
Abstract
Introduction
Trauma registries are a means for improving trauma care in low- and middle-income countries, though a number of challenges for the sustainability of these trauma registries exist. Mobile health applications represent a promising technology for low- and middle-income country trauma registries. The development, implementation and evaluation of a mobile application trauma registry for use at the Mbarara Regional Referral Hospital, Uganda is demonstrated.
Methods
A paper-based trauma registry was implemented at the Mbarara Regional Referral Hospital. Based on feedback from local stakeholders, this was developed into an open-source mobile application version of the trauma registry. The mobile application was evaluated by 17 healthcare workers using a modified Unified Theory of Acceptance and Use of Technology questionnaire and qualitative analysis.
Results
Unified Theory of Acceptance and Use of Technology scores showed the majority of participants responding positively to the major constructs of Performance Expectancy, Effort Expectancy, Social Influence and Facilitating Conditions, with mean Likert scores (out of 7) of 6.41 (±1.43), 6.25 (±1.41), 5.44 (±1.43) and 5.32 (±1.99), respectively. There was also a young average user age (29.1 years). Qualitative analysis identified response themes of ease of use, efficiency and potential for future research and clinical use; users also suggested expansion of the type of platforms the application was available on.
Conclusion
Though a number of challenges exist for sustaining trauma registries in low- and middle-income countries, substantial involvement of local stakeholders and responsiveness to feedback should be used to facilitate the use of these technologies in developing countries. This study demonstrates a potential methodology for developing and evaluating trauma registry technologies for use in low- and middle-income countries.
Keywords
Introduction
Trauma is a significant source of global morbidity and mortality, with 90% of trauma deaths occurring in low- and middle-income countries (LMICs). 1 An essential step for developing effective trauma care systems in LMICs is the collection and evaluation of injury data using a trauma registry, a repository of trauma patient data used for quality improvement.2–4 A number of trauma registries have previously been established in LMICs, however, significant challenges exist for sustaining trauma registries in this setting, including a lack of funding and human resources.4–6
The use of electronic health (eHealth) technologies and mobile health (mHealth) technologies has been proposed as tools to help overcome these barriers and advance data collection in LMICs. Mobile devices are a relatively low-cost technology, with continually improving functionality and widespread accessibility in many LMICs. 7 In Uganda there are an estimated 25 million mobile phone subscriptions for a country of 37.7 million; in all LMICs, there are an estimated 103.8 mobile cellular subscriptions per 100 persons worldwide.8,9 In fact, due to the relative prevalence of mobile phones compared to personal computers, mHealth is likely to leapfrog other eHealth technologies in LMICs. 10 While most mHealth technologies in LMICs utilize short-message services, a growing number of mHealth phone applications are also being used. 11 The feasibility of mHealth for trauma registries has been demonstrated by Zargaran et al. with a tablet-based application used in a South African trauma centre. 12 The use of mobile applications for trauma registries in LMICs is, therefore, an affordable and practical option.
Despite the relative prevalence of mHealth technologies in LMICs, there is limited evidence to evaluate the use of mHealth in this setting. In one scoping review on mHealth applications, there was limited published research found on the topic, with only one qualitative evaluation model developed to evaluate medical mobile applications, and no evaluation models for electronic or mobile trauma registries. 13 While there are a few qualitative evaluation systems proposed for trauma registries, these are not specific to electronic or mobile platforms.4,14 However, all of these models of evaluation are qualitative or descriptive frameworks only and do not assess or predict use of the application.
Beyond the literature on eHealth/mHealth and trauma registries, there are a number of other technology evaluation models. One of the best-validated quantitative analyses for technology evaluation and prediction of future use is the Unified Theory of Acceptance and Use of Technology (UTAUT) questionnaire.15,16 The UTAUT formulates a unified model incorporating data from eight other information technology acceptance models and was found to predict approximately 70% of variance in an individual's intention to use a specific technology. 15 The UTAUT evaluates behavioural intention to use through three major constructs: Performance Expectancy (‘degree to which an individual believes that using the system will help him or her attain gains in job performance’), Effort Expectancy (‘degree of ease associated with use of the system’) and Social Influence (‘degree to which an individual believes that important others believe he or she should use the new system’). It also incorporates two direct determinants of usage behaviour: Facilitating Conditions (‘degree to which an individual believes that an organizational and technical infrastructure exists to support use of the system’) and Behavioural Intention to Use. Indirect constructs including Attitude towards Technology, Self-Efficacy and Anxiety are also incorporated into the original UTAUT model but are generally non-significant as they are captured by the other major constructs. All constructs are then modified by four contingencies: age, gender, experience and voluntariness. 15
The UTAUT has been specifically validated in healthcare technology, however, in this context, the model can be simplified as age has been found to be the only important modifier for healthcare technology, with a younger user age significantly correlated to intention to use (Figure 1). 17 The use of UTAUT in healthcare contexts in LMICs has also been demonstrated; however, the exact significance of major constructs may differ, and the degree of predictive performance has been shown to vary; it has also been utilized in African settings.18–20 While there remains some variation in performance in different contexts, this study remains well validated for evaluating technology in healthcare environments. The UTAUT was therefore identified as a relevant means of quantitative evaluation for implementing a mobile application trauma registry at the Mbarara Regional Referral Hospital (MRRH) in Uganda, along with open-ended, qualitative feedback from healthcare professionals at MRRH.
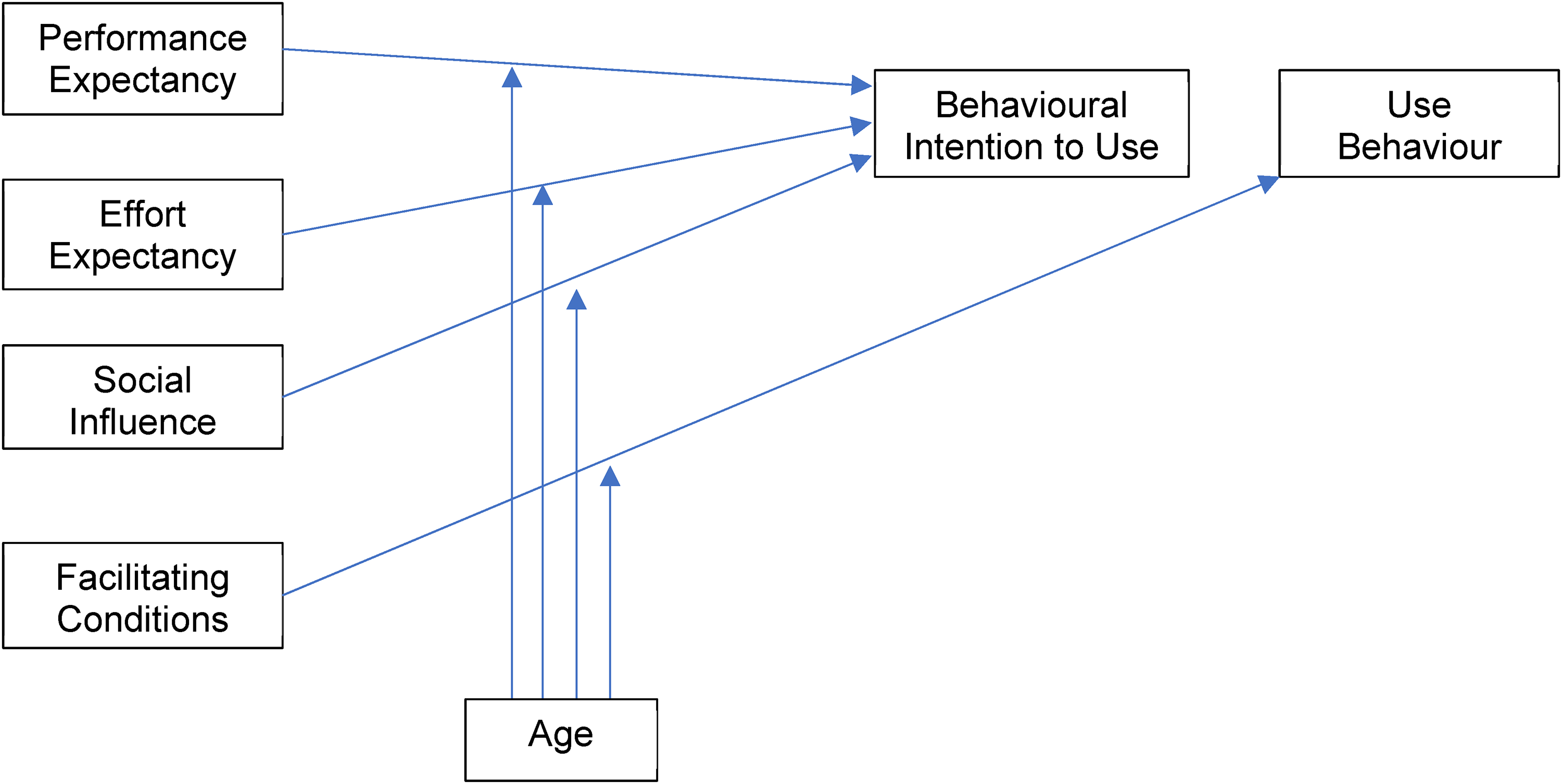
Modified Unified Theory of Acceptance and Use of Technology (UTAUT) for use by physicians (adapted from Venkatesh et al.). 15
Methods
Process of developing a mobile application trauma registry
A paper-based pilot trauma registry utilizing a minimal data set was developed, validated and implemented at MRRH in Uganda in conjunction with McMaster University (Canada) and the not-for-profit organization Innovative Canadians for Change (ICChange). Literature review, needs assessment and workflow assessment at MRRH was completed to initially develop the paper-based data collection tool which was then validated with a retrospective chart review. Data were collected from 2017 to 2019 by 2 part-time nurse data collectors for over 3600 trauma patients, both paediatric and adult, seen within 14 days of injury at MRRH in the Accidents and Emergencies Department and followed up by the surgical ward. Data were de-identified and later inputted into a secure, data-encrypted, password-protected data server in a locked room located at MRRH. A document linking personal identifiers to case identification codes was stored separately in a password-encrypted document and paper copies are stored separately in a locked filing cabinet in a locked office. A document linking personal identifiers to case identification codes is stored separately from the trauma registry data collection information in a password-protected document.
Through consultation with local stakeholders including medical staff, hospital administrators and medical records and information technology staff, the introduction of an electronic modality to facilitate data collection and analysis was identified as a priority to avoid duplication of workload. However, a lack of computer infrastructure was also identified as a concern for implementing eHealth technologies for use with the trauma registry. Local trauma healthcare providers suggested a mobile phone application as a more accessible means of accessing and inputting data into the trauma registry due to high mobile phone ownership and utilization. An Android-based mobile application was thus created to upload trauma patient data to the local data server, encompassing the same minimal data set as the paper-based trauma registry (online Supplementary Figure 2a and 2b). Data from this password-encrypted mobile application would be uploaded to the secure, password-encrypted server stored in a locked room at MRRH.
A lack of reliable internet access was identified as another concern and is echoed in the literature as a barrier to e-health in many developing countries. 21 Therefore, the ability to store data locally in the application when used in an off-line mode was incorporated into the design of the mobile application (data can then be uploaded to a server once connectivity is re-established). Furthermore, to reduce future implementation costs for other health care organizations wishing to adopt this technology, the mobile application was open-sourced so that a separate, secure version of the software could be utilized by other LMIC institutions in the future. Privacy protections for future use of the mobile application were built into the application, and these included password-protection, data encryption and de-identification of data within the mobile application and the data server; for this study, only hypothetical patient data were utilized for evaluation of the mobile application. Finally, in order to promote the sustainability of use of the mobile application, the data server is stored onsite at MRRH to promote local ownership of the data, and feedback on the mobile application from local healthcare providers was sought.
Evaluation of a mobile application trauma registry
In order to evaluate the mobile application trauma registry, healthcare providers involved in the initial care of trauma patients and the completion of trauma registry patient data at MRRH were identified. This included resident physicians, interns and trauma nurses (more senior physicians were not included as they were considered unlikely to complete documentation for trauma patients in the A&E department). Informed consent was obtained for participation in the survey, and healthcare providers were then given a 15-minute tutorial on the use of the trauma registry mobile application and then trialed inputting mock patient data into the mobile application which they could either download on their own device or utilize on a researcher's device. A mixed-methods design was employed, with participants completing a modified UTAUT questionnaire of technology acceptance, as well as written open-ended qualitative feedback (online Supplemental material). UTAUT responses were analysed using descriptive statistics and logistic regression; qualitative feedback was analysed by thematic analysis as described by Vaismoradi et al. 22 Research ethics approval for the initial implementation of the paper-based trauma registry was obtained through the Mbarara University of Science and Technology Research Ethics Committee (MUST-REC) in Mbarara, Uganda and McMaster University in Hamilton, Canada. Research ethics approval for the evaluation of the mobile application using hypothetical patient data was obtained from MUST-REC and the University of Alberta Research Ethics Board in Edmonton, Canada.
Results
Participant demographics
A total of 17/24 (70.9%) health care providers involved directly in trauma patient care and documentation completed the mobile application tutorial and questionnaire. The average age of participants was 29.1 (±3.9) years old and 53.9% were residents (9/17), 35.3% intern doctors (6/17) and 11.8% were nurses involved in trauma care (2/17); 88.2% of participants were male.
UTAUT scores
UTAUT scores were reported on a Likert scale ranging from 1 (strongly disagree) to 7 (strongly agree) (online Supplementary Figure 3). Scores were high for the three major constructs (Performance Expectancy, Effort Expectancy and Social Influence). For Performance eExpectancy, 92.7% of responses were scored as 5 or higher (somewhat agree to strongly agree; mean = 6.4, SD ± 1.4); for effort expectancy, 94.1% of scores were 5 or higher (mean 6.3, SD ± 1.4); and for social influence, 84.4% of scores ranked as 5 or higher (mean 5.4, SD ± 1.3). Overall, 70.6% of responses in the ‘facilitating conditions’ category of responses were scored as a 5 or higher (mean 5.3, SD ± 2.0), and 86.7% of participants reported a behavioural intention to use in under 6 months (mean 2.6 months, SD ± 1.6). For the indirect UTAUT constructs, 92.1% scored 5 or higher for attitude towards Technology (mean 6.1 ± 1.4) and 83.1% scored 5 or higher for Self-Efficacy (mean 5.9 ± 1.4). Anxiety, which is scored inversely on the UTAUT, had only 35.9% of scores scoring 5 or higher, with 50% of responses slightly to strongly disagreeing on experiencing Anxiety with use of the application (mean 2.6 ± 1.6) (online Supplementary Figure 3).
The only significant difference in scores between males and females was in the Social Influence category, where female respondents had an average Likert scale score of 6.6 (SD ± 0.5) compared to males with a mean score of 5.7 (SD ± 1.3). However, there was no significant difference in behavioural intention to use within 6 months or less between any of the demographic groups.
Univariate logistic regression analysis of factors predicting a behavioural intention to use <6 months was performed. From univariate analyses, all variables with a p < 0.2 were considered for a multivariate model. The only statistically significant factor identified was Facilitating Conditions (p = 0.010*). All other UTAUT variables measured, as well as age, gender and occupation, were not statistically significant predictors of behavioural intention to use category and therefore a multivariate logistic regression could not be performed. Overall behavioural intention to use was high, with 86.7% of participants indicating that they intended to use the application within 6 months’ time if available.
Qualitative analysis
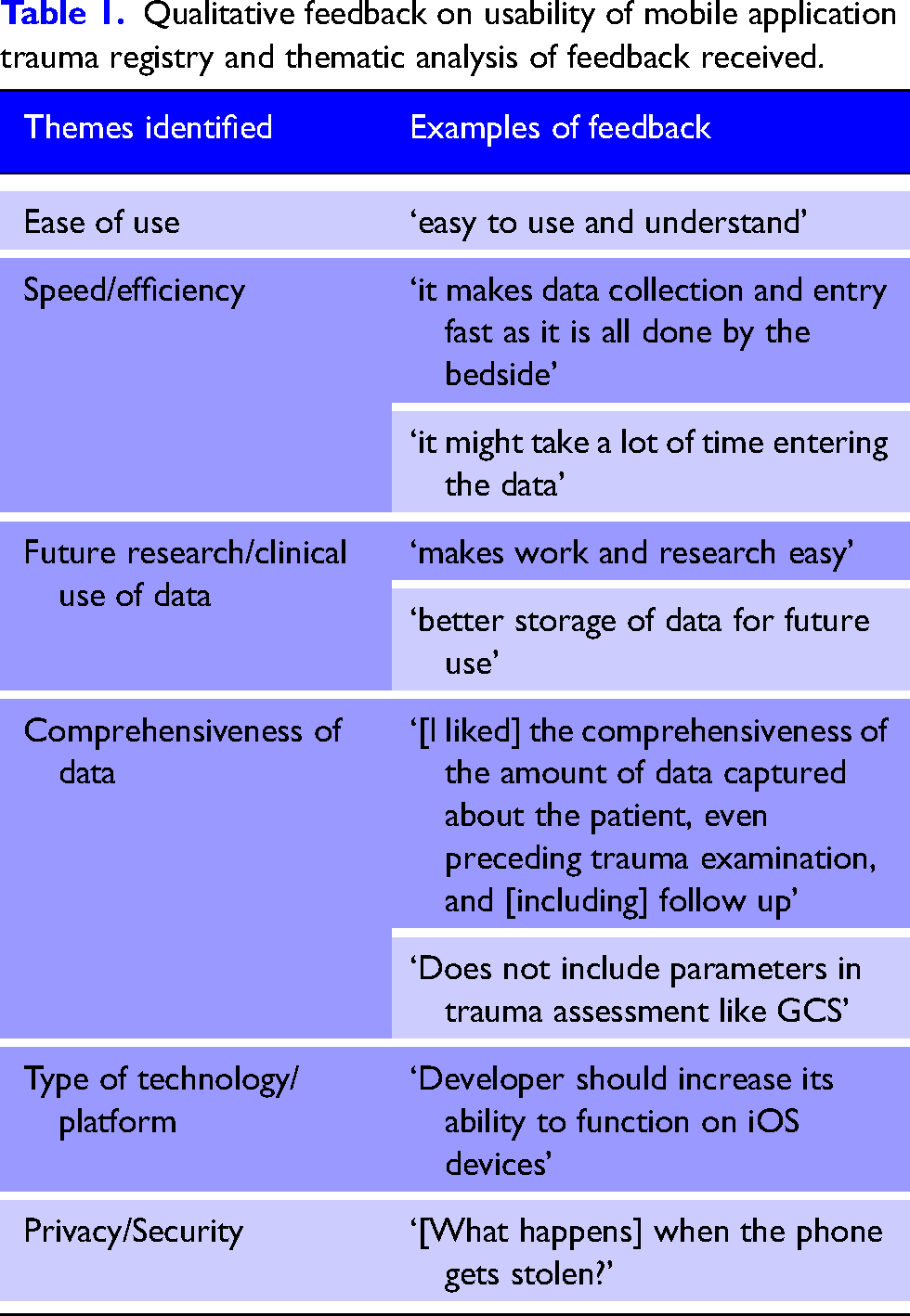
Qualitative themes identified in participant responses included ease of use, the benefits of large databases for future research and clinical work, efficiency of the mobile application and data comprehensiveness. Privacy and security concerns and type of platform were also identified as major themes from the qualitative feedback using the application (Table 1).
Qualitative feedback on usability of mobile application trauma registry and thematic analysis of feedback received.
Discussion
This study represents the implementation, development and evaluation of a mobile application trauma registry for use in a low- and middle-income setting. The analysis of this trauma registry application was done using a modified UTAUT questionnaire which predicts future usage behaviours. Overall, scores on the UTAUT survey were high, with the majority of participants responding positively to each construct on the validated questionnaire. The major constructs of Performance Expectancy, Effort Expectancy, Social Influence and Facilitating Conditions had mean Likert scores of 6.4, 6.3, 5.4 and 5.3, respectively. A young average user age (29.1 years) was also found in this study. Overall, high scores on UTAUT constructs and a young major user age have been found in previous studies to predict higher likelihood of usage behaviours in previous UTAUT studies in healthcare contexts and specifically in LMIC healthcare contexts.17–19
Facilitating Conditions refers to the infrastructural support that exists to support the use of a technology (including physical infrastructure, access to information technology support services and the time cost of using the technology). 23 In our study, Facilitating Conditions was the only major construct found to be significant in predicting the healthcare provider's intention to use the trauma registry mobile technology, and is consistent with previous studies. 18 Furthermore, this significance was supported by the qualitative responses from participants: time to use the application and type of mobile phone platforms required for use were widely cited as factors influencing the participant’s opinions of the mobile application. Although scores were still overall found to be positive for Facilitating Conditions with a mean Likert score of 5.3 and 70.6% of responses scored as a 5 or higher, this construct had relatively lower scores compared to other constructs and is, therefore, one potential area of focus for improvements to the application.
This study did not find a significant association between Performance Expectancy, Effort Expectancy, Social Influence, Self-Efficacy, Anxiety, age, or other demographic factors with future use behaviours. This is surprising, given many previous studies confirm a positive relationship between the UTAUT major constructs and intention to use in technology adoption.17,18 A significant difference in Social Influence scores did exist between males and females, however, this did not affect future intention to use the application. This lack of significance meant that a multivariate logistic regression model could not be created. The lack of significant association may reflect the limitations of a cross-sectional study with a small sample size and overall high scores reported with little variability reported, as the vast majority of participants reported high scores in all of these categories and high future use intentions. However, it was important to maintain internal validity of the study by surveying only trauma care providers at MRRH who would be likely to utilize this technology in the future, and therefore only healthcare providers involved in the direct and initial care of trauma patients were included in this survey.
Another potential limitation to this study may include non-response bias, with a response rate of 70.9% (17/24). However, though it is possible this could have led to differential misclassification if those who did not respond to the survey were more or less likely to have positive or negative responses to the application than those who did complete the survey, the reasons that responses were unable to be obtained were instead due to unavailability of healthcare providers who were away at other sites due to rotation schedule at the time of completion of the survey, which is unlikely to be related to factors of information technology acceptance. Another potential limitation of this type of study is social desirability bias, however, to mitigate the potential impact of this, local resident physicians and interns were recruited to administer surveys to their peers, surveys responses were kept anonymous with only indirectly identifying information collected, and an option to opt-out was provided discreetly on the response forms.
The results of the qualitative analysis found, in general, that healthcare providers found the application easy to use and efficient. The potential use for future research or clinical care was highlighted as a positive finding, and suggestions were made for expanding the data points collected to improve its functionality for these purposes. Several adaptations have already been made for use in a low-resource setting, including allowing data to be stored locally in the application when internet connection is lost and uploaded later. Privacy and security concerns were brought up by a few participants (‘data entry involves and includes patient names’ and ‘[what happens] when the phone gets stolen?’), and while the mobile application was designed to address these privacy concerns by utilizing data encryption, password protection and de-identification of data once uploaded to the data server, improved communication regarding these security and privacy protections needs to be incorporated into user training prior to implementation of the mobile application trauma registry.
Challenges remain for use of mobile application trauma registries in low-income settings. To improve user satisfaction, changes to the application are underway based on feedback received, including expanding use of the mobile application for multiple technology platforms and hiring local employees to provide information technology and eHealth records support onsite. The next steps to full implementation of the mobile application trauma registry include recruitment of additional local champions for use of the application, early adoption in clinical care and research and developing financial sustainability of the trauma registry so that it no longer depends on external research funding. Eventually, the development of an integrated combined eHealth record and trauma registry to reduce clinical workload could be considered if privacy and security concerns could be adequately addressed, and follow-up surveys on actual patterns of use, time commitments and quality assessments should take place following implementation.
Conclusion
This study demonstrates the process of developing and evaluating a mobile application trauma registry for use in LMICs through the use of the UTAUT questionnaire. The UTAUT represents a potential analysis method for information technology in healthcare settings and its use reflects the importance of consulting local stakeholders and front-line users of healthcare technology in LMICs.
Supplemental Material
sj-docx-1-tra-10.1177_14604086221129385 - Supplemental material for Development and evaluation of a mobile application trauma registry for use in low- and middle-income countries
Supplemental material, sj-docx-1-tra-10.1177_14604086221129385 for Development and evaluation of a mobile application trauma registry for use in low- and middle-income countries by Chantalle L. Grant, Ali Mohamad Ali, Felix Oyania, Patrick Oloya, Tessa Robinson, Brian Cameron, Martin Situma, Dean Eurich, David Bigam and Abdullah Saleh in Trauma
Supplemental Material
sj-docx-2-tra-10.1177_14604086221129385 - Supplemental material for Development and evaluation of a mobile application trauma registry for use in low- and middle-income countries
Supplemental material, sj-docx-2-tra-10.1177_14604086221129385 for Development and evaluation of a mobile application trauma registry for use in low- and middle-income countries by Chantalle L. Grant, Ali Mohamad Ali, Felix Oyania, Patrick Oloya, Tessa Robinson, Brian Cameron, Martin Situma, Dean Eurich, David Bigam and Abdullah Saleh in Trauma
Supplemental Material
sj-docx-3-tra-10.1177_14604086221129385 - Supplemental material for Development and evaluation of a mobile application trauma registry for use in low- and middle-income countries
Supplemental material, sj-docx-3-tra-10.1177_14604086221129385 for Development and evaluation of a mobile application trauma registry for use in low- and middle-income countries by Chantalle L. Grant, Ali Mohamad Ali, Felix Oyania, Patrick Oloya, Tessa Robinson, Brian Cameron, Martin Situma, Dean Eurich, David Bigam and Abdullah Saleh in Trauma
Footnotes
Acknowledgements
The authors would like to acknowledge the work of Dr. Regan Guilfoyle and Dr. Morad Hameed for their critical edits of this manuscript, and Kaiyang Fan for his administrative assistance for the logistics of this project.
Declaration of conflicting interests
AS is Chief Executive Director and Co-Founder of a not-for-profit organization Innovative Canadians for Change which contributed funding for the establishment of the Mbarara Regional Referral Hospital trauma registry. Provenance and peer review not commissioned, externally peer-reviewed.
Funding
This work was supported by the University of Alberta Department of Surgery Clinical Research Grant and the not-for-profit organization Innovative Canadians for Change.
Ethical approval
Ethical approval for this study was obtained from the Mbarara University of Science and Technology Research Ethics Committee (No. 20/08-18 and No. 03/10/16), the University of Alberta Research Ethics Board (Pro00083961), and the McMaster Hamilton Integrated Research Ethics Board (Project 1866).
Informed consent
Written informed consent was obtained from all subjects before the study.
Trial registration
Not applicable.
Guarantor
AS.
Contributorship
CG, AMA, FO, and MS participated in data collection and survey administration. Implementation and design of the trauma registry was performed in conjunction by BC, TR, MS, and AS. Authors CG, AS, DB, MS, and DE were involved in study design. Author CG was also responsible for data extraction and statistical analysis. All authors contributed to manuscript composition.
Supplemental material
Supplemental material for this article is available online.
References
Supplementary Material
Please find the following supplemental material available below.
For Open Access articles published under a Creative Commons License, all supplemental material carries the same license as the article it is associated with.
For non-Open Access articles published, all supplemental material carries a non-exclusive license, and permission requests for re-use of supplemental material or any part of supplemental material shall be sent directly to the copyright owner as specified in the copyright notice associated with the article.