
Abstract
Background:
At its inception, there was no formal provision for children within the English major trauma network. There are now combined and stand-alone centres, but the scarcity of paediatric trauma facilities in some regions can result in long patient transfers and impact patient outcomes. The objective of this study was to determine the proportion of paediatric trauma patients who may benefit from input by adult services or may be safely managed within the local adult MTC, either because of patient physiology or injury patterns.
Methods:
All trauma presentations to our urban MTC aged ≤16 over a 3-year period were retrospectively identified and grouped, based on age and weight. ‘Young adult’ mechanisms of trauma and patient destinations (whether paediatric or adult wards) were determined.
Results:
There were 847 paediatric trauma cases recorded with a mean age of 9 and a male preponderance. Based on age and weight, 10–45% of cases could be considered physiologically adult-like, and 22–28% pubertal. Almost all penetrating trauma occurred in males, increasing with age. 14% of all admissions were managed on adult wards, with frequency increasing with patient age and with mechanism of actions (MOIs) relating to interpersonal violence.
Conclusion:
In this dataset, nearly half of paediatric trauma was ‘pubertal’ or ‘adult’ in their physiology and of these most presented with ‘young adult’ MOIs. These children likely benefit from combined paediatric and adult trauma services; where these do not exist, some older patients may be safely managed within local adult MTCs.
Introduction
Trauma is the primary cause of morbidity and mortality in children in high-income countries. The mean age of presentation of paediatric trauma is 7 years with a male preponderance (3:2). 1 Overall, outcomes following major trauma in the UK have improved in the last decade, especially following severe injury. The development of major trauma networks between 2010 and 2012, with associated centralisation of trauma care, is believed to be fundamental to this.2–4
At its inception, there was no formal provision for children within the English major trauma network. Paediatric Major Trauma Centres (MTCs) were subsequently designated and now comprise five stand-alone Paediatric MTCs and 11 combined Adult and Paediatric MTCs, leaving 10 Adult-only MTCs. It is believed that, overall, paediatric trauma managed at paediatric centres has better outcomes: patients have shorter lengths of stay, fewer invasive interventions and less radiation exposure. 5 Most importantly a reduction in mortality in the under 5 year olds has been demonstrated.5,6 However, the scarcity of paediatric care facilities in some regions may result in long patient transfers and ultimately impact patient outcomes. So far, nuances like this have not been addressed in the literature.
The reported advantage of paediatric MTCs is less marked in older children, those with severe injury and following penetrating trauma.5,7,8 The significantly higher volume of penetrating trauma seen by adult trauma teams means the expertise for managing these patients may reside amongst adult clinicians.9,10 A similar precept may be true for severe injury which is also more frequently seen by adult teams. Additionally, older children may have adult-type physiology and may respond better to adult algorithms for resuscitation and ongoing care. A combined approach involving adult and paediatric trauma services may be best for a subset of paediatric patients. This is supported by data demonstrating improved paediatric outcomes in combined centres, including higher rates of splenic preservation. 5
At our urban, combined MTC, paediatric trauma patients are initially assessed by a trauma team that encompasses paediatric and adult trauma expertise. The team is supported by paediatric physicians. Inpatient care, including operative management, continues to involve both paediatric and adult trauma surgeons, in addition to paediatric physicians and allied services. Patients can be referred to trauma psychologists from the adult service, charities that support victims of interpersonal violence, and social services. Patients are managed on either the paediatric or adult trauma ward, depending on patient needs and security risks for other patients. The trauma team flexes to provide equivalent care in either location.
In some geographical locations, paediatric MTCs are separate from adult MTCs. Where integrated paediatric and adult services do not exist and where the paediatric MTC is some distance away, there may be an argument for the management of some paediatric patients within the adult MTC. The Trauma Audit and Research Network (TARN) is a UK-wide registry that prospectively collates data from all MTCs and trauma units (TUs) and issues quarterly reports to ensure ongoing adherence to high-level trauma care. In 2012, a TARN report found that 50.6% of paediatric trauma underwent multiple hospital transfers prior to definitive care. Additionally, for children with injury severity scores (ISS) of >15, only 28.6% were eventually transferred to an MTC with paediatric services, without detrimental outcomes in patients who were not transferred. 11 Accurate identification of patients who do not require transfer out of the local adult MTC has the potential to decrease the logistical, financial and clinical implications of inter-hospital transfers.
The purpose of this study was to determine the proportion of paediatric trauma patients who may benefit from input by adult services or may be managed within the local adult MTC, either because of patient physiology or mechanism of action (MOI).
Methods
All trauma presentations aged 16 and under at the time of injury, presenting between 01/01/2017 and 31/12/2019 were extracted from the hospital’s major trauma database. This database is prospectively maintained and is used to populate TARN, the national trauma database. All trauma called patients are included, in addition to any non-trauma called but TARN-eligible patients. It includes patient demographics, mechanism of injury, injury pattern, place of admission, discharge details and mortality.
Weights within 6 months of the date of injury were extracted from clinical records. When more than one weight was documented, the weight closest to the date of injury was used. TARN definitions for MOI were used. Results are presented using descriptive statistics.
There is no clear definition of ‘adult’ and ‘paediatric’ within the literature. Given these difficulties in defining adult versus paediatric physiology, multiple criteria were used.
12
These were:
Royal College of Nursing (RCN) method: Children older than or equal to 12 years of age were considered to have adult-like physiology, and those younger than 12 paediatric physiology. This was based on the RCN definition of normal cardiovascular and respiratory observations by age. These markers of physiology resemble those of adults by age 12.
13
Royal College of Paediatric and Child Health (RCPCH) growth chart method: Girls aged over 13 and boys over 14 are classed as pubertal, and girls over 16 and boys over 17 were classed as adult. This was based on the age at which children are expected to have entered and completed puberty as outlined in the RCPCH growth charts. The RCPCH definitions of sexual maturity correlate to published data on sexual maturity, skeletal age and peak height velocity which in turn are reproducible markers of anatomical and physiological maturity.14,15 In order to avoid relying exclusively on age, the 50th centile weight for these respective ages was also extracted from the growth charts, and patients weighing above this were also classed into each respective category (see Supplementary Online Material: Appendix 1).16,17
Injury mechanism was grouped as either being an adult, paediatric or generic mechanism for the purpose of the discussion. Falls from less than 2 m and burns were considered paediatric mechanism. Stabbings, cyclist versus other vehicles and motorcycle versus other vehicle RTAs were considered adult mechanisms (see Supplementary Online Material: Appendix 2).
Results
There were 847 paediatric trauma cases recorded over 36 months. There were seven early deaths (defined as death prior to discharge from the index presentation). The mean age of presentation was 9 years of age (median 11 years, range 0–16) with a bimodal distribution (initial peak in incidence in 0–3 year olds and a second, higher peak, in 14–15 year olds). Traumatic injury was more prevalent in males across all age groups (70.4% of cases, Figure 1).
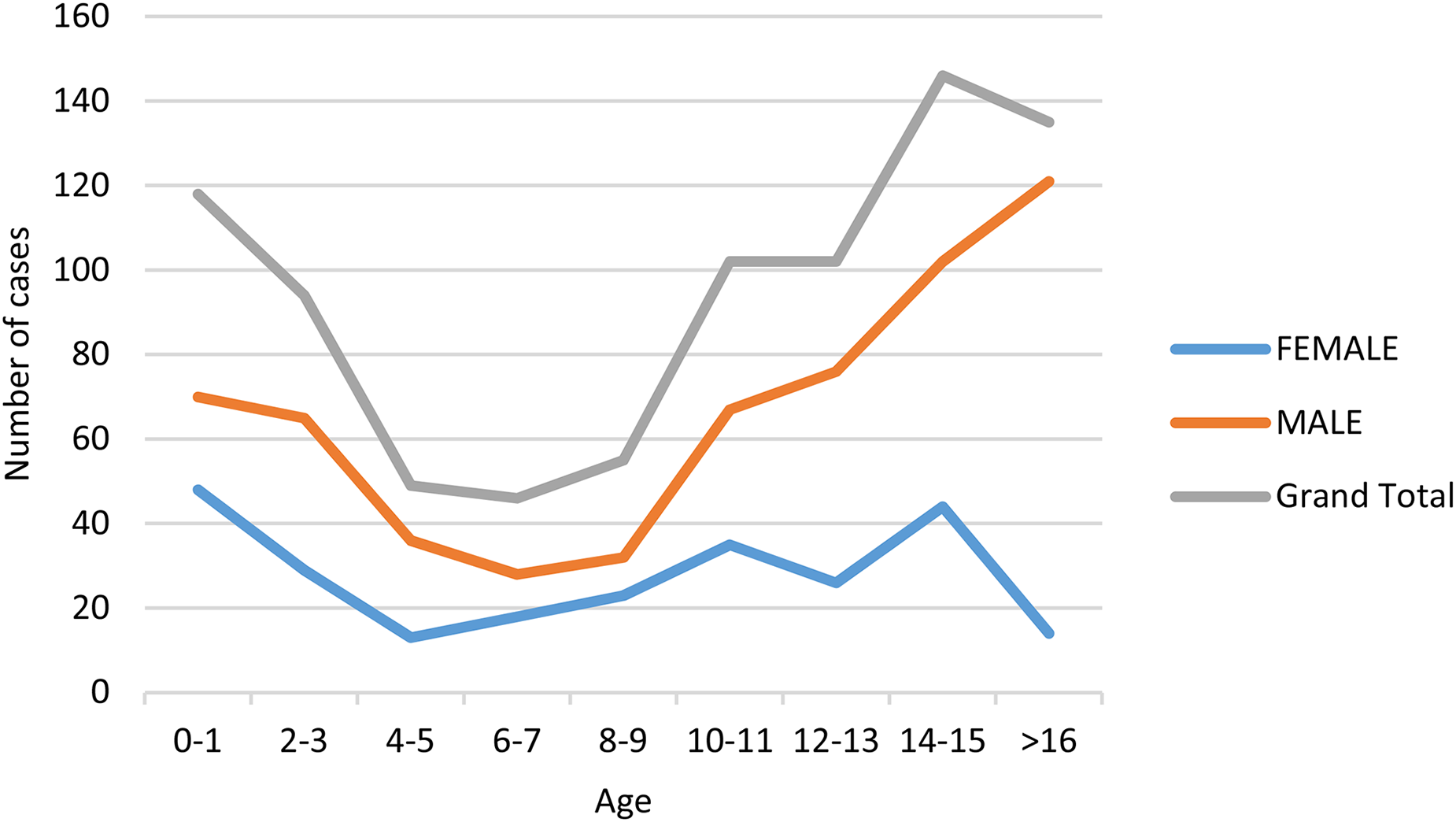
Patient age at time of presentation. Trauma was more common in males, with a peak incidence before the age of 3 and after the age of 12.
Weight/age
Age was recorded in all cases and weight was recorded for 52% of patients (n = 438, 38–62% of patients per age group). There was no difference in the proportion of patients who had a weight recorded between the different age groups (data not shown). Using the RCPCH-based previously described definitions, patients were categorised as children, pubertal or adult (Figure 2).
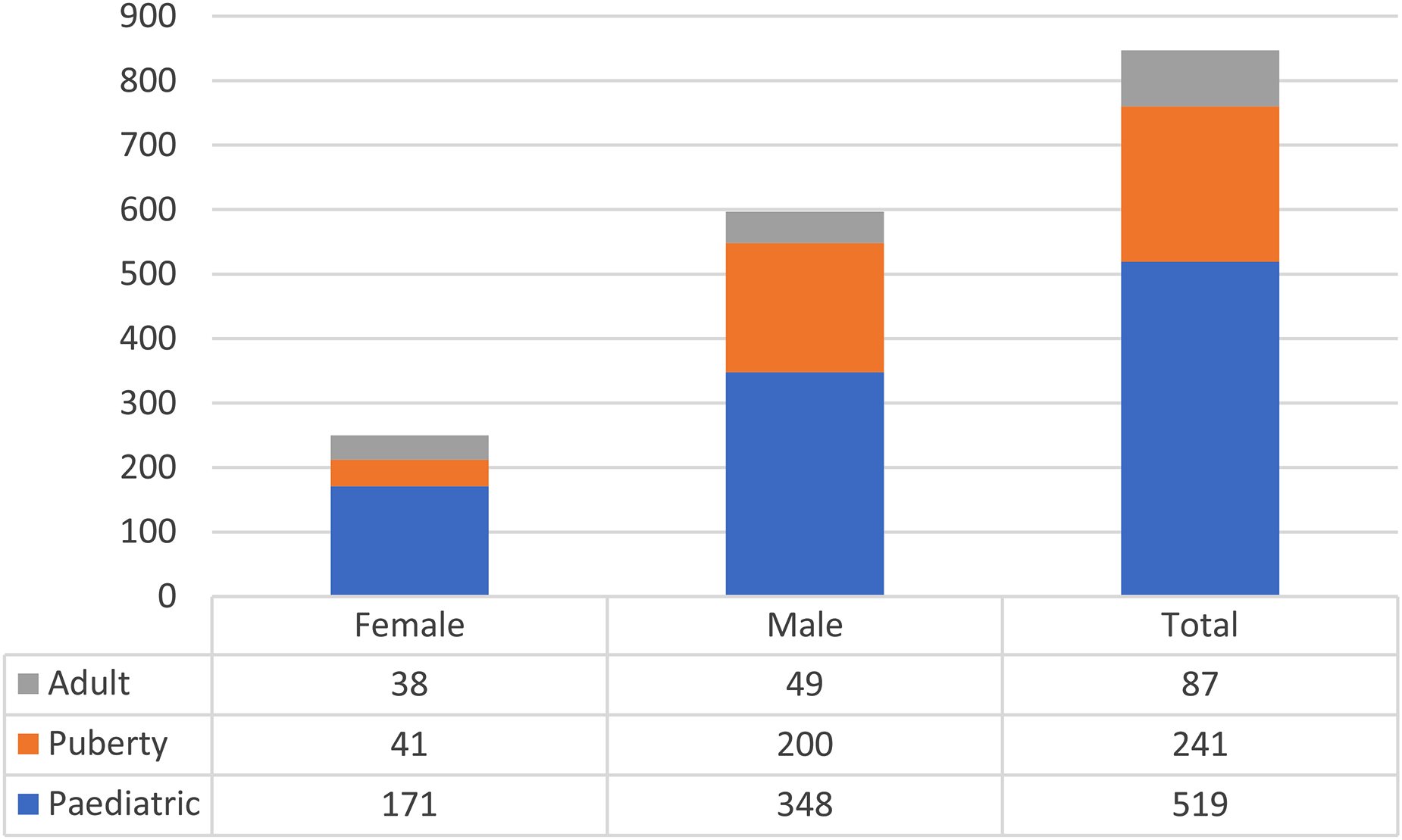
A graph to show the subdivision of paediatric trauma by physiology. Patients were categorised as pubertal, paediatric or adult based on their weight where available, and age. 38% of cases were either considered adult (10%) or pubertal (28%).
Of the cases with a recorded weight, 18% had a weight or age consistent with adulthood and 22% had a weight or age consistent with puberty. When patients’ weights were not available, they were categorised by age only; when combined 28% of cases were pubertal and 10% adult-like cases (total 38%). When age was used in isolation for categorisation (the RCN-based method), 45% of all patients were ‘adult-like’; of this latter group, 22% were female and 78% male.
Mechanism of injury
Overall blunt trauma was more frequent than penetrating trauma (Figure 3), although penetrating trauma surpassed blunt trauma in children over the age of 14. There was a rise in penetrating trauma amongst older male subjects that was not replicated in the female population; 94% of penetrating trauma occurred in males.
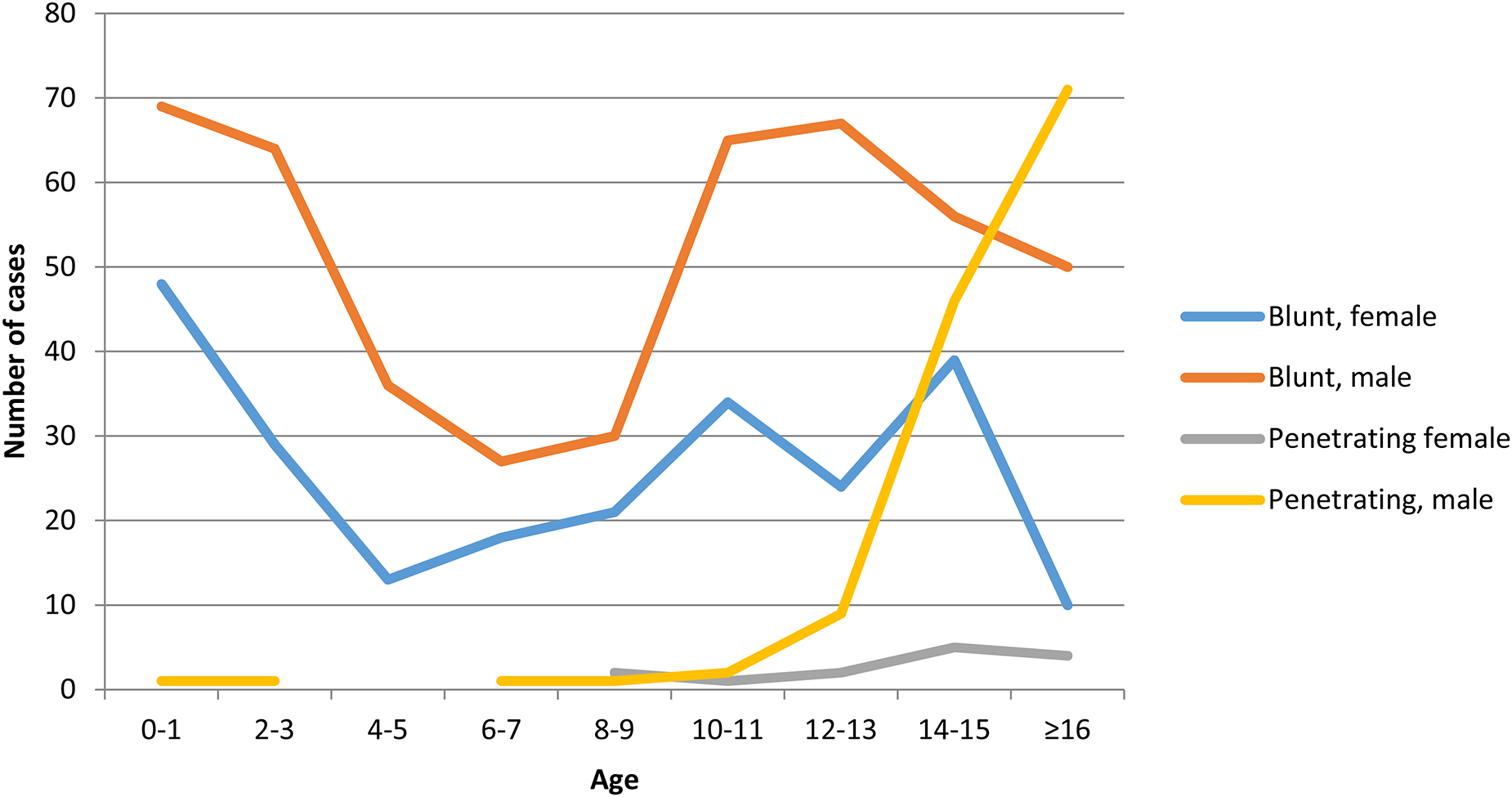
A graph to show the categorisation of trauma as either ‘blunt’ or ‘penetrating’ by age and sex. Overall, there was a predominance of blunt trauma. However, in males over the age of 12 penetrating trauma began to rise sharply, with a similar smaller increase in incidence seen in the female population.
MOI varied with age (Figure 4). The most common MOI in the under-2 year old population was fall from height (45% <2 m, 18% >2 m) followed by burns/inhalation (21%). Fall from height remained the most common MOI until the age of 12. Pedestrian versus car Road Traffic Collision (RTC) increased with age peaking at age 12–13 where it represented the most frequent MOI (48%). Over the age of 14, interpersonal violence increased significantly making up 66% of all trauma cases in 16 year olds.
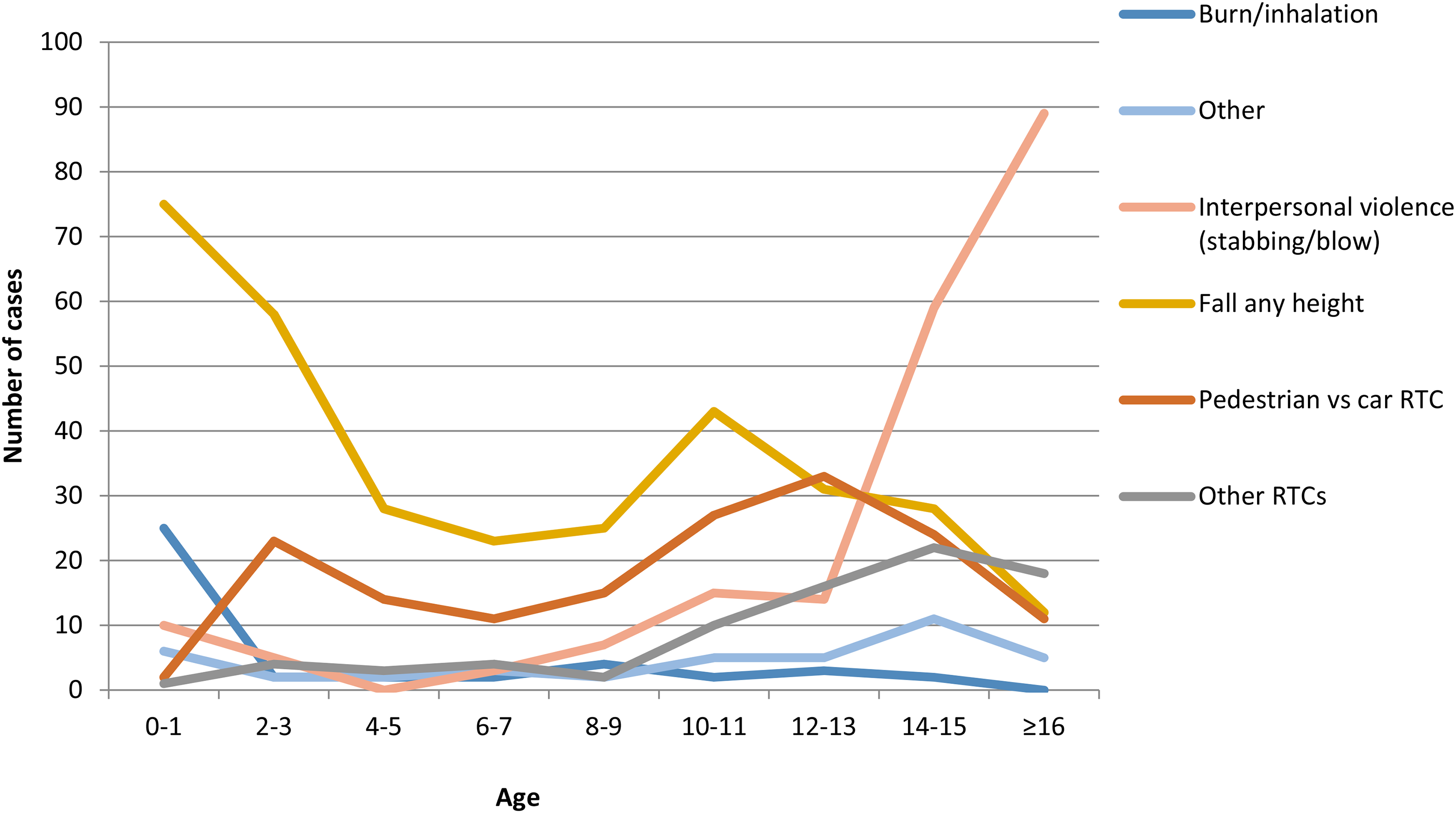
A graph to show MOI by age. Fall from height was the most frequent MOI in younger children but decreased in frequency with advancing age. Interpersonal violence became increasing common with advancing age and was the most common MOI in the over 13 year old age group. Pedestrian vs car RTCs was a common MOI across ages. All injury mechanisms with fewer than 10 cases were grouped under ‘other’ including one animal attacks, one crush injuries and two electrocutions.
Place of admission
Overall, 59% of all trauma patients were admitted to a ward, 31% of patients were discharged from A&E, 5% were transferred straight for intervention and in 13% the patient destination was not recorded (Figure 5).
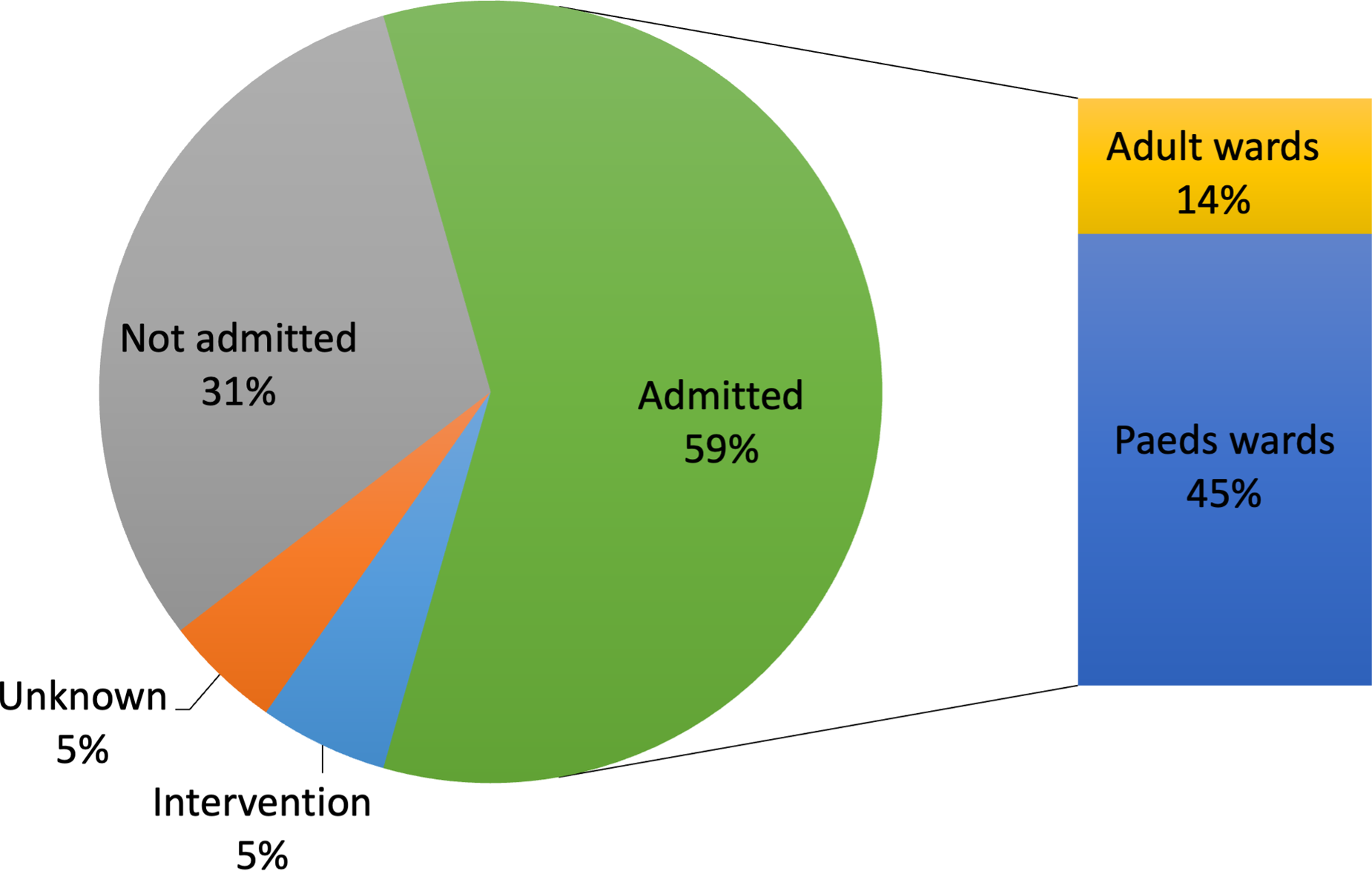
This pie-chart displays patient destination from the emergency department. Most patients were admitted to hospital, and of those 14% were managed on adult wards.
In total, 14% of all admissions were managed on adult wards. Frequency of admission to adult ward increased with patient age (5% of patients aged 14–15 and 27% of patients aged 16–17). All 14–15 year olds managed on adult wards were admitted following stabbings, and 64% of the 16 year olds on adult wards were victims of violent crimes.
Discussion
Do adult trauma surgeons have a role to play in the management of paediatric trauma?
Trauma is a disease of deranged physiology. Of all clinicians, paediatric teams are most skilled in managing pre-pubertal patients whose physiology is most different to adults.5,6 ‘Pubertal’ and ‘adult-like’ children are physiologically more similar to the adult population and may be less reliant on specialist paediatric resuscitation. Anatomical changes seen with age are also an important consideration in the management of paediatric patients. The same MOI may be associated with different injury patterns and have different management considerations. For instance, with advancing age the liver and spleen take up proportionally less intra-abdominal space and become shielded by the rib cage. In terms of anatomy, ‘pubertal’ and ‘adult-like’ children more closely resemble adults than infants, and MOIs will be associated with adult-like patterns of injury.18,19 Thus 32–45% of patients from the cohort presented here might benefit from input by adult trauma clinicians experienced in adult physiology and patterns of injury.
The prevalence of MOIs varies hugely across the different stages of childhood. In the pubertal years, interpersonal violence outstrips other MOIs, peaking in incidence at age 16. A large proportion of this burden is due to penetrating trauma, especially in pubertal males. In the literature, the peak incidence of penetrating trauma is reported to be at 26 years of age (although frequency has increased year on year in 16–19 year olds 10 ). Put together, the literature and our data hint at ‘young adult’ MOIs which coupled with ‘young adult’ (pubertal or adult) physiology blur the artificial distinction made by health services between paediatric and adult.
In the UK, less than 5% of trauma occurs in children. Thus it could be argued that where the distinction between paediatric and adult trauma is blurred, adult surgeons may carry the numerical weight of experience for managing such cases. 9 Given the strong association between higher trauma volume and improved outcomes it would seem sensible to involve adult clinicians in the management of paediatric trauma. 20
Could combined MTCs offer best care for some paediatric patients?
Overall, 32–45% of patients in this cohort were physiologically adult or pubertal. Both in terms of physiology and pattern of injury, these patients are likely to benefit from the inclusion of adult trauma specialists in their care. This is most readily achieved by combined MTCs and so co-location of adult and paediatric trauma services within a combined MTC may represent the best model for delivery of paediatric trauma care.
Evans et al. came to a different conclusion with their data, suggesting that adolescent trauma mortality is lower when managed at paediatric versus adult or combined centres. 21 However, in that study, only 8% of adolescent trauma was managed in children's MTCs and no allowance was made for significant differences in MOIs between sites. Likewise, adolescent patients in paediatric MTCs had significantly lower injury severity scores, longer time to CT scan and lower rates of consultant-led care than those managed in adult or combined centres. More concerningly, older teens had higher mortality when managed in paediatric MTCs, in keeping with data from McCarthy et al. who found no mortality benefit with the management of adolescents in paediatric centres. 5 Evans et al. also excluded all patients who presented via (TUs). As some very unwell patients might initially be taken to local (TUs) for stabilisation, we believe this represents a fundamental flaw in the study design. We believe that a more careful look at integrated paediatric data from across the country would enable robust conclusions to be drawn about the best management of paediatric trauma.
The outcome data in the literature do not take into account the softer measures of successful trauma management which must also be considered in any integrated data review. Interpersonal violence was the second most common cause of trauma in our cohort (25% of all patients). Beyond their medical needs, these patients have complex psychosocial needs. In combined (and paediatric) MTCs, care is delivered by a multidisciplinary team with senior specialist nurses focusing on the holistic aspects of care, involving social services and charities for the prevention of interpersonal violence. Patients presenting secondary to interpersonal violence also have specific security issues. There is controversy about where these patients should be managed, in order to both provide best care for the patient and protect other patients from harm.
The optimal solution would be a secure adolescent ward but in the absence of this we make a decision regarding the patient location on a case-by-case basis. In the cohort presented here, 23% of paediatric patients were successfully managed on the adult trauma ward, with paediatric services input, as per our usual multidisciplinary approach. Flexing care to meet individual patient needs in this way can only be provided by a fully integrated paediatric and adult trauma service and again supports the argument for the co-location of services. An integrated model of paediatric trauma care has the added advantage of enabling shared learning between adult and paediatric teams. This maximises opportunities for case discussion which in turn contributes to improved care moving forward.
How should paediatric trauma be managed where adult and paediatric services are not co-located?
Despite significant progression in the organisation of trauma care in England over the last decade, patients in some parts of the UK must travel large distances to access specialist paediatric trauma services, often bypassing local adult MTCs. Longer transfer times in paediatrics delays time to definitive care and is a predictor of longer length of stay. 22 Furthermore, in adult studies, secondary transfer is associated with imaging and surgical delays as well as increased severity-adjusted mortality. 23 Likewise, management of paediatric patients at a greater distance from their home address is associated with longer lengths of stay and has adverse financial, social and psychological implications for both child and family.24,25
For younger patients with ‘paediatric’ physiology, it would seem reasonable to continue management at paediatric MTCs as the benefits of specialist paediatric care probably outweigh the risks associated with long transfer times. However, older patients with ‘pubertal’ or ‘adult’ like physiology could be considered for management by local adult services alone, with the right safeguarding and specialist support. From our data, applying this principle would mean that nearly half of paediatric trauma patients may not require transfer to specialist paediatric MTCs if already located within an adult MTC. Avoiding transfer could have significant cost-saving implications for health care services, decrease the length of stay and improve overall outcomes, without detrimental clinical outcomes. Further studies to address this would be beneficial.
We did not collect data on non-accidental injury (NAI); however, a prior study found NAI makes up 7.6% of UK major trauma and is associated with more severe injury and higher mortality. 26 The majority of cases occurred in patients under the age of 1 (76%) with almost all occurring in under 5 year olds; hence these cases will rarely fall under the ‘adult’ or ‘pubertal’ physiology cohort where we have proposed possible management in adult centres. We nonetheless acknowledge the need for rigorous pathways for identifying and managing these patients and propose these patients are cared for in either combined or paediatric centres irrespective of age or mechanism where these pathways are more developed.
Study limitations
One of the challenges faced in this study, and mirrored in the literature, is the difficulty in defining ‘paediatrics’. The upper age limit for paediatric care ranges worldwide, from 11.5 to 19.2 years of age. 27 To arrive at a physiologically meaningful definition of ‘paediatric’, definitions were derived from both the Royal College of Paediatrics and Child Health (RCPCH) and the Royal College of Nursing (RCN). Use of two definitions provided some internal corroboration but is an imperfect tool for definition. An international consensus on the definition of paediatric would be of great value to the literature.
This paper takes an overview of all paediatric trauma data from an urban MTC across a 3 year period. The hospital trauma database was used for case capture, rather than the TARN database. This provided a comprehensive assessment of paediatric trauma but prohibited stratification by injury severity. Additionally, a significant proportion of the included trauma comprised minor injuries that did not require hospital admission. Whilst such cases do not strictly fall under the remit of major trauma, this approach does provide a more accurate evaluation of the overall burden of paediatric trauma and those cases which would meet major trauma thresholds but are not included within TARN criteria.
This study provides a single-site view of paediatric trauma and thus concrete conclusions about the best management of paediatric trauma cannot be drawn. It is not possible to establish from this data whether management differs between adult and paediatric surgeons because both are involved in care in an integrated approach. However, the data presented here does suggest that optimum management of paediatric trauma may be more nuanced than the published literature allows and suggests a closer look at the national data is warranted.
Conclusion
The current consensus is that paediatric trauma is best managed at paediatric MTCs. The evidence to support this claim is most clear for young children but becomes increasingly blurred for older children with ‘young adult’ mechanisms of trauma. In this dataset, nearly half of children at an urban combined MTC are ‘pubertal’ or ‘adult’ in their physiology and of these most present with ‘young adult’ MOIs. These children are likely to benefit from combined paediatric and adult trauma services. Where combined services do not exist, some older patients may be safely managed within local adult MTCs. Paediatric trauma care must be individualised, considering the specific, personal needs of each patient and accepting that these are likely to change with increasing age.
Declaration
Supplemental Material
sj-docx-1-tra-10.1177_14604086221129745 - Supplemental material for How much paediatric major trauma is truly paediatric? Experience from a level 1 urban Major Trauma Centre
Supplemental material, sj-docx-1-tra-10.1177_14604086221129745 for How much paediatric major trauma is truly paediatric? Experience from a level 1 urban Major Trauma Centre by Natalia Sanchez-Thompson, Esther Platt, Christopher Aylwin, Clare Rees, Nicholas Alexander and Sheehan Hettiaratchy in Trauma
Footnotes
Conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship and/or publication of this article.
Ethical approval
Ethical approval was not sought for the present study because patient management was not modified and the paper does not report any new or experimental protocols. This study was completed in accordance with the Helsinki Declaration as revised in 2013.
Informed consent
Informed consent was not sought for the present study because no primary research was performed. All data analysed was collected as routine for internal audits.
Trial registration
IRAS project ID 287274.
Contributorship
SH conceived the study. NST and EP researched the literature. NST and SH planned the study. NST collected and analysed the data and wrote the first draft of the manuscript. EP was the main manuscript reviewer. All authors reviewed and edited the manuscript and approved the final version.
Acknowledgements
We would like to thank Joanna Graves for her assistance in obtaining the data.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.