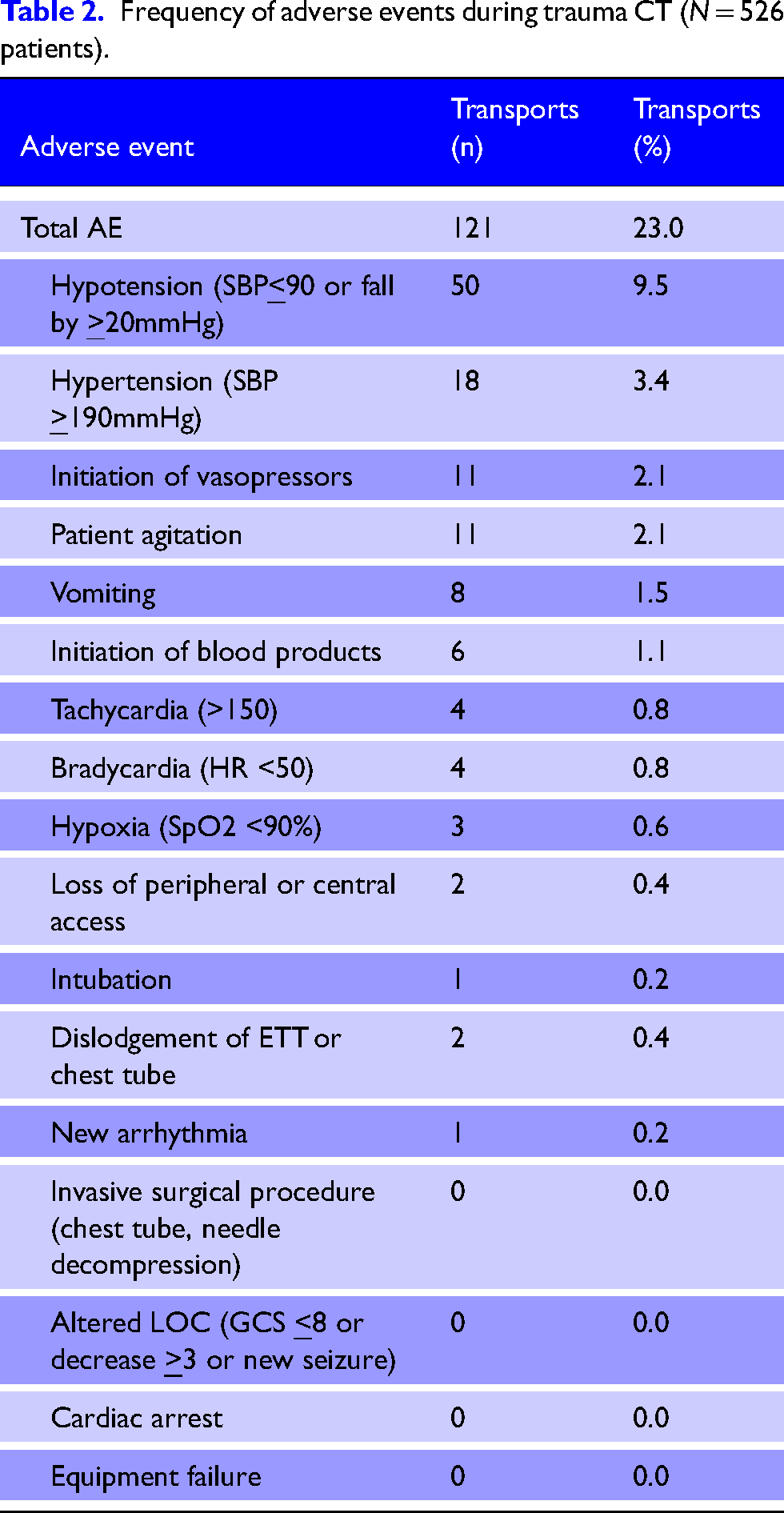
The most common AE recorded (Table 2) was hypotension n = 50 (9.5%). In one case, the CT was prematurely terminated and the patient was brought to the OR due to hemodynamic instability. Hypertension was the second most common AE n = 18 (3.4%), followed by initiation of vasopressors n = 11 (2.1%) and vomiting n = 8 (1.5%). While we did not a priori define agitation as an AE, in a subsequent review of the 91 patients who experienced AE, 11 patients (2.1%) required pharmacotherapy for agitation management. Notably, one patient required intubation for hypoxia post-sedation for agitation, and one patient required re-intubation after dislodgement of endotracheal tube during CT scan.
Frequency of adverse events during trauma CT (N = 526 patients).
Patient characteristics associated with having any AE
Using a multivariable logistic regression model, mechanical ventilation (odds ratio (OR) 1.84, 95% confidence interval (CI) 1.13–3.02) and requiring a blood transfusion (OR 2.04, 95% CI 1.11–3.75) were each significantly associated with the incidence of an AE (Table 3).
Logstic regression model of probability of having an AE after adjustment of patient characteristics.
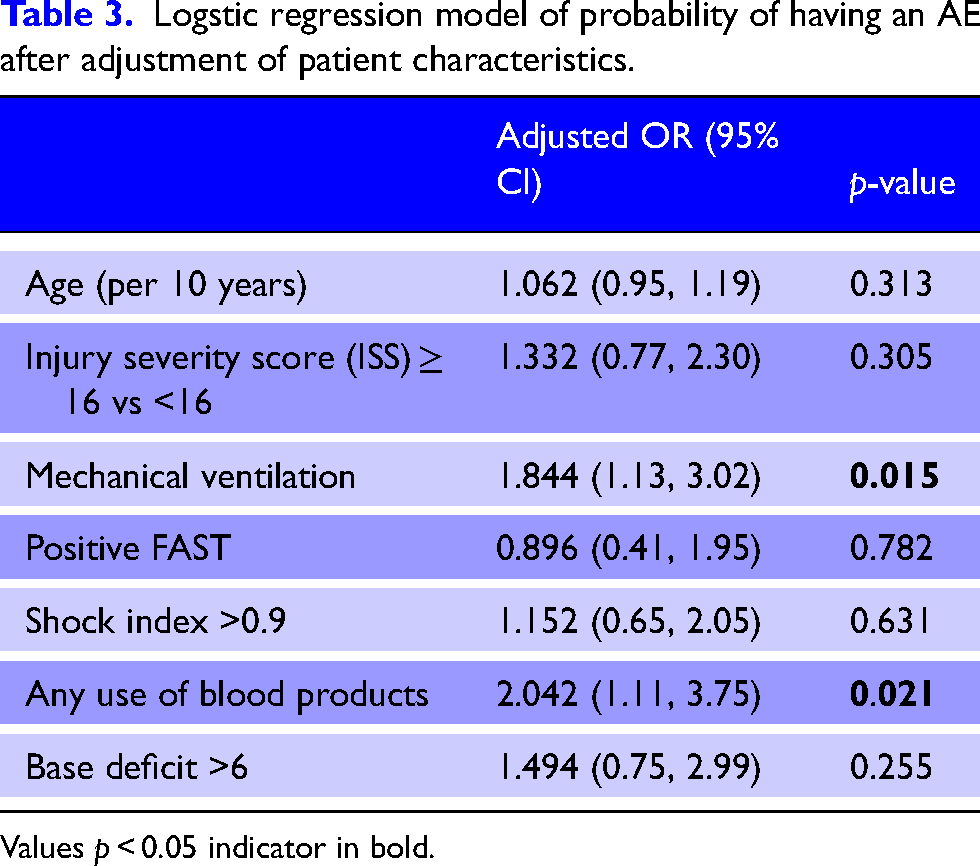
Values p < 0.05 indicator in bold.
Association of AEs and 7 day in-hospital mortality
A multivariable logistic regression analysis found a higher odds of death for patients with an ISS > 16 (OR 5.68, 95% CI 2.13–15.13), increasing age per 10 years (OR 1.51 95% CI 1.29–1.78) and requiring mechanical ventilation (OR 4.17 95% CI 2.15–8.08) (Table 4). Additionally, after adjustment, all AE was significantly associated with increased odds of death (OR 2.2, 95% CI 1.11–4.36). We conducted a ‘time to death’ analysis, which analyzed in-hospital length of stay while accounting for the competing risk of death (Table 5). While the ‘time to death’ analysis found no significant association between AE and time to death, there is an increased risk of death for older individuals, those with a higher ISS and mechanically ventilated patients.
Generalized estimating equation logistic regression model of odds of in-hospital mortality by day 7.
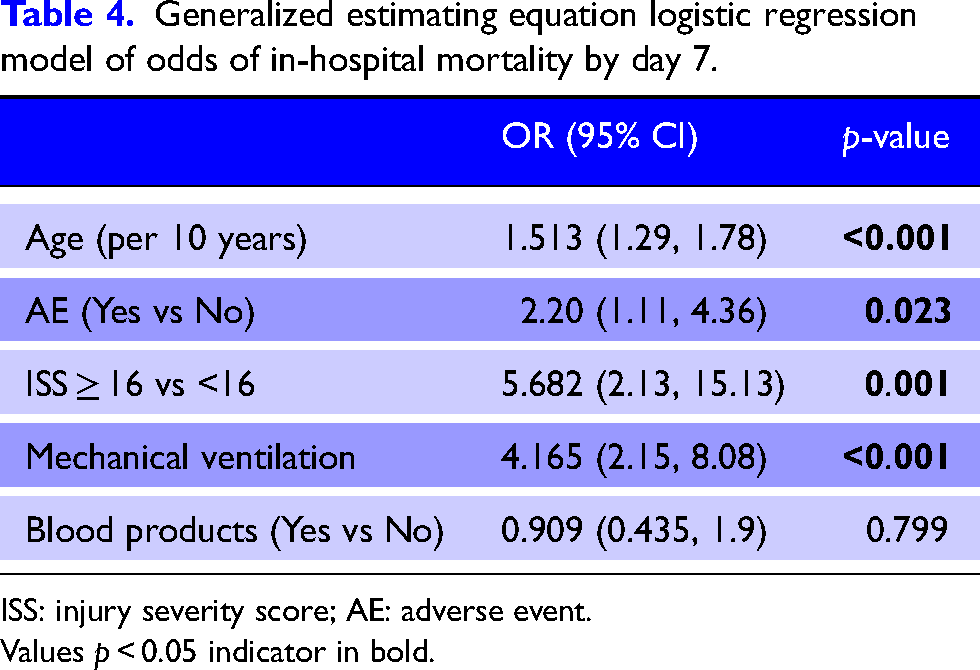
ISS: injury severity score; AE: adverse event.
Values p < 0.05 indicator in bold.
Time of death model.
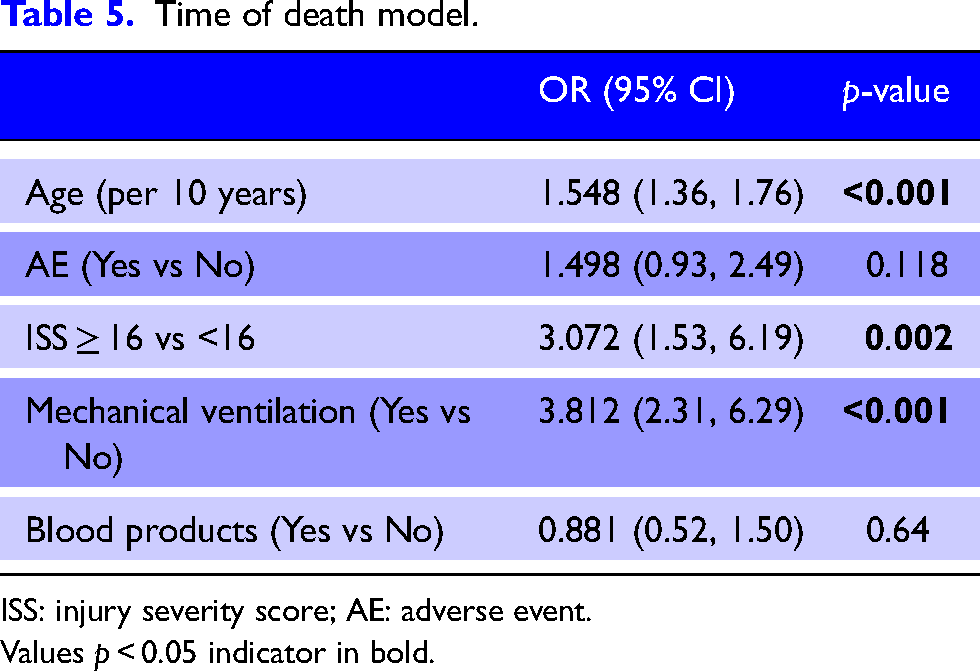
ISS: injury severity score; AE: adverse event.
Values p < 0.05 indicator in bold.
Discussion
We conducted a retrospective analysis to characterize AE among critically injured trauma patients in transit to and during emergent CT scan. We found that 17% of these patients experienced ≥1 AE, most commonly hypotension. Two patients required intubation during CT for hypoxia post-sedation and dislodgement of the endotracheal tube. Patient factors independently associated with AE in our study included mechanical ventilation and blood product administration. These AEs in CT were associated with higher odds of in-hospital mortality after adjustment for age, ISS, and mechanical ventilation.
The rate of AEs during CT scan in our study aligns with existing literature which report an incidence between 1% and 67.9%, however, these typically included non-trauma patients.8,10–12,13,16,17 In one retrospective study of 94 trauma patients undergoing emergent trauma CT, 47.9% patients experienced >1 AE. 17 In this single-centered study, patient requirement for vasopressor support and ongoing transfusion at the time of CT scanning was associated with AE. In contrast, a randomized controlled trial comparing immediate vs. selective CT scanning among trauma patients with potentially severe injuries found a < 1% rate of serious AE during CT scan, where all events resulted in death of the patient and all were hemodynamically unstable on presentation. 18 Similarly, Bashir et al. 19 found a 3% incidence of significant deterioration during CT that required intervention and cited reasons for deterioration including – undiagnosed tension pneumothorax, dislodged ETT, and catastrophic head injury resulting in hemodynamic instability. The heterogeneity in the reported AE rates in the literature is due to the absence of a standardized taxonomy of AE, challenging the comparison of AE across trauma centers. Studies that report a higher volume of AE tend to use a broad definition that span clinical events as well as non-patient related events (e.g., incorrect CT orders, delays in CT availability), 17 whereas studies with lower AE rates limit the definition of AE to serious events that may lead to intervention or patient death.19,20 A newly developed taxonomy of 67 AE that occurs during the initial phase of trauma resuscitation is an important step towards a standardized evaluation of safe trauma care across different centers. 21
In this study, hypotension occurred in 50 patients (9.5%) undergoing CT and while most were transient, six patients required blood product initiation in CT. This suggests these patients may have required further resuscitation prior to trauma bay departure. It is unsurprising that critically injured patients requiring blood products are at high risk for AE in the CT suite. These data however underscore the importance of robust protocols and strategies for patients at risk of hypotension. Mitigating significant hyper and hypotensive episodes is especially important in patients with severe traumatic brain injury. 22 To combat these predictable risks, trauma programs may look towards a pre-departure checklist that follows the principle of an “operative pause” whereby the team deliberately asks whether this patient is stable for CT or is the OR required (a “pathway pause”). Additionally, protocols may include a requirement of invasive blood pressure monitoring (e.g., arterial catheterization) among patients requiring blood products to more closely monitor hemodynamic stability and that additional blood products accompany the patient to CT along with pre-mixed vasopressors.
Other less frequent AE included hypertension, vomiting, and agitation. Each of these represents additional opportunities for targeted protocols and mitigation strategies. For example, hypertension among injured patients may be related to pain or inadequate sedation. This may indicate that quality improvement initiatives linked to timely and adequate analgesia are required. This aligns with the American College of Surgeons Trauma Quality Improvement recommendations of providing appropriate and timely pain management to trauma patients. 23
Opportunities for improvement and/or change
The CT suite represents a high-risk phase during the care of the severely injured patient. Several factors may amplify this risk including a decreased ability to directly monitor the patient in the CT scanner as well as limited access to resuscitation equipment within or in transit to radiology. The data from this study provide important information to help guide opportunities for improvement. This can be considered at multiple levels:
Design of the built environment: The future of trauma care requires purposely built environments that support rapid, efficient, and safe care. Placing the CT scan within, or in close proximity to the trauma bay reduces transport time and may improve patient safety and mortality24,25 Development of safety-focused protocols: Optimization of hemodynamic status, treatment of nausea, pain, and agitation prior to CT are key strategies to mitigate AE. With attention to the data from this study and the existing literature, safety-focused protocols
26
can be developed and implemented to direct clinician attention to high-risk patients along with mitigation strategies including consideration of common femoral artery access for resuscitative endovascular balloon occlusion of the aorta in select patients. Transport and CT suite interventions: As a final lever to improve patient safety, once the decision is made to transport to CT, support for clinicians can be achieved through appropriately selected equipment and medications for high-risk patients.
2
Limitations
This study has several limitations that must be acknowledged. As a retrospective analysis it relied on the accuracy of the patient care record which may be incomplete. This limited the ability to better describe time-associated delays that may help to better understand the clinical context and AE occurrence. Rates of AE were exclusively defined to those who were critically injured, and may not be applicable to all patients undergoing emergent trauma CT. We conducted this study at a single center which potentially limits widespread applicability, though our findings are in keeping with the existing literature providing reassurance that this study is relevant and important. Definitions for AE vary widely in the literature; consequently, we selected a broad definition to better capture and review a range of clinically important events. Finally, following the literature, we weighted all AE equally. While we recognize the potential heterogeneity between AEs, there is no standardized taxonomy or classification. To manage this limitation we provide a narrative context for two serious AE.
Conclusion
Critically injured trauma patients undergoing emergent CT scan are at risk for several AE during transport and imaging. In this study, 17% of patients experienced an AE, most commonly hypotension. Those requiring mechanical ventilation and blood product administration were more likely to experience AE and we found an association between AE in CT and higher odds of in-hospital mortality. This data supports the design of system- and process-level interventions to improve patient outcomes among trauma patients undergoing emergent CT.
Footnotes
Declaration of conflicting interests
The authors declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The authors received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
The study was approved by the Research Ethics Board of St. Michel's Hospital (REB # 20-326).