
Abstract
Lemierre’s Syndrome is a rare phenomenon with a low prevalence and is characteristically seen in patients with an oropharyngeal infection that is complicated by thrombophlebitis of the internal jugular vein and secondary septic emboli. We present the case of a 16 year old previously well male who was diagnosed with a rare case of Lemierre’s syndrome secondary to a mandibular fracture. Blood tests and radiological imaging confirmed the diagnosis, with CT scan of the patients head and neck revealing a right mandibular fracture with abscess formation, bilateral parapharyngeal abscesses, bilateral internal jugular vein thromboses, left sigmoid sinus thrombosis, cavernous sinus thrombosis, post septal orbital cellulitis with enhancing infraorbital collections and a subdural empyema overlying the left tentorium cerebelli. The treatment is usually non-operative with antibiotics and in some instances surgical drainage. In this case a combination of surgical drainage for source control and antibiotics were used. Unfortunately, despite an initial improvement in the patient’s clinical status the patient died. This is the first case of Lemierre’s syndrome secondary to blunt facial trauma reported in the scientific literature. This case highlights the importance of clinicians having a high degree of suspicion of Lemierre’s syndrome when a patient presents with typical clinical features following facial trauma.
Introduction
Lemierre’s syndrome is characterized by septic thrombophlebitis of the internal jugular vein (IJV) due to a primary orofacial infection with secondary septic embolic phenomenon1–3 It typically originates as a bacterial peritonsillar infection and extension into lateral pharyngeal spaces with initial local peritonsillar vein thrombosis which progresses to septic IJV thrombosis and embolic dissemination to end points of circulation. 1 Post-traumatic orofacial infection with resultant IJV thrombophlebitis is an uncommon but potentially fatal complication. 4 We aim to describe a rare presentation of post-traumatic Lemierre’s syndrome to alert clinicians working with orofacial trauma of this potentially fatal complication.
Case report
A 16-year-old male patient, with no known co-morbidities, was referred to the intensive care unit (ICU) with a decreased level of consciousness, meningism, pyrexia, left periorbital oedema, bilateral chemosis, left eye ophthalmoplegia, mydriasis and anesthesia of the facial dermatomes innervated by the ophthalmic and maxillary divisions of the trigeminal nerve of the left side of the face. These features were indicative of cavernous sinus thrombosis.
One month prior to this presentation he had sustained blunt facial trauma secondary to an assault resulting in an isolated right sided, open mandibular fracture involving the 3rd Molar, which was initially untreated as he delayed in seeking out immediate care and only presented to his local regional hospital 1 week after the assault. He was referred to the maxillo-facial department at the tertiary referral hospital for further management of his mandibular fracture. There was no evidence of inferior alveolar nerve injury with sensation intact. The patient was assessed as having a septic wound with a pus collection. An incision and drainage procedure was performed by the maxillo-facial surgeons, and the patient was started on empiric antibiotics. A specimen was sent for microscopy, culture and sensitivity (MCS). Streptococcus mitis/oralis (STRMO) was cultured, which was sensitive to Clindamycin, Cefotaxime and Ceftriaxone.
The patient unfortunately absconded from the hospital post-surgery without completing treatment. He returned to his local regional hospital 2 weeks later, unwell and in a confused state and with bilateral periorbital swelling. The patient was admitted to the regional hospital and antibiotics were started based on the culture and sensitivity results of the specimen obtained during the initial abscess drainage. Over the next 2 days the patient’s level of consciousness decreased significantly to a Glasgow Coma Scale (GCS) of 8/15, and he was intubated to protect his airway. At this point the patient was referred to the ICU at the tertiary referral hospital for further management.
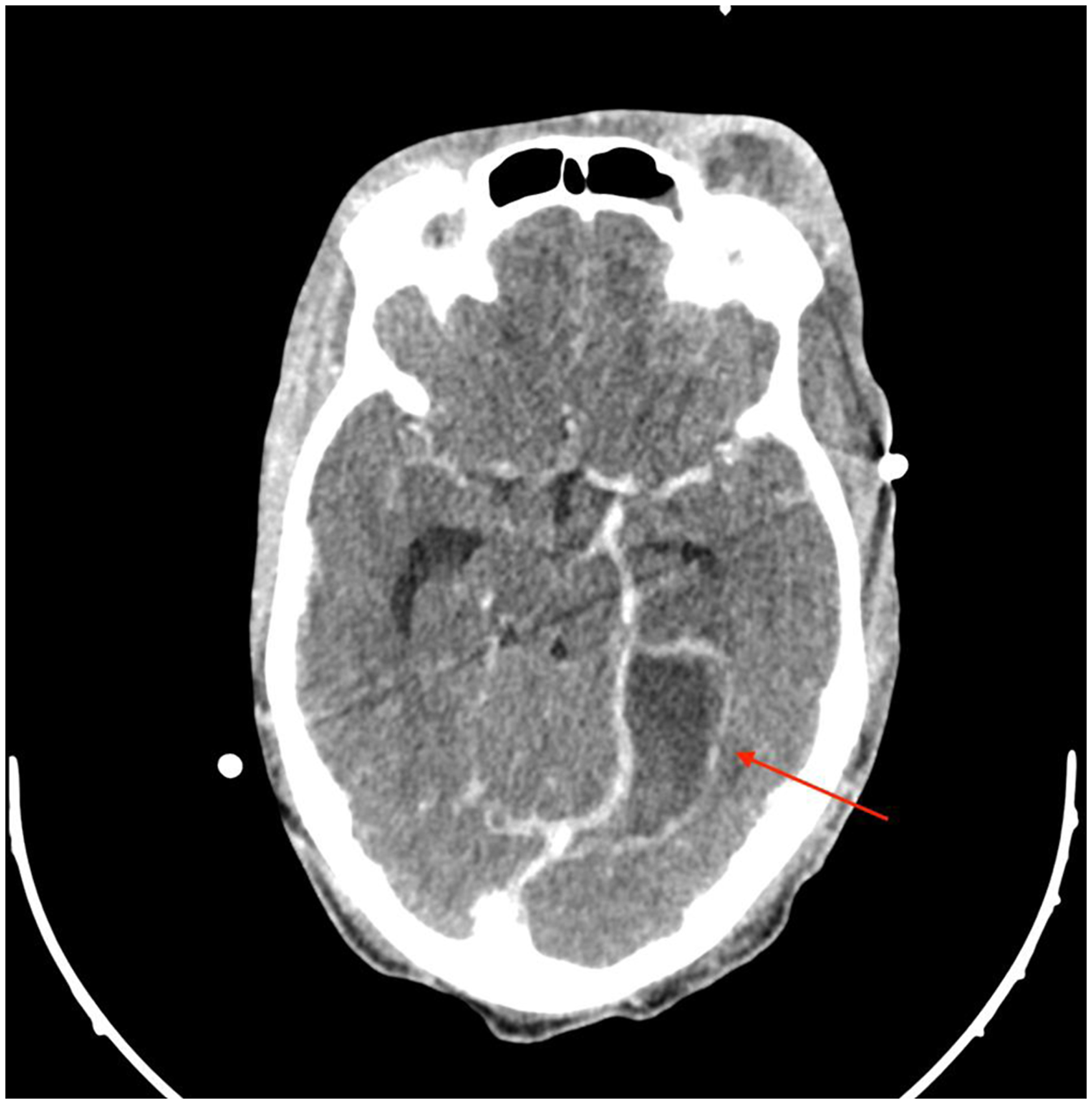
A computed tomography (CT) scan of the head demonstrated a right mandibular fracture with abscess formation lateral and medial to the mandible in the masticatory space (Figures 1 and 2), bilateral lateral parapharyngeal abscesses, bilateral internal jugular vein thromboses (Figure 3), left sigmoid sinus and cavernous sinus thromboses, post septal orbital cellulitis with enhancing infraorbital collections and a subdural empyema overlying the left tentorium cerebelli (Figure 4). In addition, the CT chest showed multiple cavitary lesions scattered throughout the lung fields bilaterally, in keeping with septic embolic phenomena (Figure 5). The patient however displayed no clinical signs of respiratory distress. The decreased level of consciousness was caused by subdural empyema and raised intracranial pressure secondary to spread of infection from the parapharyngeal/masticatory space Scout CT view showing the right mandibular fracture. Axial CT demonstrating an abscess in the right masticator space. Coronal CT showing thrombosis of the right internal jugular vein. Axial CT demonstrating left medial temporal subdural empyema. CT Chest with right sided pulmonary septic emboli.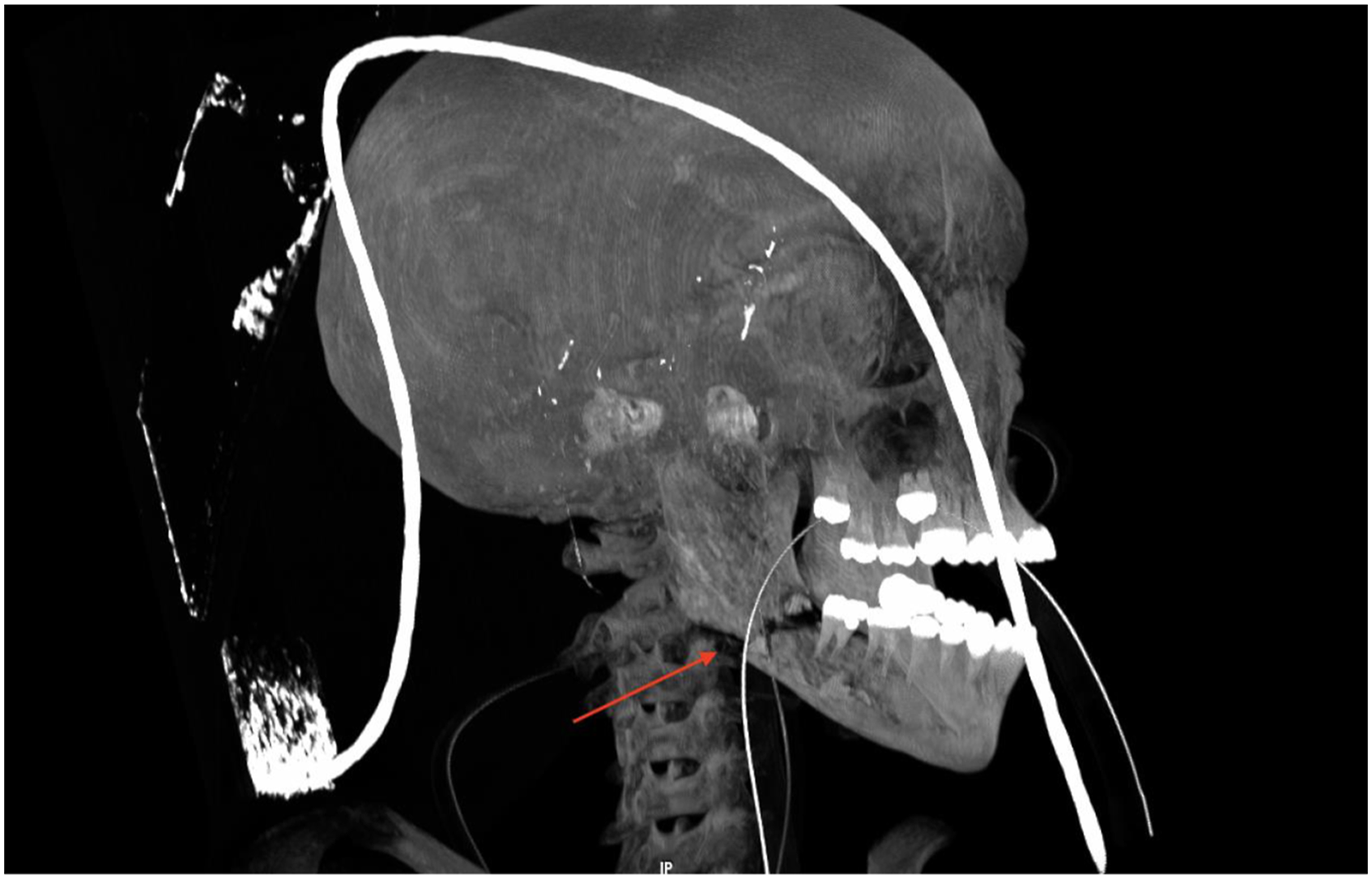



He was taken to theatre for urgent surgical drainage of the mandibular abscess with tooth extraction, transoral drainage of the bilateral parapharyngeal abscesses, drainage of the left orbital abscess, as well as a left temporal craniotomy and drainage of the subdural empyema. Post-surgical treatment included analgesia, empiric antimicrobial treatment with Ceftriaxone and Metronidazole, seizure prophylaxis with Sodium Valproate, therapeutic doses of unfractionated heparin as well as standard ICU care. He needed minimal ventilatory support and did not require inotropes for hemodynamic support.
Pus and blood cultures identified the bacterium Streptococcus constellatus which was sensitive to penicillin. Fusobacterium necrophorum was not cultured despite the microbiologist being alerted to the presence of Lemierre's Syndrome and adequate culture preparation for anaerobic organisms. Daily blood collections were performed to assess the trend of the infective markers. There was a downward trend of the C-reactive protein (CRP) from 207 to 115 and the white cell count (WCC) from 33.78 to 22.2 1 day after surgery and initiation of antimicrobial therapy.
His level of consciousness subsequently improved, and he was extubated 13 hours after surgery. On day two post-surgery his GCS rapidly declined to 5/15, E 1 V 1 M 3 and he developed bradycardia with hypertension. This was in keeping with a Cushing reflex suggestive of raised intracranial pressure. The patient was re-intubated and taken for an urgent CT scan of the head and neck with CT angiography. The scan showed a new onset acute hydrocephalus, residual subdural empyema and new onset left carotid artery thrombosis Figure 6 with resultant complete occlusion and right internal carotid artery thrombosis with partial occlusion. The mandibular, parapharyngeal, masticatory and orbital abscesses were adequately drained. Coronal CT image of thrombosis of the left internal carotid artery.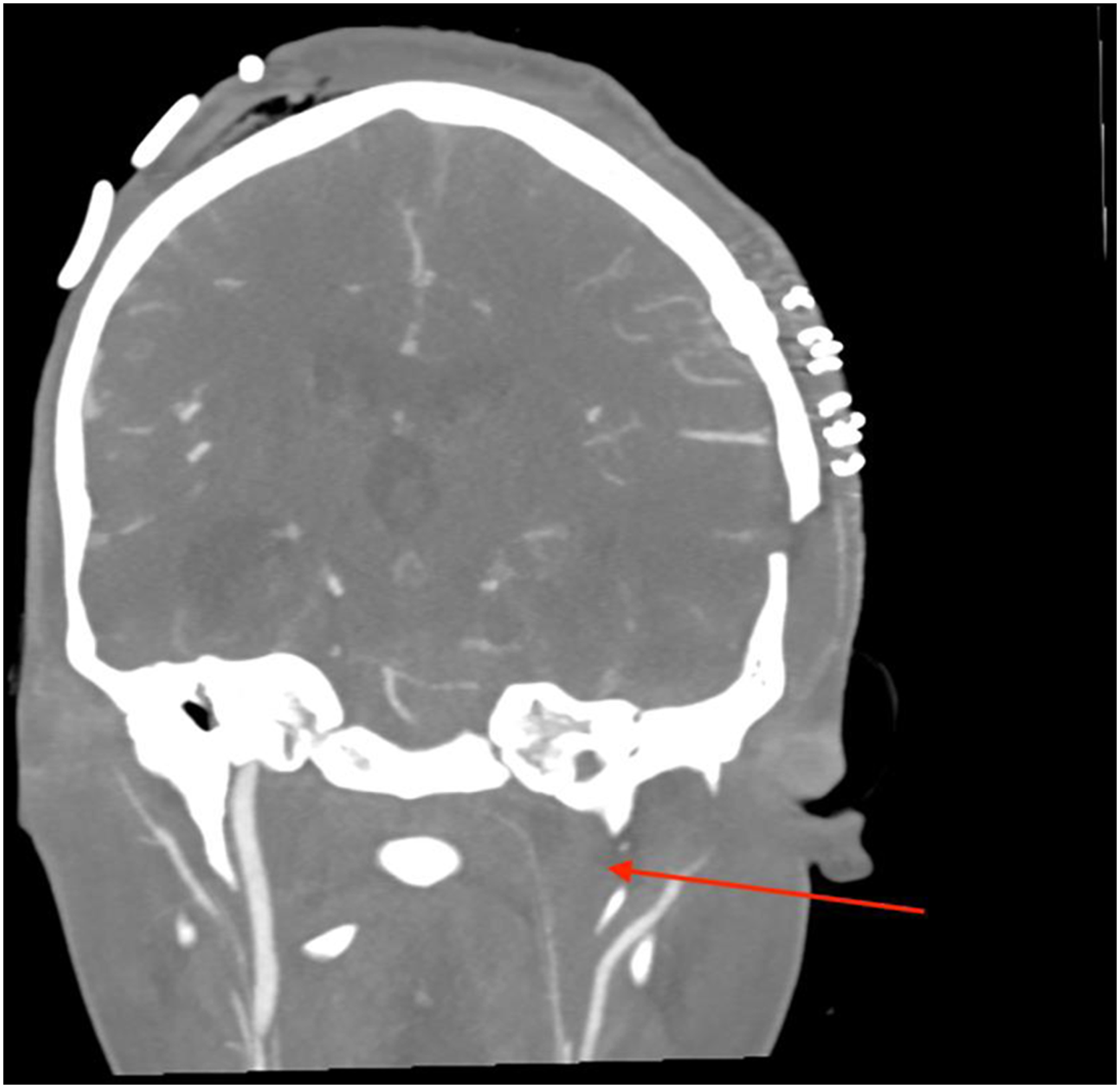
An emergency ventriculostomy with placement of an external ventricular drain was performed within 30 minutes of CT findings with an opening pressure of 45 cm H2O. Despite these measures he died 4 hours after the ventriculostomy procedure.
Discussion
Andre Lemierre first described septic thrombophlebitis after tonsillitis in 20 people in 1936. 5 The progression to Lemierre’s syndrome occurs in three phases: oropharyngeal infection, extension of infection into parapharyngeal space with thrombophlebitis of the IJV and then eventually septic emboli which may progress to septic shock in 7% of cases, and acute respiratory distress syndrome in 10%. The lungs are the most common site of septic emboli. Propagation of the IJV thrombus can result in central nervous system abscess formation as well as cavernous sinus thrombosis. 1 Arterial thrombosis occurs in only 2.9% of cases. 2
The most likely spread of organisms in the above case is via the pterygoid venous plexus, which is situated in the masticatory space, where an abscess had formed. The pterygoid venous plexus drains via the maxillary vein before it forms the retromandibular vein. In addition, the orbital and intracranial sepsis may be a result of retrograde spread via the inferior ophthalmic vein which drains into the pterygoid plexus as well as into the cavernous sinus. 6
The main site of infection is the palatine tonsils in 87.1% of cases. 2 Other sites that can serve as the primary site of infection are odontogenic infections, mastoiditis, sinusitis, otitis and soft tissue infections of the head and neck. The most common responsible bacterium is F. necrophorum (found in 80% percent of cases). 2 Five percent of cases are solely due to other organisms with Streptococcus species, Bacteroides species, Staphylococcus aureus and Klebsiella pneumoniae reported1,3,7 The remainder of cases demonstrate polymicrobial involvement 2
The condition typically affects young and previously healthy patients. Up to 90% of patients who develop Lemierre's Syndrome are between 10 and 35 years old. 1 Male patients are at higher risk, and there is a seasonal predilection to autumn and winter. 8 It is a rare syndrome with an estimated prevalence of 0.6–2.3 per million population, and has been referred to as the “forgotten disease” due to its rarity2,7,9 Advanced Lemierre's syndrome is a life-threatening condition even with appropriate antibiotics and surgical management, with a mortality rate as high as 18%. 1 There have been some cases reported to occur secondary to penetrating neck trauma and a single case secondary to blunt cervical trauma.4,10
Lemierre's syndrome is a clinical diagnosis and should be suspected in patients with neck swelling, 5 respiratory symptoms, with the presence of peritonsillar or retropharyngeal abscess formation. Imaging findings confirming IJV thrombosis, presence of infective emboli and blood cultures aid the diagnosis. 4 Although the most common offending organism, F. necrophorum, is usually a pan-sensitive organism, most patients are treated with broad spectrum antibiotics due to severity of presenting illness and concern for polymicrobial infection. There is overlap between the usual causative organisms in mandibular osteomyelitis which are of odontogenic source and microorganisms associated with Lemierres syndrome such as gram negative rods, Staphylococcus and Streptococcal species and anaerobes such as the genus Fusobacterium. 11
A two-to-six-week antibiotic course is recommended. Failure to respond to antibiotics and development of abscesses are indications for surgical management. There is no consensus on the role of anticoagulants however it is strongly recommended if there is clot progression, evidence of septic emboli or dural venous sinus thrombosis.8,12
With the widespread use of penicillin in the 1960’s and 1970’s the incidence of Lemierres Syndrome declined, however there is an increasing number of cases being reported in recent literature which may reflect reporting bias or the changing nature of antibiotic stewardship with decreased exposure to antibiotics for other conditions.9,10,13
Conclusion
Despite the greater awareness of Lemierre's syndrome, untreated facial trauma remains a rare cause, yet can be deadly, as in the case we have presented. Clinicians must maintain a high level of suspicion in patients who present with the typical symptoms following head and neck trauma, as early detection may avoid the progression to life-threatening sequela.
Footnotes
Declaration of conflicting interests
The author(s) declared no potential conflicts of interest with respect to the research, authorship, and/or publication of this article.
Funding
The author(s) received no financial support for the research, authorship, and/or publication of this article.
Ethical approval
Ethical approval to report this case was obtained from the Human Research Ethics Committee of Stellenbosch University (Reference number: C21/08/029; 30 August 2021).
Informed Consent
Written informed consent was obtained from a legally authorized representative(s) for anonymised patient information to be published in this article.
Guarantor
SC.
Contributorship
SK wrote the first draft of the manuscript. All authors reviewed and edited the manuscript and approved the final version of the manuscript.